
Medical and Surgical Strategies in Vulvar Paget Disease: Let’s Throw Some Light!

 ,
, 
 ,
,
Abstract
1. Introduction
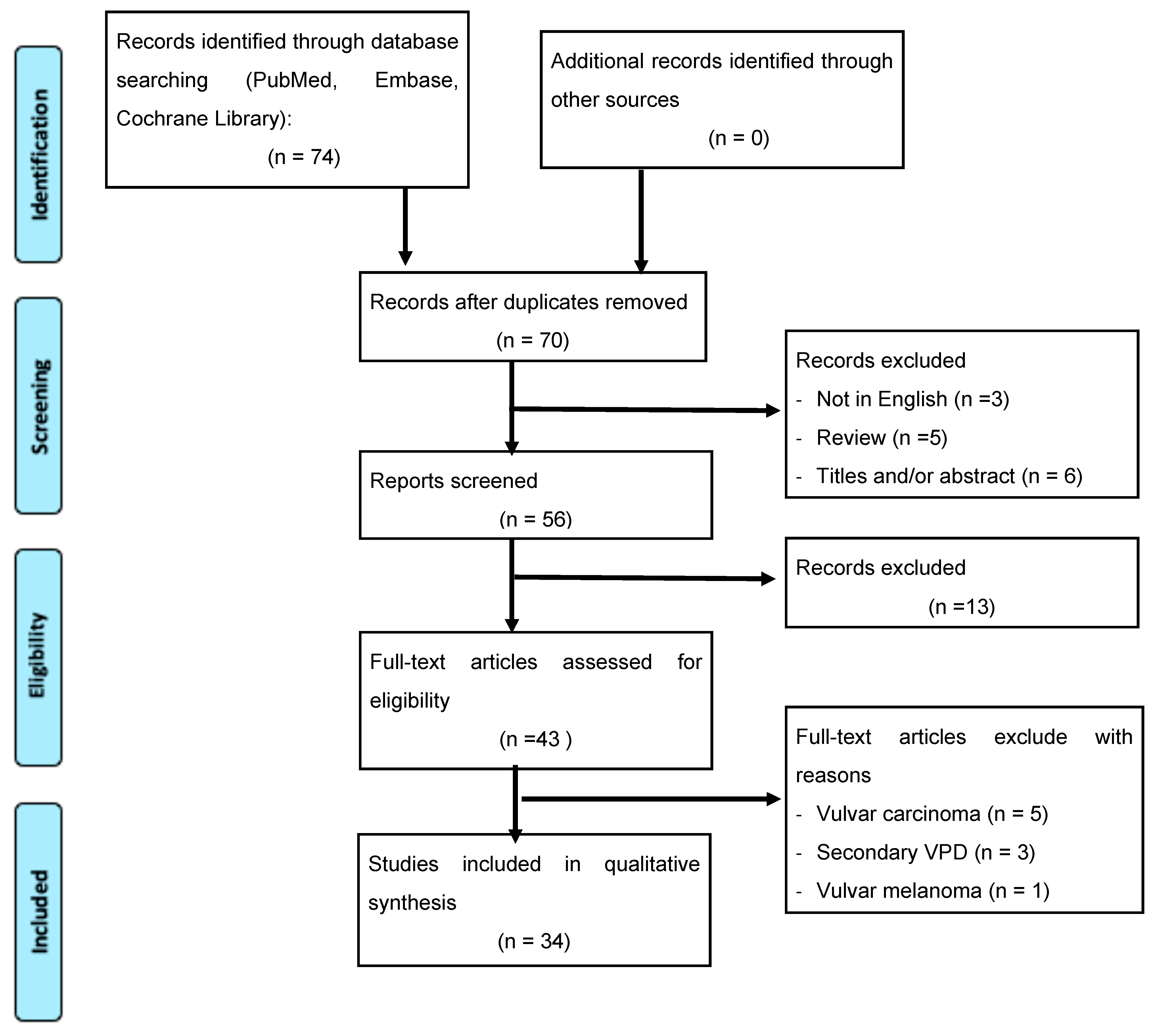
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Delport, E.S. Extramammary Paget’s disease of the vulva: An annotated review of the current literature. Australas. J. Dermatol. 2013, 54, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, J.; Flanagan, A. Mammary and extramammary Paget’s disease. J. Clin. Pathol. 2000, 53, 742–749. [Google Scholar] [CrossRef] [PubMed]
- Lam, C.; Funaro, D. Extramammary Paget’s disease: Summary of current knowledge. Dermatol. Clin. 2010, 28, 807–826. [Google Scholar] [CrossRef]
- Terlou, A.; Blok, L.J.; Helmerhorst, T.J.; van Beurden, M. Premalignant epithelial disorders of the vulva: Squamous vulvar intraepithelial neoplasia, vulvar Paget’s disease and melanoma in situ. Acta Obstet. Gynecol. Scand. 2010, 89, 741–748. [Google Scholar] [CrossRef] [PubMed]
- Noel, A.; Bhat, R.M.; Rao, S.V.; Fernandes, S. An unusual secondary extramammary Paget’s disease of vulva. Indian J. Sex. Transm. Dis. AIDS 2020, 41, 210–212. [Google Scholar] [CrossRef] [PubMed]
- Van der Linden, M.; Meeuwis, K.A.; Bulten, J.; Bosse, T.; van Poelgeest, M.I.; de Hullu, J.A. Paget disease of the vulva. Crit. Rev. Oncol. Hematol. 2016, 101, 60–74. [Google Scholar] [CrossRef]
- McDaniel, B.; Brown, F.; Crane, J.S. Extramammary Paget Disease; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- St Claire, K.; Hoover, A.; Ashack, K.; Khachemoune, A. Extramammary Paget disease. Dermatol Online J. 2019, 25, 1. [Google Scholar] [CrossRef]
- Konstantinova, A.M.; Kazakov, D.V. Extramammary Paget disease of the vulva. Semin. Diagn. Pathol. 2021, 38, 50687. [Google Scholar] [CrossRef]
- Garganese, G.; Anchora, L.P.; Fragomeni, S.M.; Mantovani, G.; Santoro, A.; Gentileschi, S.; Corrado, G.; Lombisani, A.; Lancellotta, V.; Tagliaferri, L.; et al. “Clock mapping” prior to excisional surgery in vulvar Paget’s disease: Tailoring the surgical plan. Arch. Gynecol. Obstet. 2022, 306, 473–480. [Google Scholar] [CrossRef]
- Wang, L.C.; Blanchard, A.; Judge, D.E.; Lorincz, A.A.; Medenica, M.M.; Busbey, S. Successful treatment of recurrent extramammary Paget’s disease of the vulva with topical imiquimod 5% cream. J. Am. Acad. Dermatol. 2003, 49, 769–772. [Google Scholar] [CrossRef]
- Ho, S.A.; Aw, D.C. Extramammary Paget’s disease treated with topical imiquimod 5% cream. Dermatol. Ther. 2010, 23, 423–427. [Google Scholar] [CrossRef]
- Tonguc, E.; Güngor, T.; Var, T.; Ozat, M.; Sahin, I.; Sirvan, L. Treatment of recurrent vulvar Paget disease with imiquimod cream: A case report and review of the literature. Arch. Gynecol. Obstet. 2011, 283, 97–101. [Google Scholar] [CrossRef]
- Feldmeyer, L.; Kerl, K.; Kamarashev, J.; de Viragh, P.; French, L.E. Treatment of vulvar Paget disease with topical imiquimod: A case report and review of the literature. J. Dermatol. Case Rep. 2011, 5, 42–46. [Google Scholar] [CrossRef]
- Anton, C.; Luiz, A.V.; Carvalho, F.M.; Baracat, E.C.; Carvalho, J.P. Clinical treatment of vulvar Paget’s disease: A case report. Clinics 2011, 66, 1109–1111. [Google Scholar] [CrossRef] [PubMed]
- Dogan, A.; Hilal, Z.; Krentel, H.; Cetin, C.; Hefler, L.A.; Grimm, C.; Tempfer, C.B. Paget’s Disease of the Vulva Treated with Imiquimod: Case Report and Systematic Review of the Literature. Gynecol. Obstet. Investig. 2017, 82, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Vicentini, C.; Carpentier, O.; Lecomte, F.; Thecua, E.; Mortier, L.; Mordon, S.R. Treatment of a vulvar Paget’s disease by photodynamic therapy with a new light emitting fabric based device. Lasers Surg. Med. 2017, 49, 177–180. [Google Scholar] [CrossRef]
