

Three-Dimensional Semantic Segmentation of Diabetic Retinopathy Lesions and Grading Using Transfer Learning
 , ,
, ,  and
and
Abstract
:1. Introduction
- (1)
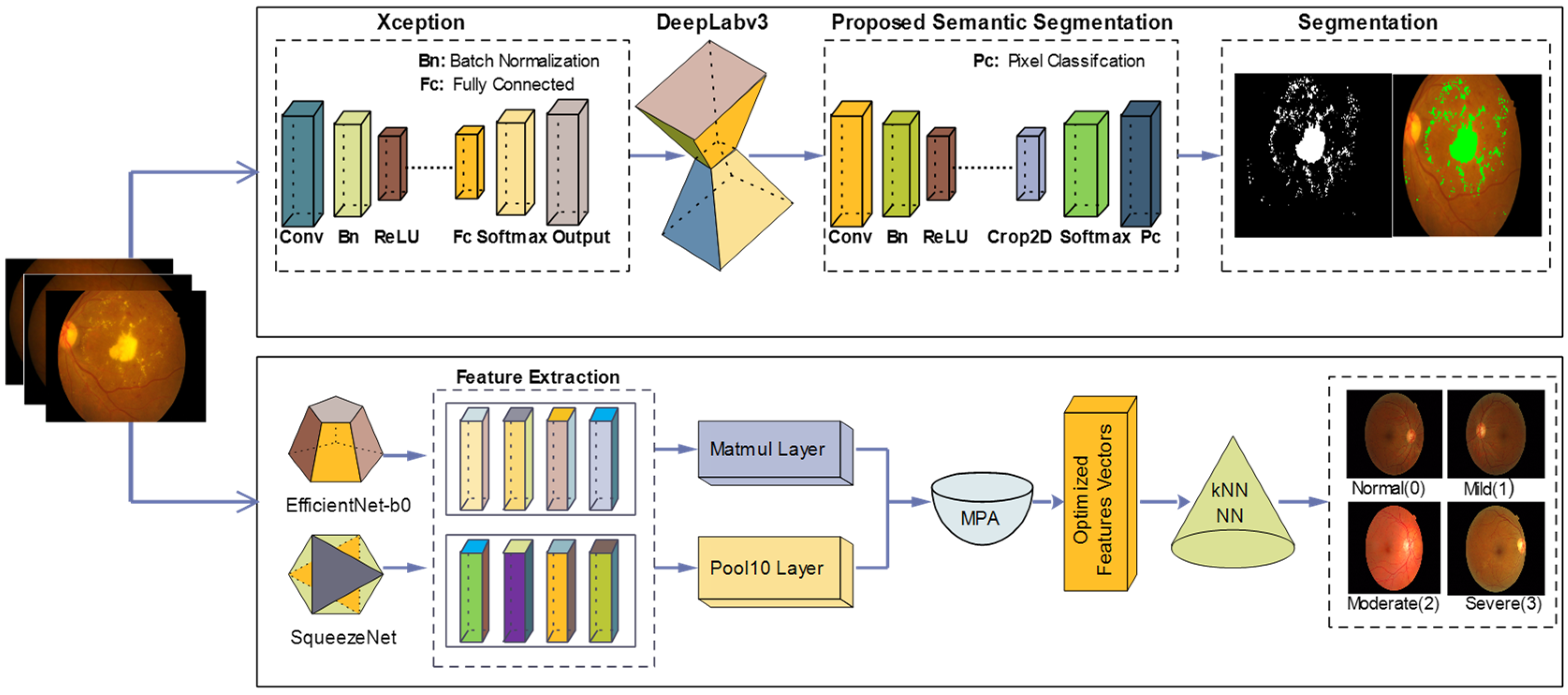
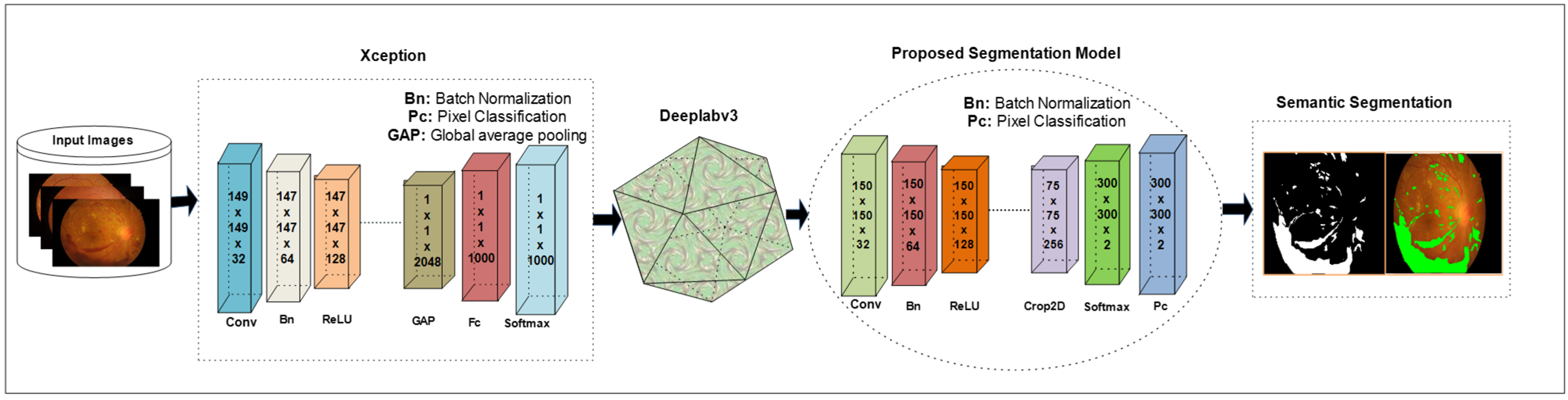
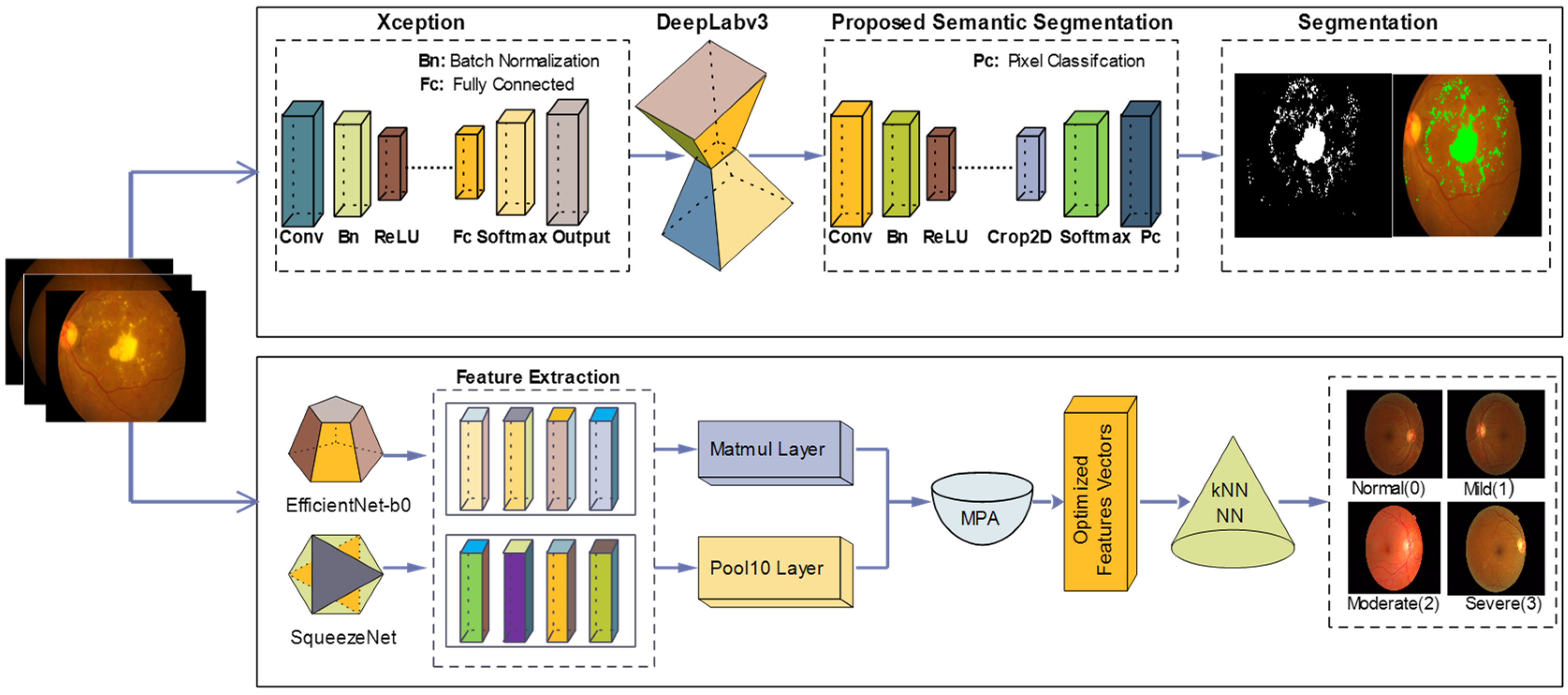
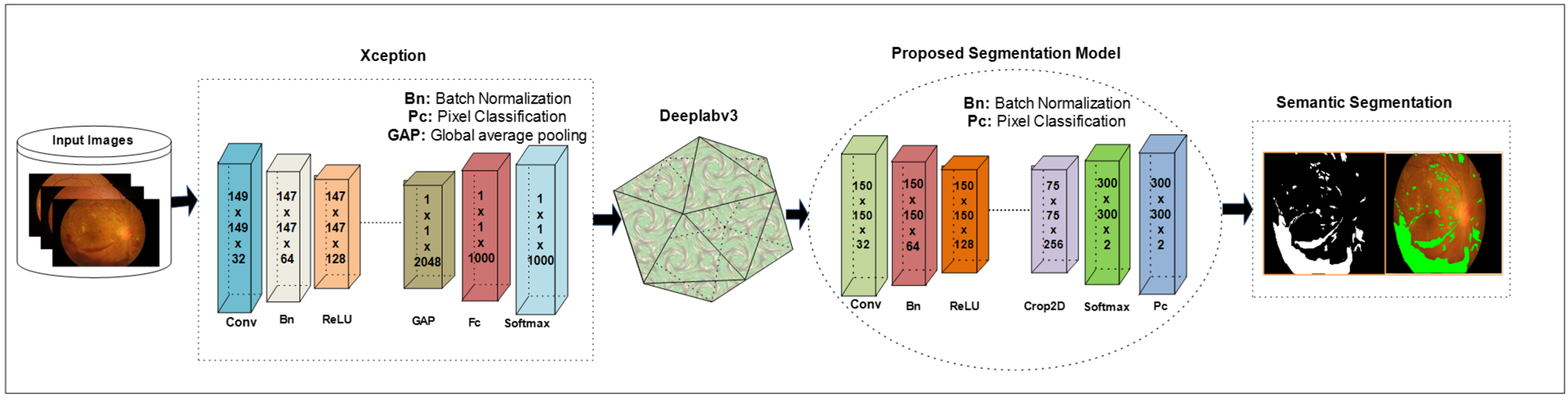
- The pre-trained Xception model is combined with the Deeplabv3 model. The output of these models is trained on the selected hyperparameters that are finalized after experiments for DR lesion segmentation.
