
Management of the Two-Week Wait Pathway for Skin Cancer Patients, before and during the Pandemic: Is Virtual Consultation an Option?


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Inclusion Criteria
2.3. Exclusion Criteria
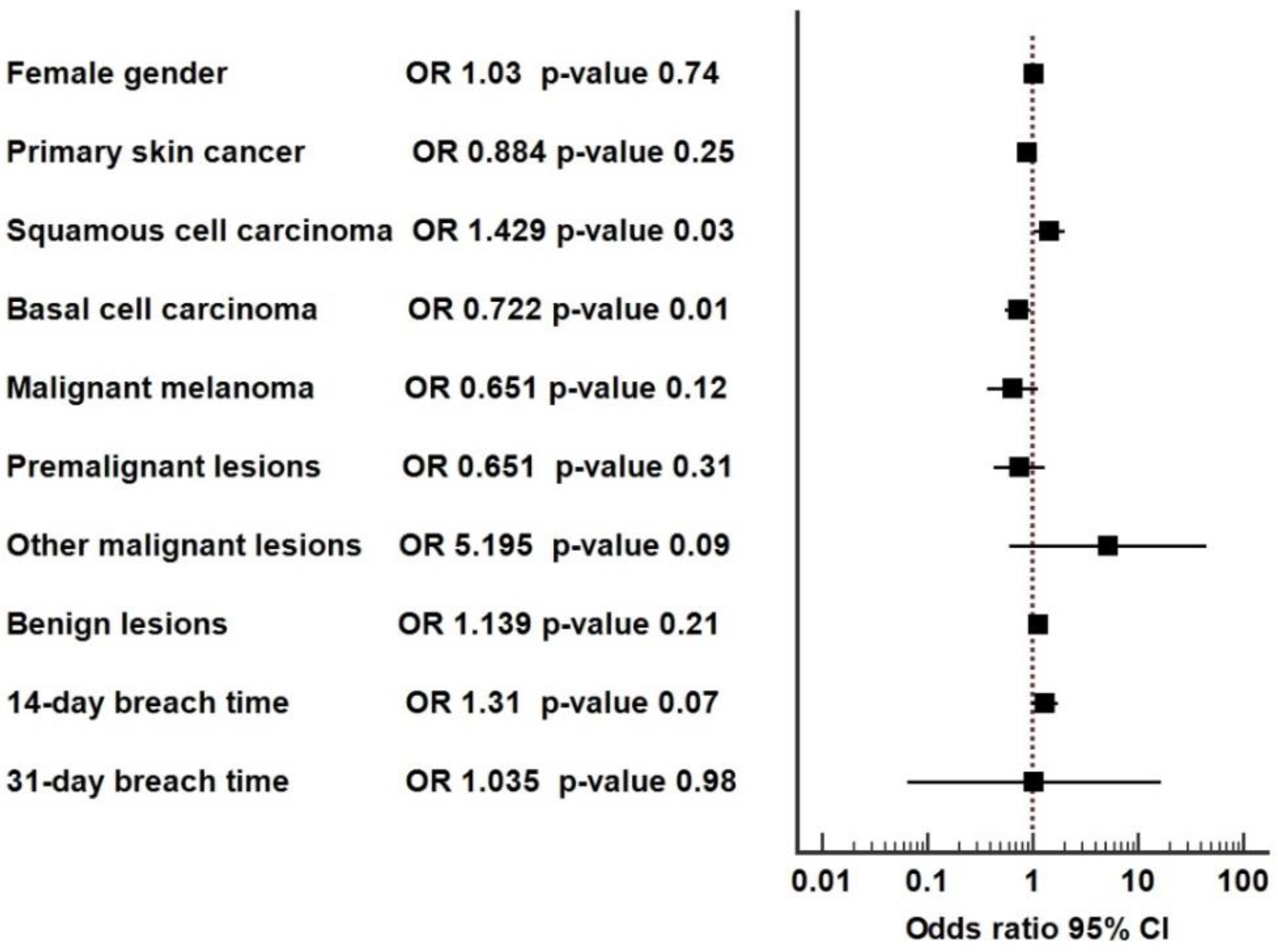
2.4. Statistical Analysis
3. Results
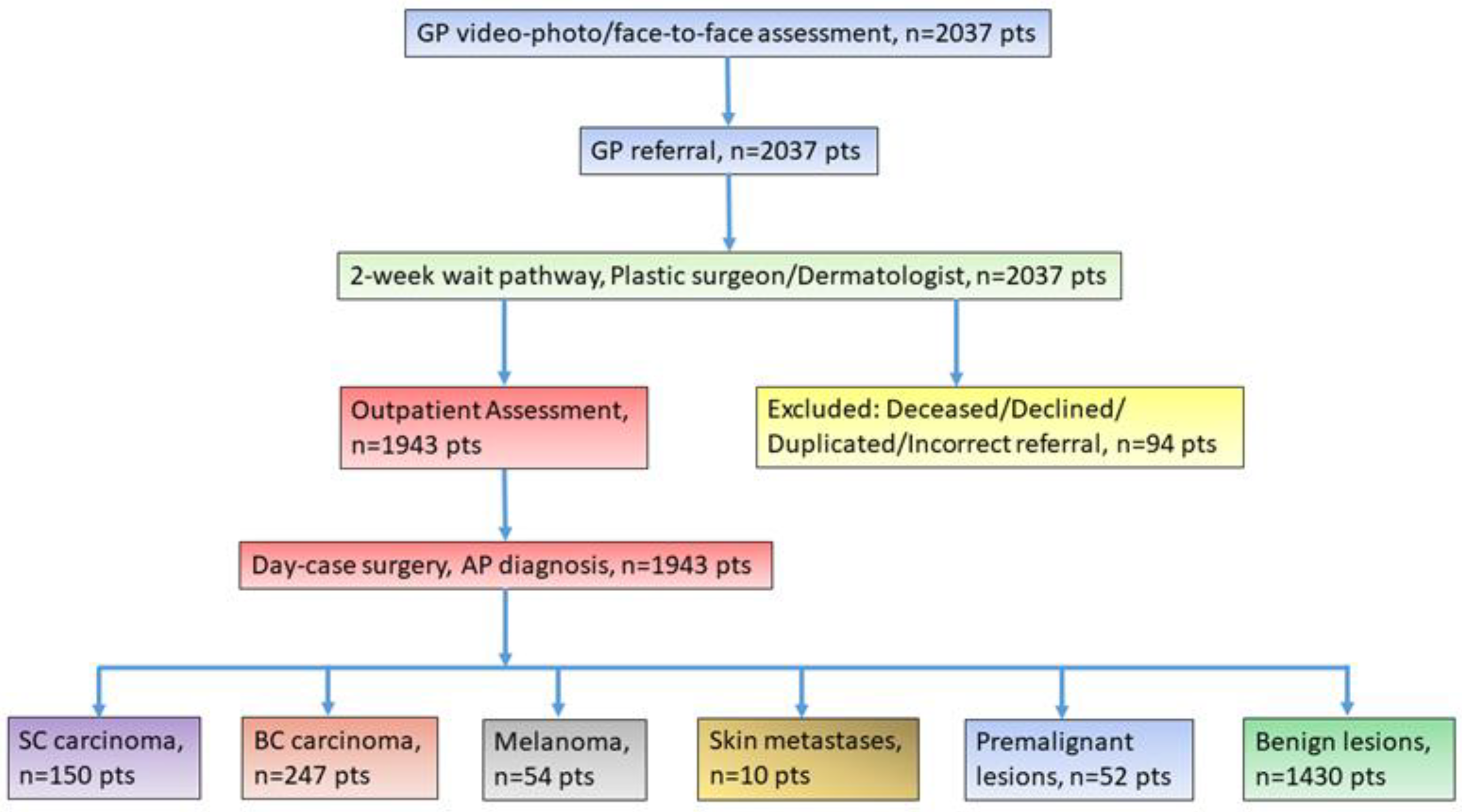
3.1. Patient Population
3.2. Baseline Characteristics
4. Discussion
4.1. Rationale for the Study
4.2. Added Value to the Literature
4.3. Comparison with Other Studies
4.4. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Green, A.C.; Baade, P.; Coory, M.; Aitken, J.F.; Smithers, M. Population-Based 20-Year Survival among People Diagnosed with Thin Melanomas in Queensland, Australia. J. Clin. Oncol. 2012, 30, 1462–1467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lomas, A.; Leonardi-Bee, J.; Bath-Hextall, F. A Systematic Review of Worldwide Incidence of Nonmelanoma Skin Cancer. Br. J. Dermatol. 2012, 166, 1069–1080. [Google Scholar] [CrossRef] [PubMed]
- Overview: Suspected Cancer: Recognition and Referral: Guidance. NICE. Available online: https://www.nice.org.uk/guidance/ng12 (accessed on 19 June 2022).