- Johnson, J.; O’Laughlin, D. Paget disease of the vulva. JAAPA 2019, 32, 33–34. [Google Scholar] [CrossRef]
- Bouceiro-Mendes, R.; Mendonça-Sanches, M.; Soares-de-Almeida, L.; Correia-Fonseca, I. A Case of Chronic and Relapsing Paget Disease of the Vulva. Rev. Bras. Ginecol. Obstet. 2019, 41, 412–416. [Google Scholar] [CrossRef] [PubMed]
- Bajracharya, A.; Shrestha, S.; Singh, M.; Shrestha, S.; Lama, S.; Singh, J. Vulvar Paget’s disease associated with squamous cell carcinoma: A case report. Ann. Med. Surg. 2022, 74, 103320. [Google Scholar] [CrossRef] [PubMed]
- Hatch, K.D.; Davis, J.R. Complete resolution of Paget disease of the vulva with imiquimod cream. J. Low Genit. Tract. Dis. 2008, 12, 90–94. [Google Scholar] [CrossRef] [PubMed]
- Challenor, R.; Hughes, G.; Fitton, A.R. Multidisciplinary treatment of vulval extramammary Paget’s disease to maintain sexual function: An imiquimod success story. J. Obstet. Gynaecol. 2009, 29, 252–254. [Google Scholar] [CrossRef] [PubMed]
- Sendagorta, E.; Herranz, P.; Feito, M.; Ramírez, P.; Floristán, U.; Feltes, R.; Benito, D.M.; Casado, M. Successful treatment of three cases of primary extramammary Paget’s disease of the vulva with Imiquimod--proposal of a therapeutic schedule. J. Eur. Acad. Dermatol. Venereol. 2010, 24, 490–492. [Google Scholar] [CrossRef] [PubMed]
- Baiocchi, G.; Begnami, M.D.; Fukazawa, E.M.; Surima, W.S.; Badiglian-Filho, L.; Costa, F.D.; Oliveira, R.A.; Faloppa, C.C.; Kumagai, L.Y.; Soares, F.A. Conservative management of extramammary paget disease with imiquimod. J. Low Genit. Tract. Dis. 2012, 16, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.H.; Jue, M.S.; Kim, E.J.; Joh, O.J.; Song, K.Y.; Park, H.J. Extramammary paget disease: Minimal surgical therapy. Ann. Dermatol. 2013, 25, 213–217. [Google Scholar] [CrossRef]
- Sanderson, P.; Innamaa, A.; Palmer, J.; Tidy, J. Imiquimod therapy for extramammary Paget’s disease of the vulva: A viable non-surgical alternative. J. Obstet. Gynaecol. 2013, 33, 479–483. [Google Scholar] [CrossRef]
- Marchitelli, C.; Peremateu, M.S.; Sluga, M.C.; Berasategui, M.T.; Lopez, D.G.; Wernicke, A.; Velazco, A.; Gogorza, S. Treatment of primary vulvar paget disease with 5% imiquimod cream. J. Low Genit. Tract. Dis. 2014, 18, 347–350. [Google Scholar] [CrossRef]
- Nagai, Y.; Kazama, S.; Yamada, D.; Miyagawa, T.; Murono, K.; Yasuda, K.; Nishikawa, T.; Tanaka, T.; Kiyomatsu, T.; Hata, K.; et al. Perianal and Vulvar Extramammary Paget Disease: A Report of Six Cases and Mapping Biopsy of the Anal Canal. Ann. Dermatol. 2016, 28, 624–628. [Google Scholar] [CrossRef]
- Nitecki, R.; Davis, M.; Watkins, J.C.; Wu, Y.E.; Vitonis, A.F.; Muto, M.G.; Berkowitz, R.S.; Horowitz, N.S.; Feltmate, C.M. Extramammary Paget Disease of the Vulva: A Case Series Examining Treatment, Recurrence, and Malignant Transformation. Int. J. Gynecol. Cancer 2018, 28, 632–638. [Google Scholar] [CrossRef]
- Kosmidis, C.S.; Sevva, C.; Roulia, P.; Koulouris, C.; Varsamis, N.; Koimtzis, G.; Theodorou, V.; Mystakidou, C.M.; Georgakoudi, E.; Anthimidis, G. Extramammary Paget’s Disease of the Vulva: Report of Two Cases. Medicina 2021, 57, 1029. [Google Scholar] [CrossRef]
- Cai, Y.; Sheng, W.; Xiang, L.; Wu, X.; Yang, H. Primary extramammary Paget’s disease of the vulva: The clinicopathological features and treatment outcomes in a series of 43 patients. Gynecol. Oncol. 2013, 129, 412–416. [Google Scholar] [CrossRef]
