
Problem-Solving Treatment for People Recently Diagnosed with Visual Impairment: Pilot Randomised Controlled Trial

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
Participants
- adults (≥18 years of age);
- community-dwelling (i.e., not living in a care home);
- diagnosed with severe, irreversible sight loss, or registered as sight impaired (partially sighted) or severely sight impaired (blind) within the previous 3 months.
2.2. Procedure
2.3. Outcomes and Assessments
- (i)
- psychological distress, as measured by the Hospital Anxiety and Depression Scale [20];
- (ii)
- (iii)
- (iv)
- problem-solving ability, measured by the Social Problem Solving Inventory—Revised: Short [25];
- (v)
- self-efficacy, measured by the Generalized Self-efficacy Scale [26].
2.3.1. Randomisation Procedures
2.3.2. Intervention and Control Groups
2.4. Statistical Methods
3. Results
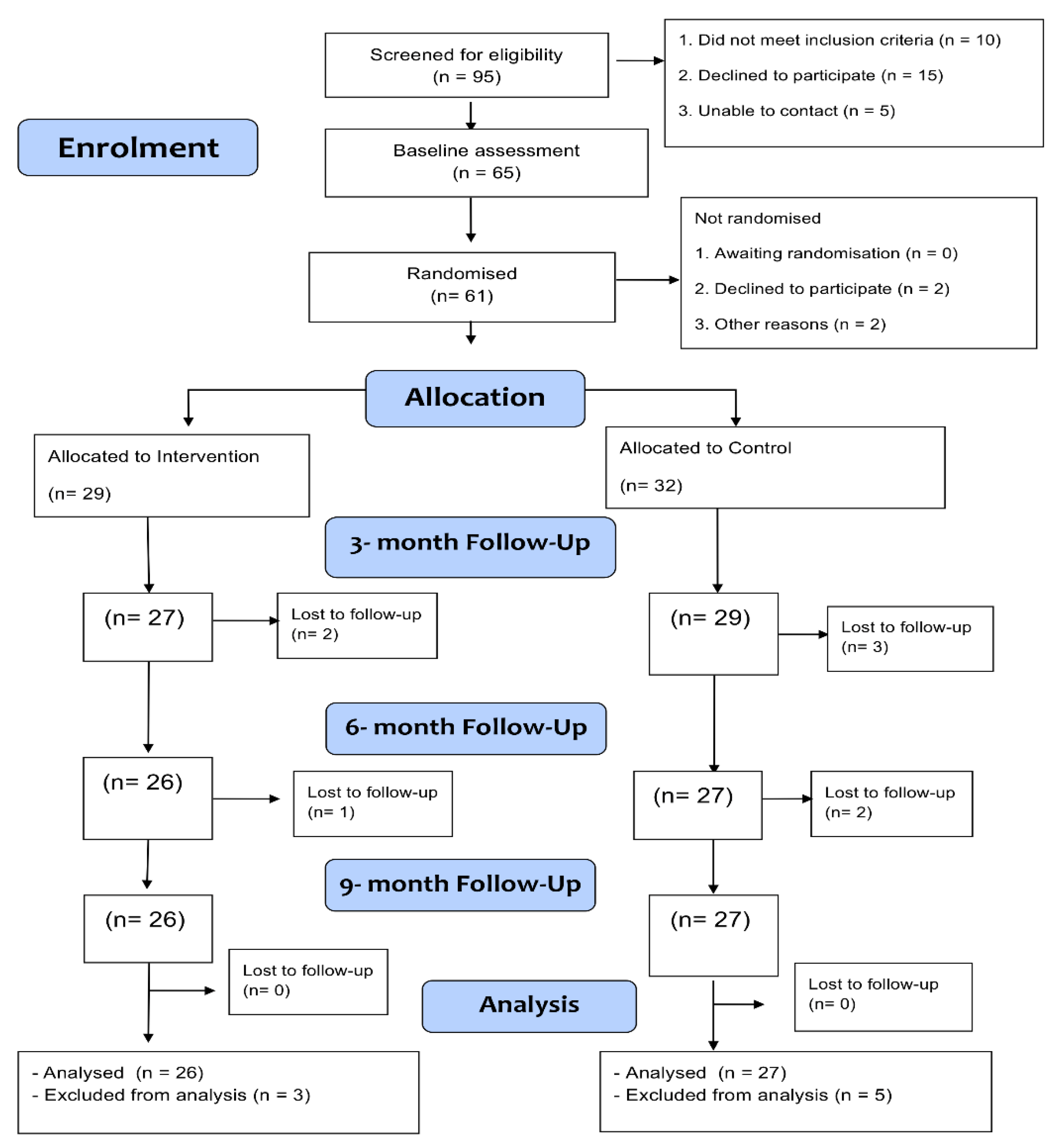
3.1. Recruitment and Retention
3.2. Participants
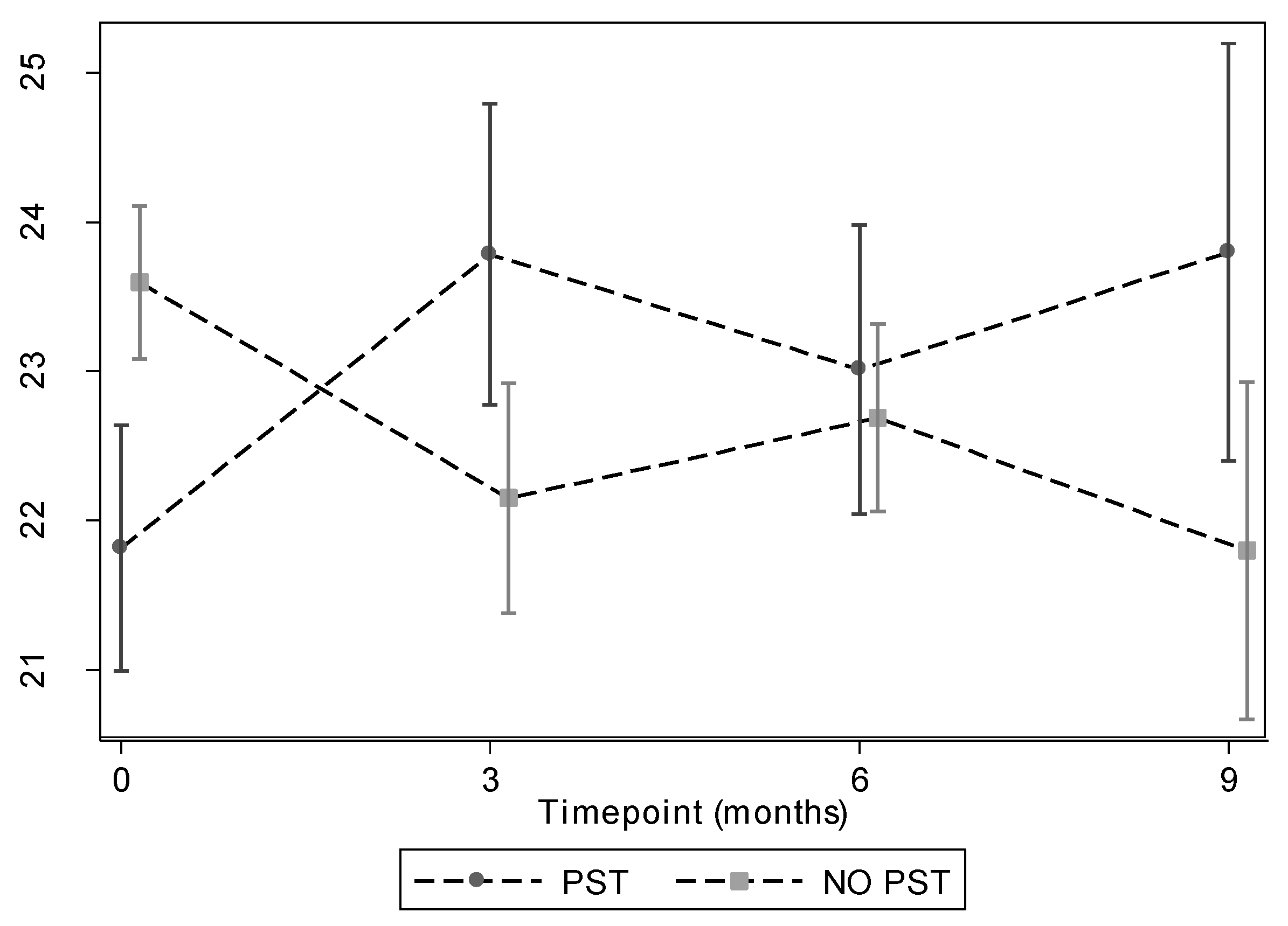
3.3. Primary Outcome Analyses
3.4. Secondary Outcome Analyses
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Evans, J.R.; Fletcher, A.E.; Wormald, R.P.L. Depression and anxiety in visually impaired older people. Ophthalmology 2007, 114, 283–288. [Google Scholar] [CrossRef]
- Horowitz, A.; Reinhardt, J.P. Mental health issues in visual impairment: Research in depression, disability, and rehabilitation. In The Lighthouse Handbook on Vision Impairment and Rehabilitation: Volume II—Vision Rehabilitation; Silverstone, B.M., Lang, M., Rosenthal, R., Faye, E., Eds.; Oxford University Press: New York, NY, USA, 2000. [Google Scholar]
- De Leo, D.; Hickey, P.A.; Meneghel, G.; Cantor, C.H. Blindness, fear of sight loss, and suicide. Psychosomatics 1999, 40, 339–344. [Google Scholar] [CrossRef]
- Orr, A.L. The Psychosocial Aspects of Aging and Vision Loss. J. Gerontol. Soc. Work 1991, 17, 1–14. [Google Scholar] [CrossRef]