- Ayda, H.-R.; Johanna, O. Diagnostic Accuracy amongst Two Week Wait Referrals for Skin Malignancy. J. Dermatol. Res. Ther. 2021, 7, 111. [Google Scholar] [CrossRef]
- Piccolo, D.; Smolle, J.; Wolf, I.H.; Peris, K.; Hofmann-Wellenhof, R.; Dell’Eva, G.; Burroni, M.; Chimenti, S.; Kerl, H.; Soyer, H.P. Face-To-Face Diagnosis vs. Telediagnosis of Pigmented Skin Tumors. Arch. Dermatol. 1999, 135, 1467–1471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perednia, D.A.; Brown, N.A. Teledermatology: One application of telemedicine. Bull. Med. Libr. Assoc. 1995, 83, 42–47. [Google Scholar] [PubMed]
- The Two-Week Wait Skin Cancer Pathway: Innovative Approaches to Support Early Diagnosis of Skin Cancer as Part of the NHS COVID-19 Recovery Plan. Available online: https://www.england.nhs.uk/wp-content/uploads/2022/04/B0829-suspected-skin-cancer-two-week-wait-pathway-optimisation-guidance.pdf (accessed on 18 June 2022).
- Deda, L.C.; Goldberg, R.H.; Jamerson, T.A.; Lee, I.; Tejasvi, T. Dermoscopy Practice Guidelines for Use in Telemedicine. NPJ Digit. Med. 2022, 5, 55. [Google Scholar] [CrossRef] [PubMed]
- Nittari, G.; Khuman, R.; Baldoni, S.; Pallotta, G.; Battineni, G.; Sirignano, A.; Amenta, F.; Ricci, G. Telemedicine Practice: Review of the Current Ethical and Legal Challenges. Telemed. e-Health 2020, 26, 1427–1437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nittari, G.; Savva, D.; Tomassoni, D.; Tayebati, S.K.; Amenta, F. Telemedicine in the COVID-19 Era: A Narrative Review Based on Current Evidence. Int. J. Environ. Res. Public Health 2022, 19, 5101. [Google Scholar] [CrossRef] [PubMed]
- Battineni, G.; Chintalapudi, N.; Amenta, F. Maritime Telemedicine: Design and Development of an Advanced Healthcare System Called Marine Doctor. J. Pers. Med. 2022, 12, 832. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.S.; Lappan, C.M.; Sperling, L.C.; Meyerle, J.H. Utilization of telemedicine in the U.S. military in a deployed setting. Mil. Med. 2014, 179, 1347–1353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.; Finnane, A.; Soyer, H.P. Recent Trends in Teledermatology and Teledermoscopy. Dermatol. Pract. Concept. 2018, 8, 214–223. [Google Scholar] [CrossRef] [PubMed]
- Abi-Saab, L.S.; Meirelles, B.H.S.; Demo, M.L.O. Economic Assessment of Teledermatology in the State of Santa Catarina—Brazil. Public Health 2021, 201, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Loh, C.H.; Tam, Y.C.; Oh, C.C. Teledermatology in the COVID-19 Pandemic: A Systematic Review. JAAD Int. 2021, 5, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Chuchu, N.; Dinnes, J.; Takwoingi, Y.; Matin, R.N.; Bayliss, S.E.; Davenport, C.; Moreau, J.F.; Bassett, O.; Godfrey, K.; O’Sullivan, C.; et al. Teledermatology for Diagnosing Skin Cancer in Adults. Cochrane Database Syst. Rev. 2018, 12, 12. [Google Scholar] [CrossRef] [PubMed]
