
The Adjuvant Therapy of Intravenous Laser Irradiation of Blood (ILIB) on Pain and Sleep Disturbance of Musculoskeletal Disorders


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
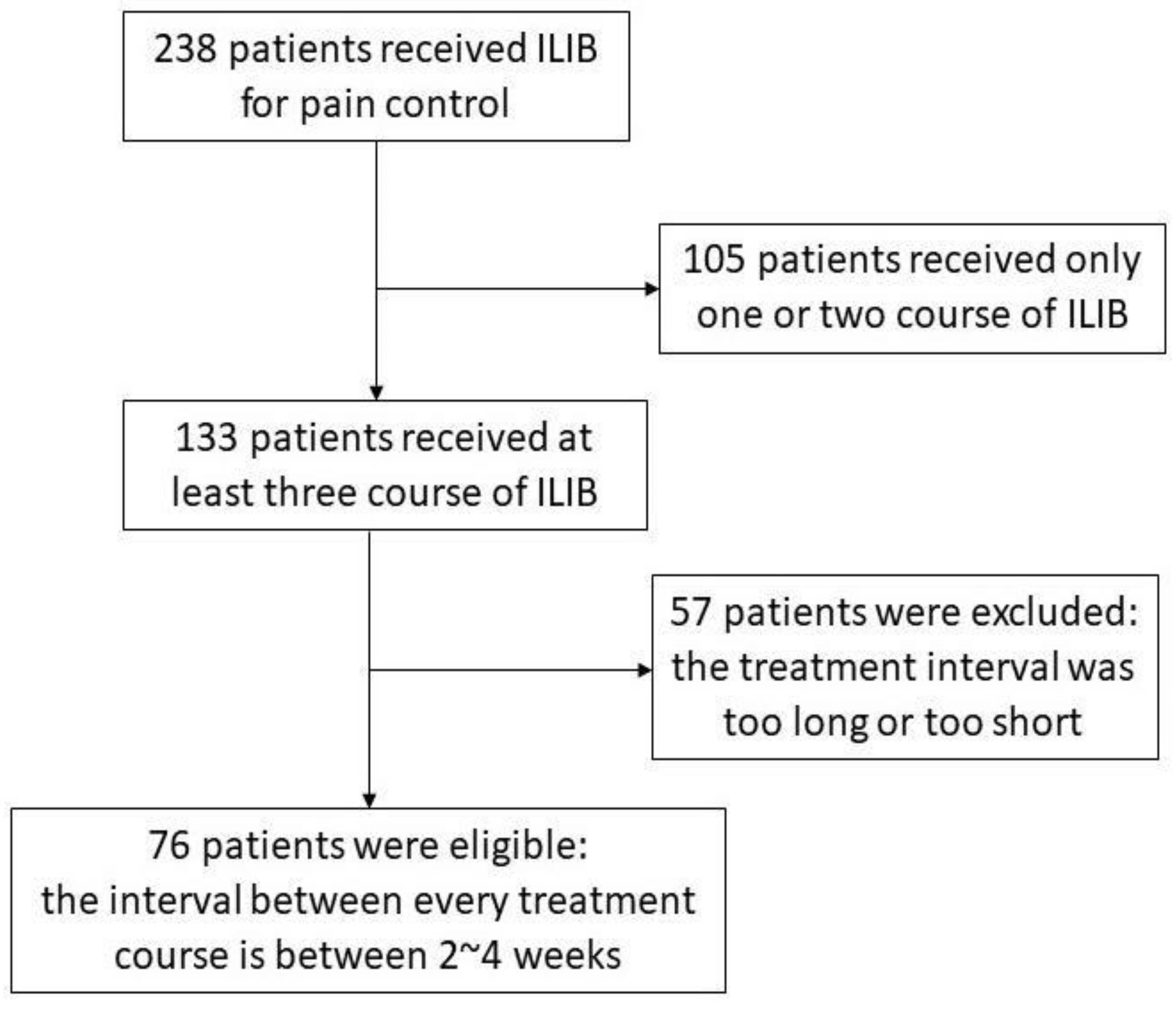
2.2. Participants
2.3. Study Variables
2.4. Identification Characteristics for ILIB Treatment Optimization
2.5. Statistical Analysis
3. Results
3.1. Patient’s Profile
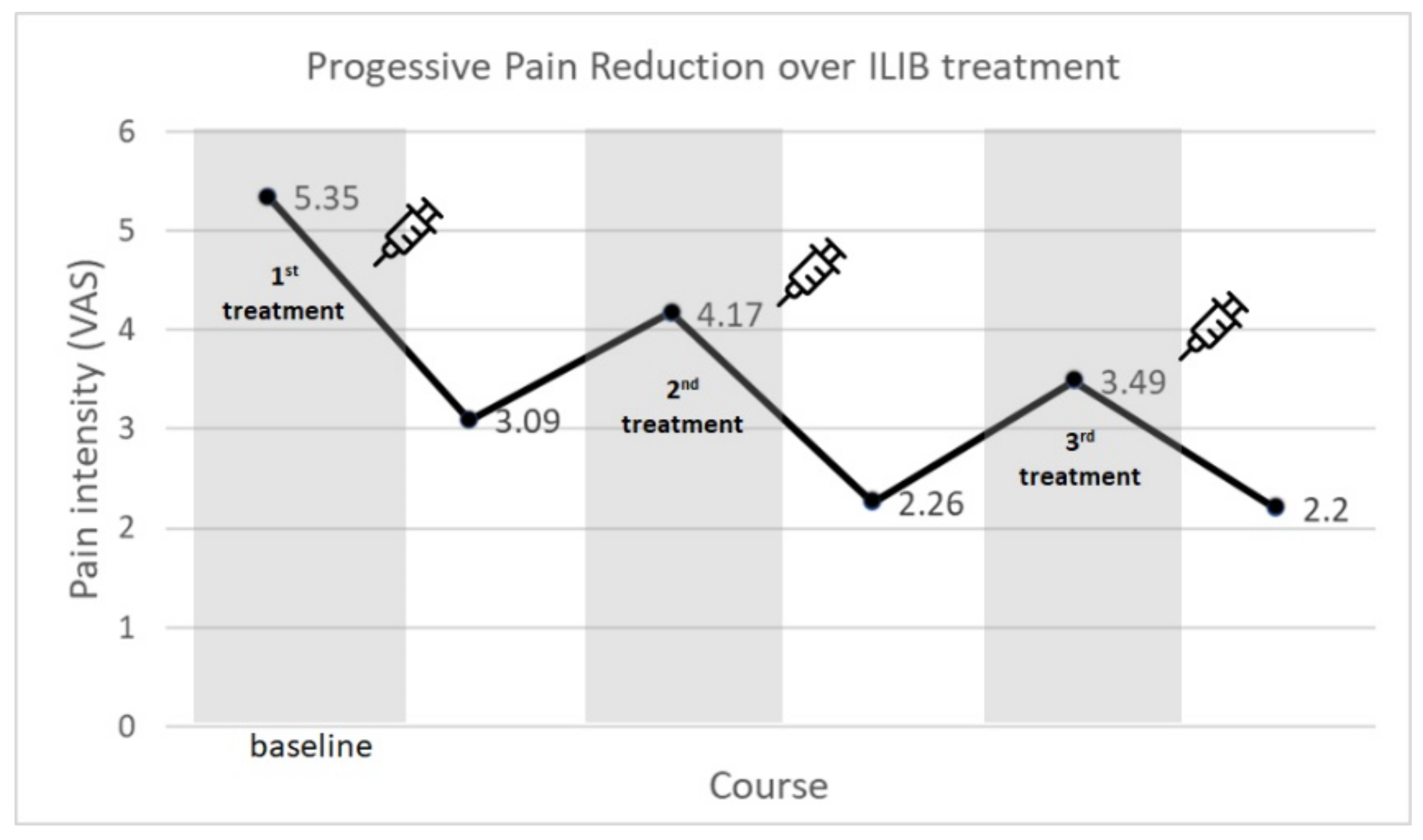
3.2. Total Participants’ VAS Score Trend
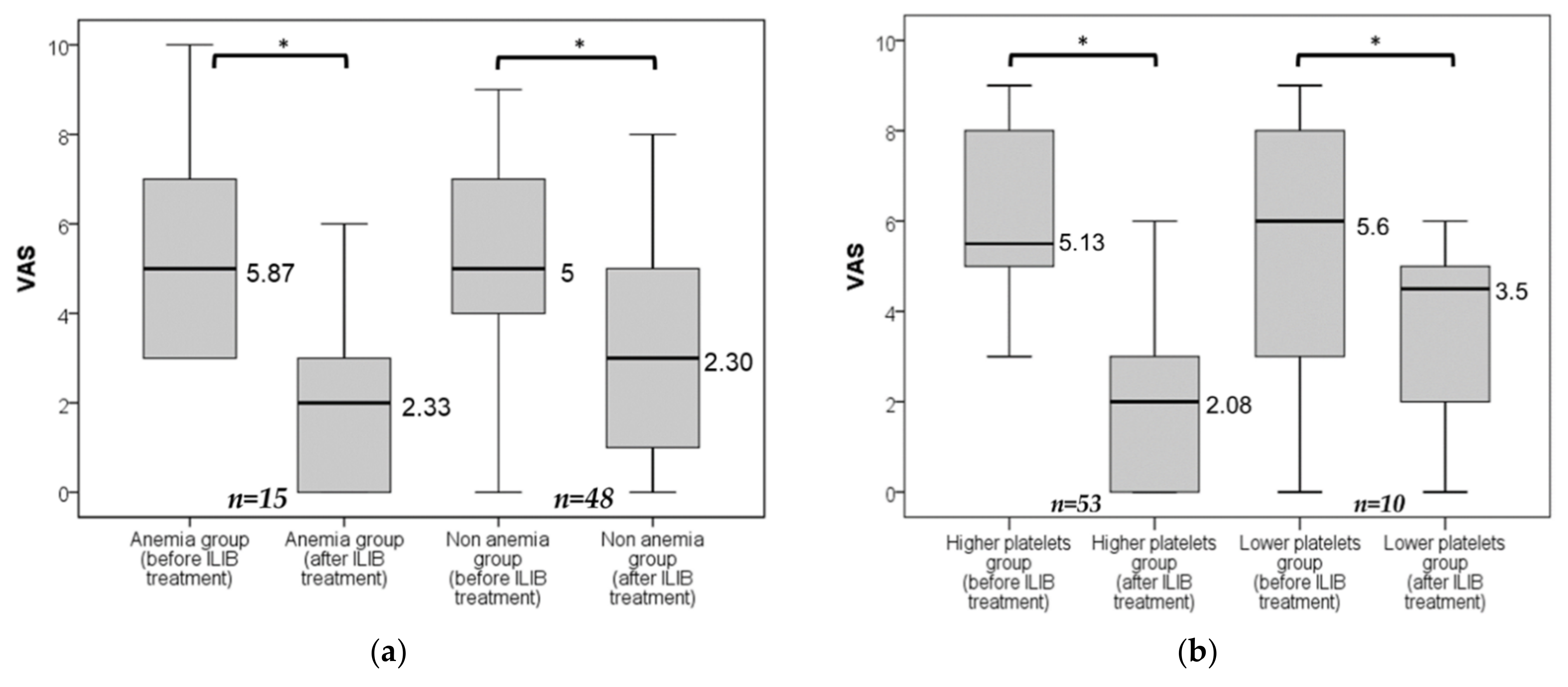
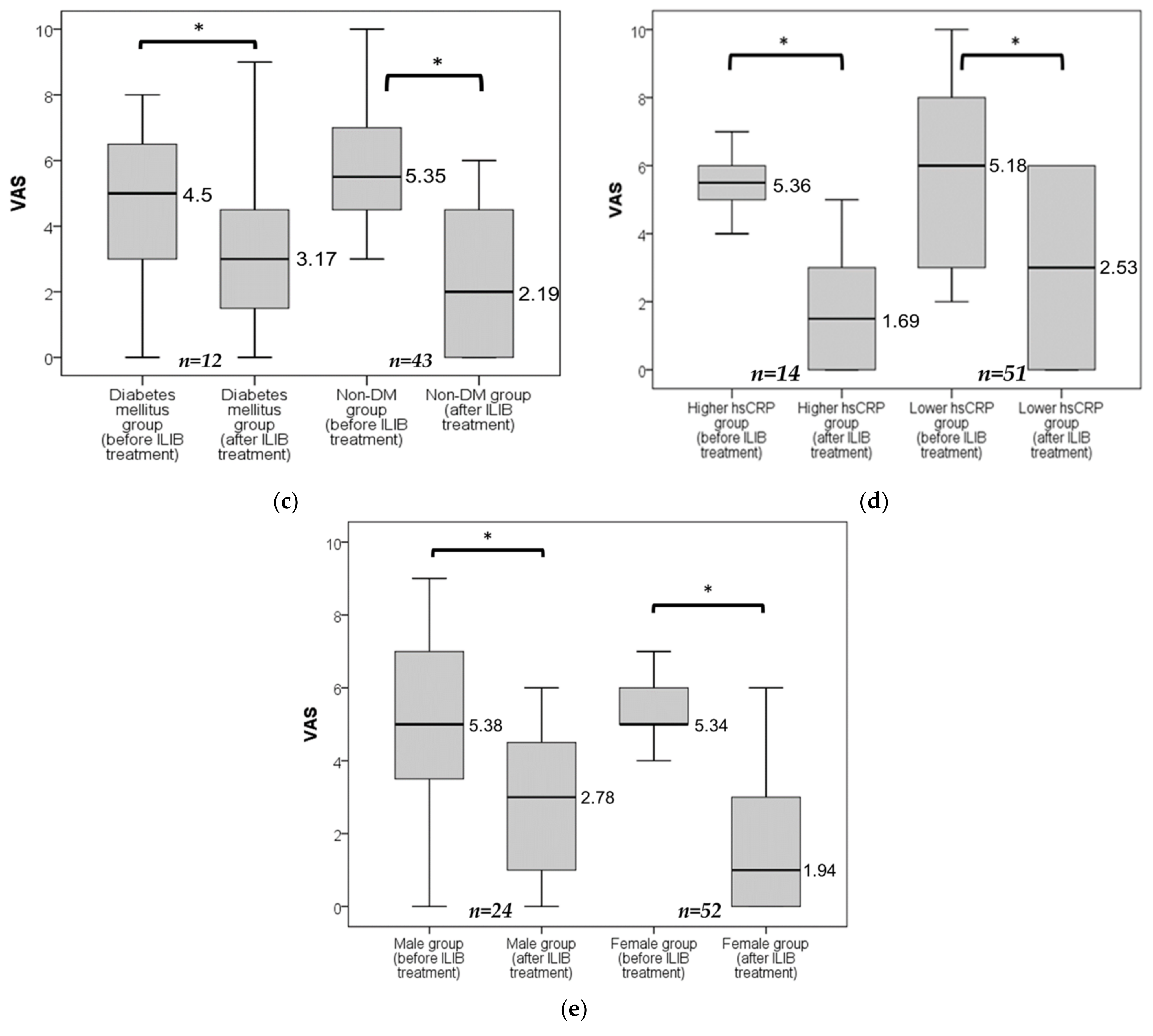
3.3. Identification Characteristics for ILIB Treatment Optimization
3.4. Pain Control Effect in the Groups of Different Pain Intensity
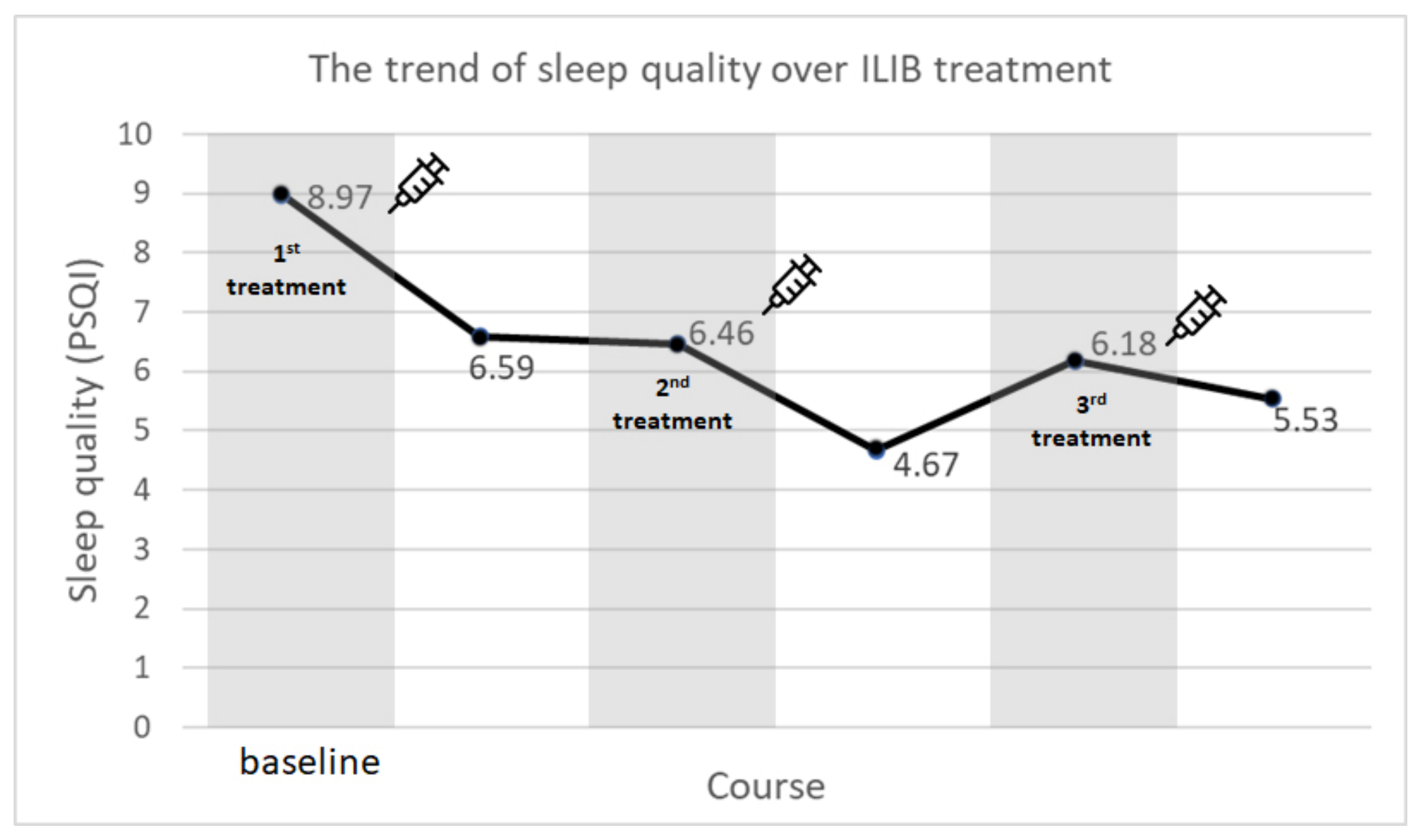
3.5. Participants’ Sleep Quality
3.6. The Safety of ILIB Treatment
3.7. Participants Who Only Received 1 or 2 Courses of ILIB
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cieza, A.; Causey, K.; Kamenov, K.; Hanson, S.W.; Chatterji, S.; Vos, T. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2021, 396, 2006–2017. [Google Scholar] [CrossRef]
- Malanga, G.A.; Yan, N.; Stark, J. Mechanisms and efficacy of heat and cold therapies for musculoskeletal injury. Postgrad. Med. 2015, 127, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Chou, R.; Deyo, R.; Friedly, J.; Skelly, A.; Hashimoto, R.; Weimer, M.; Fu, R.; Dana, T.; Kraegel, P.; Griffin, J.; et al. Nonpharmacologic Therapies for Low Back Pain: A Systematic Review for an American College of Physicians Clinical Practice Guideline. Ann. Intern. Med. 2017, 166, 493–505. [Google Scholar] [CrossRef] [PubMed]
- Da Silva Leal, M.V.; Lima, M.O.; Nicolau, R.A.; De Carvallho, T.M.T.; Abreu, J.A.D.C.; Pessoa, D.R.; Arisawa, E.A.L.S. Effect of Modified Laser Transcutaneous Irradiation on Pain and Quality of Life in Patients with Diabetic Neuropathy. Photobiomodulation Photomed. Laser Surg. 2020, 38, 138–144. [Google Scholar] [CrossRef]
- Chiran, D.A.; Litscher, G.; Weber, M.; Ailioaie, L.; Ailioaie, C.; Litscher, D. Intravenous Laser Blood Irradiation Increases Efficacy of Etanercept in Selected Subtypes of Juvenile Idiopathic Arthritis: An Innovative Clinical Research Approach. Evid. Based Complementary Altern. Med. 2013, 2013, 168134. [Google Scholar] [CrossRef]
- Wu, P.Y.; Penn, I.W.; Lin, P.H.; Wang, J.C.; Chuang, E.; Wu, S.H.; Chuang, T.Y. Effects of Intravenous Laser Irradiation of Blood on Pain, Function and Depression of Fibromyalgia Patients. Gen. Med. 2018, 6, 1–8. [Google Scholar] [CrossRef]
