


Use of Three-Dimensional Cell Culture Models in Drug Assays for Anti-Cancer Agents in Oral Cancer: Protocol for a Scoping Review

 ,
,  , ,
, ,  and
and
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Research Questions
- What protocols and techniques are recommended for applying three-dimensional culture methods in preclinical trials of anti-cancer drugs targeting oral cancer?
- Which 3D culture models have been predominantly utilized in preclinical drug trials for oral cancer treatment, and what are their primary applications?
- What are the documented advantages and challenges of using 3D culture models in preclinical drug trials for oral cancer as compared to traditional 2D models?
2.2. Study Design
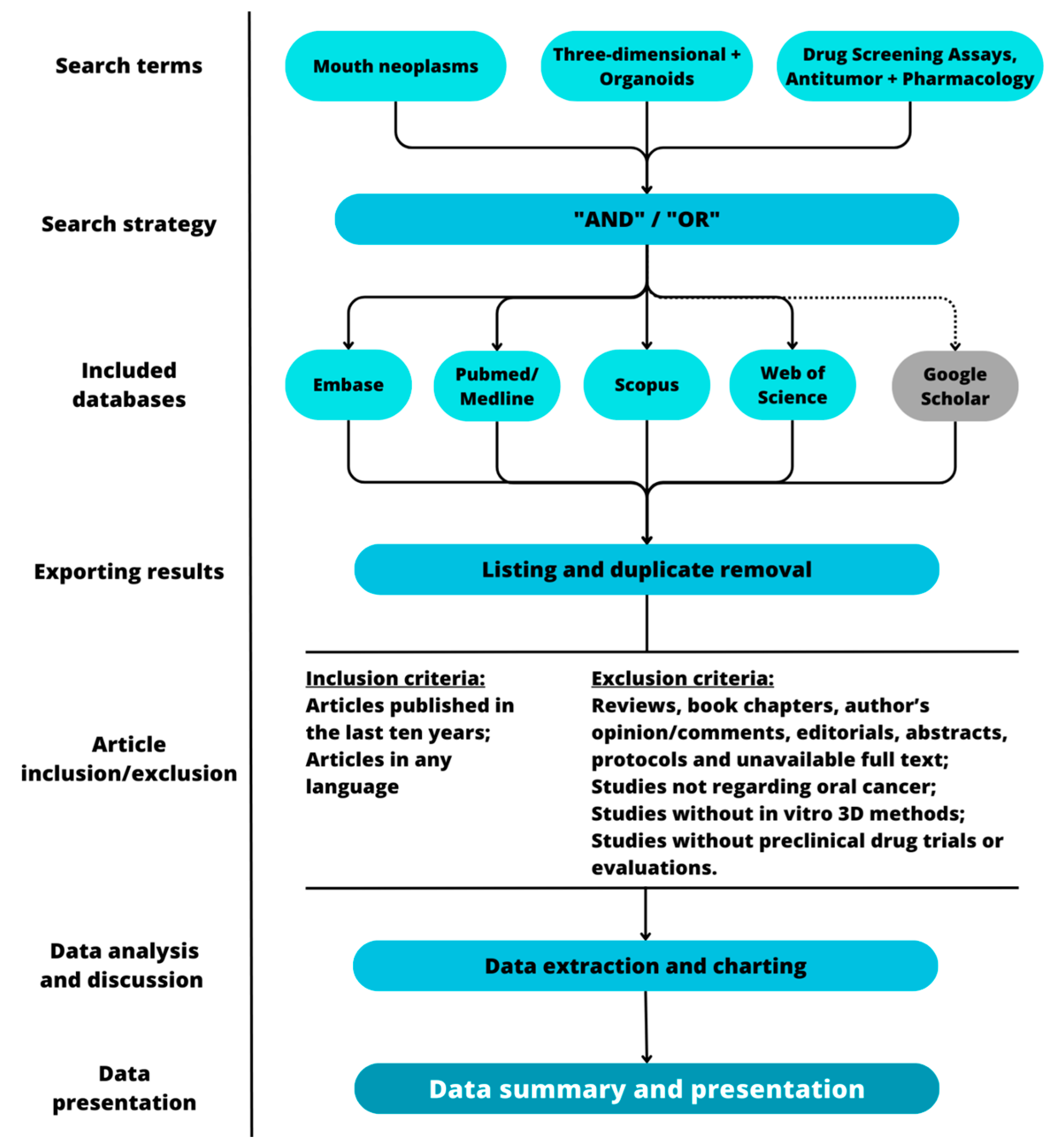
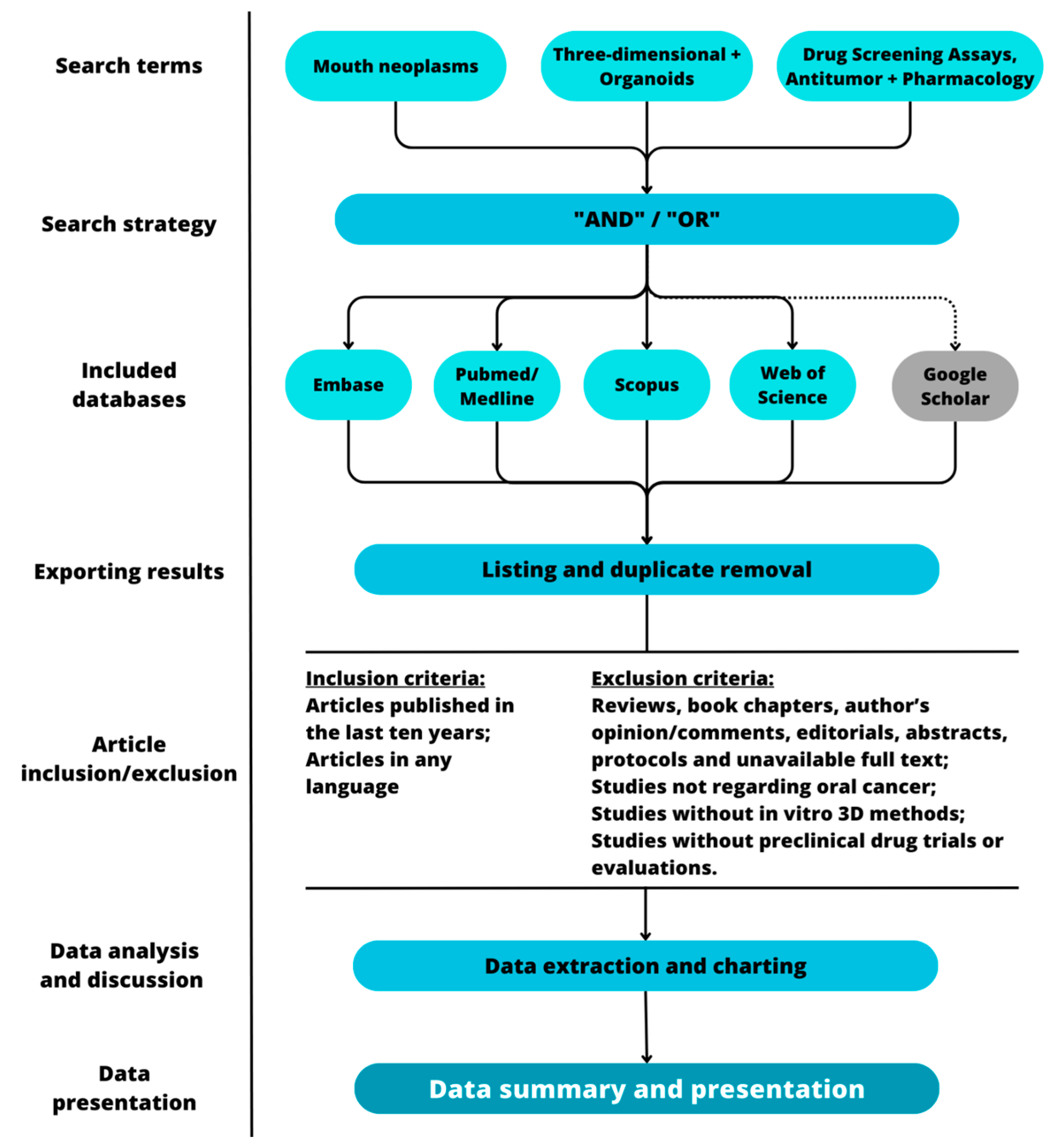
2.3. Search Strategy
2.4. Study Selection
2.4.1. Inclusion Criteria
2.4.2. Exclusion Criteria
- Reviews of any sort, book chapters, author’s opinion/comments, editorials, meeting abstracts, conference abstracts and study protocols, and articles without available full text;
- Studies not regarding oral cancer;
- Studies that did not employ in vitro three-dimensional methods of any sort;
- Studies that did not perform preclinical drug trials or evaluations.