- De Magnis, A.; Checcucci, V.; Catalano, C.; Corazzesi, A.; Pieralli, A.; Taddei, G.; Fambrini, M. Vulvar paget disease: A large single-centre experience on clinical presentation, surgical treatment, and long-term outcomes. J. Low Genit. Tract. Dis. 2013, 17, 104–110. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.; Yuan, B.; Wang, Y.; Xue, F. Clinicopathologic study of vulvar Paget’s disease in China. J. Low Genit. Tract. Dis. 2014, 18, 281–284. [Google Scholar] [CrossRef]
- Sopracordevole, F.; Di Giuseppe, J.; De Piero, G.; Canzonieri, V.; Buttignol, M.; Giorda, G.; Ciavattini, A. Surgical Treatment of Paget Disease of the Vulva: Prognostic Significance of Stromal Invasion and Surgical Margin Status. J. Low Genit. Tract. Dis. 2016, 20, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Onaiwu, C.O.; Salcedo, M.P.; Pessini, S.A.; Munsell, M.F.; Euscher, E.E.; Reed, K.E.; Schmeler, K.M. Paget’s disease of the vulva: A review of 89 cases. Gynecol. Oncol. Rep. 2016, 19, 46–49. [Google Scholar] [CrossRef] [PubMed]
- Nasioudis, D.; Bhadra, M.; Ko, E.M. Extramammary Paget disease of the vulva: Management and prognosis. Gynecol. Oncol. 2020, 157, 146–150. [Google Scholar] [CrossRef] [PubMed]
- Loiacono, R.M.R.; Traversi, P.; Deliso, M.A.; Gargano, G.; Kardhashi, A.; Francescato, R.; Loizzi, V.; Spinelli, M.; Lovascio, S.; Fiorito, M.; et al. Paget disease of the vulva an analysis of 24 cases. Medicine 2019, 98, e17018. [Google Scholar] [CrossRef]
- Preti, M.; Micheletti, L.; Borella, F.; Cosma, S.; Marrazzu, A.; Gallio, N.; Privitera, S.; Tancredi, A.; Bevilacqua, F.; Benedetto, C. Vulvar Paget’s disease and stromal invasion: Clinico-pathological features and survival outcomes. Surg. Oncol. 2021, 38, 101581. [Google Scholar] [CrossRef]
- Borella, F.; Preti, M.; Vieira-Baptista, P.; Pérez-López, F.R.; Bertero, L.; Gallio, N.; Micheletti, L.; Benedetto, C. Vulvar Paget’s disease: Outcomes of 51 patients treated with imiquimod cream. Maturitas 2022, 163, 23–27. [Google Scholar] [CrossRef]
- Luyten, A.; Sörgel, P.; Clad, A.; Gieseking, F.; Maass-Poppenhusen, K.; Lellé, R.J.; Harter, P.; Buttmann, N.; Petry, K.U. Treatment of extramammary Paget disease of the vulva with imiquimod: A retrospective, multicenter study by the German Colposcopy Network. J. Am. Acad. Dermatol. 2014, 70, 644–650. [Google Scholar] [CrossRef]
- Rioli, D.I.; Samimi, M.; Beneton, N.; Hainaut, E.; Martin, L.; Misery, L.; Quereux, G. Efficacy and tolerance of photodynamic therapy for vulvar Paget’s disease: A multicentric retrospective study. Eur. J. Dermatol. 2018, 28, 351–355. [Google Scholar] [CrossRef]
- Cowan, R.A.; Black, D.R.; Hoang, L.N.; Park, K.J.; Soslow, R.A.; Backes, F.J.; Gardner, G.J.; Abu-Rustum, N.R.; Leitao, M.M., Jr.; Eisenhauer, E.L.; et al. A pilot study of topical imiquimod therapy for the treatment of recurrent extramammary Paget’s disease. Gynecol. Oncol. 2016, 142, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Van der Linden, M.; Van Hees, C.L.; Van Beurden, M.; Bulten, J.; van Dorst, E.B.; Esajas, M.D.; Meeuwis, K.A.; Boll, D.; van Poelgeest, M.I.; de Hullu, J.A. The Paget Trial: Topical 5% imiquimod cream for noninvasive vulvar Paget disease. Am. J. Obstet. Gynecol. 2022, 227, 250.e1–250.e8. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, F.; Bardazzi, F.; Messori, S.; Abbenante, D.; Barisani, A.; Vaccari, S. Photodynamic therapy following fractional CO2 laser for treatment of primary vulvar Paget’s disease: Does it really work? J. Dermatolog. Treat. 2021, 32, 800–802. [Google Scholar] [CrossRef] [PubMed]
- Asel, M.; LeBoeuf, N.R. Extramammary Paget’s Disease. Hematol. Oncol. Clin. N. Am. 2019, 33, 73–85. [Google Scholar] [CrossRef] [PubMed]