- Momenzadeh, S.; Abbasi, M.; Ebadifar, A.; Aryani, M.; Bayrami, J.; Nematollahi, F. The intravenous laser blood irradiation in chronic pain and fibromyalgia. J. Lasers Med. Sci. 2015, 6, 6. [Google Scholar]
- Itoh, T.; Murakami, H.; Orihashi, K.; Sueda, T.; Kusumoto, Y.; Kakehashi, M.; Matsuura, Y. Low Power Laser Protects Human Erythrocytes In an In Vitro Model of Artificial Heart-Lung Machines. Artif. Organs 2000, 24, 870–873. [Google Scholar] [CrossRef]
- Zhong, P.; Zhou, M.; He, L.; Zhu, C.; Chen, N. Intravascular low-level helium-neon laser irradiation on blood for acute ischemic stroke. Cochrane Database Syst. Rev. 2017, 2017, CD008917. [Google Scholar] [CrossRef]
- Mi, X.-Q.; Chen, J.-Y.; Liang, Z.-J.; Zhou, L.-W. In Vitro Effects of Helium-Neon Laser Irradiation on Human Blood: Blood Viscosity and Deformability of Erythrocytes. Photomed. Laser Surg. 2005, 22, 477–482. [Google Scholar] [CrossRef]
- Wasik, M.; Gorska, E.; Modzelewska, M.; Nowicki, K.; Jakubczak, B.; Demkow, U. The influence of low-power helium-neon laser irradiation on function of selected peripheral blood cells. J. Physiol. Pharmacol. 2007, 58 (Suppl. 5), 729–737. [Google Scholar]
- Mikhaylov, V.A. The use of Intravenous Laser Blood Irradiation (ILBI) at 630–640 nm to prevent vascular diseases and to increase life expectancy. Laser Ther. 2015, 24, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.F.; Tsai, Y.A.; Wu, S.B.; Wei, Y.H.; Tsai, P.Y.; Chuang, T.Y. Effects of Intravascular Laser Irradiation of Blood in Mitochondria Dysfunction and Oxidative Stress in Adults with Chronic Spinal Cord Injury. Photomed. Laser Surg. 2012, 30, 579–586. [Google Scholar] [CrossRef]
- Pastore, D.; Greco, M.; Passarella, D. Specific helium-neon laser sensitivity of the purified cytochrome c oxidase. Int. J. Radiat. Biol. 2000, 76, 863–870. [Google Scholar] [CrossRef]
- Tomé, R.F.F.; Silva, D.F.B.; Dos Santos, C.A.O.; de Vasconcelos Neves, G.; Rolim, A.K.A.; de Castro Gomes, D.Q. ILIB (intravascular laser irradiation of blood) as an adjuvant therapy in the treatment of patients with chronic systemic diseases—an integrative literature review. Lasers Med Sci. 2020, 35, 1899–1907. [Google Scholar] [CrossRef]
- Momenzadeh, S.; Akhyani, V.; Razaghi, Z.; Ebadifar, A.; Abbasi, M. Evaluation of the Effects of Intravenous and Percutaneous Low Level Laser Therapy in the Management of Shoulder Myofascial Pain Syndrome. J. Lasers Med. Sci. 2016, 7, 16–20. [Google Scholar] [CrossRef]
- McCormack, H.M.; Horne, D.J.; Sheather, S. Clinical applications of visual analogue scales: A critical review. Psychol. Med. 1988, 18, 1007–1019. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Nahm, F.S. Nonparametric statistical tests for the continuous data: The basic concept and the practical use. Korean J. Anesthesiol. 2016, 69, 8–14. [Google Scholar] [CrossRef]