- Scott, I.U.; Smiddy, W.E.; Schiffman, J.; Feuer, W.J.; Pappas, C.J. Quality of life of low-vision patients and the impact of low-vision services. Am. J. Ophthalmol. 1999, 128, 54–62. [Google Scholar] [CrossRef]
- Mynors-Wallis, L.M.; Gath, D.H.; Day, A.; Baker, F. Randomised controlled trial of problem solving treatment, antidepressant medication, and combined treatment for major depression in primary care. BMJ 2000, 320, 26–30. [Google Scholar] [CrossRef]
- Hawton, K.; Kirk, J. Problem-solving. In Cognitive Behaviour Therapy for Psychiatric Problems; Hawton, K., Salkovskis, P., Kirk, J., Clark, D., Eds.; Oxford University Press: Oxford, UK, 1989; pp. 406–426. [Google Scholar]
- Kendrick, T.; Simons, L.; Mynors-Wallis, L.; Gray, A.; Lathlean, J.; Pickering, R.; Harris, S.; Rivero-Arias, O.; Gerard, K.; Thompson, C. A trial of problem-solving by community mental health nurses for anxiety, depression and life difficulties among general practice patients. The CPN-GP study. Health Technol. Assess. 2005, 9, 1–104. [Google Scholar] [CrossRef]
- Allen, S.M. A problem-solving approach to stress reduction among younger women with breast carcinoma: A randomized controlled trial. Cancer 2002, 94, 3089–3100. [Google Scholar] [CrossRef]
- Didjurgeit, U.; Kruse, J.; Schmitz, N.; Stückenschneider, P.; Sawicki, P.T. A time-limited, problem-orientated psychotherapeutic intervention in Type 1 diabetic patients with complications: A randomized controlled trial. Diabet. Med. 2002, 19, 814–821. [Google Scholar] [CrossRef]
- Gellis, Z.D.; McGinty, J.; Horowitz, A.; Bruce, M.L.; Misener, E. Problem-Solving Therapy for Late-Life Depression in Home Care: A Randomized Field Trial. Am. J. Geriatr. Psychiatry 2007, 15, 968–978. [Google Scholar] [CrossRef]
- Perri, M.G.; Nezu, A.M.; McKelvey, W.F.; Shermer, R.L.; Renjilian, D.A.; Viegener, B.J. Relapse prevention training and problem-solving therapy in the long-term management of obesity. J Consult. Clin. Psychol. 2001, 69, 722–726. [Google Scholar] [CrossRef]