- Finnane, A.; Dallest, K.; Janda, M.; Soyer, H.P. Teledermatology for the Diagnosis and Management of Skin Cancer. JAMA Dermatol. 2017, 153, 319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matteucci, P.; Pinder, R.; Magdum, A.; Stanley, P. Accuracy in Skin Lesion Diagnosis and the Exclusion of Malignancy. J. Plast. Reconstr. Aesthetic Surg. 2011, 64, 1460–1465. [Google Scholar] [CrossRef] [PubMed]
- Westbrook, R.H.; Goyal, N.; Gawkrodger, D.J. Diagnostic Accuracy for Skin Cancer: Comparison of General Practitioner with Dermatologist and Dermatopathologist. J. Dermatol. Treat. 2006, 17, 57–58. [Google Scholar] [CrossRef] [PubMed]
- Shariff, Z.; Roshan, A.; Williams, A.M.; Platt, A.J. 2-Week Wait Referrals in Suspected Skin Cancer: Does an Instructional Module for General Practitioners Improve Diagnostic Accuracy? Surgeon 2010, 8, 247–251. [Google Scholar] [CrossRef] [PubMed]
- Cox, N.H.; Madan, V.; Sanders, T. The, U.K. Skin Cancer “Two-Week Rule” Proforma: Assessment of Potential Modifications to Improve Referral Accuracy. Br. J. Dermatol. 2008, 158, 1293–1298. [Google Scholar] [CrossRef] [PubMed]
- Andrew, T.W.; Alrawi, M.; Lovat, P. Reduction in Skin Cancer Diagnoses in the UK during the COVID-19 Pandemic. Clin. Exp. Dermatol. 2020, 46, 145–146. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Characteristics | Value |
|---|---|
| Number (%) | 1943 (100%) |
| Age at diagnosis, yo, mean ± SD (95% CI) | 61.9 ± 18.3 |
| Female gender, n (%) | 1045 (53.8%) |
| Time to first being seen (days), median (IQR) | 12 (6) |
| Total skin malignant/premalignant lesions, n (%) | 513 (26.4%) |
| Skin primary malignancies (SCC, MM, BCC,), n (%) | 451 (23.2%) |
| SCC, n (%) | 150 (7.7%) |
| MM, n (%) | 54 (2.8%) |
| BCC, n (%) | 247 (12.7%) |
| Metastases and other secondary malignancies, n (%) | 10 (0.5%) |
| Premalignant conditions (Bowen’s disease/lentigo maligna), n (%) | 52 (2.7%) |
| Skin benign lesions, n (%) | 1430 (73.6%) |
| 14-day breach time, n (%) | 192 (9.9%) |
| 31-day breach time, n (%) | 2 (0.1%) |
| 62-day breach time, n (%) | 1 (0.05%) |
| No lesion present at the OPA, n (%) | 27/1943 (1.3%) |
| Declined the OPA, n (%) | 63/2037 (3.1%) |
| Deceased prior to the OPA, n (%) | 6/2037 (0.3%) |
| Duplicate referrals, n (%) | 12/2037 (0.6%) |
| Incorrect referrals, n (%) | 11/2037 (0.5%) |
| Unfit for the OPA, n (%) | 2/2037 (0.1%) |
| Characteristic | Face-to-Face-Consultation | Virtual Video Consultation | p-Value |