- (2)
- Two transform learning models, efficient-net-b0 and squeeze-net, are employed for feature extraction from the selected fully connected layers such as MATMUL and pool-10, respectively.
- (3)
- The extracted features from MATMUL and pool-10 layers are fused in serial. The adequate features are determined using MPA.
- (4)
- For selection of the best features, the MPA model is trained on the selected hyperparameters. The selected features using the MPA model are passed to the KNN and NN classifiers for DR grade classification.
2. Related Work
3. Proposed Methodology
3.1. Proposed Semantic Segmentation Model
3.2. Classification of DR Lesions Using Deep Features
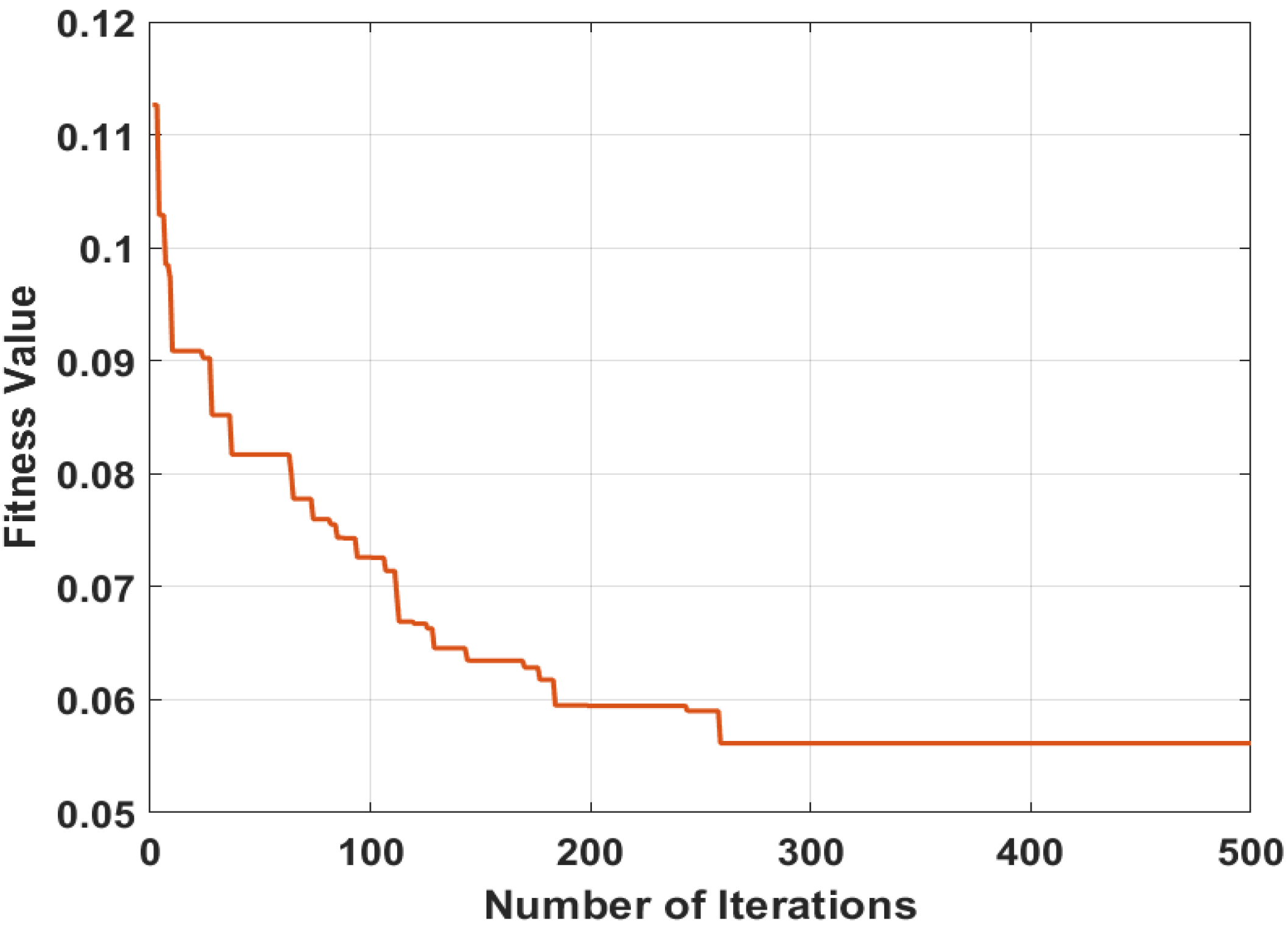
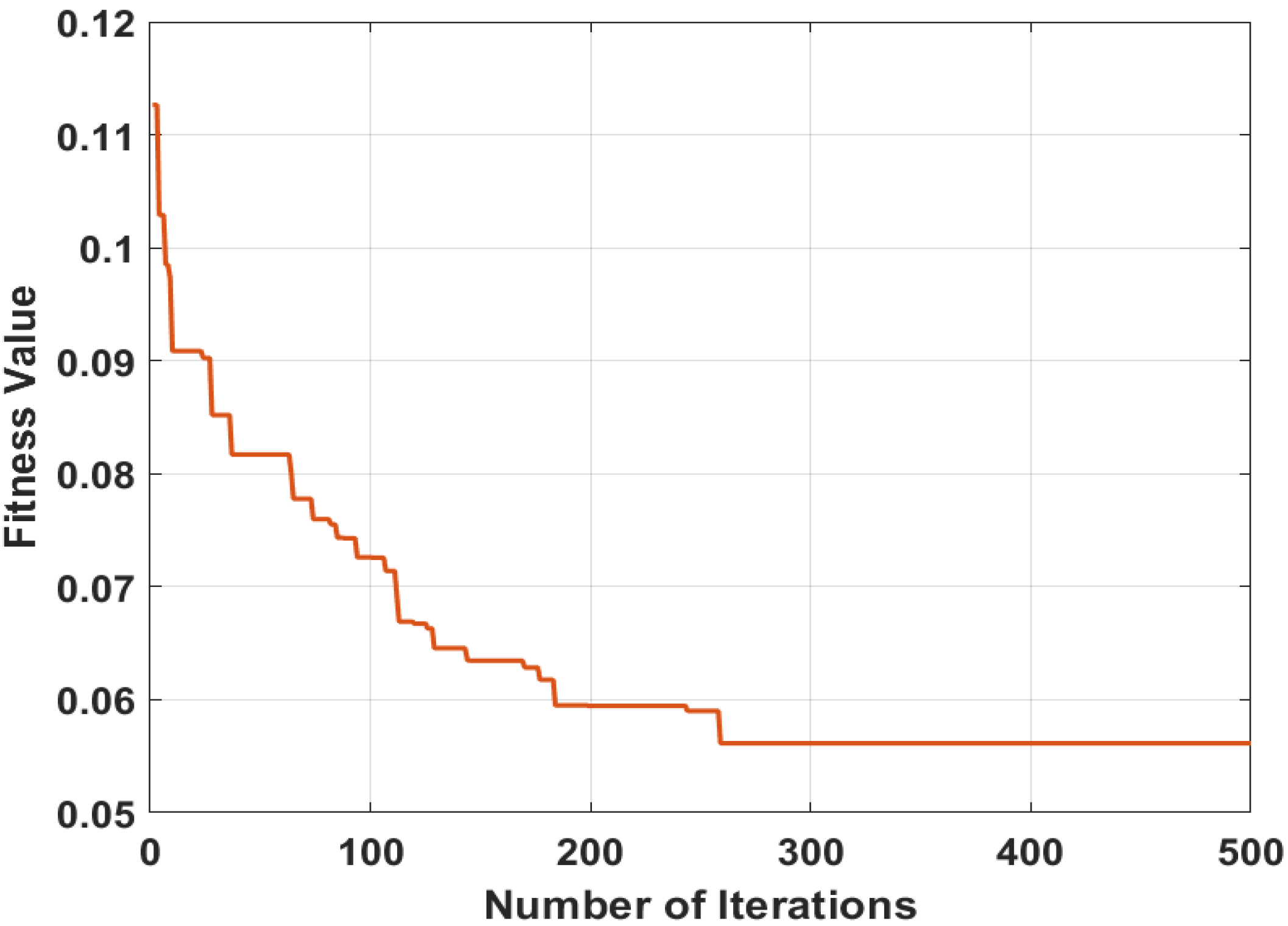
3.3. Feature Selection Using MPA
4. Experimental Discussion
- (1)
- Grade0 = 1092 images
- (2)
- Grade1 = 1224 images
- (3)
- Grade2 = 1976 images
- (4)
- Grade3 = 1016 images
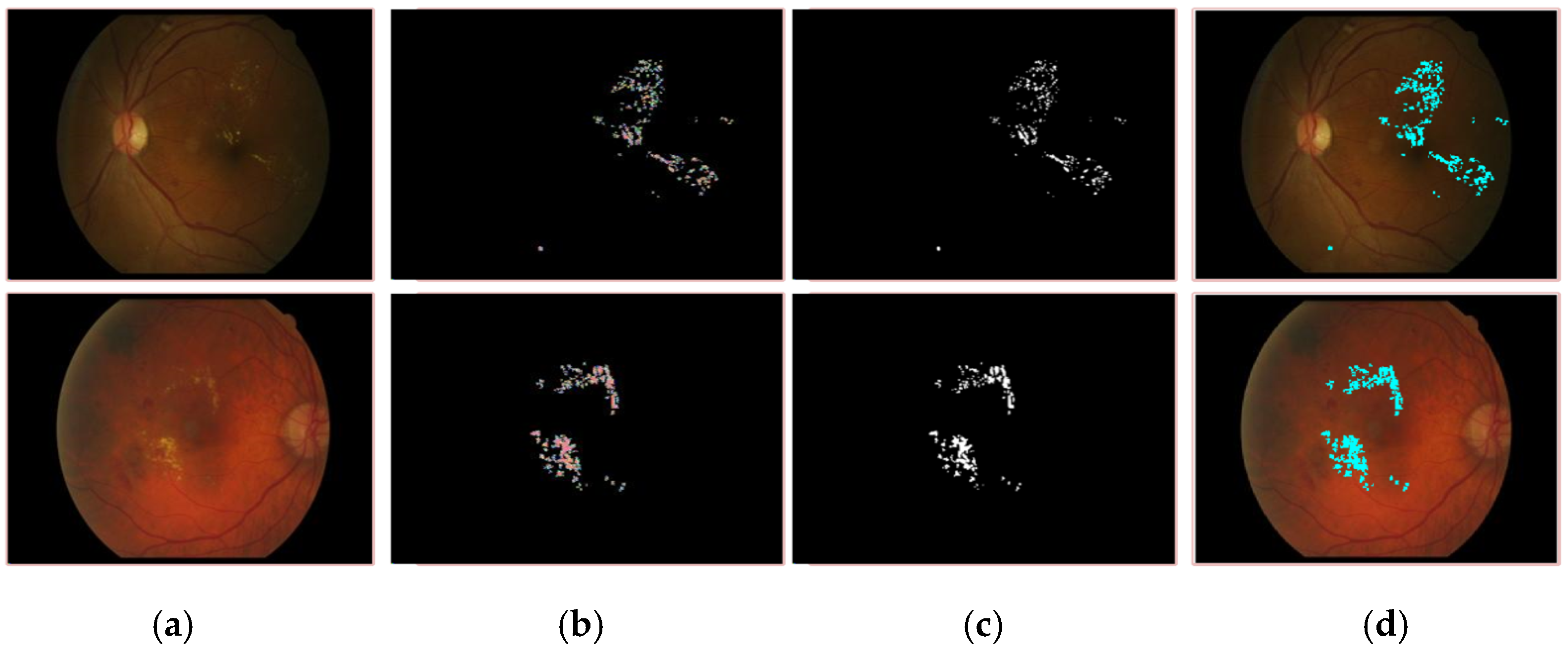
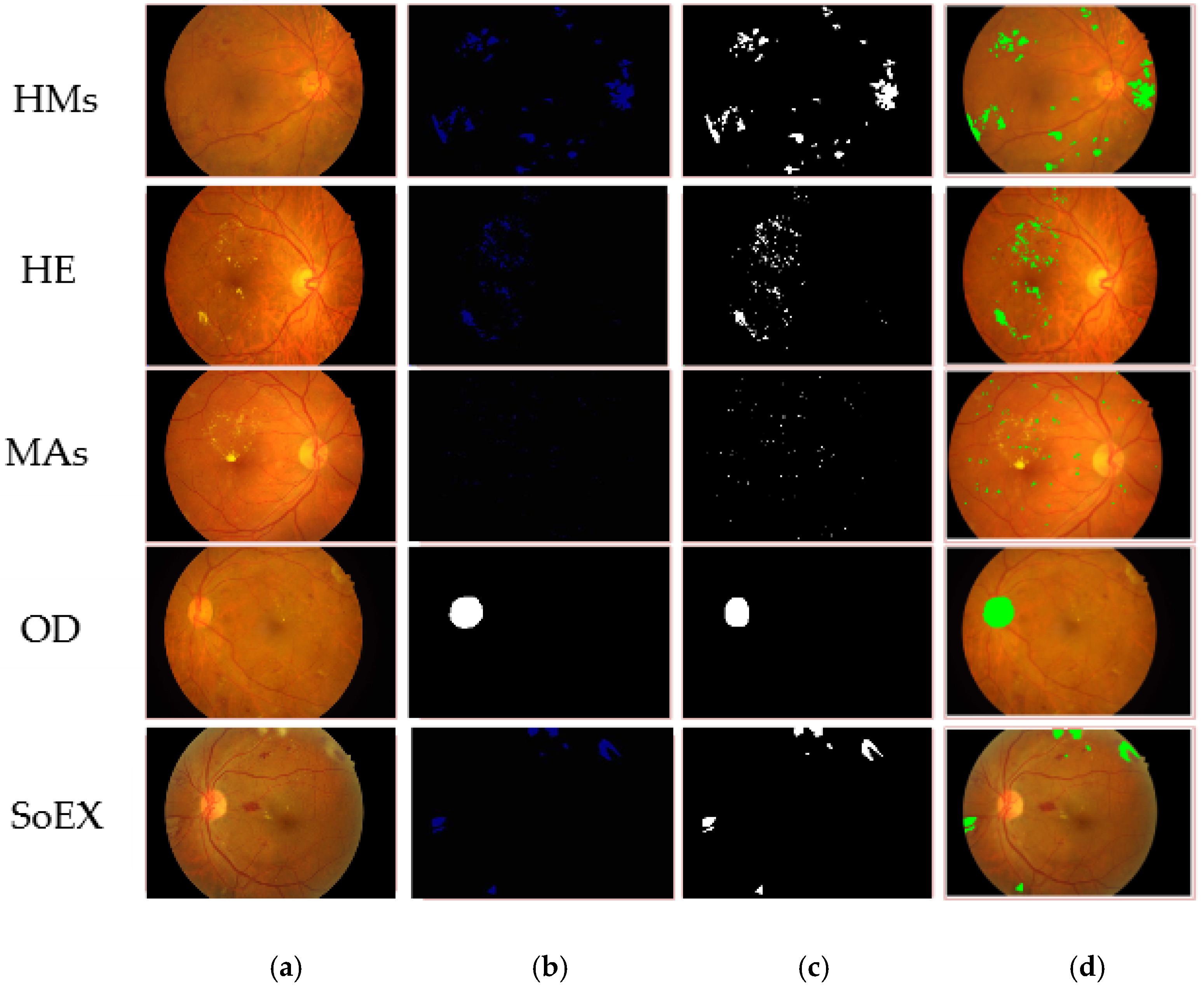
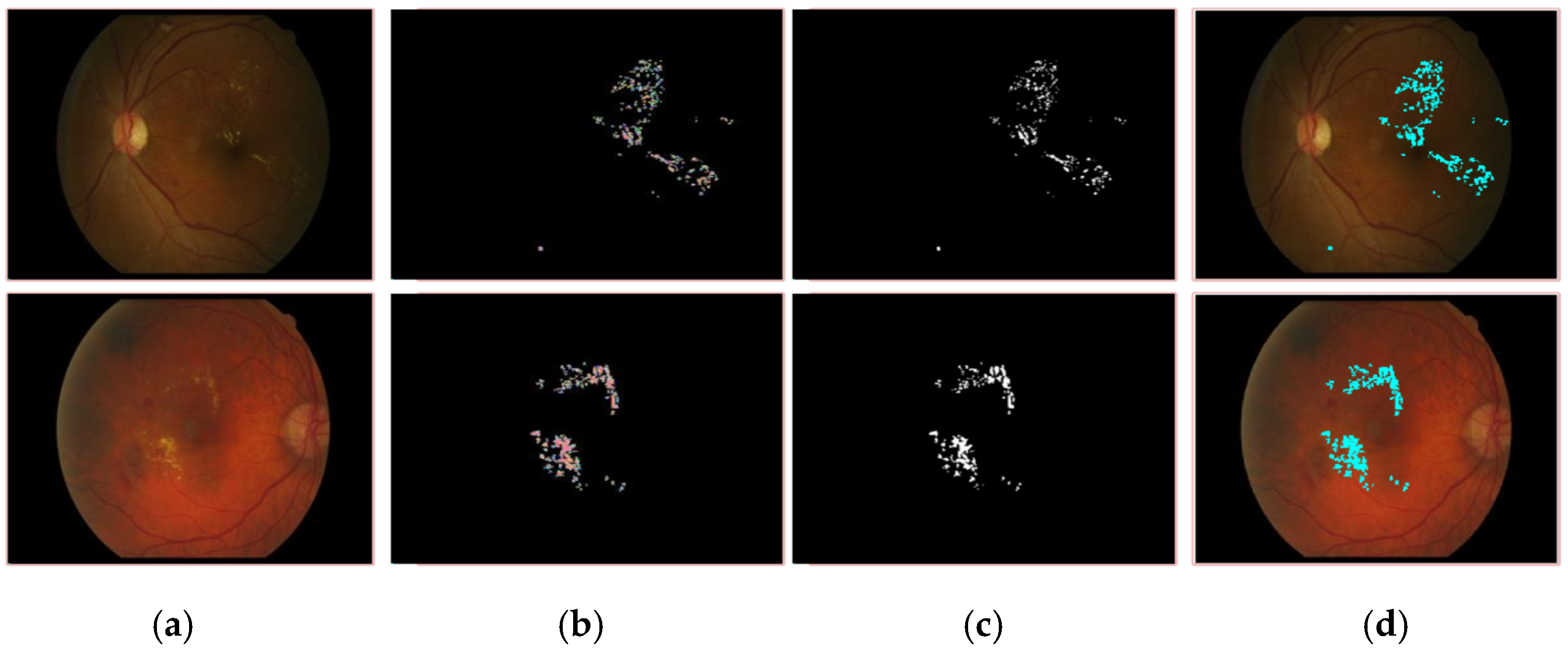
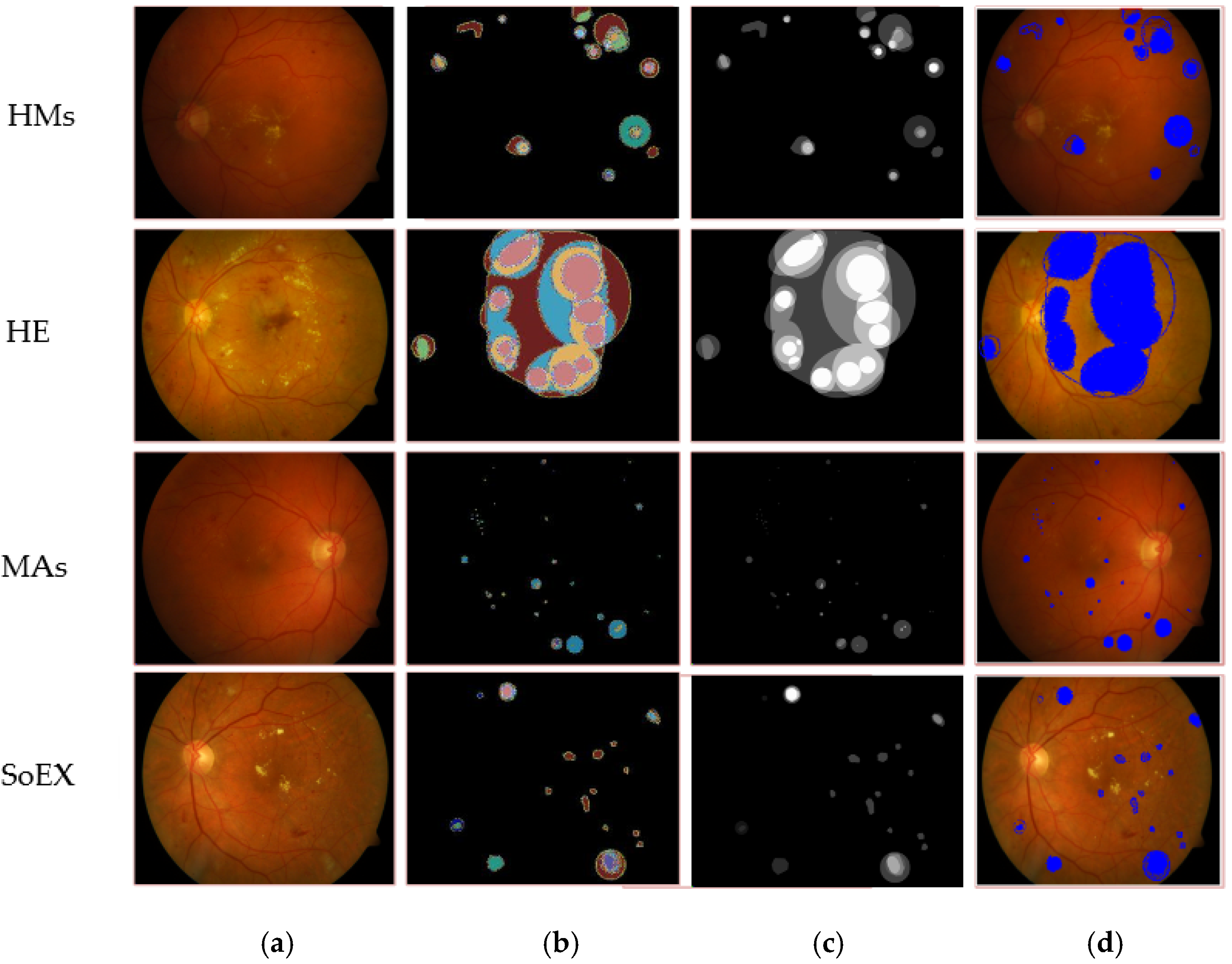
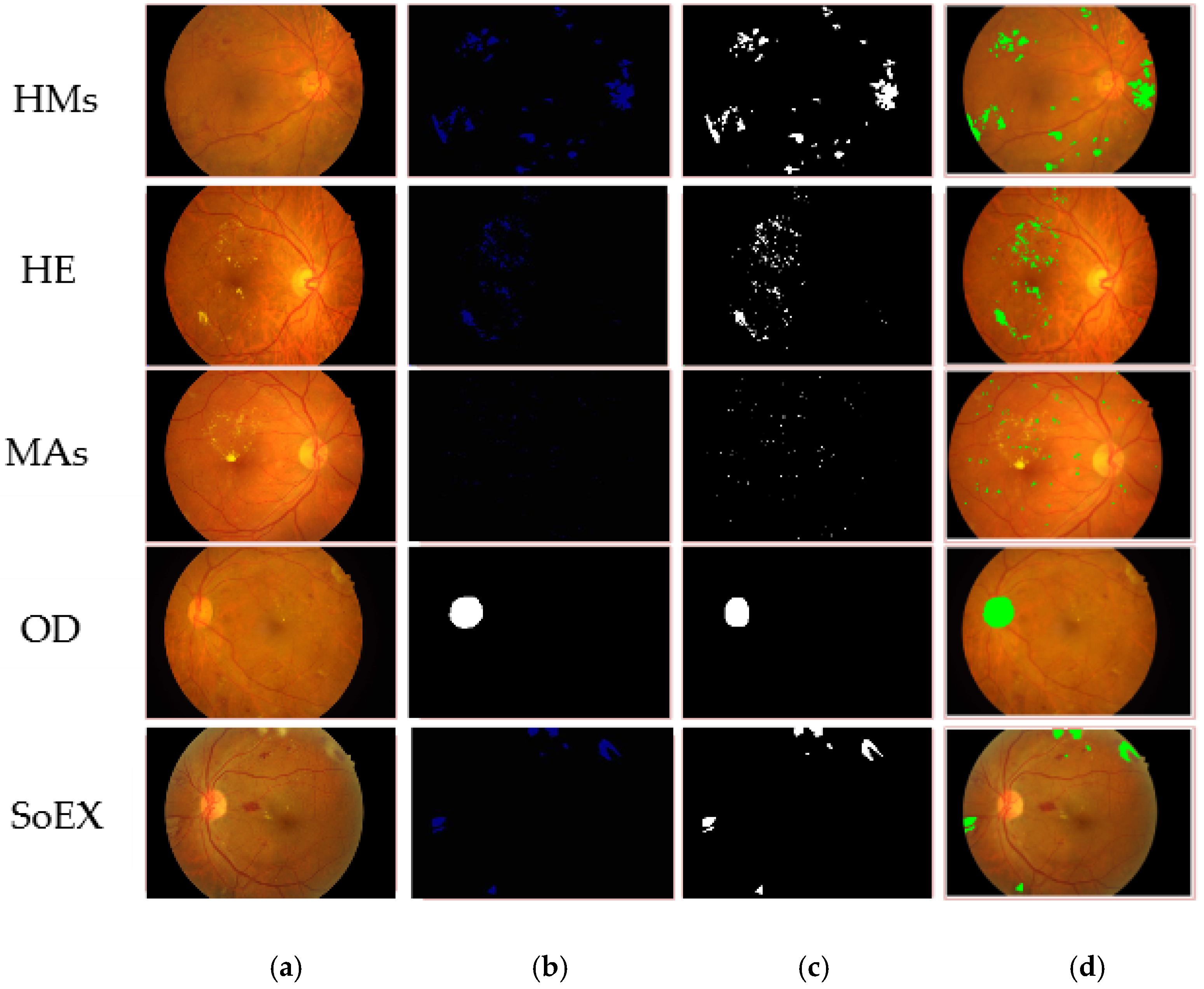
4.1. Experiment 1: DR-Lesions Segmentation
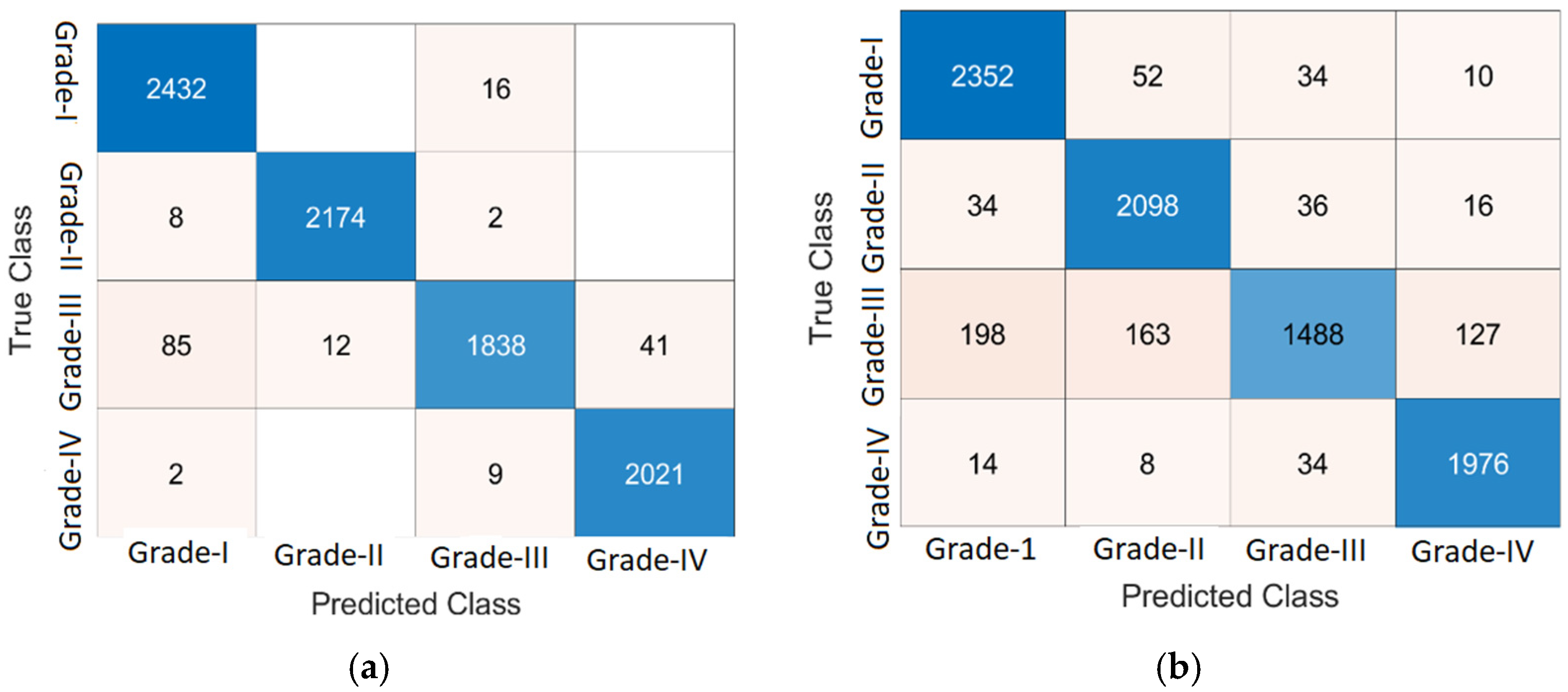
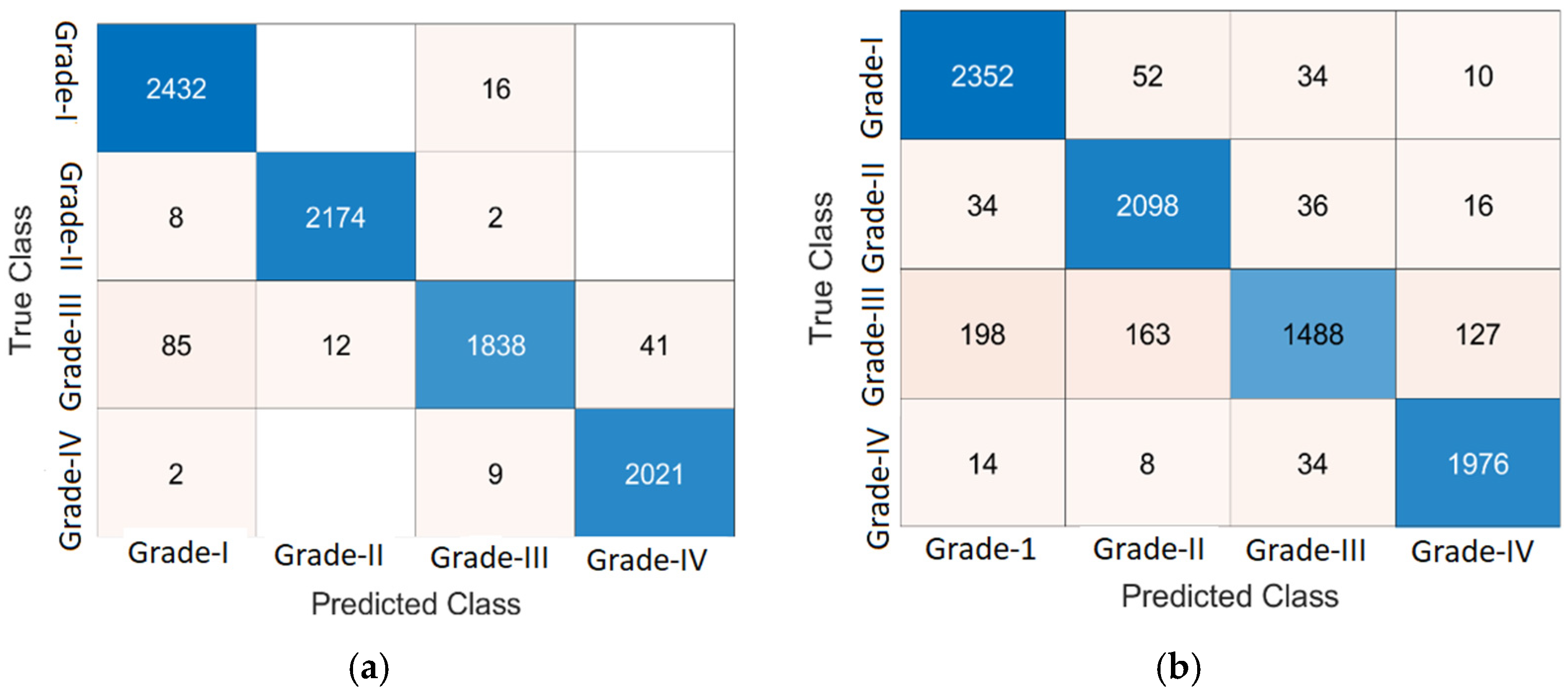
4.2. Experiment 2: DR Lesions Classification
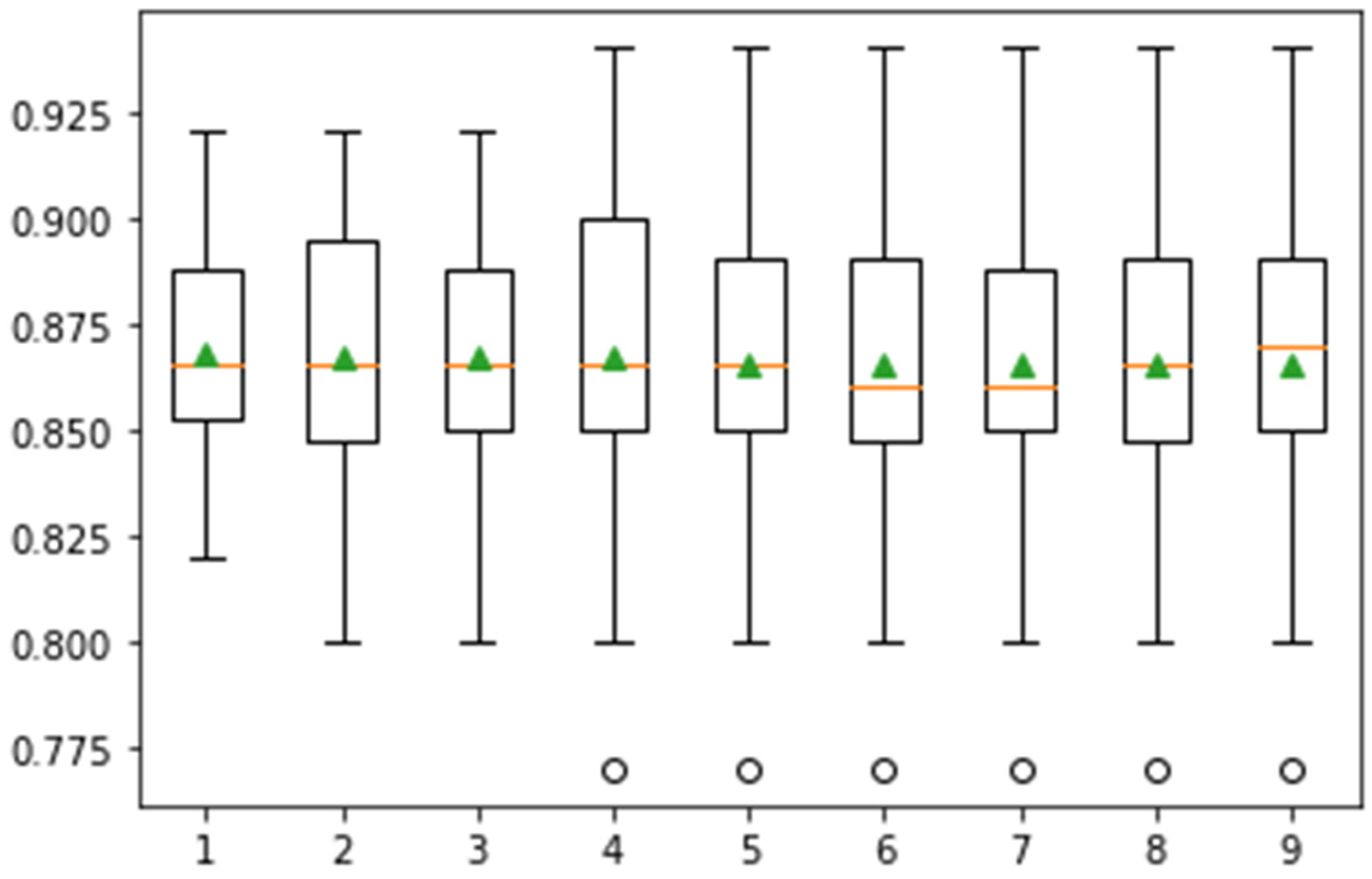
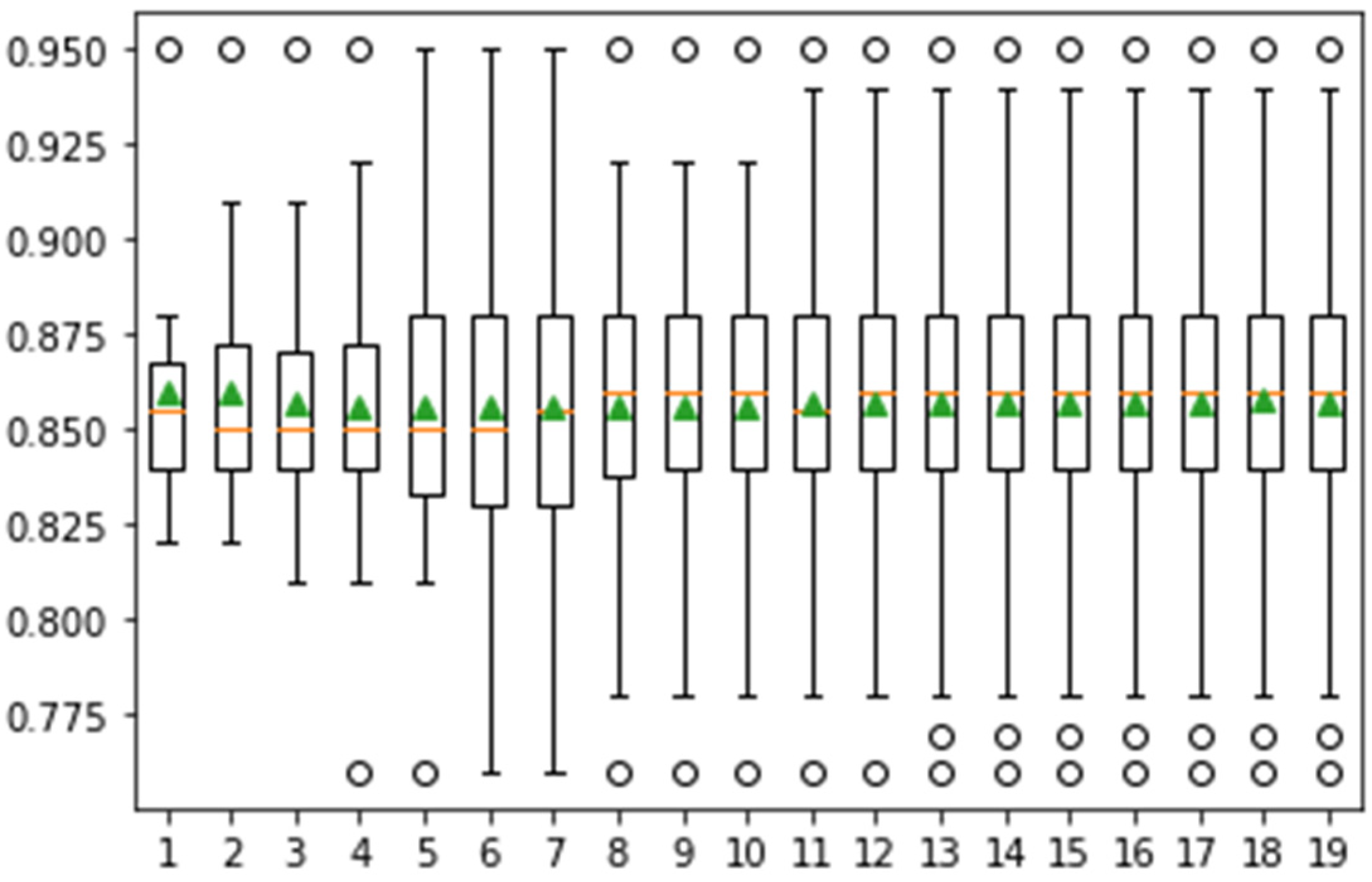
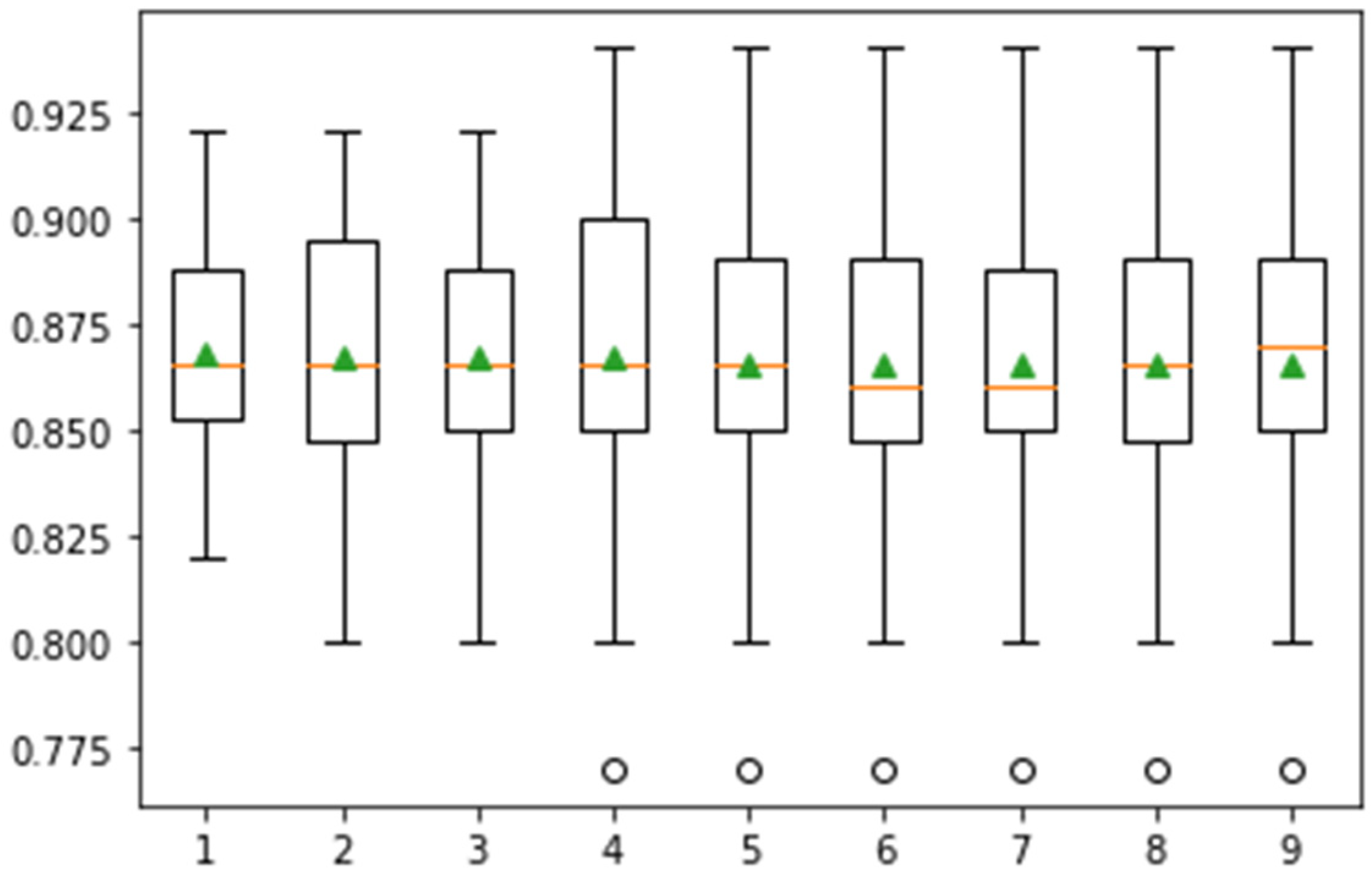
4.3. Significance Test
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Martinez-Murcia, F.J.; Ortiz, A.; Ramírez, J.; Górriz, J.M.; Cruz, R. Deep residual transfer learning for automatic diagnosis and grading of diabetic retinopathy. Neurocomputing 2021, 452, 424–434. [Google Scholar] [CrossRef]
- Amin, J.; Sharif, M.; Yasmin, M.; Ali, H.; Fernandes, S.L. A method for the detection and classification of diabetic retinopathy using structural predictors of bright lesions. J. Comput. Sci. 2017, 19, 153–164. [Google Scholar] [CrossRef]
- Amin, J.; Anjum, M.A.; Malik, M. Fused information of DeepLabv3+ and transfer learning model for semantic segmentation and rich features selection using equilibrium optimizer (EO) for classification of NPDR lesions. Knowl.-Based Syst. 2022, 249, 108881. [Google Scholar] [CrossRef]
- Wong, T.Y.; Sun, J.; Kawasaki, R.; Ruamviboonsuk, P.; Gupta, N.; Lansingh, V.C.; Maia, M.; Mathenge, W.; Moreker, S.; Muqit, M.M.; et al. Guidelines on Diabetic Eye Care: The International Council of Ophthalmology Recommendations for Screening, Follow-up, Referral, and Treatment Based on Resource Settings. Ophthalmology 2018, 125, 1608–1622. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, C.; Ferris, F.; Klein, R.; Lee, P.; Agardh, C.D.; Davis, M.; Dills, D.; Kampik, A.; Pararajasegaram, R.; Verdaguer, J.T. Proposed international clinical diabetic retinopathy and diabetic macular edema disease severity scales. Ophthalmology 2003, 110, 1677–1682. [Google Scholar] [CrossRef]
- Dubow, M.; Pinhas, A.; Shah, N.; Cooper, R.F.; Gan, A.; Gentile, R.C.; Hendrix, V.; Sulai, Y.N.; Carroll, J.; Chui, T.Y.P.; et al. Classification of Human Retinal Microaneurysms Using Adaptive Optics Scanning Light Ophthalmoscope Fluorescein Angiography. Investig. Opthalmol. Vis. Sci. 2014, 55, 1299–1309. [Google Scholar] [CrossRef]
- Murugesan, N.; Üstunkaya, T.; Feener, E.P. Thrombosis and Hemorrhage in Diabetic Retinopathy: A Perspective from an Inflammatory Standpoint. Semin. Thromb. Hemost. 2015, 41, 659–664. [Google Scholar] [CrossRef]