- Bindu, S.; Mazumder, S.; Bandyopadhyay, U. Non-steroidal anti-inflammatory drugs (NSAIDs) and organ damage: A current perspective. Biochem. Pharmacol. 2020, 180, 114147. [Google Scholar] [CrossRef]
- Iagnocco, A.; Naredo, E. Ultrasound-guided corticosteroid injection in rheumatology: Accuracy or efficacy? Rheumatology 2010, 49, 1427–1428. [Google Scholar] [CrossRef][Green Version]
- Yang, W.-H.; Lin, S.-P.; Chang, S.-T. Case report: Rapid improvement of crossed cerebellar diaschisis after intravascular laser irradiation of blood in a case of stroke. Medicine 2017, 96, e5646. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Chang, S.-T. Benefits of intravascular laser Irradiation of Blood on Motor and Sensory Recovery Viewing from Brain Function Images: Portrait of a Case with Chronic Sjögren’s Syndrome, Transverse Myelitis, and Guillain-Barré Syndrome. Biomed. J. Sci. Tech. Res. 2019, 14, 10738–10741. [Google Scholar] [CrossRef]
- Chang, S.-T. Reversal of Impaired Blood Flow of the Basal Ganglion from the Prior Focal Perfusion Defect in a Case of Ischemic Infarction: Observation during the Two Stages of Administration of Intravenous Laser Irradiation of Blood. J. Med. Study Res. 2019, 2, 11. [Google Scholar] [CrossRef]