2.5. Data Extraction and Charting
- What subtype or subtypes of oral cancer were evaluated (e.g., cell line, cell bank, origin, topographical location on the mouth)?
- What were the cell culture conditions (culture medium, additives, atmosphere, temperature)?
- What was the three-dimensional model or models used (e.g., spheroids, organoids, organ-on-a-chip) and their specifications (e.g., protocol steps, use of scaffolds, patient-derived explants)?
- What were the evaluated compounds and their relevant information (e.g., purchase, concentration)? Were they antineoplastic agents?
- What was the treatment protocol (e.g., application scheme, duration, association with other treatments)?
- What were the control group(s)/conditions?
- What assays were performed to evaluate compound effects (e.g., cell death, cytotoxicity, invasion, migration)? What were their results?
- What statistical analysis was performed? How many samples (e.g., number of spheroids or organoids) were used? How many assay repetitions were made?
- What are the authors’ conclusions?
- Overall, does the study mention all data accurately?
2.6. Analysis Plan
2.6.1. Data Analysis Approach
2.6.2. Data Summary
3. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- El-Naggar, A.K. WHO Classification of Head and Neck Tumours; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Gondivkar, S.M.; Gadbail, A.R.; Sarode, S.C.; Hedaoo, A.; Dasgupta, S.; Sharma, B.; Sharma, A.; Gondivkar, R.S.; Yuwanati, M.; Patil, S.; et al. Oral and general health-related quality of life in oral squamous cell carcinoma patients-comparative analysis of different treatment regims. J. Oral Biol. Craniofac. Res. 2021, 11, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Bavle, R.M.; Venugopal, R.; Konda, P.; Muniswamappa, S.; Makarla, S. Molecular Classification of Oral Squamous Cell Carcinoma. J. Clin. Diagn. Res. 2016, 10, ZE18. [Google Scholar] [CrossRef] [PubMed]
- Jehn, P.; Dittmann, J.; Zimmerer, R.; Stier, R.; Jehn, M.; Gellrich, N.C.; Tavassol, F.; Spalthoff, S. Survival Rates According to Tumour Location in Patients with Surgically Treated Oral and Oropharyngeal Squamous Cell Carcinoma. Anticancer Res. 2019, 39, 2527–2533. [Google Scholar] [CrossRef]
- Zandberg, D.P.; Tallon, L.J.; Nagaraj, S.; Sadzewicz, L.K.; Zhang, Y.; Strome, M.B.; Zhao, X.E.; Vavikolanu, K.; Zhang, X.; Papadimitriou, J.C.; et al. Intratumor genetic heterogeneity in squamous cell carcinoma of the oral cavity. Head Neck 2019, 41, 2514–2524. [Google Scholar] [CrossRef]
- Hunter, K.D.; Lambert, D.W.; Coletta, R.D. Editorial: The Translational and Therapeutic Potential of the Tumor Microenvironment in Oral Cancer. Front. Oral Health 2021, 2, 66. [Google Scholar] [CrossRef]
- Weinberg, R.A. The Biology of Cancer; W.W. Norton & Company: New York, NY, USA, 2013. [Google Scholar] [CrossRef]
- Elmusrati, A.; Wang, J.; Wang, C.Y. Tumor microenvironment and immune evasion in head and neck squamous cell carcinoma. Int. J. Oral Sci. 2021, 13, 24. [Google Scholar] [CrossRef]
- Peltanova, B.; Raudenska, M.; Masarik, M. Effect of tumor microenvironment on pathogenesis of the head and neck squamous cell carcinoma: A systematic review. Mol. Cancer 2019, 18, 63. [Google Scholar] [CrossRef]
