
COVID-19 Vaccines during Pregnancy and Breastfeeding: A Systematic Review


Abstract
:1. Introduction
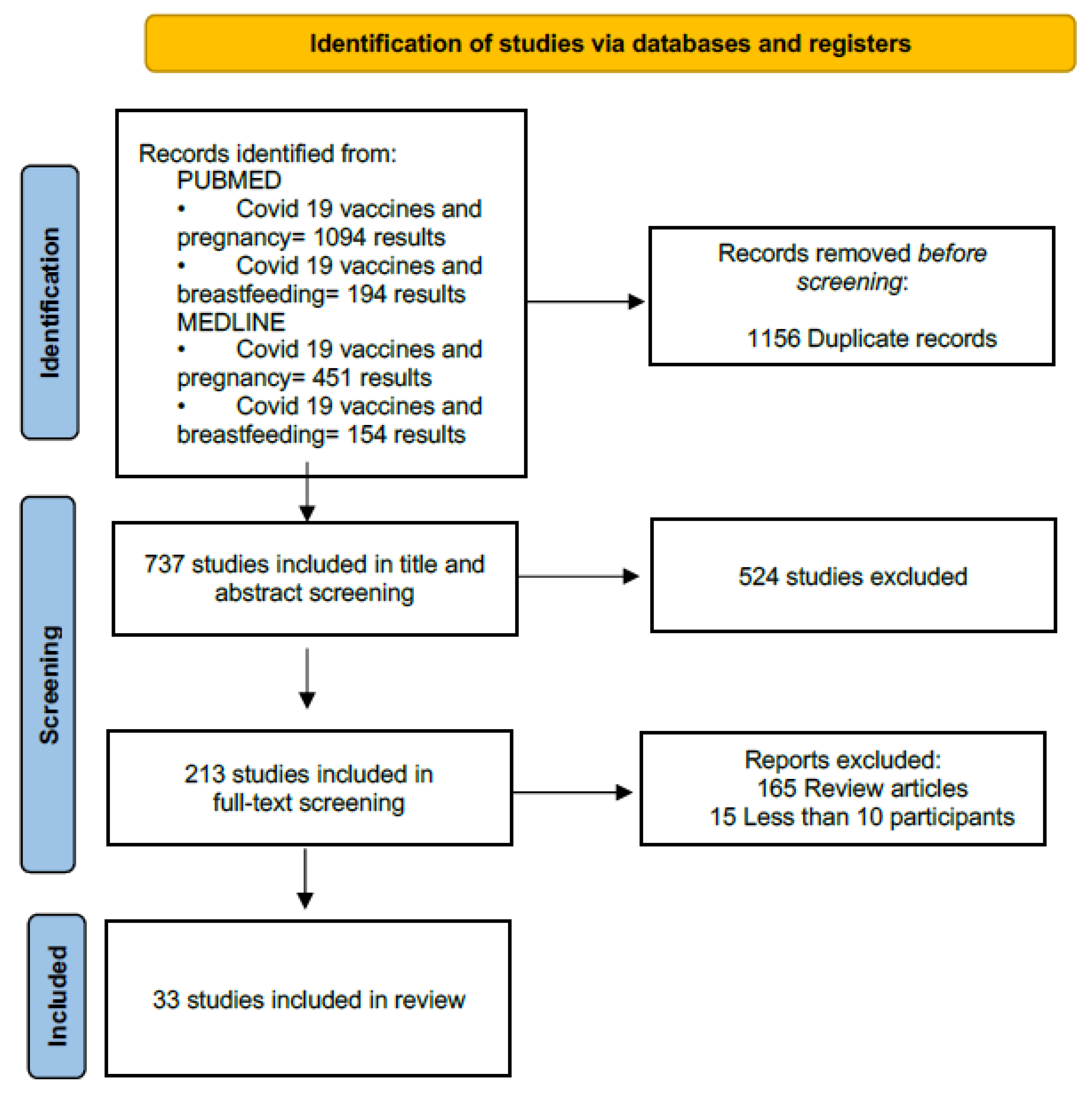
2. Materials and Methods
3. Results

{kind=link}
| Author | Population | N | Study Design | Vaccine Type | No Dose | Country | Date of Publication |
|---|---|---|---|---|---|---|---|
| Atyeo [28] | Pregnant, breastfeeding and non-pregnant. | 131 | Observational cohort | Pfizer or Moderna | 2 | USA | 10/2021 |
| Bertrand [29] | Breastfeeding vaccinated | 180 | Observational cohort | Pfizer or Moderna | 1 or 2 | USA | 08/2021 |
| Calil [27] | Breastfeeding vaccinated | 20 | Observational cohort | CoronaVac (Biotech) | 2 | Brazil | 06/2021 |
| Charepe [30] | Breastfeeding and not | 24 | Observational cohort | Pfizer | 2 | Portugal | 09/2021 |
| Collier [31] | Pregnant and breastfeeding vaccinated and unvaccinated infected | 131 | Observational cohort | Pfizer or Moderna | Does not specify | USA | 03/2021 |
| Esteve-Palau [32] | Breastfeeding vaccinated | 33 | Observational cohort | Pfizer | 2 | Spain | 08/2021 |
| Rosenberg-Friedman [33] | Breastfeeding vaccinated | 10 | Observational cohort | Pfizer | 2 | Israel | 03/2021 |
| Golan [34] | Breastfeeding vaccinated | 50 | Observational cohort | Pfizer or Moderna | 2 | USA | 11/2021 |
| Gonçalves [35] | Breastfeeding, vaccinated | 23 | Observational cohort | Pfizer or Moderna | 2 | Portugal | 12/2021 |
| Gray [36] | Pregnant, breastfeeding and non-pregnant. | 131 | Observational cohort | Pfizer or Moderna | 1 or 2 | USA | 09/2021 |
| Guida [37] | Breastfeeding, vaccinated | 10 | Observational cohort | Pfizer | 2 | Italy | 07/2021 |
| Jakuszko [38] | Breastfeeding vaccinated and not vaccinated | 60 | Observational cohort | Pfizer | 2 | Poland | 06/2021 |
| Juncker [39] | Breastfeeding vaccinated | 26 | Observational cohort | Pfizer | 2 | Netherlands | 08/2021 |
| Kachikis [40] | Pregnant, breastfeeding and planning pregnancy vaccinated. | 17,525 | Observational cohort | Pfizer or Moderna | 1 or 2 | USA | 08/2021 |
| Kadali [19] | Pregnant vaccinated | 38 | Cross-sectional | Pfizer or Moderna | 1 or 2 | USA | 10/2021 |