- Amin, J.; Sharif, M.; Yasmin, M. A Review on Recent Developments for Detection of Diabetic Retinopathy. Scientifica 2016, 2016, 6838976. [Google Scholar] [CrossRef]
- Decencière, E.; Zhang, X.; Cazuguel, G.; Lay, B.; Cochener, B.; Trone, C.; Gain, P.; Ordóñez-Varela, J.-R.; Massin, P.; Erginay, A.; et al. Feedback on a publicly distributed image database: The messidor database. Image Anal. Ster. 2014, 33, 231–234. [Google Scholar] [CrossRef]
- Mateen, M.; Wen, J.; Nasrullah, N.; Sun, S.; Hayat, S. Exudate Detection for Diabetic Retinopathy Using Pretrained Convolutional Neural Networks. Complexity 2020, 2020, 5801870. [Google Scholar] [CrossRef] [Green Version]
- Adem, K. Exudate detection for diabetic retinopathy with circular Hough transformation and convolutional neural networks. Expert Syst. Appl. 2018, 114, 289–295. [Google Scholar] [CrossRef]
- Saxena, G.; Verma, D.K.; Paraye, A.; Rajan, A.; Rawat, A. Improved and robust deep learning agent for preliminary detection of diabetic retinopathy using public datasets. Intell. Med. 2020, 3–4, 100022. [Google Scholar] [CrossRef]
- Amin, J.; Sharif, M.; Rehman, A.; Raza, M.; Mufti, M.R. Diabetic retinopathy detection and classification using hybrid feature set. Microsc. Res. Tech. 2018, 81, 990–996. [Google Scholar] [CrossRef] [PubMed]
- Koh, J.E.W.; Ng, E.Y.K.; Bhandary, S.V.; Laude, A.; Acharya, U.R. Automated detection of retinal health using PHOG and SURF features extracted from fundus images. Appl. Intell. 2017, 48, 1379–1393. [Google Scholar] [CrossRef]
- Nazir, T.; Irtaza, A.; Shabbir, Z.; Javed, A.; Akram, U.; Mahmood, M.T. Diabetic retinopathy detection through novel tetragonal local octa patterns and extreme learning machines. Artif. Intell. Med. 2019, 99, 101695. [Google Scholar] [CrossRef] [PubMed]
- Sungheetha, A.; Sharma, R. Design an early detection and classification for diabetic retinopathy by deep feature extraction based convolution neural network. J. Trends Comput. Sci. Smart Technol. 2021, 3, 81–94. [Google Scholar] [CrossRef]
- Shanthi, T.; Sabeenian, R. Modified Alexnet architecture for classification of diabetic retinopathy images. Comput. Electr. Eng. 2019, 76, 56–64. [Google Scholar] [CrossRef]
- Sambyal, N.; Saini, P.; Syal, R.; Gupta, V. Modified U-Net architecture for semantic segmentation of diabetic retinopathy images. Biocybern. Biomed. Eng. 2020, 40, 1094–1109. [Google Scholar] [CrossRef]
- Sambyal, N.; Saini, P.; Syal, R.; Gupta, V. Modified residual networks for severity stage classification of diabetic retinopathy. Evol. Syst. 2022, 163, 1–19. [Google Scholar] [CrossRef]
- Xiao, Q.; Zou, J.; Yang, M.; Gaudio, A.; Kitani, K.; Smailagic, A.; Costa, P.; Xu, M. Improving Lesion Segmentation for Diabetic Retinopathy Using Adversarial Learning. In Image Analysis and Recognition; Springer Nature Switzerland AG: Cham, Switzerland, 2019; pp. 333–344. [Google Scholar] [CrossRef]
- Amin, J.; Sharif, M.; Yasmin, M.; Fernandes, S.L. A distinctive approach in brain tumor detection and classification using MRI. Pattern Recognit. Lett. 2017, 139, 118–127. [Google Scholar] [CrossRef]
- Sharif, M.I.; Li, J.P.; Amin, J.; Sharif, A. An improved framework for brain tumor analysis using MRI based on YOLOv2 and convolutional neural network. Complex Intell. Syst. 2021, 7, 2023–2036. [Google Scholar] [CrossRef]
- Saba, T.; Mohamed, A.S.; El-Affendi, M.; Amin, J.; Sharif, M. Brain tumor detection using fusion of hand crafted and deep learning features. Cogn. Syst. Res. 2019, 59, 221–230. [Google Scholar] [CrossRef]