- Lan, C.-C.E.; Wu, S.-B.; Wu, C.-S.; Shen, Y.-C.; Chiang, T.-Y.; Wei, Y.-H.; Yu, H.-S. Induction of primitive pigment cell differentiation by visible light (helium–neon laser): A photoacceptor-specific response not replicable by UVB irradiation. J. Mol. Med. 2011, 90, 321–330. [Google Scholar] [CrossRef]
- Amjadi, A.; Mirmiranpor, H.; Khandani, S.; Sobhani, S.O.; Shafaee, Y. Intravenous Laser Wavelength Irradiation Effect on Interleukins: IL-1α, IL-1β, IL6 in Diabetic Rats. Laser Ther. 2019, 28, 267–273. [Google Scholar] [CrossRef]
- Hughes, C.M.; McCullough, C.A.; Bradbury, I.; Boyde, C.; Hume, D.; Yuan, J.; Quinn, F.; McDonough, S. Acupuncture and Reflexology for Insomnia: A Feasibility Study. Acupunct. Med. 2009, 27, 163–168. [Google Scholar] [CrossRef]
- Kim, J.; Lee, S.H.; Kim, T.-H. Improvement of sleep quality after treatment in patients with lumbar spinal stenosis: A prospective comparative study between conservative versus surgical treatment. Sci. Rep. 2020, 10, 14135. [Google Scholar] [CrossRef]