| Lechosa-Muñiz [20] | Breastfeeding vaccinated | 110 | Cross-Sectional | Pfizer, Moderna, or AstraZeneca | 1 or 2 | Spain | 08/2021 |
| Low [41] | Breastfeeding, vaccinated or unvaccinated or infected | 25 | Observational cohort | Pfizer | 2 | Singapore | 08/2021 |
| McLaurin-Jiang [21] | Breastfeeding vaccinated | 4455 | Cross-sectional | Pfizer or Moderna | 1 or 2 | USA | 06/2021 |
| Mithal [42] | Pregnant vaccinated | 27 | Observational cohort | Pfizer or Moderna | 1 or 2 | USA | 08/2021 |
| Montalti [43] | Breastfeeding and pregnant | 600 | Observational cohort | Pfizer | 2 | Italy | 08/2021 |
| Olearo [44] | Breastfeeding, vaccinated or not, having had de infection or not | 21 | Observational cohort | Pfizer | 1 or 2 | Germany | 09/2022 |
| Perez [45] | Pregnant or breastfeeding vaccinated | 30 | Observational cohort | Pfizer or Moderna | 1 | USA | 02/2022 |
| Perl [46] | Breastfeeding vaccinated | 84 | Observational cohort | Pfizer | 2 | Israel | 04/2021 |
| Pietrasanta [47] | Breastfeeding vaccinated and their babies | 24 | Observational cohort | Pfizer | 2 | Italy | 06/2022 |
| Prabhu [48] | Pregnant vaccinated | 122 | Observational cohort | Pfizer or Moderna | 1 or 2 | USA | 04/2021 |
| Rottenstreich [49] | Pregnant vaccinated | 20 | Observational cohort | Pfizer | 2 | Israel | 04/2021 |
| Scrimin [50] | Breastfeeding vaccinated, infected or not | 42 | Observational cohort | Pfizer, Moderna, or AstraZeneca | 1 or 2 | Italy | 01/2022 |
| Selma-Royo [25] | Breastfeeding vaccinated vs Breastfeeding not vaccinated | 86 | Observational cohort | Pfizer, Moderna, or AstraZeneca | 2 | Spain | 04/2021 |
| Shanes [22] | Pregnant vaccinated and unvaccinated | 200 | Case control | Not mentioned | Not mentioned | USA | 08/2021 |
| Shimabukuro [51] | Pregnant vaccinated | 35,691 | Observational cohort | Pfizer or Moderna | 1 or 2 | USA | 04/2021 |
| Theiler [23] | Pregnant vaccinated vs not vaccinated | 2002 | Case- control | Pfizer, Janssen, or Moderna | 1 or 2 | USA | 11/2021 |
| Young [17] | Breastfeeding vaccinated or infected | 77 | Observational cohort | Moderna or Pfizer | 2 | USA | 11/2021 |