- Amin, J.; Sharif, M.; Raza, M.; Saba, T.; Anjum, M.A. Brain tumor detection using statistical and machine learning method. Comput. Methods Programs Biomed. 2019, 177, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Amin, J.; Sharif, M.; Raza, M.; Yasmin, M. Detection of Brain Tumor based on Features Fusion and Machine Learning. J. Ambient Intell. Humaniz. Comput. 2018, 1274, 1–17. [Google Scholar] [CrossRef]
- Amin, J.; Sharif, M.; Gul, N.; Yasmin, M.; Shad, S.A. Brain tumor classification based on DWT fusion of MRI sequences using convolutional neural network. Pattern Recognit. Lett. 2019, 129, 115–122. [Google Scholar] [CrossRef]
- Sharif, M.; Amin, J.; Raza, M.; Yasmin, M.; Satapathy, S.C. An integrated design of particle swarm optimization (PSO) with fusion of features for detection of brain tumor. Pattern Recognit. Lett. 2019, 129, 150–157. [Google Scholar] [CrossRef]
- Amin, J.; Sharif, M.; Yasmin, M.; Saba, T.; Anjum, M.A.; Fernandes, S.L. A New Approach for Brain Tumor Segmentation and Classification Based on Score Level Fusion Using Transfer Learning. J. Med. Syst. 2019, 43, 326. [Google Scholar] [CrossRef]
- Amin, J.; Sharif, M.; Raza, M.; Saba, T.; Sial, R.; Shad, S.A. Brain tumor detection: A long short-term memory (LSTM)-based learning model. Neural Comput. Appl. 2019, 32, 15965–15973. [Google Scholar] [CrossRef]
- Amin, J.; Sharif, M.; Raza, M.; Saba, T.; Rehman, A. Brain tumor classification: Feature fusion. In Proceedings of the 2019 International Conference on Computer and Information Sciences (ICCIS), Aljouf, Saudi Arabia, 3–4 April 2019; pp. 1–6. [Google Scholar]
- Amin, J.; Sharif, M.; Yasmin, M.; Saba, T.; Raza, M. Use of machine intelligence to conduct analysis of human brain data for detection of abnormalities in its cognitive functions. Multimedia Tools Appl. 2019, 79, 10955–10973. [Google Scholar] [CrossRef]
- Amin, J.; Sharif, A.; Gul, N.; Anjum, M.A.; Nisar, M.W.; Azam, F.; Bukhari, S.A.C. Integrated design of deep features fusion for localization and classification of skin cancer. Pattern Recognit. Lett. 2019, 131, 63–70. [Google Scholar] [CrossRef]
- Amin, J.; Sharif, M.; Gul, N.; Raza, M.; Anjum, M.A.; Nisar, M.W.; Bukhari, S.A.C. Brain Tumor Detection by Using Stacked Autoencoders in Deep Learning. J. Med. Syst. 2019, 44, 32. [Google Scholar] [CrossRef]
- Sharif, M.; Amin, J.; Raza, M.; Anjum, M.A.; Afzal, H.; Shad, S.A. Brain tumor detection based on extreme learning. Neural Comput. Appl. 2020, 32, 15975–15987. [Google Scholar] [CrossRef]
- Amin, J.; Sharif, M.; Anjum, M.A.; Raza, M.; Bukhari, S.A.C. Convolutional neural network with batch normalization for glioma and stroke lesion detection using MRI. Cogn. Syst. Res. 2019, 59, 304–311. [Google Scholar] [CrossRef]
- Muhammad, N.; Sharif, M.; Amin, J.; Mehboob, R.; Gilani, S.A.; Bibi, N.; Javed, H.; Ahmed, N. Neurochemical Alterations in Sudden Unexplained Perinatal Deaths—A Review. Front. Pediatr. 2018, 6, 6. [Google Scholar] [CrossRef] [PubMed]
- Sharif, M.; Amin, J.; Nisar, M.W.; Anjum, M.A.; Muhammad, N.; Shad, S. A unified patch based method for brain tumor detection using features fusion. Cogn. Syst. Res. 2019, 59, 273–286. [Google Scholar] [CrossRef]
- Sharif, M.; Amin, J.; Siddiqa, A.; Khan, H.U.; Malik, M.S.A.; Anjum, M.A.; Kadry, S. Recognition of Different Types of Leukocytes Using YOLOv2 and Optimized Bag-of-Features. IEEE Access 2020, 8, 167448–167459. [Google Scholar] [CrossRef]