- Tolia, M.; Tsoukalas, N.; Sofoudis, C.; Giaginis, C.; Spyropoulou, D.; Kardamakis, D.; Kouloulias, V.; Kyrgias, G. Primary extramammary invasive Paget’s vulvar disease: What is the standard, what are the challenges and what is the future for radiotherapy? BMC Cancer 2016, 16, 563. [Google Scholar] [CrossRef]
- Machida, H.; Moeini, A.; Roman, L.D.; Matsuo, K. Effects of imiquimod on vulvar Paget’s disease: A systematic review of literature. Gynecol. Oncol. 2015, 139, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Fontanelli, R.; Papadia, A.; Martinelli, F.; Lorusso, D.; Grijuela, B.; Merola, M.; Solima, E.; Ditto, A.; Raspagliesi, F. Photodynamic therapy with M-ALA as non surgical treatment option in patients with primary extramammary Paget’s disease. Gynecol. Oncol. 2013, 130, 90–94. [Google Scholar] [CrossRef]
- Hanna, E.; Abadi, R.; Abbas, O. Imiquimod in dermatology: An overview. Int. J. Dermatol. 2016, 55, 831–844. [Google Scholar] [CrossRef]
- Ewing, T.L. Paget’s disease of the vulva treated by combined surgery and laser. Gynecol. Oncol. 1991, 43, 137–140. [Google Scholar] [CrossRef]
- Kato, T.; Fujimoto, N.; Fujii, N.; Tanaka, T. Mapping biopsy with punch biopsies to determine surgical margin in extramammary Paget’s disease. J. Dermatol. 2013, 40, 968–972. [Google Scholar] [CrossRef]
- Iavazzo, C.; Gkegkes, I.; Fotiou, A. Vulvar’s Paget’s disease treated with a combination of clock mapping and imiquimod. Arch. Gynecol. Obstet. 2022. [Google Scholar] [CrossRef] [PubMed]
- Ishizuki, S.; Nakamura, Y. Extramammary Paget’s Disease: Diagnosis, Pathogenesis, and Treatment with Focus on Recent Developments. Curr. Oncol. 2021, 28, 2969–2986. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors | Country | Type of Study | Sample Size, n (Case/Control) | Inclusion Criteria | Age (Years) | Other Neoplasm | Disease STATUS | Symptoms (n–%) | Vulvar Lesion (Before Treatment) | Previous Vulvar Surgery/Medical Therapy n (%) |
|---|---|---|---|---|---|---|---|---|---|---|
| Hatch et al. (2008) [21] | USA | Case series | 2 | NA | 68 60 | None | 2 (100%) Relapse | Pain (2–100%) Urinary retention (1–50%) | Erythema | 1 (50%) Local resection 1 (50%) Radical vulvectomy |
| Challenor et al. (2009) [22] | UK | Case series | 2 | NA | 48 66 | None | 2 (100%) Primary | Itching (2–100%) Soreness (1–50%) | erythema | NR |
| Sendagorta et al. (2010) [23] | Spain | Case series | 3 | NA | 66 58 82 | None | 3 (100%) Primary | Pruritis (2–66.6%) Burning (1–33.3%) | Lichenified plaque (1–33.3 %) Erythematous plaque (2–66.6%) Erosions (1–33.3%) | NR |
| Baiocchi et al. (2012) [24] | Brazil | Case series | 4 | NA | 62.2 (56–80) | None | 2 (50%) Primary 2 (50%) Relapse | (4–100%) Pruritis | (4–100%) Erythematous plaque (1–25%) Erosions | (4–100%) Topical antifungals/steroids (1–25%) Simple vulvectomy (1–25%) Wide vulvar resection (1–25%) PDT |
| Choi et al. (2013) [25] | Korea | Case series | 3 |
| 73 (65–81) | NR | 3 (100%) Primary | NR | Erythema | treatment |
| Sanderson et al. (2013) [26] | UK | Case series | 6 |
| 71.5 (58–85) | NR | 5 (83.3%) Primary 1 (16.6%) Relapse | Irritation (1–16,6%) Itching (3–50%) Soreness (3–50%) Inflammation (1–16.6%) Painful (1–16.6%) | Plaque | 2 (33.2%) Topical steroids 1 (16.6%) Skinning posterior vulvectomy with reconstruction |
| Cai et al. (2013) [31] | China | Retrospective | 43 |
| 68.6 (52–85) | NR | 43 (100%) Primary | Pruritis (95.3%) Pain (18.6%) Bleeding (16.3%) Discharge (13.9%) | Erythematous (81.4%) Ulceration (32.6%) Erosion (30.2%) Median size 4.8 cm2 (1–10 cm2) | (26–61.9%) Topical antifungals/ steroids |
| De Magnis et al. (2013) [32] | Italy | Retrospective | 34 |
| 68.7 | 5 (14,7%) Breast cancer 2 (5.8%) Vulvar ADC 1 (2.9%) Bladder cancer 1 (2.9%) Lung cancer 1 (2.9%) Basal cell carcinoma 1 (2.9%) Cutaneous Melanoma 1 (2.9%) Vaginal SCC | 34 (100%) Primary | Itching (76.5%) Burning (58.8%) | NR | NR |