- Areán, P.A.; Raue, P.; Mackin, R.S.; Kanellopoulos, D.; McCulloch, C.; Alexopoulos, G.S. Problem-Solving Therapy and Supportive Therapy in Older Adults with Major Depression and Executive Dysfunction. Am. J. Psychiatry 2010, 167, 1391–1398. [Google Scholar] [CrossRef] [PubMed]
- Rovner, B.W.; Casten, R.J.; Hegel, M.T.; Leiby, B.E.; Tasman, W.S. Preventing Depression in Age-Related Macular Degeneration. Arch. Gen. Psychiatry 2007, 64, 886–892. [Google Scholar] [CrossRef] [PubMed]
- Keyes, C.L.M. Mental Illness and/or Mental Health? Investigating Axioms of the Complete State Model of Health. J. Consult. Clin. Psychol. 2005, 73, 539–548. [Google Scholar] [CrossRef] [PubMed]
- Tennant, R.; Hiller, L.; Fishwick, R.; Platt, S.; Joseph, S.; Weich, S.; Parkinson, J.; Secker, J.; Stewart-Brown, S. The Warwick-Edinburgh mental well-being scale (WEMWBS): Development and UK validation. Health Qual. Life Outcomes 2007, 5, 63. [Google Scholar] [CrossRef]
- Weich, S.; Brugha, T.; King, M.; McManus, S.; Bebbington, P.; Jenkins, R.; Cooper, C.; McBride, O.; Stewart-Brown, S. Mental well-being and mental illness: Findings from the Adult Psychiatric Morbidity Survey for England 2007. Br. J. Psychiatry 2011, 199, 23–28. [Google Scholar] [CrossRef]
- Gray, N.S.; O’Connor, C.; Knowles, J.; Pink, J.; Simkiss, N.J.; Williams, S.D.; Snowden, R.J. The Influence of the COVID-19 Pandemic on Mental Well-Being and Psychological Distress: Impact Upon a Single Country. Front. Psychiatry 2020, 11, 594115. [Google Scholar] [CrossRef]
- Katzman, R.; Brown, T.; Fuld, P.; Peck, A.; Schechter, R.; Schimmel, H. Validation of a short Orientation-Memory-Concentration Test of cognitive impairment. Am. J. Psychiatry 1983, 140, 734–739. [Google Scholar] [CrossRef]
- Zigmond, A.; Snaith, R. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Turano, K.; Massof, R.; Quigley, H. A self-assessment instrument designed for measuring independent mobility in RP patients: Generalizability to glaucoma patients. Investig. Ophthalmol. Vis. Sci. 2002, 43, 2874–2881. [Google Scholar]