- Anjum, M.A.; Amin, J.; Sharif, M.; Khan, H.U.; Malik, M.S.A.; Kadry, S. Deep Semantic Segmentation and Multi-Class Skin Lesion Classification Based on Convolutional Neural Network. IEEE Access 2020, 8, 129668–129678. [Google Scholar] [CrossRef]
- Sharif, M.; Amin, J.; Yasmin, M.; Rehman, A. Efficient hybrid approach to segment and classify exudates for DR prediction. Multimedia Tools Appl. 2018, 79, 11107–11123. [Google Scholar] [CrossRef]
- Amin, J.; Sharif, M.; Anjum, M.A.; Khan, H.U.; Malik, M.S.A.; Kadry, S. An Integrated Design for Classification and Localization of Diabetic Foot Ulcer Based on CNN and YOLOv2-DFU Models. IEEE Access 2020, 8, 228586–228597. [Google Scholar] [CrossRef]
- Amin, J.; Sharif, M.; Yasmin, M. Segmentation and classification of lung cancer: A review. Immunol. Endocr. Metab. Agents Med. Chem. 2016, 16, 82–99. [Google Scholar] [CrossRef]
- Umer, M.J.; Amin, J.; Sharif, M.; Anjum, M.A.; Azam, F.; Shah, J.H. An integrated framework for COVID -19 classification based on classical and quantum transfer learning from a chest radiograph. Concurr. Comput. Pract. Exp. 2021, 34, e6434. [Google Scholar] [CrossRef] [PubMed]
- Amin, J.; Anjum, M.A.; Sharif, M.; Saba, T.; Tariq, U. An intelligence design for detection and classification of COVID19 using fusion of classical and convolutional neural network and improved microscopic features selection approach. Microsc. Res. Tech. 2021, 84, 2254–2267. [Google Scholar] [CrossRef] [PubMed]
- Amin, J.; Sharif, M.; Anjum, M.A.; Siddiqa, A.; Kadry, S.; Nam, Y.; Raza, M. 3D Semantic Deep Learning Networks for Leukemia Detection. Comput. Mater. Contin. 2021, 69, 785–799. [Google Scholar] [CrossRef]
- Amin, J.; Anjum, M.A.; Sharif, M.; Kadry, S.; Nam, Y.; Wang, S. Convolutional Bi-LSTM Based Human Gait Recognition Using Video Sequences. Comput. Mater. Contin. 2021, 68, 2693–2709. [Google Scholar] [CrossRef]
- Amin, J.; Anjum, M.A.; Sharif, M.; Rehman, A.; Saba, T.; Zahra, R. Microscopic segmentation and classification of COVID -19 infection with ensemble convolutional neural network. Microsc. Res. Tech. 2021, 85, 385–397. [Google Scholar] [CrossRef]
- Saleem, S.; Amin, J.; Sharif, M.; Anjum, M.A.; Iqbal, M.; Wang, S.-H. A deep network designed for segmentation and classification of leukemia using fusion of the transfer learning models. Complex Intell. Syst. 2022, 8, 3105–3120. [Google Scholar] [CrossRef]
- Amin, J.; Anjum, M.A.; Sharif, M.; Kadry, S.; Nam, Y. Fruits and Vegetable Diseases Recognition Using Convolutional Neural Networks. Comput. Mater. Contin. 2022, 70, 619–635. [Google Scholar] [CrossRef]
- Linsky, T.W.; Vergara, R.; Codina, N.; Nelson, J.W.; Walker, M.J.; Su, W.; Barnes, C.O.; Hsiang, T.Y.; Esser-Nobis, K.; Yu, K.; et al. De novo design of potent and resilient hACE2 decoys to neutralize SARS-CoV-2. Science 2020, 370, 1208–1214. [Google Scholar] [CrossRef]
- Feng, Z.; Yang, J.; Yao, L.; Qiao, Y.; Yu, Q.; Xu, X. Deep Retinal Image Segmentation: A FCN-Based Architecture with Short and Long Skip Connections for Retinal Image Segmentation. In Proceedings of the International Conference on Neural Information Processing, Guangzhou, China, 14–18 November 2017; Springer: Berlin/Heidelberg, Germany, 2017; pp. 713–722. [Google Scholar] [CrossRef]
- Qomariah, D.; Nopember, I.T.S.; Tjandrasa, H.; Fatichah, C. Segmentation of Microaneurysms for Early Detection of Diabetic Retinopathy Using MResUNet. Int. J. Intell. Eng. Syst. 2021, 14, 359–373. [Google Scholar] [CrossRef]