| Martínez-Varea [26] | Pregnant infected vaccinated or not | 487 | Observational cohort | Pfizer, Moderna, or AstraZeneca | 2 | Spain | 12/2022 |
3.1. Safety
3.2. Efficacy
3.3. Immunogenicity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| Messenger ribonucleic acid | mARN |
| Immunoglobulin A, G, M | IgA, IgG, IgM |
References
- Ouzounian, J.G.; Elkayam, U. Physiologic changes during normal pregnancy and delivery. Cardiol. Clin. 2012, 30, 317–329. [Google Scholar] [CrossRef] [PubMed]
- Meah, V.L.; Cockcroft, J.R.; Backx, K.; Shave, R.; Stohr, E.J. Cardiac output and related haemodynamics during pregnancy: A series of meta-analyses. Heart 2016, 102, 518–526. [Google Scholar] [CrossRef] [PubMed]
- Mor, G.A. The immunology of pregnancy. In Creasy and Resnik’s Maternal-Fetal Medicine: Principles and Practice, 7th ed.; Creasy, R.K., Resnik, R., Iams, J.D., Lockwood, C.J., Moore, T.R., Greene, M., Eds.; Elsevier: Philadelphia, PA, USA, 2014; p. 80. [Google Scholar]
- Bauer, K.A. Maternal Adaptations to Pregnancy: Hematologic Changes 2022. Available online: https://www.uptodate.com/contents/maternal-adaptations-to-pregnancy-hematologic-changes?search=Maternal%20adaptations%20to%20pregnancy:%20Hematologic%20changes.&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1 (accessed on 1 November 2022).
- Allotey, J.; Stallings, E.; Bonet, M.; Yap, M.; Chatterjee, S.; Kew, T.; Zhou, D.; Coomar, D.; Sheikh, J.; Lawson, H.; et al. Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: Living systematic review and meta-analysis. BMJ 2020, 370, m3320. [Google Scholar] [CrossRef] [PubMed]
- WAPM (World Association of Perinatal Medicine) Working Group on COVID-19. Maternal and perinatal outcomes of pregnant women with SARS-CoV-2 infection. Ultrasound Obstet. Gynecol. 2021, 57, 232–241. [Google Scholar] [CrossRef] [PubMed]
- Berghella, V.; Hughes, B.L. COVID-19: Overview of Pregnancy Issues. 2022. Available online: https://www.uptodate.com/contents/covid-19-overview-of-pregnancy-issues?search=pregnant%20outcomes%20covid%20disease&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1#H3318902741 (accessed on 1 November 2022).