- Stalvey, B.T.; Owsley, C.; Sloane, M.E.; Ball, K. The Life Space Questionnaire: A Measure of the Extent of Mobility of Older Adults. J. Appl. Gerontol. 1999, 18, 460–478. [Google Scholar] [CrossRef]
- Lamoureux, E.L.; Pallant, J.F.; Pesudovs, K.; Rees, G.; Hassell, J.B.; Keeffe, J.E. The Impact of Vision Impairment Questionnaire: An Assessment of Its Domain Structure Using Confirmatory Factor Analysis and Rasch Analysis. Investig. Opthalmol. Vis. Sci. 2007, 48, 1001–1006. [Google Scholar] [CrossRef] [PubMed]
- Peacock, S.; Misajon, R.; Iezzi, A.; Richardson, J.; Hawthorne, G.; Keeffe, J. Vision and Quality of Life: Development of Methods for the VisQoL Vision-Related Utility Instrument. Ophthalmic Epidemiol. 2008, 15, 218–223. [Google Scholar] [CrossRef] [PubMed][Green Version]
- D’Zurilla, T.J.; Nezu, A.M.; Maydeu-Olivares, A. Social Problem-Solving Inventory-Revised (SPSI-R): Technical Manual; Multi-Health Systems: North Tonawanda, NY, USA, 2002. [Google Scholar]
- Schwarzer, R.; Jerusalem, M. General self-efficacy scale (GSE). In Measures in Health Psychology: A User’s Portfolio. Causal and Control Beliefs; Weinman, J., Wright, S., Johnston, M., Eds.; NFER-NELSON: Windsor, UK, 1995; pp. 35–37. [Google Scholar]
- Mynors-Wallis, L.M. Problem-Solving Treatment for Anxiety and Depression: A Practical Guide; OUP: Oxford, UK, 2005. [Google Scholar]
- Mynors-Wallis, L.M.; Gath, D.H.; Lloyd-Thomas, A.R.; Tomlinson, D. Randomised controlled trial comparing problem solving treatment with amitriptyline and placebo for major depression in primary care. BMJ 1995, 310, 441–445. [Google Scholar] [CrossRef]
- Treweek, S.; Lockhart, P.; Pitkethly, M.; Cook, J.A.; Kjeldstrom, M.; Johansen, M.; Taskila, T.K.; Sullivan, F.M.; Wilson, S.; Jackson, C.; et al. Methods to improve recruitment to randomised controlled trials: Cochrane systematic review and meta-analysis. BMJ Open 2013, 3, e002360. [Google Scholar] [CrossRef] [PubMed]
