
Goals, Expectations, and the Definition of Success for Neuromodulation for Pain According to Representatives of Neuromodulation Device Manufacturers
 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collection
2.3. Data Analysis
3. Results
3.1. Survey Respondents
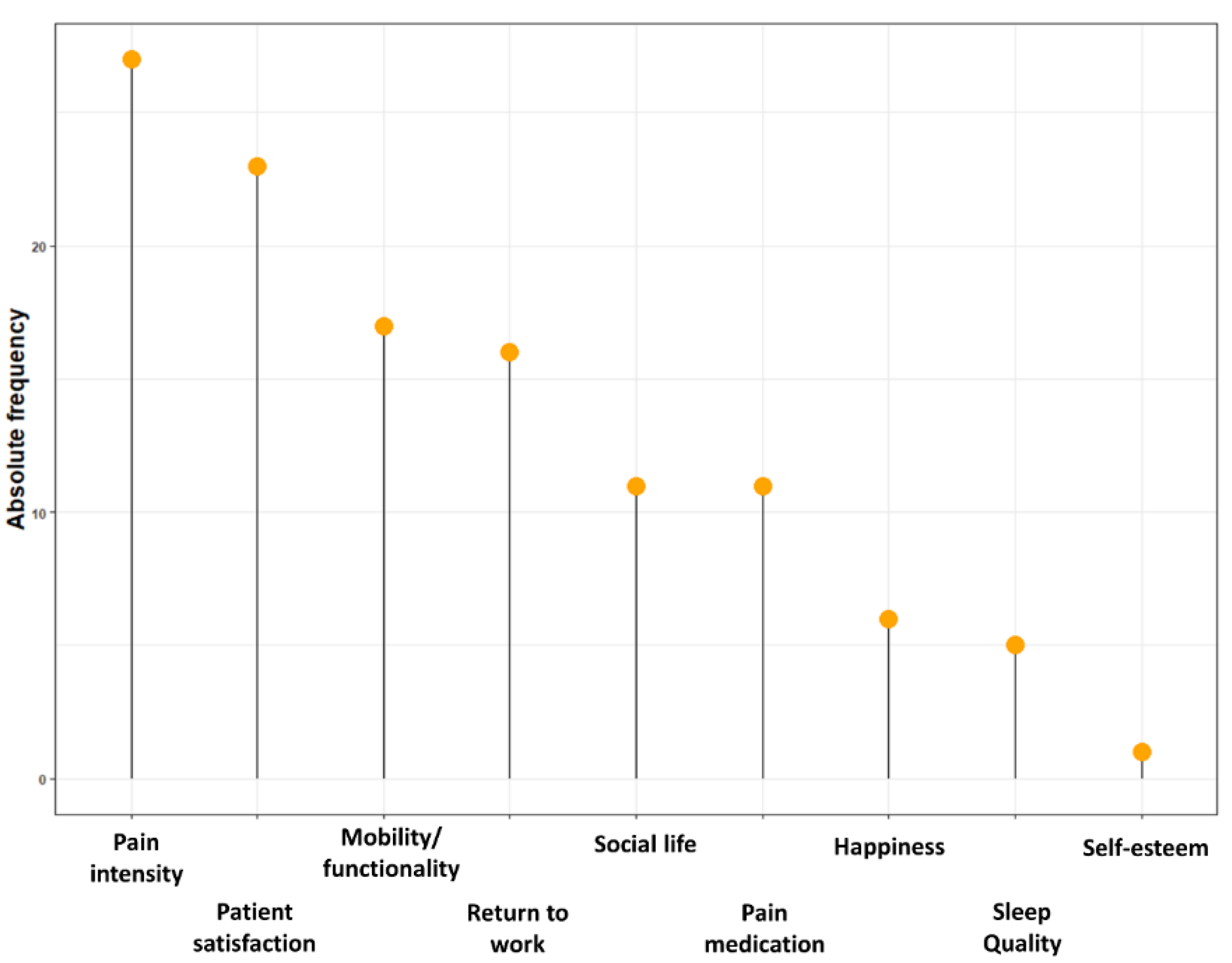
3.2. Goals and Influenceable Factors
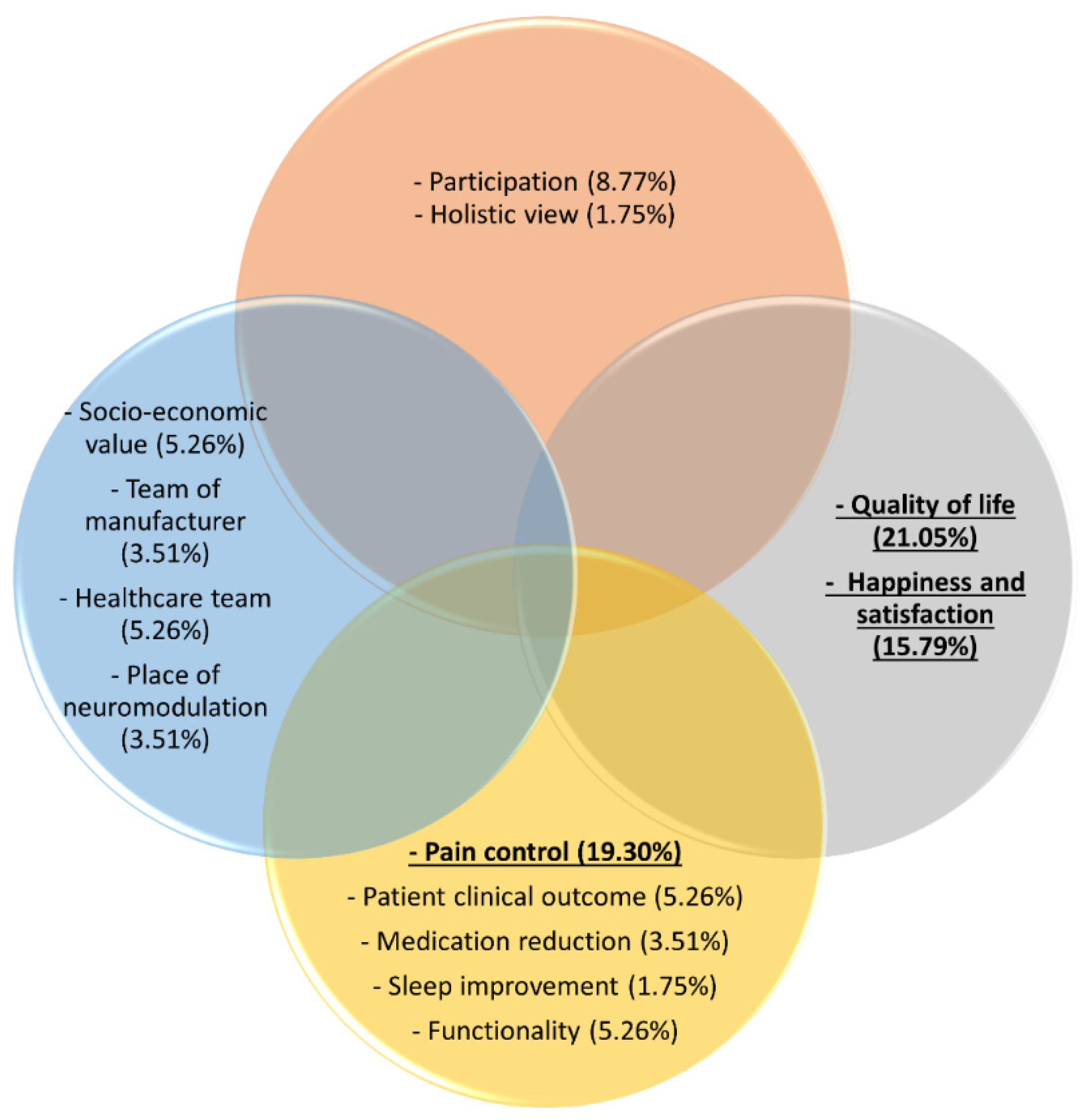
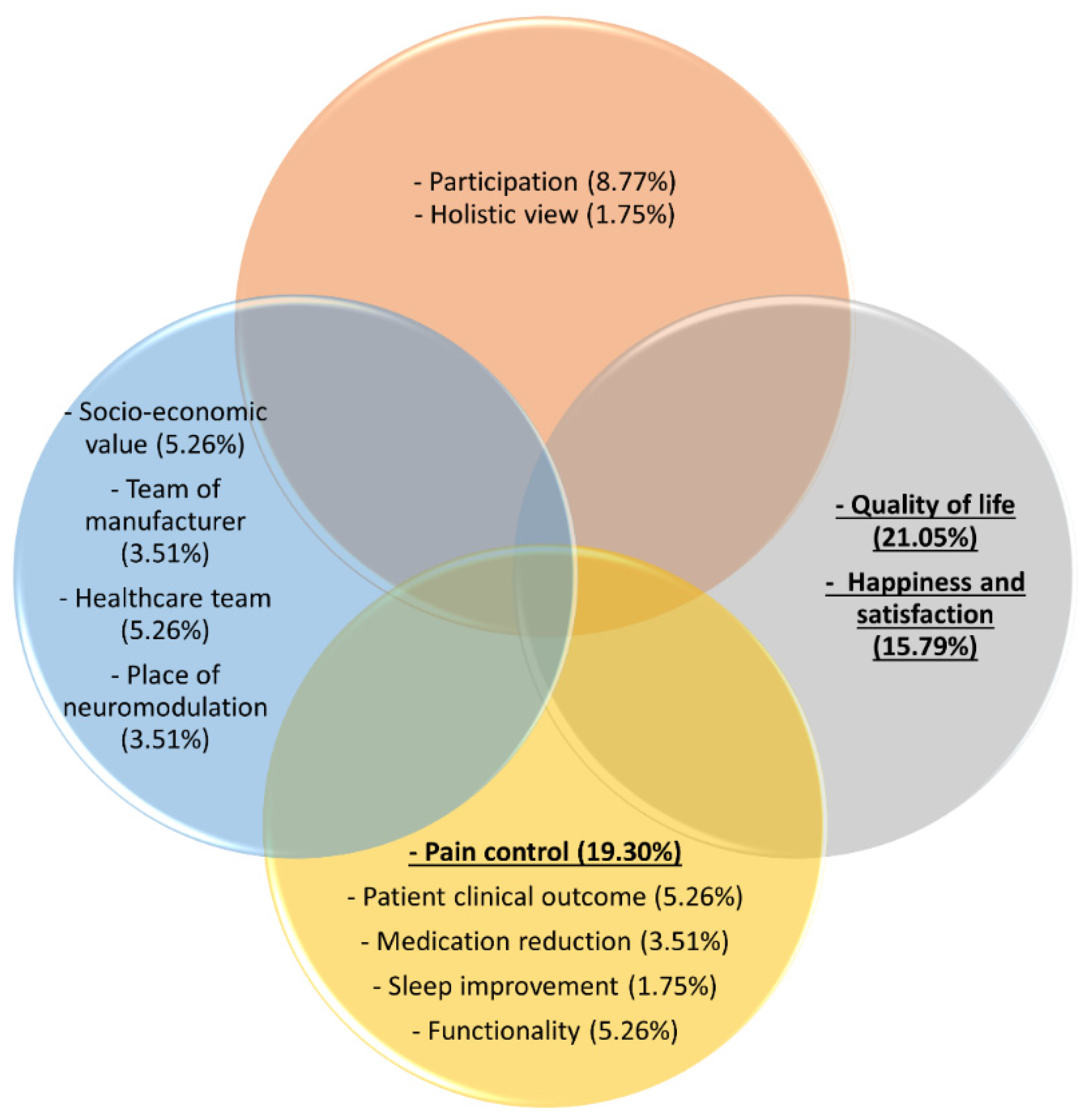
3.3. Success of Neuromodulation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wood, C.; Martiné, G.; Espagne-Dubreuilh, G.; Le Goff, K.; Moens, M.; Goudman, L.; Baron, S.; David, R.; Naïditch, N.; Billot, M.; et al. The Added Value of Intraoperative Hypnosis during Spinal Cord Stimulation Lead Implantation under Awake Anesthesia in Patients Presenting with Refractory Chronic Pain. Medicina 2022, 58, 220. [Google Scholar] [CrossRef] [PubMed]
- Thomson, S.; Huygen, F.; Prangnell, S.; De Andrés, J.; Baranidharan, G.; Belaïd, H.; Berry, N.; Billet, B.; Cooil, J.; De Carolis, G.; et al. Appropriate referral and selection of patients with chronic pain for spinal cord stimulation: European consensus recommendations and e-health tool. Eur. J. Pain 2020, 24, 1169–1181. [Google Scholar] [CrossRef]
- Goudman, L.; Rigoard, P.; Billot, M.; Duarte, R.V.; Eldabe, S.; Moens, M. Patient selection for Spinal Cord Stimulation in treatment of pain: A sequential decision-making model. A narrative review. J. Pain Res. 2022, 15, 1163. [Google Scholar] [CrossRef] [PubMed]
- Goudman, L.; De Groote, S.; Linderoth, B.; De Smedt, A.; Eldabe, S.; Duarte, R.; Moens, M. Exploration of the Supraspinal Hypotheses about Spinal Cord Stimulation and Dorsal Root Ganglion Stimulation: A Systematic Review. J. Clin. Med. 2021, 10, 2766. [Google Scholar] [CrossRef]