- McClymont, E.; Albert, A.Y.; Alton, G.D.; Boucoiran, I.; Castillo, E.; Fell, D.B.; Kuret, V.; Poliquin, V.; Reeve, T.; Scott, H.; et al. Association of SARS-CoV-2 Infection During Pregnancy with Maternal and Perinatal Outcomes. JAMA 2022, 327, 1983–1991. [Google Scholar] [CrossRef]
- Villar, J.; Ariff, S.; Gunier, R.B.; Thiruvengadam, R.; Rauch, S.; Kholin, A.; Roggero, P.; Prefumo, F.; do Vale, M.S.; Cardona-Perez, J.A.; et al. Maternal and Neonatal Morbidity and Mortality Among Pregnant Women with and Without COVID-19 Infection: The INTERCOVID Multinational Cohort Study. JAMA Pediatr. 2021, 175, 817–826. [Google Scholar] [CrossRef]
- Conde-Agudelo, A.; Romero, R. SARS-CoV-2 infection during pregnancy and risk of preeclampsia: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. 2022, 226, 68–89.e3. [Google Scholar] [CrossRef]
- Papageorghiou, A.T.; Deruelle, P.; Gunier, R.B.; Rauch, S.; Garcia-May, P.K.; Mhatre, M.; Usman, M.A.; Abd-Elsalam, S.; Etuk, S.; Simmons, L.E.; et al. Preeclampsia and COVID-19: Results from the INTERCOVID prospective longitudinal study. Am. J. Obstet. Gynecol. 2021, 225, 289.e1–289.e17. [Google Scholar] [CrossRef]
- Englund, J.A. The influence of maternal immunization on infant immune responses. J. Comp. Pathol. 2007, 137 (Suppl. 1), S16–S19. [Google Scholar] [CrossRef]
- Sutton, D.; D’Alton, M.; Zhang, Y.; Kahe, K.; Cepin, A.; Goffman, D.; Staniczenko, A.; Yates, H.; Bugansky, A.; Coletta, J.; et al. COVID-19 vaccine acceptance among pregnant, breastfeeding, and nonpregnant reproductive-aged women. Am. J. Obstet. Gynecol. MFM 2021, 3, 100403. [Google Scholar] [CrossRef]
- Goncu Ayhan, S.; Oluklu, D.; Atalay, A.; Menekse Beser, D.; Tanacan, A.; Moraloglu Tekin, O.; Sahin, D. COVID-19 vaccine acceptance in pregnant women. Int. J. Gynaecol. Obstet. 2021, 154, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Skjefte, M.; Ngirbabul, M.; Akeju, O.; Escudero, D.; Hernandez-Diaz, S.; Wyszynski, D.F.; Wu, J.W. COVID-19 vaccine acceptance among pregnant women and mothers of young children: Results of a survey in 16 countries. Eur. J. Epidemiol. 2021, 36, 197–211. [Google Scholar] [CrossRef]
- Tao, L.; Wang, R.; Han, N.; Liu, J.; Yuan, C.; Deng, L.; Han, C.; Sun, F.; Liu, M.; Liu, J. Acceptance of a COVID-19 vaccine and associated factors among pregnant women in China: A multi-center cross-sectional study based on health belief model. Hum. Vaccines Immunother. 2021, 17, 2378–2388. [Google Scholar] [CrossRef] [PubMed]
- Young, B.E.; Seppo, A.E.; Diaz, N.; Rosen-Carole, C.; Nowak-Wegrzyn, A.; Cruz Vasquez, J.M.; Ferri-Huerta, R.; Nguyen-Contant, P.; Fitzgerald, T.; Sangster, M.Y.; et al. Association of Human Milk Antibody Induction, Persistence, and Neutralizing Capacity With SARS-CoV-2 Infection vs mRNA Vaccination. JAMA Pediatr. 2022, 176, 159–168. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Kadali, R.A.K.; Janagama, R.; Peruru, S.R.; Racherla, S.; Tirumala, R.; Madathala, R.R.; Gajula, V. Adverse effects of COVID-19 messenger RNA vaccines among pregnant women: A cross-sectional study on healthcare workers with detailed self-reported symptoms. Am. J. Obstet. Gynecol. 2021, 225, 458–460. [Google Scholar] [CrossRef]