- Guo, Y.; Peng, Y. Multiple lesion segmentation in diabetic retinopathy with dual-input attentive RefineNet. Appl. Intell. 2022, 344, 1–25. [Google Scholar] [CrossRef]
- Kundu, S.; Karale, V.; Ghorai, G.; Sarkar, G.; Ghosh, S.; Dhara, A.K. Nested U-Net for Segmentation of Red Lesions in Retinal Fundus Images and Sub-image Classification for Removal of False Positives. J. Digit. Imaging, 2022; epub ahead of print. [Google Scholar] [CrossRef]
- Wan, C.; Chen, Y.; Li, H.; Zheng, B.; Chen, N.; Yang, W.; Wang, C.; Li, Y. EAD-Net: A Novel Lesion Segmentation Method in Diabetic Retinopathy Using Neural Networks. Dis. Markers 2021, 2021, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, M.; Fraz, M.M.; Barman, S. Localization and segmentation of optic disc in retinal images using Circular Hough transform and Grow Cut algorithm. PeerJ 2016, 4, e2003. [Google Scholar] [CrossRef] [PubMed]
- Chollet, F. Xception: Deep learning with depthwise separable convolutions. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 1251–1258. [Google Scholar]
- Tan, M.; Le, Q. EfficientNet: Rethinking model scaling for convolutional neural networks. Int. Conf. Mach. Learn. 2019, 6105–6114. [Google Scholar]
- Iandola, F.N.; Han, S.; Moskewicz, M.W.; Ashraf, K.; Dally, W.J.; Keutzer, K. SqueezeNet: AlexNet-level accuracy with 50x fewer parameters and <0.5 MB model size. arXiv 2016, arXiv:1602.07360. [Google Scholar]
- Balakrishnan, K.; Dhanalakshmi, R.; Khaire, U.M. Analysing stable feature selection through an augmented marine predator algorithm based on opposition-based learning. Expert Syst. 2021, 39, e12816. [Google Scholar] [CrossRef]
- Soomro, T.A.; Zheng, L.; Afifi, A.J.; Ali, A.; Soomro, S.; Yin, M.; Gao, J. Image Segmentation for MR Brain Tumor Detection Using Machine Learning: A Review. IEEE Rev. Biomed. Eng. 2022, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Gardoll, S.; Boucher, O. Classification of tropical cyclone containing images using a convolutional neural network: Performance and sensitivity to the learning dataset. EGUsphere 2022, preprint. [Google Scholar] [CrossRef]
- Chen, L.-C.; Zhu, Y.; Papandreou, G.; Schroff, F.; Adam, H. Encoder-decoder with atrous separable convolution for semantic image segmentation. In Proceedings of the European Conference on Computer Vision (ECCV), Munich, Germany, 8–14 September 2018; pp. 801–818. [Google Scholar]
- Kauppi, T.; Kalesnykiene, V.; Kamarainen, J.-K.; Lensu, L.; Sorri, I.; Raninen, A.; Voutilainen, R.; Uusitalo, H.; Kalviainen, H.; Pietila, J. The diaretdb1 diabetic retinopathy database and evaluation protocol. In Proceedings of the British Machine Vision Conference 2007, Coventry, UK, 10–13 September 2007; pp. 61–65. [Google Scholar] [CrossRef]
- Decencière, E.; Cazuguel, G.; Zhang, X.; Thibault, G.; Klein, J.-C.; Meyer, F.; Marcotegui, B.; Quellec, G.; Lamard, M.; Danno, R.; et al. TeleOphta: Machine learning and image processing methods for teleophthalmology. IRBM 2013, 34, 196–203. [Google Scholar] [CrossRef]
- Porwal, P.; Pachade, S.; Kamble, R.; Kokare, M.; Deshmukh, G.; Sahasrabuddhe, V.; Meriaudeau, F. Indian diabetic retinopathy image dataset (IDRiD): A database for diabetic retinopathy screening research. Data 2018, 3, 25. [Google Scholar] [CrossRef]
- Xu, Y.; Zhou, Z.; Li, X.; Zhang, N.; Zhang, M.; Wei, P. FFU-Net: Feature Fusion U-Net for Lesion Segmentation of Diabetic Retinopathy. BioMed Res. Int. 2021, 2021, 1–12. [Google Scholar] [CrossRef]