- Gerhart, J.I.; Burns, J.W.; Post, K.M.; Smith, D.A.; Porter, L.S.; Burgess, H.J.; Schuster, E.; Buvanendran, A.; Fras, A.M.; Keefe, F.J. Relationships Between Sleep Quality and Pain-Related Factors for People with Chronic Low Back Pain: Tests of Reciprocal and Time of Day Effects. Ann. Behav. Med. 2017, 51, 365–375. [Google Scholar] [CrossRef]
- Afolalu, E.F.; Ramlee, F.; Tang, N.K. Effects of sleep changes on pain-related health outcomes in the general population: A systematic review of longitudinal studies with exploratory meta-analysis. Sleep Med. Rev. 2017, 39, 82–97. [Google Scholar] [CrossRef]
- Sharma, S.; Kavuru, M. Sleep and Metabolism: An Overview. Int. J. Endocrinol. 2010, 2010, 270832. [Google Scholar] [CrossRef] [PubMed]
- Siegel, J.M. Why We Sleep. Sci. Am. 2003, 289, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Buchsbaum, M.S.; Gillin, J.; Wu, J.; Hazlett, E.; Sicotte, N.; Dupont, R.M.; Bunney, W.E. Regional cerebral glucose metabolic rate in human sleep assessed by positron emission tomography. Life Sci. 1989, 45, 1349–1356. [Google Scholar] [CrossRef]
- Van Cauter, E.; Polonsky, K.S.; Scheen, A.J. Roles of Circadian Rhythmicity and Sleep in Human Glucose Regulation. Endocr. Rev. 1997, 18, 716–738. [Google Scholar] [CrossRef]
- Patel, A.K.; Reddy, V.; Araujo, J.F. Physiology, Sleep Stages; StatPearls Publishing LLC: Tampa, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK526132 (accessed on 1 March 2022).