| Luyten et al. (2014) [40] | Germany | Retrospective Multicenter | 20 |
| 66.4 (41–84) | 2 (10%) Breast cancers 1 (5%) Malignant tumor of the vulva (Adc, other) | 6 (30%) Primary 14 (70%) Relapse | NR | NR | 7 (33.3%) Unspecified surgery 3 (14.2%) Laser vaporization 1 (4.7%) Photodynamic therapy |
| Marchitelli et al. (2014) [27] | Argentina | Case series | 10 |
| 71.9 (60–92) | None | 7 (70%) Primary 3 (30%) Relapse | NR | Erythematous plaque | 3 (30%) NR surgery |
| Liu et al. (2014) [33] | China | Retrospective | 85 | NR | 64,4 (33–82) | 2 (3%) Breast cancer 2 (3%) Cervical cancer 1 (1.5%) Vulvar SCC 1 (1.5%) Rectal cancer 1 (1.5%) Meningioma | 85 (100%) Primary | Pruritis (74.1%) Pain (5.9%) Vulvar lesion (20%) | Nonspecific vulvar lesions (17–20%) | NR |
| Cowan et al. (2016) [42] | USA | Prospective Multicenter | 8 |
| 71.5 (47–78) | 1 (12.5%) SCC of the face and neck 2 (25%) basal cell carcinoma 2 (25%) Breast cancer | 8 (100%) Relapse | Pruritis (5–63%) Burning (2–25%) Pain (2–25%) | Erythema (6–75%) | (6–75%) Simple partial vulvectomies (1–12.5%) Multiple vulvectomies + flaps |
| Nagai et al. (2016) [28] | Japan | Case series | 2 |
| 69 81 | NR | 2 (100%) Primary | Itching | Eczema | NR |
| Sopracordevole et al. (2016) [34] | Italy | Retrospective | 27 |
| 66.5 (36–88) | 1 (3.7%) pheochromocytoma 4 (14.8%) breast cancers (bilateral in 2 cases) 1 (3.7%) stomach and colorectal cancer 1 (3.7%) skin carcinoma | 27 (100%) Primary | Itching (64.3%) Burning + Itching (14.3%) Pain (14.3%) Burning (7.2%) | Erythemat (73.7%) Erythema + hyperkeratosis (31.6%) | None |
| Onaiwu et al. (2016) [35] | USA | Retrospective | 89 |
| 67 (32–89) | 13 (14.6%) Breast cancer 7 (7.9%) Vulvar cancer 6 (6.7%) Bladder cancer 5 (5.6%) Colo-rectal cancer 4 (4.5%) Endometrial cancer | NR | Pruritis (43–48.3%) | NR | NR |
| Rioli et al. (2018) [41] | France | Retrospective Multicentric | 13 |
| 70.1 (52–84) | 1 (7.6%) Lung Adc | NR Primary NR Relapse | NR | NR | 10 (76.9%) Topical imiquimod 8 (61.5%) NR Surgery 6 (46.1) Carbon dioxide laser treatment |
| Nitecki et al. (2018) [29] | USA | Case series | 44 |
| 67 (50–92) | 3 (6.8%) Breast cancer 1 (2.2%) Urothelial cancer 1 (2.2%) Lung cancer 2 (4.5%) Cutaneous carcinoma | 44 (100%) Primary | Pain (10–22%) Pruritis (10–22%) Pain + pruritus (6–13%) | NR | NR |
| Nasioudis et al. (2019) [36] | USA | Retrospective | 2602 |
| 72 (31–90) | 960 (36.9%) NR tumor | NR | NR | Median size 3–4 cm2 | NR |
| Loiacono et al. (2019) [37] | Italy | Retrospective | 24 |
| 69.3 (38–84) | 3 (12.5%) Breast cancer 2 (8%) Endometrial Adc 1 (4%) Vulvar SCC 1 (4%) Ovarian cancer 1 (4%) Melanoma 1 (4%) Adc of the ampulla of Vater 1 (4%) Urothelial carcinoma 1 (4%) Myelodysplastic syndrome | NR | Itching (1–4%) Pruritis (1–4%) Itching + burning + pruritis + vulvar lesions (5–21%) Pain + pruritis (3–13%) Unknown (14–58%) | Median size 48.9 cm2 (2.5–143 cm2) | NR |
| Preti et al. (2021) [38] | Italy | Retrospective | 122 |
| 65 (36–92) | NR | 122 (100%) Primary | Itching (59–61%) Burning sensation (18–18%) Itching + Burning (20–21%) | Median size 15 cm2 (10–30 cm2) | NR |
| Kosmidis et al. (2021) [30] | Greece | Case series | 2 | NA | 81 69 | None | 2 (100%) Primary | Pruritis + burning Pruritis + swelling | Erythematous plaque (12.5 × 14.5 cm) Eczematous plaque + erosion (2.4 × 7.8 cm–1 cm × 2 cm) | NR |
| Ferrara et al. (2021) [44] | Italy | Prospective | 10 |
| 79 (67–92) | NR | 7 (70%) Primary 3 (30%) Relapse | NR | NR | 4 (40%) NR surgery |
| Borella et al. (2022) [39] | Italy | Retrospective | 55 |