- Rigoard, P.; Gatzinsky, K.; Deneuville, J.-P.; Duyvendak, W.; Naiditch, N.; Van Buyten, J.-P.; Eldabe, S. Optimizing the Management and Outcomes of Failed Back Surgery Syndrome: A Consensus Statement on Definition and Outlines for Patient Assessment. Pain Res. Manag. 2019, 2019, 3126464. [Google Scholar] [CrossRef] [PubMed]
- Malfliet, A.; Coppieters, I.; Van Wilgen, P.; Kregel, J.; De Pauw, R.; Dolphens, M.; Ickmans, K. Brain changes associated with cognitive and emotional factors in chronic pain: A systematic review. Eur. J. Pain 2017, 21, 769–786. [Google Scholar] [CrossRef]
- Wijma, A.J.; Van Wilgen, C.P.; Meeus, M.; Nijs, J. Clinical biopsychosocial physiotherapy assessment of patients with chronic pain: The first step in pain neuroscience education. Physiother. Theory Pract. 2016, 32, 368–384. [Google Scholar] [CrossRef]
- Naiditch, N.; Billot, M.; Moens, M.; Goudman, L.; Cornet, P.; Le Breton, D.; Roulaud, M.; Ounajim, A.; Page, P.; Lorgeoux, B.; et al. Persistent Spinal Pain Syndrome Type 2 (PSPS-T2), a Social Pain? Advocacy for a Social Gradient of Health Approach to Chronic Pain. J. Clin. Med. 2021, 10, 2817. [Google Scholar] [CrossRef]
- Naiditch, N.; Billot, M.; Goudman, L.; Cornet, P.; Roulaud, M.; Ounajim, A.; Page, P.; Lorgeoux, B.; Baron, S.; Nivole, K.; et al. Professional Status of Persistent Spinal Pain Syndrome Patients after Spinal Surgery (PSPS-T2): What Really Matters? A Prospective Study Introducing the Concept of “Adapted Professional Activity” Inferred from Clinical, Psychological and Social Influence. J. Clin. Med. 2021, 10, 5055. [Google Scholar] [CrossRef]
- Dekker, J.; De Groot, V.; Ter Steeg, A.M.; Vloothuis, J.; Holla, J.; Collette, E.; Satink, T.; Post, L.; Doodeman, S.; Littooij, E. Setting meaningful goals in rehabilitation: Rationale and practical tool. Clin. Rehabil. 2019, 34, 3–12. [Google Scholar] [CrossRef]
- Goudman, L.; De Smedt, A.; Linderoth, B.; Eldabe, S.; Witkam, R.; Henssen, D.; Moens, M. Identifying goals in patients with chronic pain: A European survey. Eur. J. Pain 2021, 25, 1959–1970. [Google Scholar] [CrossRef]