- Lechosa-Muniz, C.; Paz-Zulueta, M.; Mendez-Legaza, J.M.; Irure-Ventura, J.; Cuesta Gonzalez, R.; Calvo Montes, J.; López-Hoyos, M.; Llorca, J.; Cabero-Pérez, M.J. Induction of SARS-CoV-2-Specific IgG and IgA in Serum and Milk with Different SARS-CoV-2 Vaccines in Breastfeeding Women: A Cross-Sectional Study in Northern Spain. Int. J. Environ. Res. Public Health 2021, 18, 8831. [Google Scholar] [CrossRef]
- McLaurin-Jiang, S.; Garner, C.D.; Krutsch, K.; Hale, T.W. Maternal and Child Symptoms Following COVID-19 Vaccination Among Breastfeeding Mothers. Breastfeed Med. 2021, 16, 702–709. [Google Scholar] [CrossRef]
- Shanes, E.D.; Otero, S.; Mithal, L.B.; Mupanomunda, C.A.; Miller, E.S.; Goldstein, J.A. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Vaccination in Pregnancy: Measures of Immunity and Placental Histopathology. Obstet. Gynecol. 2021, 138, 281–283. [Google Scholar] [CrossRef]
- Theiler, R.N.; Wick, M.; Mehta, R.; Weaver, A.L.; Virk, A.; Swift, M. Pregnancy and birth outcomes after SARS-CoV-2 vaccination in pregnancy. Am. J. Obstet. Gynecol. MFM 2021, 3, 100467. [Google Scholar] [CrossRef]
- Abbott, D.S.; Radford, S.K.; Seed, P.T.; Tribe, R.M.; Shennan, A.H. Evaluation of a quantitative fetal fibronectin test for spontaneous preterm birth in symptomatic women. Am. J. Obstet. Gynecol. 2013, 208, 122.e1–122.e6. [Google Scholar] [CrossRef] [PubMed]
- Selma-Royo, M.; Bauerl, C.; Mena-Tudela, D.; Aguilar-Camprubi, L.; Perez-Cano, F.J.; Parra-Llorca, A.; Lerin, C.; Martínez-Costa, C.; Collado, M.C. Anti-SARS-CoV-2 IgA and IgG in human milk after vaccination is dependent on vaccine type and previous SARS-CoV-2 exposure: A longitudinal study. Genome Med. 2022, 14, 42. [Google Scholar] [CrossRef]
- Martínez-Varea, A.; Satorres, E.; Florez, S.; Domenech, J.; Desco-Blay, J.; Monfort-Pitarch, S.; Hueso, M.; Perales-Marín, A.; Diago-Almela, V. Comparison of Maternal–Fetal Outcomes among Unvaccinated and Vaccinated Pregnant Women with COVID-19. J. Pers. Med. 2022, 12, 2008. [Google Scholar] [CrossRef] [PubMed]
- Calil, V.; Palmeira, P.; Zheng, Y.; Krebs, V.L.J.; Carvalho, W.B.; Carneiro-Sampaio, M. CoronaVac can induce the production of anti-SARS-CoV-2 IgA antibodies in human milk. Clinics 2021, 76, e3185. [Google Scholar] [CrossRef] [PubMed]
- Atyeo, C.; DeRiso, E.A.; Davis, C.; Bordt, E.A.; De Guzman, R.M.; Shook, L.L.; Yonker, L.M.; Fasano, A.; Akinwunmi, B.; Lauffenburger, D.A.; et al. COVID-19 mRNA vaccines drive differential antibody Fc-functional profiles in pregnant, lactating, and nonpregnant women. Sci. Transl. Med. 2021, 13, eabi8631. [Google Scholar] [CrossRef] [PubMed]