| 63 (36–92) | NR | 24 (43.6%) Primary 31 (56.3%) Relapse | Itching (29–59%) Burning (15–27%) | Max diameter 60 mm (5–290) | 31 (56%) NR surgery |
| Van der Linden et al. (2022) [43] | The Netherlands | prospective multicentric open-label observational cohort study | 24 |
| 67 (42–84) | NR | 20 (83.3%) Primary 4 (16.6%) Relapse | Itching (20–83.3%) Pain (11–45.8%) Burning sensation (17–70.8%) Strangury (7–29.2%) Dyspareunia (5/13–38.5%) | Erythema (24–100%) Scaling (15–62.5%) Ulceration (6–25%) Median size 16 cm2 (3–130 cm2) | 1 (4.1%) Partial vulvectomy 2 (8.2%) NR surgery 1 (4.1%) Vulvectomy 1 (4.1%) Local excision 1 (4.1%) topical 5% imiquimod cream |
| Authors | Medical Treatment | Type of Medical/Other Treatment | Duration of Therapy (Weeks) | Surgical Treatment | Type of Surgical Treatment n (%) | Dermal Invasion |
|---|---|---|---|---|---|---|
| Hatch et al. (2008) [21] | 2 (100%) | Topical imiquimod cream 3 times a week Topical imiquimod cream 1 times a day Topical imiquimod cream 2 times a day Topical imiquimod cream 1 times a day Topical 5% imiquimod cream 3 times a week + clobetasol, 0.1% cream | 8 w 4 w 2 w 5 w 12 w | None | NA | NR |
| Challenor et al. (2009) [22] | 2 (100%) | Topical imiquimod 5% cream 3 times a week (6 w after surgery) Topical imiquimod 5% cream 3 times a week (8 w after surgery) | 12 w 12 w | 2 (100%) | 1 (50%) Skinning vulvectomy and reconstruction with split skin graft 1 (50%) Skinning vulvectomy with reconstruction by V-Y advancement flaps | NR |
| Sendagorta et al. (2010) [23] | 3 (100%) | Topical imiquimod 5% cream daily Topical 5% imiquimod cream 3 times a week | 3 w 3 w | None | NA | NR |
| Baiocchi et al. (2012) [24] | 4 (100%) | (3–75%) Topical 5% imiquimod cream 3 times a week (1–25%) Topical 5% imiquimod cream 2 times a week (1–25%) External RT(54 Gy) | 31.5 w (4–52) | 1 (25%) | Simple vulvectomy | None |
| Choi et al. (2013) [25] | 3 (100%) | Topical 5% imiquimod cream 3 times a week | 24 w | 3 (100%) | Local wide excision | None |
| Sanderson et al. (2013) [26] | 6 (100%) | (6–100%) Topical 5% imiquimod cream 3 times a week (3–50%) clobetasone/oxytetracycline/nystatin cream | 8–16 w | 1 (16.6%) | Vulvectomy | None |
| Cai et al. (2013) [31] | 14 (32.6%) | 8 (18.6%) Definitive RT at a median dose 60 Gy + CT 2 (cycle) 6 (14%) adjuvant RT | NR | 35 (81.4%) | 17 (48.5%) Radical vulvectomy 8 (22.8%) Simple vulvectomy 10 (28.5%) Wide local excision 5 (14.3%) Inguinal LND | 7 (16.2%) |
| De Magnis et al. (2013) [32] | None | NA | NA | 34 (100%) | 2 (5.9%) Radical vulvectomy1 1 (2.9%) Total simple vulvectomy 10 (29.4%) Partial simple vulvectomy 21 (61.7%) Wide local excision | 4 (11.7%) |
| Luyten et al. (2014) [40] | 20 (100%) | Topical 5% imiquimod cream 2 times a week Topical 5% imiquimod cream 3 times a week | 15.4 w (4–52) | None | NA | NR |
| Marchitelli et al. (2014) [27] | 10 (100%) | Topical 5% imiquimod cream 3 times a week | 22 w (16–28) | None | NA | NR |
| Liu et al. (2014) [33] | 2 (2.9%) | 2 (2.9%) RT | NR | 69 (81%) | 12 (17.4%) Wide local excision 2 (2.9%) Partial vulvectomy 26 (37.6%) Simple vulvectomy 24 (34.7%) Radical vulvectomy 19 (27.5%) Inguinal lymphadenectomy | 13 (20′%) |
| Cowan et al. (2016) [42] | 8 (100%) | Topical 5% imiquimod cream 3 times a week | 12 w | None | NA | NA |
| Nagai et al. (2016) [28] | NR | NR | NA | 2 (100%) | 2 (100%) Wide local excision + split thickness skin graft 1 (50%) LNF dissection | 1 (50%) |
| Sopracordevole et al. (2016) [34] | 2 (7.4%) | CO2 laser excision | NA | 25 (92.5%) | (5–20%) Wide local excision (8–32%) Simple partial vulvectomy (9–36%) Simple total vulvectomy (1–4%) Skinning) total vulvectomy (2–8%) Total vulvectomy with inguino-femoral lymphadenectomy (11–40.7%) Plastic surgery (V-Y plasty, transposition flap, rotational flap, skin graft) | 11 (44%) |