- Chadwick, A.; Frazier, A.; Khan, T.W.; Young, E. Understanding the Psychological, Physiological, and Genetic Factors Affecting Precision Pain Medicine: A Narrative Review. J. Pain Res. 2021, 14, 3145–3161. [Google Scholar] [CrossRef]
- Ba, N.A.S.; Rosenow, J.M. Ethical Considerations in the Implantation of Neuromodulatory Devices. Neuromodulation Technol. Neural Interface 2021, 25, 222–231. [Google Scholar] [CrossRef]
- Goudman, L.; Bruzzo, A.; Van De Sande, J.; Moens, M. Goal Identification Before Spinal Cord Stimulation: A Qualitative Exploration in Potential Candidates. Pain Pract. 2019, 20, 247–254. [Google Scholar] [CrossRef]
- Náfrádi, L.; Kostova, Z.; Nakamoto, K.; Schulz, P.J. The doctor–patient relationship and patient resilience in chronic pain: A qualitative approach to patients’ perspectives. Chronic Illn. 2018, 14, 256–270. [Google Scholar] [CrossRef]
- Lambing, A.; Nichols, C.D.; Munn, J.E.; Anderson, T.L.; Tortella, B.J.; Witkop, M.L. Patient, caregiver, and provider perceptions of pain and pain management in adolescents and young adults with bleeding disorders. Haemophilia 2017, 23, 852–860. [Google Scholar] [CrossRef]
- Clingan, J.A.; Patel, A.; Maher, D.P. Survey of Spinal Cord Stimulation Hardware Currently Available for the Treatment of Chronic Pain in the United States. Front. Pain Res. 2020, 1, 572907. [Google Scholar] [CrossRef]
- Bala, K.; Sharma, K. Role of Medical Representatives in Influencing Medicine Prescription Behaviour of Doctors. J. Bus. Thought 2020, 10, 39–52. [Google Scholar] [CrossRef]
- Ali, K.E.; Naser, A.Y.; Al-Rousan, R.; Alwafi, H.; AbuAlhommos, A.K.; Alsairafi, Z.K.; Salawati, E.M.; Samannodi, M.; Dairi, M.S. The attitude and acceptability towards medical promotional tools and their influence on physicians’ prescribing practices in Jordan and Iraq: A cross-sectional study. BMC Health Serv. Res. 2022, 22, 105. [Google Scholar] [CrossRef]