- Matte, B.F.; Kumar, A.; Placone, J.K.; Zanella, V.G.; Martins, M.D.; Engler, A.J.; Lamers, M.L. Matrix stiffness mechanically conditions EMT and migratory behavior of oral squamous cell carcinoma. J. Cell Sci. 2019, 132, 224360. [Google Scholar] [CrossRef]
- Henke, E.; Nandigama, R.; Ergün, S. Extracellular Matrix in the Tumor Microenvironment and Its Impact on Cancer Therapy. Front. Mol. Biosci. 2020, 6, 470149. [Google Scholar] [CrossRef]
- Kumar, D.; New, J.; Vishwakarma, V.; Joshi, R.; Enders, J.; Lin, F.; Dasari, S.; Gutierrez, W.R.; Leef, G.; Ponnurangam, S.; et al. Cancer-associated fibroblasts drive glycolysis in a targetable signaling loop implicated in head and neck squamous cell carcinoma progression. Cancer Res. 2018, 78, 3769. [Google Scholar] [CrossRef] [PubMed]
- Kumar, K.V.; Hema, K.N. Extracellular matrix in invasion and metastasis of oral squamous cell carcinoma. J. Oral Maxillofac. Pathol. 2019, 23, 10. [Google Scholar] [CrossRef] [PubMed]
- Popova, N.V.; Jücker, M. The Functional Role of Extracellular Matrix Proteins in Cancer. Cancers 2022, 14, 238. [Google Scholar] [CrossRef]
- Chaicharoenaudomrung, N.; Kunhorm, P.; Noisa, P. Three-dimensional cell culture systems as an in vitro platform for cancer and stem cell modeling. World J. Stem Cells 2019, 11, 1065–1083. [Google Scholar] [CrossRef] [PubMed]
- Jensen, C.; Teng, Y. Is It Time to Start Transitioning From 2D to 3D Cell Culture? Front. Mol. Biosci. 2020, 7, 33. [Google Scholar] [CrossRef] [PubMed]
- Law, A.M.K.; Rodriguez de la Fuente, L.; Grundy, T.J.; Fang, G.; Valdes-Mora, F.; Gallego-Ortega, D. Advancements in 3D Cell Culture Systems for Personalizing Anti-Cancer Therapies. Front. Oncol. 2021, 11, 782766. [Google Scholar] [CrossRef]
- Anderson, N.M.; Simon, M.C. The tumor microenvironment. Curr. Biol. 2020, 30, R921–R925. [Google Scholar] [CrossRef]
- Baghban, R.; Roshangar, L.; Jahanban-Esfahlan, R.; Seidi, K.; Ebrahimi-Kalan, A.; Jaymand, M.; Kolahian, S.; Javaheri, T.; Zare, P. Tumor microenvironment complexity and therapeutic implications at a glance. Cell Commun. Signal. 2020, 18, 59. [Google Scholar] [CrossRef]
- Reinfeld, B.I.; Madden, M.Z.; Wolf, M.M.; Chytil, A.; Bader, J.E.; Patterson, A.R.; Sugiura, A.; Cohen, A.S.; Ali, A.; Do, B.T.; et al. Cell Programmed Nutrient Partitioning in the Tumor Microenvironment. Nature 2021, 593, 282. [Google Scholar] [CrossRef]
- Vaziri-Gohar, A.; Cassel, J.; Mohammed, F.S.; Zarei, M.; Hue, J.J.; Hajihassani, O.; Graor, H.J.; Srikanth, Y.V.; Karim, S.A.; Abbas, A.; et al. Limited nutrient availability in the tumor microenvironment renders pancreatic tumors sensitive to allosteric IDH1 inhibitors. Nat. Cancer 2022, 3, 852–865. [Google Scholar] [CrossRef]
- Emami Nejad, A.; Najafgholian, S.; Rostami, A.; Sistani, A.; Shojaeifar, S.; Esparvarinha, M.; Nedaeinia, R.; Haghjooy Javanmard, S.; Taherian, M.; Ahmadlou, M.; et al. The role of hypoxia in the tumor microenvironment and development of cancer stem cell: A novel approach to developing treatment. Cancer Cell Int. 2021, 21, 62. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhao, L.; Li, X.F. Hypoxia and the Tumor Microenvironment. Technol. Cancer Res. Treat. 2021, 20, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Aromataris, E.; Munn, Z. JBI Manual for Evidence Synthesis; JBI: North Adelaide, Australia, 2020. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMAScR): Checklist and Explanation. Ann Intern Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Pavan, L.M.C.; Rêgo, D.F.; Elias, S.T.; De Luca Canto, G.; Guerra, E.N.S. In vitro Anti-Tumor Effects of Statins on Head and Neck Squamous Cell Carcinoma: A Systematic Review. PLoS ONE 2015, 10, e0130476. [Google Scholar] [CrossRef]