- Nollett, C.L.; Bray, N.; Bunce, C.; Casten, R.J.; Edwards, R.T.; Hegel, M.T.; Janikoun, S.; Jumbe, S.E.; Ryan, B.; Shearn, J.; et al. Depression in Visual Impairment Trial (DEPVIT): A Randomised Clinical Trial of Depression Treatments in People with Low Vision. Investig. Ophthalmol. Vis. Sci. 2016, 57, 4247–4254. [Google Scholar] [CrossRef] [PubMed]
- Van der Aa, H.P.; van Rens, G.H.; Comijs, H.C.; Margrain, T.H.; Gallindo-Garre, F.; Twisk, J.W.; van Nispen, R.M. Stepped care for depression and anxiety in visually impaired older adults: Multicenter randomized controlled trial. Br. Med. J. 2015, 351, h6127. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Problem-Solving Treatment (N = 29) | No Treatment (N = 32) | |
|---|---|---|
| Age (years) | 70.9 (19.5) | 75.6 (15.8) |
| Female | 18 (62.1) | 17 (53.1) |
| Severely sight impaired (blind) | 12 (41.4) | 14 (43.8) |
| Cause of vision impairment: macular degeneration | ||
| 13 (44.8) | 15 (46.9) | |
| WEMBS | ||
| Raw score | 45.7 (11.2) | 50.5 (7.2) |
| Rasch score | 21.8 (4.4) | 23.6 (2.9) |
| HADS | ||
| Anxiety | 6.1 (4.0) | 4.6 (4.1) |
| Depression | 7.4 (4.4) | 5.8 (3.2) |
| Total | 13.5 (7.3) | 10.5 (6.9) |
| IVIQ | ||
| Mobility and independence | 1.6 (0.5) | 1.8 (0.5) |
| Emotion and well-being | 1.9 (0.5) | 2.1 (0.6) |
| Reading and information | 1.7 (0.6) | 1.9 (0.6) |
| Total score | 1.7 (0.5) | 1.9 (0.5) |
| Rasch total score | 51.5 (6.5) | 53.5 (6.1) |
| VISQOL | ||
| Injure | 0.7 (0.3) | 0.7 (0.3) * |
| Cope | 0.7 (0.3) | 0.8 (0.2) |
| Friendships | 0.9 (0.2) | 0.9 (0.2) |
| Assistance | 0.9 (0.2) | 1.0 (0.1) |
| Roles | 0.6 (0.4) | 0.7 (0.4) |
| Confidence | 0.8 (0.3) | 0.8 (0.3) |
| Total Dimension Score | 0.6 (0.3) | 0.7 (0.2) |
| Life Spaces Questionnaire | 4.9 (1.8) | 4.7 (1.8) * |
| Independent Mobility | ||
| Total score | 2.7 (0.8) | 2.4 (0.9) |
| Rasch score | −0.2 (1.0) | −0.6 (1.4) |
| SPSIRS total score | 12.2 (0.9) n = 24 | 12.1 (0.5) n = 21 |
| Self-efficacy score | 2.9 (0.7) | 2.9 (0.4) |
| WEMBS Score | PST | No PST | Treatment Effect (95% CI) | Overall Treatment Effect (95% CI) | p-Value |
|---|---|---|---|---|---|
| Baseline | 45.7 (11.2) | 50.5 (7.2) | - | ||