- Wade, D. Goal setting in rehabilitation: An overview of what, why and how. Clin. Rehabil. 2009, 23, 291–295. [Google Scholar] [CrossRef] [Green Version]
- Workneh, B.D.; Gebrehiwot, M.G.; Bayo, T.A.; Gidey, M.T.; Belay, Y.B.; Tesfaye, D.M.; Kassa, T.T. Influence of Medical Representatives on Prescribing Practices in Mekelle, Northern Ethiopia. PLoS ONE 2016, 11, e0156795. [Google Scholar] [CrossRef]
- Fugh-Berman, A.; Ahari, S. Following the Script: How Drug Reps Make Friends and Influence Doctors. PLoS Med. 2007, 4, e150. [Google Scholar] [CrossRef] [PubMed]
- Goudman, L.; De Smedt, A.; Billot, M.; Roulaud, M.; Rigoard, P.; Moens, M. Opinions of healthcare providers about neuromodulation for pain: Results of an online survey at the 2nd Joint Congress of the INS European Chapters. Neuromodulation Technol. Neural Interface 2022. [Google Scholar] [CrossRef]
- Moens, M.; Goudman, L.; Brouns, R.; Msc, A.V.E.; De Jaeger, M.; Huysmans, E.; Putman, K.; Verlooy, J.; Moens, M.; Msc, L.G.; et al. Return to Work of Patients Treated with Spinal Cord Stimulation for Chronic Pain: A Systematic Review and Meta-Analysis. Neuromodulation Technol. Neural Interface 2018, 22, 253–261. [Google Scholar] [CrossRef]
- Szmuda, T.; Słoniewski, P.; Ali, S.; Aleksandrowicz, K. Does Spinal Cord Stimulation Due to Failed Back Surgery Syndrome Lead to Permanent Occupational Disability? Neuromodulation Technol. Neural Interface 2020, 23, 653–659. [Google Scholar] [CrossRef]
- Gopal, H.; Fitzgerald, J.; McCrory, C. Spinal cord stimulation for FBSS and CRPS: A review of 80 cases with on-table trial of stimulation. J. Back Musculoskelet. Rehabil. 2016, 29, 7–13. [Google Scholar] [CrossRef]
- Goudman, L.; De Smedt, A.; Forget, P.; Eldabe, S.; Moens, M. High-Dose Spinal Cord Stimulation Reduces Long-Term Pain Medication Use in Patients with Failed Back Surgery Syndrome Who Obtained at Least 50% Pain Intensity and Medication Reduction During a Trial Period: A Registry-Based Cohort Study. Neuromodulation Technol. Neural Interface 2021, 24, 520–531. [Google Scholar] [CrossRef]