- Bertrand, K.; Honerkamp-Smith, G.; Chambers, C.D. Maternal and Child Outcomes Reported by Breastfeeding Women Following Messenger RNA COVID-19 Vaccination. Breastfeed Med. 2021, 16, 697–701. [Google Scholar] [CrossRef]
- Charepe, N.; Gonçalves, J.; Juliano, A.M.; Lopes, D.G.; Canhão, H.; Soares, H.; Serrano, E.F. COVID-19 mRNA vaccine and antibody response in lactating women: A prospective cohort study. BMC Pregnancy Childbirth 2021, 21, 632. [Google Scholar] [CrossRef]
- Collier, A.Y.; McMahan, K.; Yu, J.; Tostanoski, L.H.; Aguayo, R.; Ansel, J.; Chandrashekar, A.; Patel, S.; Bondzie, E.A.; Sellers, D.; et al. Immunogenicity of COVID-19 mRNA Vaccines in Pregnant and Lactating Women. JAMA 2021, 325, 2370–2380. [Google Scholar] [CrossRef]
- Esteve-Palau, E.; Gonzalez-Cuevas, A.; Guerrero, M.E.; Garcia-Terol, C.; Alvarez, M.C.; Casadevall, D.; Diaz-Brito, V. Quantification of Specific Antibodies Against SARS-CoV-2 in Breast Milk of Lactating Women Vaccinated With an mRNA Vaccine. JAMA Netw. Open 2021, 4, e2120575. [Google Scholar] [CrossRef]
- Rosenberg-Friedman, M.; Kigel, A.; Bahar, Y.; Werbner, M.; Alter, J.; Yogev, Y.; Dror, Y.; Lubetzky, R.; Dessau, M.; Gal-Tanamy, M.; et al. BNT162b2 mRNA vaccine elicited antibody response in blood and milk of breastfeeding women. Nat. Commun. 2021, 12, 6222. [Google Scholar] [CrossRef]
- Golan, Y.; Prahl, M.; Cassidy, A.G.; Gay, C.; Wu, A.H.B.; Jigmeddagva, U.; Lin, C.Y.; Gonzalez, V.J.; Basilio, E.; Chidboy, M.A.; et al. COVID-19 mRNA Vaccination in Lactation: Assessment of Adverse Events and Vaccine Related Antibodies in Mother-Infant Dyads. Front. Immunol. 2021, 12, 777103. [Google Scholar] [CrossRef] [PubMed]
- Goncalves, J.; Juliano, A.M.; Charepe, N.; Alenquer, M.; Athayde, D.; Ferreira, F.; Archer, M.; Amorim, M.J.; Serrano, F.; Soares, H. Secretory IgA and T cells targeting SARS-CoV-2 spike protein are transferred to the breastmilk upon mRNA vaccination. Cell Rep. Med. 2021, 2, 100468. [Google Scholar] [CrossRef] [PubMed]
- Gray, K.J.; Bordt, E.A.; Atyeo, C.; Deriso, E.; Akinwunmi, B.; Young, N.; Baez, A.M.; Shook, L.L.; Cvrk, D.; James, K.; et al. Coronavirus disease 2019 vaccine response in pregnant and lactating women: A cohort study. Am. J. Obstet. Gynecol. 2021, 225, 303.e1–303.e17. [Google Scholar] [CrossRef] [PubMed]
- Guida, M.; Terracciano, D.; Cennamo, M.; Aiello, F.; La Civita, E.; Esposito, G.; Gargiulo, V.; Maruotti, G.; Portella, G.; Sarno, L. COVID-19 Vaccine mRNABNT162b2 Elicits Human Antibody Response in Milk of Breastfeeding Women. Vaccines 2021, 9, 785. [Google Scholar] [CrossRef] [PubMed]
- Jakuszko, K.; Kościelska-Kasprzak, K.; Żabińska, M.; Bartoszek, D.; Poznański, P.; Rukasz, D.; Kłak, R.; Królak-Olejnik, B.; Krajewska, M. Immune Response to Vaccination against COVID-19 in Breastfeeding Health Workers. Vaccines 2021, 9, 663. [Google Scholar] [CrossRef] [PubMed]