- Valizadeh, A.; Ghoushchi, S.J.; Ranjbarzadeh, R.; Pourasad, Y. Presentation of a Segmentation Method for a Diabetic Retinopathy Patient’s Fundus Region Detection Using a Convolutional Neural Network. Comput. Intell. Neurosci. 2021, 2021, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Jadhav, M.L.; Shaikh, M.Z.; Sardar, V.M. Automated Microaneurysms Detection in Fundus Images for Early Diagnosis of Diabetic Retinopathy. In Data Engineering and Intelligent Computing; Springer: Singapore, 2021; pp. 87–95. [Google Scholar] [CrossRef]
- Sharma, A.; Shinde, S.; Shaikh, I.I.; Vyas, M.; Rani, S. Machine Learning Approach for Detection of Diabetic Retinopathy with Improved Pre-Processing. In Proceedings of the 2021 International Conference on Computing, Communication, and Intelligent Systems (ICCCIS), Greater Noida, India, 19–20 February 2021; pp. 517–522. [Google Scholar] [CrossRef]
- Nneji, G.U.; Cai, J.; Deng, J.; Monday, H.N.; Hossin, A.; Nahar, S. Identification of Diabetic Retinopathy Using Weighted Fusion Deep Learning Based on Dual-Channel Fundus Scans. Diagnostics 2022, 12, 540. [Google Scholar] [CrossRef] [PubMed]
- Kalyani, G.; Janakiramaiah, B.; Karuna, A.; Prasad, L.V.N. Diabetic retinopathy detection and classification using capsule networks. Complex Intell. Syst. 2021, 2821, 1–14. [Google Scholar] [CrossRef]
- Gangwar, A.K.; Ravi, V. Diabetic Retinopathy Detection Using Transfer Learning and Deep Learning. In Evolution in Computational Intelligence; Springer: Singapore, 2020; pp. 679–689. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Optimizer | Epochs for Training | Size Batch | Learning Rate | Error Rate |
|---|---|---|---|---|
| Sgdm | 200 | 32 | 0.0001 | 0.02 |
| Adam | 16 | 0.04 | ||
| RmsProp | 8 | 0.06 | ||
| Momentum | 64 | 0.07 |
| Lower Bound (lb) | 0 |
| Upper Bound (ub) | 1 |
| Threshold (thres) | 0.5 |
| Levy Component (beta) | 1.5 |
| Constant (P) | 0.5 |
| Fish Aggregating Devices Effect (FADs) | 0.2 |
| DR Levels | Description | Grades |
|---|---|---|
| Normal | Healthy | 0 |
| Mild (NPDR) | Mas | 1 |
| Moderate (NPDR) | Few MAs or HMs | 2 |
| PDR | More MAs and HMs | 3 |
| Datasets | Description |
|---|---|
| DIARETDB1 | Total images:89 Normal:5 Mild NPDR:84 |
| e-ophtha-EX | Normal: 35 Exudates:47 |
| IDRiD | MAs:81 HE:81 HMs:80 SoEX:40 |
| Datasets | Lesions | mIoU | mDice | F1-Score | Precision (P) | Recall | Accuracy (Acc) |
|---|---|---|---|---|---|---|---|
| e-ophtha-EX | EX | 0.94 | 0.97 | 0.98 | 0.94 | 0.99 | 0.96 |
| DIARETDB1 | HM | 0.87 | 0.83 | 0.72 | 0.87 | 0.99 | 0.87 |
| HE | 0.71 | 0.83 | 0.92 | 0.71 | 0.99 | 0.71 | |
| MA | 0.87 | 0.83 | 0.72 | 0.87 | 0.99 | 0.87 | |
| SE | 0.86 | 0.88 | 0.87 | 0.86 | 1.00 | 0.86 | |
| IDRiD | HM | 0.86 | 0.88 | 0.88 | 0.86 | 1.00 | 0.86 |
| HE | 0.88 | 0.84 | 0.81 | 0.88 | 1.00 | 0.88 | |
| MA | 0.71 | 0.83 | 0.92 | 0.71 | 1.00 | 0.71 | |
| OD | 0.86 | 0.87 | 0.87 | 0.86 | 1.00 | 0.86 | |
| SE | 0.84 | 0.83 | 0.82 | 0.87 | 0.98 | 0.97 |
| Ref | Year | Method | Dataset | Results |
|---|---|---|---|---|
| [53] | 2022 | Dual-input attentive RefineNet (DARNet) | IDRiD | 0.95 Acc |
| [67] | 2021 | U-Net | 0.87 Sensitivity | |
| [68] | 2021 | U-Net | 0.83 Acc | |
| [69] | 2021 | SVM | 0.80 Acc | |
| Proposed Model | 0.96 Acc, 0.98 Sensitivity | |||
| [53] | 2022 | DARNet | E-ophtha-EX | 0.96 Acc |
| Proposed Model | 0.97 Acc | |||
| [54] | 2022 | Nested U-Net | DIARETDB1 | 0.88 Sensitivity |
| [52] | 2021 | MResUNet | 0.61 Sensitivity | |
| [70] | 2020 | U-Net | 0.85 Sensitivity | |
| Proposed Model | 0.99 Sensitivity | |||