- Pollard, E.M.; Lamer, T.J.; Moeschler, S.M.; Gazelka, H.M.; Hooten, W.M.; Bendel, M.A.; Warner, N.S.; Murad, M.H. The effect of spinal cord stimulation on pain medication reduction in intractable spine and limb pain: A systematic review of randomized controlled trials and meta-analysis. J. Pain Res. 2019, 12, 1311–1324. [Google Scholar] [CrossRef]
- Pilitsis, J.G.; Fahey, M.; Custozzo, A.; Chakravarthy, K.; Capobianco, R. Composite Score Is a Better Reflection of Patient Response to Chronic Pain Therapy Compared with Pain Intensity Alone. Neuromodulation Technol. Neural Interface 2020, 24, 68–75. [Google Scholar] [CrossRef]
- Goudman, L.; De Smedt, A.; Eldabe, S.; Rigoard, P.; Linderoth, B.; De Jaeger, M.; Moens, M.; Consortium, D. High-dose spinal cord stimulation for patients with failed back surgery syndrome: A multicenter effectiveness and prediction study. Pain 2020, 162, 582–590. [Google Scholar] [CrossRef]
- Goudman, L.; Billot, M.; Duarte, R.V.; Eldabe, S.; Rigoard, P.; Moens, M. Gradation of Clinical Holistic Response as New Composite Outcome to Evaluate Success in Spinal Cord Stimulation Studies for Pain. Neuromodulation Technol. Neural Interface, 2021; ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Rigoard, P.; Ounajim, A.; Goudman, L.; Louis, P.-Y.; Yousri, S.; Roulaud, M.; Bouche, B.; Wood, C.; Page, P.; Lorgeoux, B.; et al. A Novel Multi-Dimensional Clinical Response Index Dedicated to Improve Pain Global Assessment in Patients with Persistent Spinal Pain Syndrome after Spinal Surgery, Based on a Real-Life Prospective Multicentric Study (PREDIBACK) and Machine Learning Techniques. J. Clin. Med. 2021, 10, 4910. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, R.M.; Hays, R.D. Health-Related Quality of Life Measurement in Public Health. Annu. Rev. Public Health 2022, 43, 355–373. [Google Scholar] [CrossRef]