- Léger, D.; Debellemaniere, E.; Rabat, A.; Bayon, V.; Benchenane, K.; Chennaoui, M. Slow-wave sleep: From the cell to the clinic. Sleep Med. Rev. 2018, 41, 113–132. [Google Scholar] [CrossRef]
- Lanfranco, F.; Motta, G.; Minetto, M.A.; Ghigo, E.; Maccario, M. Growth hormone/insulin-like growth factor-I axis in obstructive sleep apnea syndrome: An update. J. Endocrinol. Investig. 2010, 33, 192–196. [Google Scholar] [CrossRef]
- Van Cauter, E.; Plat, L. Physiology of growth hormone secretion during sleep. J. Pediatr. 1996, 128, S32–S37. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disease | Number (n) |
|---|---|
| Spinal enthesopathy | 19 |
| Periostitis | 11 |
| Radiculopathy (HIVD) | 8 |
| Osteoarthritis | 6 |
| Polyneuropathy | 5 |
| Degenerative joint disease | 4 |
| Myofascial pain syndrome | 4 |
| Spondylolisthesis | 4 |
| Tendinitis | 3 |
| Frozen shoulder | 3 |
| Other diseases a | 8 |
| Before Treatment | After Treatment | p Value | |||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| 1st course of ILIB | 5.35 | 2.12 | 3.09 | 1.98 | <0.001 |
| 2nd course of ILIB | 4.17 | 2.34 | 2.26 | 2.11 | <0.001 |
| 3rd course of ILIB | 3.49 | 2.44 | 2.20 | 2.33 | <0.001 |
| VAS Score | ||||
|---|---|---|---|---|
| Before All ILIB Treatments Mean ± SEM | After All ILIB Treatments Mean ± SEM | p Value | n | |
| Spinal enthesopathy | 5.74 ± 1.94 | 1.44 ± 1.98 | 0.001 * | 19 |
| Periostitis | 4.36 ± 1.20 | 2.00 ± 1.34 | 0.007 * | 11 |
| Radiculopathy (HIVD) | 6.00 ± 1.51 | 1.63 ± 2.07 | 0.017 * | 8 |
| Osteoarthritis | 6.17 ± 2.23 | 4.83 ± 3.25 | 0.066 | 6 |
| Polyneuropathy | 6.00 ± 3.16 | 2.40 ± 2.30 | 0.042 * | 5 |
| Pain Intensity | Before Treatment | After Treatment | p Value | n | |||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean Difference | |||
| mild | 2.35 | 1.06 | 1.88 | 2.32 | 0.47 | 0.352 | 17 |
| moderate | 5.52 | 0.88 | 1.65 | 1.93 | 3.87 | <0.001 | 44 |
| severe | 8.27 | 0.59 | 4.13 | 2.56 | 4.14 | 0.001 | 15 |
| Before Treatment | After Treatment | p Value | |||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||
| 1st course of ILIB | 8.97 | 4.18 | 6.59 | 4.63 | <0.001 |
| 2nd course of ILIB | 6.46 | 4.19 | 4.67 | 3.70 | <0.001 |
| 3rd course of ILIB | 6.18 | 4.58 | 5.53 | 4.29 | 0.011 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fu, C.-M.; Wang, N.-K.; Cheng, Y.-Y.; Chang, S.-T. The Adjuvant Therapy of Intravenous Laser Irradiation of Blood (ILIB) on Pain and Sleep Disturbance of Musculoskeletal Disorders. J. Pers. Med. 2022, 12, 1333. https://doi.org/10.3390/jpm12081333
Fu C-M, Wang N-K, Cheng Y-Y, Chang S-T. The Adjuvant Therapy of Intravenous Laser Irradiation of Blood (ILIB) on Pain and Sleep Disturbance of Musculoskeletal Disorders. Journal of Personalized Medicine. 2022; 12(8):1333. https://doi.org/10.3390/jpm12081333
Chicago/Turabian StyleFu, (Jimmy) Chun-Ming, Nai-Kuang Wang, Yuan-Yang Cheng, and Shin-Tsu Chang. 2022. "The Adjuvant Therapy of Intravenous Laser Irradiation of Blood (ILIB) on Pain and Sleep Disturbance of Musculoskeletal Disorders" Journal of Personalized Medicine 12, no. 8: 1333. https://doi.org/10.3390/jpm12081333
APA StyleFu, C.-M., Wang, N.-K., Cheng, Y.-Y., & Chang, S.-T. (2022). The Adjuvant Therapy of Intravenous Laser Irradiation of Blood (ILIB) on Pain and Sleep Disturbance of Musculoskeletal Disorders. Journal of Personalized Medicine, 12(8), 1333. https://doi.org/10.3390/jpm12081333