- Xiao, Z.; Li, C.W.; Shan, J.; Luo, L.; Feng, L.; Lu, J.; Li, S.F.; Long, D.; Li, Y.P. Interventions to improve chronic cyclosporine A nephrotoxicity through inhibiting renal cell apoptosis: A systematic review. Chin. Med. J. 2013, 126, 3767–3774. [Google Scholar] [CrossRef]
- Xue, H.; Li, J.; Xie, H.; Wang, Y. Review of Drug Repositioning Approaches and Resources. Int. J. Biol. Sci. 2018, 14, 1232–1244. [Google Scholar] [CrossRef]
- Wouters, O.J.; McKee, M.; Luyten, J. Estimated Research and Development Investment Needed to Bring a New Medicine to Market, 2009–2018. JAMA 2020, 323, 844–853. [Google Scholar] [CrossRef]
- Yeu, Y.; Yoon, Y.; Park, S. Protein localization vector propagation: A method for improving the accuracy of drug repositioning. Mol. Biosyst. 2015, 11, 2096–2102. [Google Scholar] [CrossRef]
- Cavalcante, B.R.R.; Freitas, R.D.; de Oliveira Siquara da Rocha, L.; Rocha, G.V.; de Carvalho Pachêco, T.C.; Pereira Ramos, P.I.; Gurgel Rocha, C.A. In silico approaches for drug repurposing in oncology: Protocol for a scoping review of existing evidence. PLoS ONE 2022, 17, e0271002. [Google Scholar] [CrossRef]
- Kapałczyńska, M.; Kolenda, T.; Przybyła, W.; Zajączkowska, M.; Teresiak, A.; Filas, V.; Ibbs, M.; Bliźniak, R.; Łuczewski, Ł.; Lamperska, K. 2D and 3D cell cultures—A comparison of different types of cancer cell cultures. Arch. Med. Sci. 2018, 14, 910. [Google Scholar] [CrossRef] [PubMed]
- Stock, K.; Estrada, M.F.; Vidic, S.; Gjerde, K.; Rudisch, A.; Santo, V.E.; Barbier, M.; Blom, S.; Arundkar, S.C.; Selvam, I.; et al. Capturing tumor complexity in vitro: Comparative analysis of 2D and 3D tumor models for drug discovery. Sci. Rep. 2016, 6, 28951. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Brown, P.C.; Chow, E.C.Y.; Ewart, L.; Ferguson, S.S.; Fitzpatrick, S.; Freedman, B.S.; Guo, G.L.; Hedrich, W.; Heyward, S.; et al. 3D cell culture models: Drug pharmacokinetics, safety assessment, and regulatory consideration. Clin. Transl. Sci. 2021, 14, 1659–1680. [Google Scholar] [CrossRef]
- Brancato, V.; Oliveira, J.M.; Correlo, V.M.; Reis, R.L.; Kundu, S.C. Could 3D models of cancer enhance drug screening? Biomaterials 2020, 232, 119744. [Google Scholar] [CrossRef]
- Barbosa, M.A.G.; Xavier, C.P.R.; Pereira, R.F.; Petrikaitė, V.; Vasconcelos, M.H. 3D Cell Culture Models as Recapitulators of the Tumor Microenvironment for the Screening of Anti-Cancer Drugs. Cancers 2021, 14, 190. [Google Scholar] [CrossRef]
- Poornima, K.; Francis, A.P.; Hoda, M.; Eladl, M.A.; Subramanian, S.; Veeraraghavan, V.P.; El-Sherbiny, M.; Asseri, S.M.; Hussamuldin, A.B.A.; Surapaneni, K.M.; et al. Implications of Three-Dimensional Cell Culture in Cancer Therapeutic Research. Front. Oncol. 2022, 12, 891673. [Google Scholar] [CrossRef] [PubMed]
- Farhat, J.; Pandey, I.; AlWahsh, M. Transcending toward Advanced 3D-Cell Culture Modalities: A Review about an Emerging Paradigm in Translational Oncology. Cells 2021, 10, 1657. [Google Scholar] [CrossRef]