| 3 months | 50.3 (9.6) | 48.0 (9.8) | 2.61 (0.27, 4.95) | 2.44 | |
| 6 months | 49.3 (11.2) | 49.8 (6.9) | 1.78 (−0.60, 4.16) | (0.40 | 0.019 |
| 9 months | 50.2 (12.0) | 47.0 (12.2) | 3.11 (0.53, 5.69) | 4.47) |
| PST | No PST | Treatment Effect (95% CI) | p-Value | |
|---|---|---|---|---|
| HADS Anxiety | ||||
| At baseline | 6.1 (4.0) | 4.6 (4.1) | −1.29 (−2.39, −0.18) | 0.022 |
| At 3 months | 5.1 (3.6) | 5.3 (4.2) | ||
| At 6 months | 5.2 (3.9) | 4.3 (3.1) | ||
| At 9 months | 4.7 (3.6) | 5.6 (4.5) | ||
| HADS Depression | ||||
| At baseline | 7.4 (4.4) | 5.8 (3.2) | −1.33 (−2.62, −0.05) | 0.042 |
| At 3 months | 5.5 (3.0) | 6.4 (3.6) | ||
| At 6 months | 6.7 (4.4) | 6.2 (2.0) | ||
| At 9 months | 5.9 (3.7) | 6.5 (3.5) | ||
| HADS Total | ||||
| At baseline | 13.5 (7.3) | 10.4 (6.9) | −2.76 (−4.92, −0.60) | 0.012 |
| At 3 months | 10.6 (5.6) | 11.7 (6.9) | ||
| At 6 months | 11.9 (7.2) | 10.4 (4.1) | ||
| At 9 months | 10.7 (6.2) | 12.1 (7.4) | ||
| IVIQ Total Score | ||||
| At baseline | 1.7 (0.5) | 1.9 (0.5) | 0.23 (0.08, 0.37) | 0.002 |
| At 3 months | 1.8 (0.5) | 1.8 (0.4) | ||
| At 6 months | 1.9 (0.5) | 1.8 (0.4) | ||
| At 9 months | 1.9 (0.5) | 1.8 (0.5) | ||
| IVIQ Rasch Total Score | ||||
| At baseline | 51. 5 (6.5) | 53.5 (6.1) | 3.50 (1.49, 5.51) | <0.001 |
| At 3 months | 53.0 (7.0) | 51.8 (5.7) | ||
| At 6 months | 54.2 (7.9) | 51.9 (4.6) | ||
| At 9 months | 54.1 (7.4) | 52.5 (6.0) | ||
| VISQOL Total Dimension Score | ||||
| At baseline | 0.6 (0.3) | 0.7 (0.2) | 0.07 (−0.02, 0.16) | 0.112 |
| At 3 months | 0.6 (0.3) | 0.6 (0.3) | ||
| At 6 months | 0.7 (0.2) | 0.7 (0.3) | ||
| At 9 months | 0.6 (0.3) | 0.6 (0.3) | ||
| Life Spaces Questionnaire Score | ||||
| At baseline | 4.9 (1.8) | 4.7 (1.8) | 0.22 (−0.31, 0.75) | 0.418 |
| At 3 months | 4.8 (1.8) | 4.7 (1.5) | ||
| At 6 months | 4.9 (2.0) | 4.3 (2.0) | ||
| At 9 months | 4.6 (2.2) | 4.4 (2.0) | ||
| Independent Mobility Total Score | ||||
| At baseline | 2.6 (0.8) | 2.4 (0.9) | −0.05 (−0.29, 0.18) | 0.650 |
| At 3 months | 2.6 (0.8) | 2.3 (0.8) | ||