- Juncker, H.G.; Mulleners, S.J.; van Gils, M.J.; de Groot, C.J.M.; Pajkrt, D.; Korosi, A.; van Goudoever, J.B.; van Keulen, B.J. The Levels of SARS-CoV-2 Specific Antibodies in Human Milk Following Vaccination. J. Hum. Lact. 2021, 37, 477–484. [Google Scholar] [CrossRef] [PubMed]
- Kachikis, A.; Englund, J.A.; Singleton, M.; Covelli, I.; Drake, A.L.; Eckert, L.O. Short-term Reactions Among Pregnant and Lactating Individuals in the First Wave of the COVID-19 Vaccine Rollout. JAMA Netw. Open 2021, 4, e2121310. [Google Scholar] [CrossRef] [PubMed]
- Low, J.M.; Gu, Y.; Ng, M.S.F.; Amin, Z.; Lee, L.Y.; Ng, Y.P.M.; Shunmuganathan, B.D.; Niu, Y.; Gupta, R.; Tambyah, P.A.; et al. Codominant IgG and IgA expression with minimal vaccine mRNA in milk of BNT162b2 vaccinees. NPJ Vaccines 2021, 6, 105. [Google Scholar] [CrossRef]
- Mithal, L.B.; Otero, S.; Shanes, E.D.; Goldstein, J.A.; Miller, E.S. Cord blood antibodies following maternal coronavirus disease 2019 vaccination during pregnancy. Am. J. Obstet. Gynecol. 2021, 225, 192–194. [Google Scholar] [CrossRef]
- Montalti, M.; Guaraldi, F.; Di Valerio, Z.; Ragghianti, B.; Tedesco, D.; Mannucci, E.; Monami, M.; Gori, D. Adherence to and early adverse events of COVID-19 vaccine in a cohort of 600 Italian breastfeeding and pregnant physicians. Hum. Vaccines Immunother. 2022, 18, 2106747. [Google Scholar] [CrossRef]
- Olearo, F.; Radmanesh, L.S.; Felber, N.; von Possel, R.; Emmerich, P.; Pekarek, N.; Pfefferle, S.; Nörz, D.; Hansen, G.; Diemert, A.; et al. Anti-SARS-CoV-2 antibodies in breast milk during lactation after infection or vaccination: A cohort study. J. Reprod. Immunol. 2022, 153, 103685. [Google Scholar] [CrossRef] [PubMed]
- Perez, S.E.; Luna Centeno, L.D.; Cheng, W.A.; Marentes Ruiz, C.J.; Lee, Y.; Congrave-Wilson, Z.; Powell, R.L.; Stellwagen, L.; Pannaraj, P.S. Human Milk SARS-CoV-2 Antibodies up to 6 Months After Vaccination. Pediatrics 2022, 149, e2021054260. [Google Scholar] [CrossRef]
- Perl, S.H.; Uzan-Yulzari, A.; Klainer, H.; Asiskovich, L.; Youngster, M.; Rinott, E.; Youngster, I. SARS-CoV-2-Specific Antibodies in Breast Milk After COVID-19 Vaccination of Breastfeeding Women. JAMA 2021, 325, 2013–2014. [Google Scholar] [CrossRef] [PubMed]
- Pietrasanta, C.; Darwich, A.; Ronchi, A.; Crippa, B.; Spada, E.; Mosca, F.; Pugni, L.; Rescigno, M. Humoral response to anti-SARS-CoV-2 vaccine in breastfeeding mothers and mother-to-infant antibody transfer through breast milk. NPJ Vaccines 2022, 7, 63. [Google Scholar] [CrossRef] [PubMed]
- Prabhu, M.; Murphy, E.A.; Sukhu, A.C.; Yee, J.; Singh, S.; Eng, D.; Zhao, Z.; Riley, L.E.; Yang, Y.J. Antibody Response to Coronavirus Disease 2019 (COVID-19) Messenger RNA Vaccination in Pregnant Women and Transplacental Passage into Cord Blood. Obstet. Gynecol. 2021, 138, 278–280. [Google Scholar] [CrossRef] [PubMed]