- Fumagalli, A.; Drost, J.; Suijkerbuijk, S.J.E.; van Boxtel, R.; de Ligt, J.; Offerhaus, G.J.; Begthel, H.; Beerling, E.; Tan, E.H.; Sansom, O.J.; et al. Genetic dissection of colorectal cancer progression by orthotopic transplantation of engineered cancer organoids. Proc. Natl. Acad. Sci. USA 2017, 114, E2357–E2364. [Google Scholar] [CrossRef]
- Fumagalli, A.; Suijkerbuijk, S.J.E.; Begthel, H.; Beerling, E.; Oost, K.C.; Snippert, H.J.; van Rheenen, J.; Drost, J. A surgical orthotopic organoid transplantation approach in mice to visualize and study colorectal cancer progression. Nat. Protoc. 2018, 13, 235–247. [Google Scholar] [CrossRef]
- Fujii, M.; Shimokawa, M.; Date, S.; Takano, A.; Matano, M.; Nanki, K.; Ohta, Y.; Toshimitsu, K.; Nakazato, Y.; Kawasaki, K.; et al. A colorectal tumor organoid library demonstrates progressive loss of niche factor requirements during tumorigenesis. Cell Stem Cell 2016, 18, 827–838. [Google Scholar] [CrossRef]
- Ki, C.S.; Shih, H.; Lin, C.C. Effect of 3D matrix compositions on the efficacy of EGFR inhibition in pancreatic ductal adenocarcinoma cells. Biomacromolecules 2013, 14, 3017–3026. [Google Scholar] [CrossRef] [PubMed]
- de Morais, E.F.; Almangush, A.; Salo, T.; da Silva, S.D.; Kujan, O.; Coletta, R.D. Emerging histopathological parameters in the prognosis of oral squamous cell carcinomas. Histol. Histopathol. 2023, 18634. [Google Scholar] [CrossRef]
- Liu, C.; Wang, M.; Zhang, H.; Li, C.; Zhang, T.; Liu, H.; Zhu, S.; Chen, J. Tumor microenvironment and immunotherapy of oral cancer. Eur. J. Med. Res. 2022, 27, 198. [Google Scholar] [CrossRef] [PubMed]
- Shao, C.; Zhang, Q.; Kuang, G.; Fan, Q.; Ye, F. Construction and application of liver cancer models in vitro. Eng. Regen. 2022, 3, 310–322. [Google Scholar] [CrossRef]
- Rebelo, S.P.; Pinto, C.; Martins, T.R.; Harrer, N.; Estrada, M.F.; Loza-Alvarez, P.; Cabeçadas, J.; Alves, P.M.; Gualda, E.J.; Sommergruber, W.; et al. 3D-3-culture: A tool to unveil macrophage plasticity in the tumour microenvironment. Biomaterials 2018, 163, 185–197. [Google Scholar] [CrossRef]
- Pasch, C.A.; Favreau, P.F.; Yueh, A.E.; Babiarz, C.P.; Gillette, A.A.; Sharick, J.T.; Karim, M.R.; Nickel, K.P.; DeZeeuw, A.K.; Sprackling, C.M.; et al. Patient-derived cancer organoid cultures to predict sensitivity to chemotherapy and radiation. Clin. Cancer Res. 2019, 25, 5376–5387. [Google Scholar] [CrossRef]
- Gomez, K.E.; Wu, F.; Keysar, S.B.; Morton, J.J.; Miller, B.; Chimed, T.S.; Le, P.N.; Nieto, C.; Chowdhury, F.N.; Tyagi, A.; et al. Cancer Cell CD44 Mediates Macrophage/Monocyte-Driven Regulation of Head and Neck Cancer Stem Cells. Cancer Res. 2020, 80, 4185–4198. [Google Scholar] [CrossRef]
- Jubelin, C.; Muñoz-Garcia, J.; Griscom, L.; Cochonneau, D.; Ollivier, E.; Heymann, M.F.; Vallette, F.M.; Oliver, L.; Heymann, D. Three-dimensional in vitro culture models in oncology research. Cell Biosci. 2022, 12, 155. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Population | Concept | Context |
|---|---|---|
| N/A | Three-dimensional models used for drug screening | Oral Cancer |
| Database | Strategy |
|---|---|