- Yang, F.; Devlin, N.; Luo, N. Cost-Utility Analysis Using EQ-5D-5L Data: Does How the Utilities Are Derived Matter? Value Health 2018, 22, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Liang, F.; Zhu, J.; Mo, M.; Zhou, C.; Jia, H.; Xie, L.; Zheng, Y.; Zhang, S. Role of industry funders in oncology RCTs published in high-impact journals and its association with trial conclusions and time to publication. Ann. Oncol. 2018, 29, 2129–2134. [Google Scholar] [CrossRef] [PubMed]
- Wareham, K.J.; Hyde, R.M.; Grindlay, D.; Brennan, M.L.; Dean, R.S. Sponsorship bias and quality of randomised controlled trials in veterinary medicine. BMC Veter Res. 2017, 13, 234. [Google Scholar] [CrossRef] [PubMed]
- Flacco, M.E.; Manzoli, L.; Boccia, S.; Capasso, L.; Aleksovska, K.; Rosso, A.; Scaioli, G.; De Vito, C.; Siliquini, R.; Villari, P.; et al. Head-to-head randomized trials are mostly industry sponsored and almost always favor the industry sponsor. J. Clin. Epidemiol. 2015, 68, 811–820. [Google Scholar] [CrossRef] [PubMed]
- Bicket, M.C.; Dunn, R.Y.; Ahmed, S.U. High-Frequency Spinal Cord Stimulation for Chronic Pain: Pre-Clinical Overview and Systematic Review of Controlled Trials. Pain Med. 2016, 17, 2326–2336. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Goals of Representatives of Neuromodulation Device Manufacturers | All Respondents (N = 39) | Respondents with Patient Contact (N = 13) | Respondents from Higher Management (N = 15) |
|---|---|---|---|
| To improve the economic value of your company | 9 (7.8%) | 3 (7.9%) | 4 (8.9%) |
| To have a major impact on health-economic aspects | 12 (10.3%) | 2 (5.3%) | 8 (17.8%) |
| To become a key opinion leader in innovation | 8 (6.9%) | 3 (7.9%) | 0 (0.0%) |
| To become a trusted partner for physicians | 25 (21.5%) | 9 (23.7%) | 8 (17.8%) |