| Grade | Accuracy | Precision | Recall | F1 Score | Overall Accuracy | |
|---|---|---|---|---|---|---|
| Weighted KNN | 0 | 86.57% | 1.00 | 0.68 | 0.81 | 84.87% |
| 1 | 97.08% | 0.94 | 0.94 | 0.94 | ||
| 2 | 87.77% | 0.47 | 1.00 | 0.64 | ||
| 3 | 98.32% | 0.94 | 0.99 | 0.96 | ||
| Optimizable KNN | 0 | 98.72% | 0.99 | 0.96 | 0.98 | 97.97% |
| 1 | 99.75% | 1.00 | 0.99 | 0.99 | ||
| 2 | 98.09% | 0.93 | 0.99 | 0.96 | ||
| 3 | 99.40% | 0.99 | 0.98 | 0.99 | ||
| Cosine KNN | 0 | 96.75% | 0.99 | 0.91 | 0.95 | 93.66% |
| 1 | 95.56% | 0.84 | 0.99 | 0.90 | ||
| 2 | 96.53% | 0.94 | 0.91 | 0.93 | ||
| 3 | 98.48% | 0.98 | 0.96 | 0.97 | ||
| Fine KNN | 0 | 97.94% | 1.00 | 0.94 | 0.96 | 97.13% |
| 1 | 99.29% | 0.99 | 0.98 | 0.99 | ||
| 2 | 97.73% | 0.91 | 0.99 | 0.95 | ||
| 3 | 99.29% | 0.98 | 0.99 | 0.98 |
| Narrow Neural Network | Grade | Accuracy | Precision | Recall | F1 Score | Overall Accuracy |
| 0 | 95.80% | 0.96 | 0.90 | 0.93 | 89.31% | |
| 1 | 95.67% | 0.96 | 0.88 | 0.92 | ||
| 2 | 90.94% | 0.67 | 0.91 | 0.77 | ||
| 3 | 96.20% | 0.97 | 0.88 | 0.92 | ||
| Medium Neural Network | 0 | 95.78% | 0.96 | 0.90 | 0.93 | 90.65% |
| 1 | 96.38% | 0.96 | 0.91 | 0.93 | ||
| 2 | 92.11% | 0.72 | 0.92 | 0.81 | ||
| 3 | 97.04% | 0.97 | 0.91 | 0.94 | ||
| Wide Neural Network | 0 | 96.04% | 0.96 | 0.91 | 0.93 | 91.60% |
| 1 | 96.42% | 0.96 | 0.90 | 0.93 | ||
| 2 | 93.15% | 0.75 | 0.93 | 0.83 | ||
| 3 | 97.58% | 0.97 | 0.93 | 0.95 | ||
| Bilayered Neural Network | 0 | 95.35% | 0.95 | 0.89 | 0.92 | 88.87% |
| 1 | 95.56% | 0.95 | 0.88 | 0.92 | ||
| 2 | 90.47% | 0.67 | 0.89 | 0.76 | ||
| 3 | 96.35% | 0.96 | 0.89 | 0.93 | ||
| Trilayered Neural Network | 0 | 94.12% | 0.94 | 0.86 | 0.90 | 87.33% |
| 1 | 95.34% | 0.95 | 0.88 | 0.91 | ||
| 2 | 89.04% | 0.61 | 0.87 | 0.72 | ||
| 3 | 96.16% | 0.96 | 0.89 | 0.92 |
| Ref# | Year | Method | Dataset | Overall Acc% | Grade-0% | Grade-1% | Grade-2% | Grade-3% |
|---|---|---|---|---|---|---|---|---|
| [71] | 2022 | WFDLN | Messidor | 0.98 | - | - | - | - |
| [17] | 2019 | Modified Alexnet | - | 0.96 | 0.96 | 0.95 | 0.96 | |
| [1] | 2021 | ResNet50 | - | 0.93 | 0.93 | 0.81 | 0.92 | |
| [72] | 2021 | CapsNet | - | 0.97 | 0.97 | 0.97 | 0.98 | |
| [73] | 2021 | Inception-ResNet-v2 | 0.72 | - | - | - | - | |
| Proposed method | 0.99 | 0.98 | 0.99 | 0.98 | 0.99 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shaukat, N.; Amin, J.; Sharif, M.; Azam, F.; Kadry, S.; Krishnamoorthy, S. Three-Dimensional Semantic Segmentation of Diabetic Retinopathy Lesions and Grading Using Transfer Learning. J. Pers. Med. 2022, 12, 1454. https://doi.org/10.3390/jpm12091454
Shaukat N, Amin J, Sharif M, Azam F, Kadry S, Krishnamoorthy S. Three-Dimensional Semantic Segmentation of Diabetic Retinopathy Lesions and Grading Using Transfer Learning. Journal of Personalized Medicine. 2022; 12(9):1454. https://doi.org/10.3390/jpm12091454
Chicago/Turabian StyleShaukat, Natasha, Javeria Amin, Muhammad Sharif, Faisal Azam, Seifedine Kadry, and Sujatha Krishnamoorthy. 2022. "Three-Dimensional Semantic Segmentation of Diabetic Retinopathy Lesions and Grading Using Transfer Learning" Journal of Personalized Medicine 12, no. 9: 1454. https://doi.org/10.3390/jpm12091454
APA StyleShaukat, N., Amin, J., Sharif, M., Azam, F., Kadry, S., & Krishnamoorthy, S. (2022). Three-Dimensional Semantic Segmentation of Diabetic Retinopathy Lesions and Grading Using Transfer Learning. Journal of Personalized Medicine, 12(9), 1454. https://doi.org/10.3390/jpm12091454