| PubMed/Medline | ((“Mouth Neoplasms” [Mesh] OR “Mouth Neoplasms” OR “Mouth Neoplasm” OR “Neoplasm, Mouth” OR “Neoplasms, Oral” OR “Neoplasm, Oral” OR “Oral Neoplasm” OR “Oral Neoplasms” OR “Cancer of Mouth” OR “Mouth Cancers” OR “Oral Cancer” OR “Cancer, Oral” OR “Cancers, Oral” OR “Oral Cancers” OR “Cancer of the Mouth” OR “Mouth Cancer” OR “Cancer, Mouth” OR “Cancers, Mouth” OR “Oral Tongue Squamous Cell Carcinoma” OR “Oral Squamous Cell Carcinoma” OR “Oral Cavity Squamous Cell Carcinoma” OR “Oral Squamous Cell Carcinomas” OR “Squamous Cell Carcinoma of the Mouth”) AND (“Cell Culture Techniques, Three Dimensional” [Mesh] OR “Cell Culture Techniques, Three Dimensional” OR “3D Cell Culture” OR “3D Cell Cultures” OR “Cell Culture, 3D” OR “Cell Cultures, 3D” OR “Cultures, 3D Cell” OR “3-Dimensional Cell Culture” OR “3 Dimensional Cell Culture” OR “3-Dimensional Cell Cultures” OR “Three-Dimensional Cell Culture” OR “Cell Culture, Three-Dimensional” OR “Cell Cultures, Three-Dimensional” OR “Three Dimensional Cell Culture” OR “Three-Dimensional Cell Cultures” OR “3-D Cell Culture” OR “3 D Cell Culture” OR “3-D Cell Cultures” OR “Cell Culture, 3-D” OR “Scaffold Cell Culture Techniques” OR “Scaffold Cell Culture” OR “Cell Culture, Scaffold” OR “Cell Cultures, Scaffold” OR “Scaffold Cell Cultures” OR “Organoids” [Mesh] OR “Organoids” OR “Organoid”)) AND (“Drug Screening Assays, Antitumor” [Mesh] OR “Drug Screening Assays, Antitumor” OR “Antitumor Drug Screening Assays” OR “Cancer Drug Test” OR “Antitumor Drug Screen” OR “Anti-Cancer Drug Screens” OR “Anti Cancer Drug Screens” OR “Anti-Cancer Drug Screen” OR “Screen, Anti-Cancer Drug” OR “Anticancer Drug Sensitivity Tests” OR “Tumor-Specific Drug Screening Tests” OR “Tumor Specific Drug Screening Tests” OR “Pharmacology” [Mesh] OR “Pharmacology” OR “Pharmacologies”) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Freitas de Morais, E.; Siquara da Rocha, L.d.O.; de Souza Santos, J.L.; Freitas, R.D.; Souza, B.S.d.F.; Coletta, R.D.; Gurgel Rocha, C.A. Use of Three-Dimensional Cell Culture Models in Drug Assays for Anti-Cancer Agents in Oral Cancer: Protocol for a Scoping Review. J. Pers. Med. 2023, 13, 1618. https://doi.org/10.3390/jpm13111618
Freitas de Morais E, Siquara da Rocha LdO, de Souza Santos JL, Freitas RD, Souza BSdF, Coletta RD, Gurgel Rocha CA. Use of Three-Dimensional Cell Culture Models in Drug Assays for Anti-Cancer Agents in Oral Cancer: Protocol for a Scoping Review. Journal of Personalized Medicine. 2023; 13(11):1618. https://doi.org/10.3390/jpm13111618
Chicago/Turabian StyleFreitas de Morais, Everton, Leonardo de Oliveira Siquara da Rocha, John Lenon de Souza Santos, Raíza Dias Freitas, Bruno Solano de Freitas Souza, Ricardo D. Coletta, and Clarissa A. Gurgel Rocha. 2023. "Use of Three-Dimensional Cell Culture Models in Drug Assays for Anti-Cancer Agents in Oral Cancer: Protocol for a Scoping Review" Journal of Personalized Medicine 13, no. 11: 1618. https://doi.org/10.3390/jpm13111618
APA StyleFreitas de Morais, E., Siquara da Rocha, L. d. O., de Souza Santos, J. L., Freitas, R. D., Souza, B. S. d. F., Coletta, R. D., & Gurgel Rocha, C. A. (2023). Use of Three-Dimensional Cell Culture Models in Drug Assays for Anti-Cancer Agents in Oral Cancer: Protocol for a Scoping Review. Journal of Personalized Medicine, 13(11), 1618. https://doi.org/10.3390/jpm13111618