| To provide excellent service at the highest standards for physicians | 24 (20.7%) | 9 (23.7%) | 9 (20.0%) |
| To provide excellent service at the highest standards for patients | 26 (22.4%) | 8 (21.0%) | 11 (24.4%) |
| To improve my personal technical/marketing/management skills | 3 (2.6%) | 2 (5.3%) | 0 (0.0%) |
| To have superior quality/superior clinical results/etc. compared to our competitors | 7 (6.0%) | 2 (5.3%) | 3 (6.7%) |
| To have the highest impact on national regulations | 1 (0.9%) | 0 (0.0%) | 1 (2.2%) |
| To have the broadest portfolio in neuromodulation for pain | 1 (0.9%) | 0 (0.0%) | 1 (2.2%) |
| Expectations of Representatives of Neuromodulation Device Manufacturers | All Respondents (N = 39) | Respondents with Patient Contact (N = 13) | Respondents from Higher Management (N = 15) |
|---|---|---|---|
| Pain intensity | 27 (23.1%) | 8 (20.5%) | 9 (20.2%) |
| Mobility/functionality | 17 (14.5%) | 4 (10.2%) | 6 (13.3%) |
| Pain medication use | 11 (9.4%) | 4 (10.2%) | 5 (11.1%) |
| Sleep quality | 5 (4.3%) | 3 (7.7%) | 0 (0.0%) |
| Capacity to return to work | 16 (13.7%) | 6 (15.4%) | 9 (20.2%) |
| Participation in social life | 11 (9.4%) | 4 (10.2%) | 5 (11.1%) |
| Self-esteem | 1 (0.8%) | 0 (0.0%) | 0 (0.0%) |
| Feeling of happiness | 6 (5.1%) | 4 (10.2%) | 1 (2.2%) |
| Patient satisfaction | 23 (19.7%) | 6 (15.4%) | 10 (22.2%) |
| Components Included in Definition of Success of Neuromodulation for Pain | All Respondents (N = 35) | Respondents with Patient Contact (N = 13) | Respondents from Higher Management (N = 14) |
|---|---|---|---|
| Pain control | 11 (19.3%) | 5 (22.7%) | 3 (15.8%) |
| Quality of life | 12 (21%) | 4 (18.2%) | 5 (26.3%) |
| Happiness and satisfaction | 9 (15.8%) | 2 (9.1%) | 1 (5.3%) |
| Participation | 5 (8.8%) | 1 (4.5%) | 3 (15.8%) |
| Holistic view | 1 (1.8%) | 1 (4.5%) | 0 (0.0%) |
| Socioeconomic value | 3 (5.3%) | 2 (9.1%) | 1 (5.3%) |