|---|---|---|---|
| Number (%) | 988 (50.8%) | 955 (49.2%) | |
| Age, years, mean ± SD (95% CI) | 62.5 ± 18.0 (61.4–63.7) | 61.2 ± 18.7 (60.0–61.5) | 0.09 |
| Female gender, n (%) | 535 (54.1%) | 510 (53.4%) | 0.75 |
| Time to first being seen (days), median (IQR) | 12 (5) | 12 (6) | 0.25 |
| Primary skin malignancy, n (%) | 240 (24.3%) | 211 (22.1%) | 0.25 |
| SCC, n (%) | 64 (6.5%) | 86 (9%) | 0.04 |
| MM, n (%) | 33 (3.3%) | 21 (2.2%) | 0.13 |
| BCC, n (%) | 143 (14.5%) | 104 (10.9%) | 0.02 |
| Metastases/other malignant lesions, n (%) | 3 (0.3%) | 7 (0.7%) | 0.21 |
| Premalignant lesions, n (%) | 30 (3%) | 22 (2.3%) | 0.32 |
| Benign lesions, n (%) | 715 (72.4%) | 715 (74.9%) | 0.21 |
| 14-day breach time, n (%) | 86 (8.7%) | 106 (11.1%) | 0.08 |
| 31-day breach time, n (%) | 1 (0.1%) | 1 (0.1%) | 1 |
| 62-day breach time, n (%) | 1 (0.1%) | 0 (0%) | 1 |
| Excluded from the study, n (%) | 43/2037 (4.2%) | 51/2037 (5.1%) | 0.34 |
| Deceased prior to the OPA, n (%) | 3/1031 (0.3%) | 3/1006 (0.3%) | 1 |
| Declined the OPA, n (%) | 34/1031 (3.3%) | 29/1006 (2.9%) | 0.61 |
| Incorrect referral, n (%) | 2/1031 (0.2%) | 9/1006 (0.9%) | 0.03 |
| Duplication, n (%) | 3/1031 (0.3%) | 9/1006 (0.9%) | 0.09 |
| Unfit for the OPA, n (%) | 1/1031 (0.1%) | 1/1006 (0.1%) | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chiru, M.-R.; Hindocha, S.; Burova, E.; Bejan, G.-C.; Manea, L.-M.; Ghilencea, L.-N. Management of the Two-Week Wait Pathway for Skin Cancer Patients, before and during the Pandemic: Is Virtual Consultation an Option? J. Pers. Med. 2022, 12, 1258. https://doi.org/10.3390/jpm12081258
Chiru M-R, Hindocha S, Burova E, Bejan G-C, Manea L-M, Ghilencea L-N. Management of the Two-Week Wait Pathway for Skin Cancer Patients, before and during the Pandemic: Is Virtual Consultation an Option? Journal of Personalized Medicine. 2022; 12(8):1258. https://doi.org/10.3390/jpm12081258
Chicago/Turabian StyleChiru, Maria-Roxana, Sandip Hindocha, Ekaterina Burova, Gabriel-Cristian Bejan, Laura-Maria Manea, and Liviu-Nicolae Ghilencea. 2022. "Management of the Two-Week Wait Pathway for Skin Cancer Patients, before and during the Pandemic: Is Virtual Consultation an Option?" Journal of Personalized Medicine 12, no. 8: 1258. https://doi.org/10.3390/jpm12081258
APA StyleChiru, M.-R., Hindocha, S., Burova, E., Bejan, G.-C., Manea, L.-M., & Ghilencea, L.-N. (2022). Management of the Two-Week Wait Pathway for Skin Cancer Patients, before and during the Pandemic: Is Virtual Consultation an Option? Journal of Personalized Medicine, 12(8), 1258. https://doi.org/10.3390/jpm12081258