| Onaiwu et al. (2016) [35] | 6 (6%) | (4–4.5%) imiquimod (1–1.1%) 5-fluorouracil (1–1.1%) laser ablation | NR | 74 (83.1%) | (55–61.8%) Wide local excision (13–14.6%) Radical vulvectomy (4–4.5%) Skinning vulvectomy (2–2.3%) MMS surgery | 3 (3.4%) |
| Rioli et al. (2018) [41] | 13 (100%) | Topical 16% methyl aminolevulinate (MAL) + PDT + (1–7.6%) Carbon dioxide laser | NA | None | NA | 3 (23%) |
| Nitecki et al. (2018) [29] | 20 (45.4%) | Topical 5% imiquimod cream | NR | 42 (95.4%) | (3–7%) MMS surgery (8–19%) Wide local excision (11–26%) Simple partial vulvectomy (17–40%) Radical partial vulvectomy (3–7%) Radical total vulvectomy (6–14%) Reconstructions with advancement flaps (1–2%) Inguinal LNF | 12 (27%) |
| Nasioudis et al. (2019) [36] | 156 (5.9%) | (26–0.9%) laser or other ablative methods (35–1.3%%) RT, (72–2.7%) immunotherapy (23–0.8%) C | NR | 2412 (92.6%) | (1133–46.9%) Local excision (824–34.1%) Simple/partial vulvectomy (172–7.1%) Total vulvectomy (155–6.4%) Radical vulvectomy (102–4.2%) NR (109–6.8%) LND | 1608 (61.8%) |
| Loiacono et al. (2019) [37] | 2 (8%) | (2–8%) Imiquimod and 5-fluorouracil (before surgery) | NR | 24 (100%) | (6–25%) Wide local excision (8–33%) Simple vulvectomy (10–42%) Extended vulvectomy (2–8%) LND (7–29%) Reconstructions with advancement flaps | 4 (17%) |
| Preti et al. (2021) [38] | 27 (33%) | (13–48%) Topical 5% imiquimod cream (10–37%) Topical corticosteroid cream (4–15%) Laser vaporization | NR | 95 (77%) | (41–44%) Local wide excision (26–27%) Hemi-vulvectomy (20–22%) Total vulvectomy (16–13%) Inguinal bilateral LND | 16 (16.8%) invasive 20 (21%) Microinvasive |
| Kosmidis et al. (2021) [30] | None | NA | NA | 2 (100%) | Wide local excision + lateral flaps Wide local excision + bilateral flaps | None |
| Ferrara et al. (2021) [44] | 10 (100%) | Fractional CO2 Laser irradiation followed by PDT every 2 weeks | 5 times 8 w | None | NA | None |
| Borella et al. (2022) [39] | 55 (100%) | 31 (56%) Topical 5% imiquimod cream 2 times a week 24 (44%) Topical 5% imiquimod cream 3 times a week | <144 w | None | NA | None |
| Van der Linden et al. (2022) [43] | 24 (100%) | 22 (91.7%) Topical 5% imiquimod cream 3 times a week 2 (8.3%) Topical 5% imiquimod cream 3 times a week+/- Topical 3% lidocaine in Vaseline ointment | 16 w | None | NA | None |
| Authors | FUP | Clinical Response n (%) | Vulvar Lesion (After Treatment) | Positive Margin Status | Side Effects (n–%) | OS Median (m)/yrs (%) |
|---|---|---|---|---|---|---|
| Hatch et al. (2008) [21] | 12 m 6 m | CR: 2 (100%) | NR | NA | Skin erosion (1–50%) Skin ulceration (1–50%) Hyperpigmentation (1–50%) | NR |
| Challenor et al. (2009) [22] | 4 m 3 m | CR: 2 (100%) | NR | 2 (100%) (After surgery) | NR | 3.5 m |
| Sendagorta et al. (2010) [23] | 26 m 22 m 20 m | CR: 3 (100%) | NR | NA | Moderate local irritation | NR |
| Baiocchi et al. (2012) [24] | 21 m 40 m NR NR | PR: 1 (25%) CR: 3 (75%) R: 1 (25%) | NR | 1 (25%) | Local irritation (4–100%) Local pain (4–100%) Vaginal bleeding (1–25%) | 30.5 m |
| Choi et al. (2013) [25] | 38 m (34–46) | CR: 3 (100%) | NR | NR | NR | 100% (38 m) |
| Sanderson et al. (2013) [26] | 18 m (12–24) | CR: 3 (50%) R: 1 (16.6%) PD: 2 (33.3%) | NR | NR | (2–33.2%) Soreness (3–50%) Erythema (2–33.2%) Irritation | 18 m |
| Cai et al. (2013) [31] | 54 m (7–169) | R:12 (34.3%) | NR | 16 (47%) | NR | 124.5 m (intraepithelial) 70.8 m (invasive) 21.3 m (adnexal Adc) |