| Team of manufacturer | 2 (3.5%) | 0 (0.0%) | 2 (10.5%) |
| Healthcare team | 3 (5.3%) | 0 (0.0%) | 1 (5.3%) |
| Place of neuromodulation | 2 (3.5%) | 1 (4.5%) | 1 (5.3%) |
| Patient clinical outcome | 3 (5.3%) | 2 (9.1%) | 1 (5.3%) |
| Medication reduction | 2 (3.5%) | 2 (9.1%) | 0 (0.0%) |
| Sleep improvement | 1 (1.8%) | 1 (4.5%) | 0 (0.0%) |
| Functionality | 3 (5.3%) | 1 (4.5%) | 1 (5.3%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moens, M.; Alliet, W.; Billot, M.; De Smedt, A.; Flamée, P.; Vanhonacker, D.; Roulaud, M.; Rigoard, P.; Goudman, L. Goals, Expectations, and the Definition of Success for Neuromodulation for Pain According to Representatives of Neuromodulation Device Manufacturers. J. Pers. Med. 2022, 12, 1457. https://doi.org/10.3390/jpm12091457
Moens M, Alliet W, Billot M, De Smedt A, Flamée P, Vanhonacker D, Roulaud M, Rigoard P, Goudman L. Goals, Expectations, and the Definition of Success for Neuromodulation for Pain According to Representatives of Neuromodulation Device Manufacturers. Journal of Personalized Medicine. 2022; 12(9):1457. https://doi.org/10.3390/jpm12091457
Chicago/Turabian StyleMoens, Maarten, William Alliet, Maxime Billot, Ann De Smedt, Panagiotis Flamée, Domien Vanhonacker, Manuel Roulaud, Philippe Rigoard, and Lisa Goudman. 2022. "Goals, Expectations, and the Definition of Success for Neuromodulation for Pain According to Representatives of Neuromodulation Device Manufacturers" Journal of Personalized Medicine 12, no. 9: 1457. https://doi.org/10.3390/jpm12091457
APA StyleMoens, M., Alliet, W., Billot, M., De Smedt, A., Flamée, P., Vanhonacker, D., Roulaud, M., Rigoard, P., & Goudman, L. (2022). Goals, Expectations, and the Definition of Success for Neuromodulation for Pain According to Representatives of Neuromodulation Device Manufacturers. Journal of Personalized Medicine, 12(9), 1457. https://doi.org/10.3390/jpm12091457