- Rottenstreich, A.; Zarbiv, G.; Oiknine-Djian, E.; Zigron, R.; Wolf, D.G.; Porat, S. Efficient Maternofetal Transplacental Transfer of Anti- Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Spike Antibodies After Antenatal SARS-CoV-2 BNT162b2 Messenger RNA Vaccination. Clin. Infect. Dis. 2021, 73, 1909–1912. [Google Scholar] [CrossRef]
- Scrimin, F.; Campisciano, G.; Comar, M.; Ragazzon, C.; Davanzo, R.; Quadrifoglio, M.; Giangreco, M.; Stabile, G.; Ricci, G. IgG and IgA Antibodies Post SARS-CoV-2 Vaccine in the Breast Milk and Sera of Breastfeeding Women. Vaccines 2022, 10, 125. [Google Scholar] [CrossRef]
- Shimabukuro, T.T.; Kim, S.Y.; Myers, T.R.; Moro, P.L.; Oduyebo, T.; Panagiotakopoulos, L.; Marquez, P.L.; Olson, C.K.; Liu, R.; Chang, K.T.; et al. Preliminary Findings of mRNA COVID-19 Vaccine Safety in Pregnant Persons. N. Engl. J. Med. 2021, 384, 2273–2282. [Google Scholar] [CrossRef]
- Stuckelberger, S.; Favre, G.; Ceulemans, M.; Gerbier, E.; Lambelet, V.; Stojanov, M.; Winterfeld, U.; Baud, D.; Panchaud, A.; Pomar, L. Current Data on COVID-19 mRNA-Vaccine Safety during Pregnancy Might Be Subject to Selection Bias. Reply to Stroobandt, S.; Stroobandt, R. Data of the COVID-19 mRNA-Vaccine V-Safe Surveillance System and Pregnancy Registry Reveals Poor Embryonic and Second Trimester Fetal Survival Rate. Comment on “Stuckelberger et al. SARS-CoV-2 Vaccine Willingness among Pregnant and Breastfeeding Women during the First Pandemic Wave: A Cross-Sectional Study in Switzerland. Viruses 2021, 13, 1199”. Viruses 2021, 13, 1546. [Google Scholar]
- Fu, W.; Sivajohan, B.; McClymont, E.; Albert, A.; Elwood, C.; Ogilvie, G.; Money, D. Systematic review of the safety, immunogenicity, and effectiveness of COVID-19 vaccines in pregnant and lactating individuals and their infants. Int. J. Gynaecol. Obstet. 2022, 156, 406–417. [Google Scholar] [CrossRef]
- Zhu, F.; Zozaya, C.; Zhou, Q.; De Castro, C.; Shah, P.S. SARS-CoV-2 genome and antibodies in breastmilk: A systematic review and meta-analysis. Arch. Dis. Child. Fetal Neonatal Ed. 2021, 106, 514–521. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Novillo, B.; Martínez-Varea, A. COVID-19 Vaccines during Pregnancy and Breastfeeding: A Systematic Review. J. Pers. Med. 2023, 13, 40. https://doi.org/10.3390/jpm13010040
Novillo B, Martínez-Varea A. COVID-19 Vaccines during Pregnancy and Breastfeeding: A Systematic Review. Journal of Personalized Medicine. 2023; 13(1):40. https://doi.org/10.3390/jpm13010040
Chicago/Turabian StyleNovillo, Blanca, and Alicia Martínez-Varea. 2023. "COVID-19 Vaccines during Pregnancy and Breastfeeding: A Systematic Review" Journal of Personalized Medicine 13, no. 1: 40. https://doi.org/10.3390/jpm13010040
APA StyleNovillo, B., & Martínez-Varea, A. (2023). COVID-19 Vaccines during Pregnancy and Breastfeeding: A Systematic Review. Journal of Personalized Medicine, 13(1), 40. https://doi.org/10.3390/jpm13010040