| At 6 months | 2.6 (0.8) | 2.4 (0.6) | ||
| At 9 months | 2.7 (0.9) | 2.5 (1.0) | ||
| Independent Mobility Rasch Score | ||||
| At baseline | −0.2 (1.0) | −0.6 (1.4) | −0.11 (−0.46, 0.25) | 0.550 |
| At 3 months | −0.3 (1.2) | −0.7 (1.3) | ||
| At 6 months | −0.3 (1.2) | −0.5 (0.9) | ||
| At 9 months | −0.1 (1.2) | −0.3 (1.3) | ||
| SPSIRS Total Score | ||||
| At baseline | 12.2 (0.9) | 12.1 (0.5) | 0.14 (−0.09, 0.38) | 0.239 |
| At 6 months | 3.8 (0.7) | 3.6 (0.7) | ||
| At 9 months | 3.7 (0.9) | 3.3 (0.8) | ||
| Self Efficacy Score | ||||
| At baseline | 2.8 (0.7) | 2.9 (0.4) | 0.27 (0.06, 0.49) | 0.011 |
| At 6 months | 3.1 (0.7) | 3.0 (0.5) | ||
| At 9 months | 3.1 (0.8) | 2.7 (0.5) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Riazi, A.; Aspden, T.; Rubin, G.; Ambler, G.; Jichi, F.; Mynors-Wallice, L.; O’Driscoll, M.; Walters, K. Problem-Solving Treatment for People Recently Diagnosed with Visual Impairment: Pilot Randomised Controlled Trial. J. Pers. Med. 2022, 12, 1431. https://doi.org/10.3390/jpm12091431
Riazi A, Aspden T, Rubin G, Ambler G, Jichi F, Mynors-Wallice L, O’Driscoll M, Walters K. Problem-Solving Treatment for People Recently Diagnosed with Visual Impairment: Pilot Randomised Controlled Trial. Journal of Personalized Medicine. 2022; 12(9):1431. https://doi.org/10.3390/jpm12091431
Chicago/Turabian StyleRiazi, Afsane, Trefor Aspden, Gary Rubin, Gareth Ambler, Fatima Jichi, Laurence Mynors-Wallice, Miriam O’Driscoll, and Kate Walters. 2022. "Problem-Solving Treatment for People Recently Diagnosed with Visual Impairment: Pilot Randomised Controlled Trial" Journal of Personalized Medicine 12, no. 9: 1431. https://doi.org/10.3390/jpm12091431
APA StyleRiazi, A., Aspden, T., Rubin, G., Ambler, G., Jichi, F., Mynors-Wallice, L., O’Driscoll, M., & Walters, K. (2022). Problem-Solving Treatment for People Recently Diagnosed with Visual Impairment: Pilot Randomised Controlled Trial. Journal of Personalized Medicine, 12(9), 1431. https://doi.org/10.3390/jpm12091431