| De Magnis et al. (2013) [32] | 76.9 m (4–184) | R:15 (44.1%) Ç: 1 (2.6%) CR: 26 (76.5%) PR: 1 (2.6%) §: 1 (2.6%) | NR | 15 (44.1%) | NR | 76.9 m |
| Luyten et al. (2014) [40] | 14.4 m (4–52) | CR: 11 (55%) PR: 5 (25%) SD: 2 (10%) Interruption: 2 (10%) | NR | NR | 1 (5%) Local reaction 19 (95%) Well tolerated | 14.4 m |
| Marchitelli et al. (2014) [27] | 18.3 m (2–49) | CR: 9 (90%) PR: 1 (10%) | NR | NA | Moderate local irritation Erosion | 18.3 m |
| Liu et al. (2014) [33] | 43.6 m | R: 20 (43.5%) after 12.7 m | NR | 15 (32.6%) | NR | NR |
| Cowan et al. (2016) [42] | 35 m (5–72) | CR: 6 (75%) after 12 w PR: 2 (25%) R: 4 (67%) L-FUP: 1 (12.5%) Interruption: 1 (12.5%) | NR | NA | Erythema Pain/burning | 35 m |
| Nagai et al. (2016) [28] | 12.8 m 112 m | R: 1 (50%) after 2.9 m Ç: 1 (50%) after 12.8 m CR: 1 (50%) | NR | None | NR | 112 m |
| Sopracordevole et al. (2016) [34] | 79.5 m (12–313) | R:8 (29.6%) | NR | 10 (40%) | NR | NR |
| Onaiwu et al. (2016) [35] | 73.2 m | R: 52 (58.4%) CR: 19 (23.5%) PR: 25 (30.9%) § 45 (55.6%) LFUP 8 | No macroscopic EOD | 47 (87%) | NR | 73.2 m |
| Rioli et al. (2018) [41] | 38 m (4–75) | CR: 2 (15%) PR: 5 (38%) SD: 5 (38%) PD: 1 (8%) R: 7 (54%) after 5 m (1–17) | NR | NA | 6 (60%) Moderate/Intense pain | NR |
| Nitecki et al. (2018) [29] | 45.8 m (1–178.9) | R: 25 (56.8%) | NR | 43 (97.7%) | NR | 28.7 m |
| Nasioudis et al. (2019) [36] | 66.5 m | NR | NR | 1214 (58%) 92 NA | NR | 84.3% (early-stage disease) 73.6% (advanced stage−81.7% stage II −59.5% stage III −33% stage IV) 53.4% (No surgery) 83.6% (positive surgical margins) 84.6% (negative margins) |
| Loiacono et al. (2019) [37] | 39 m (1−240) | CR: 13 (54%) R: 8 (33%) §: 9 (37.5%) Ç: 1 (4%) LFUP 1 (4%) | NR | 12 (50%) | Wound dehiscence (4−17%) Urethral stenosis (4−17%) | 39 m |
| Preti et al. (2021) [38] | 94.6 m | R: 69/95 (73%) CR: 79/95 (83.1%) PR: 16/95 (16.8%) | NR | 77 (92%) 11 NA | NR | 98% (non-invasive and microinvasive VPD) 50% (invasive VPD) |
| Kosmidis et al. (2021) [30] | NR | NR | NR | None | None | NR |
| Ferrara et al. (2021) [44] | 12 m | CR: 2 (20%) R: 6 (60%) SD: 2 (20%) | NR | NA | Swelling + Pain 2 (20%) Hyperpigmentation | 12 m |
| Borella et al. (2022) [39] | 66 m (17−148) | CR: 22 (43%) PR: 29 (56%) Interruption: 4 (7%) | NR | NA | 2 (3.6%) Erosion and local burning 2 (3.6%) Flu like syndrome | NR |
| Van der Linden et al. (2022) [43] | 31 m (14−46) | CR: 12 (52.2%) PR: 7 (30.4%) SD: 4 (17.4%) R: 8 (34.8%) LFUP: 1 (4.1%) | 1 cm2 (0−130 cm2; t-test, p = 0.001) | NA | (67–71%) Fatigue (17–46%) Headaches (>80%) Pain | 31 m |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Della Corte, L.; Cafasso, V.; Conte, C.; Cuomo, L.; Giampaolino, P.; Lavitola, G.; Bifulco, G. Medical and Surgical Strategies in Vulvar Paget Disease: Let’s Throw Some Light! J. Pers. Med. 2023, 13, 100. https://doi.org/10.3390/jpm13010100
Della Corte L, Cafasso V, Conte C, Cuomo L, Giampaolino P, Lavitola G, Bifulco G. Medical and Surgical Strategies in Vulvar Paget Disease: Let’s Throw Some Light! Journal of Personalized Medicine. 2023; 13(1):100. https://doi.org/10.3390/jpm13010100
Chicago/Turabian StyleDella Corte, Luigi, Valeria Cafasso, Carmine Conte, Lara Cuomo, Pierluigi Giampaolino, Giada Lavitola, and Giuseppe Bifulco. 2023. "Medical and Surgical Strategies in Vulvar Paget Disease: Let’s Throw Some Light!" Journal of Personalized Medicine 13, no. 1: 100. https://doi.org/10.3390/jpm13010100
APA StyleDella Corte, L., Cafasso, V., Conte, C., Cuomo, L., Giampaolino, P., Lavitola, G., & Bifulco, G. (2023). Medical and Surgical Strategies in Vulvar Paget Disease: Let’s Throw Some Light! Journal of Personalized Medicine, 13(1), 100. https://doi.org/10.3390/jpm13010100