
Digital Twins in Healthcare: Is It the Beginning of a New Era of Evidence-Based Medicine? A Critical Review

 , ,
, ,
Abstract
:1. Introduction
2. Concept and Current Applications of DTs in Healthcare
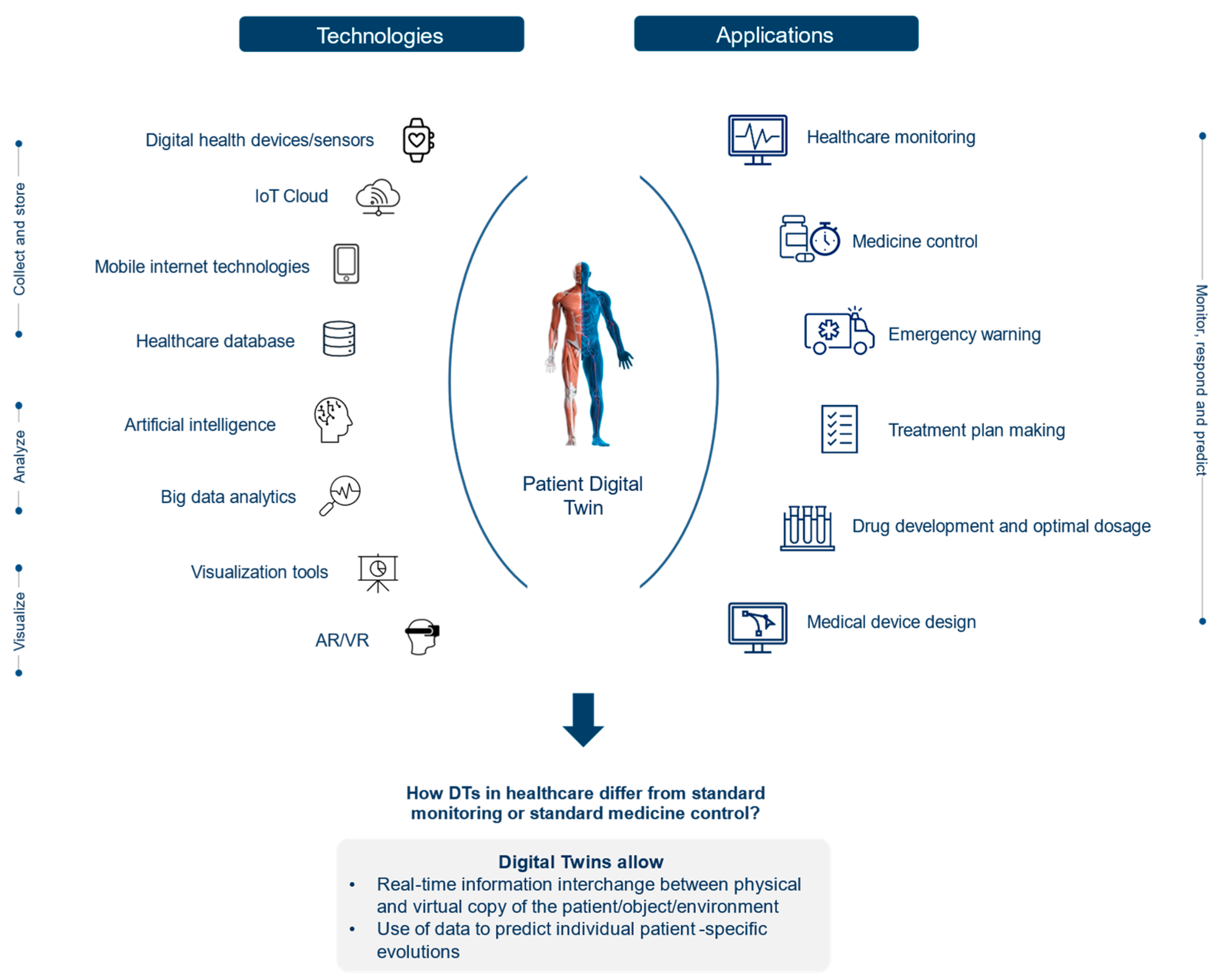
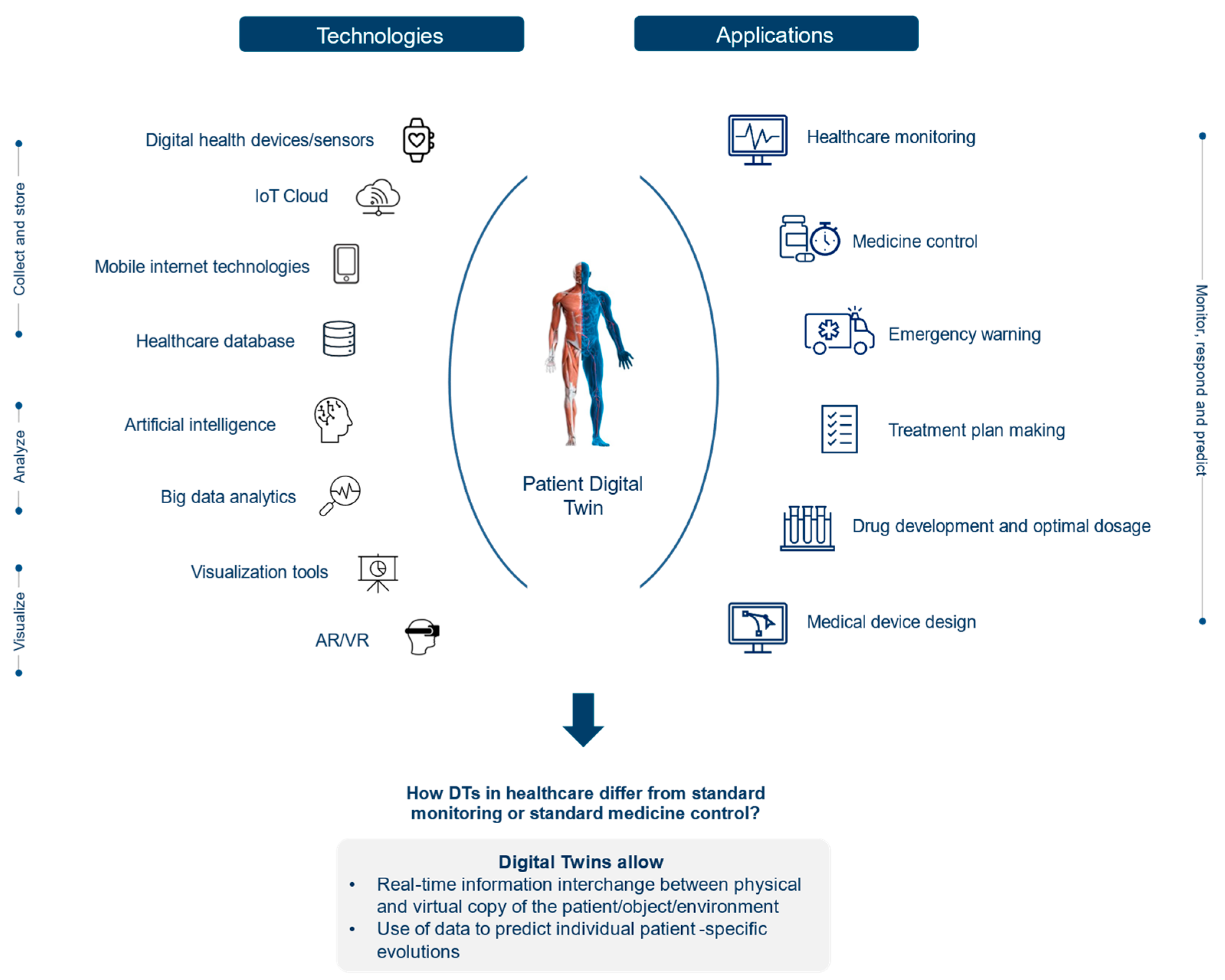
2.1. Concept of DTs in Healthcare
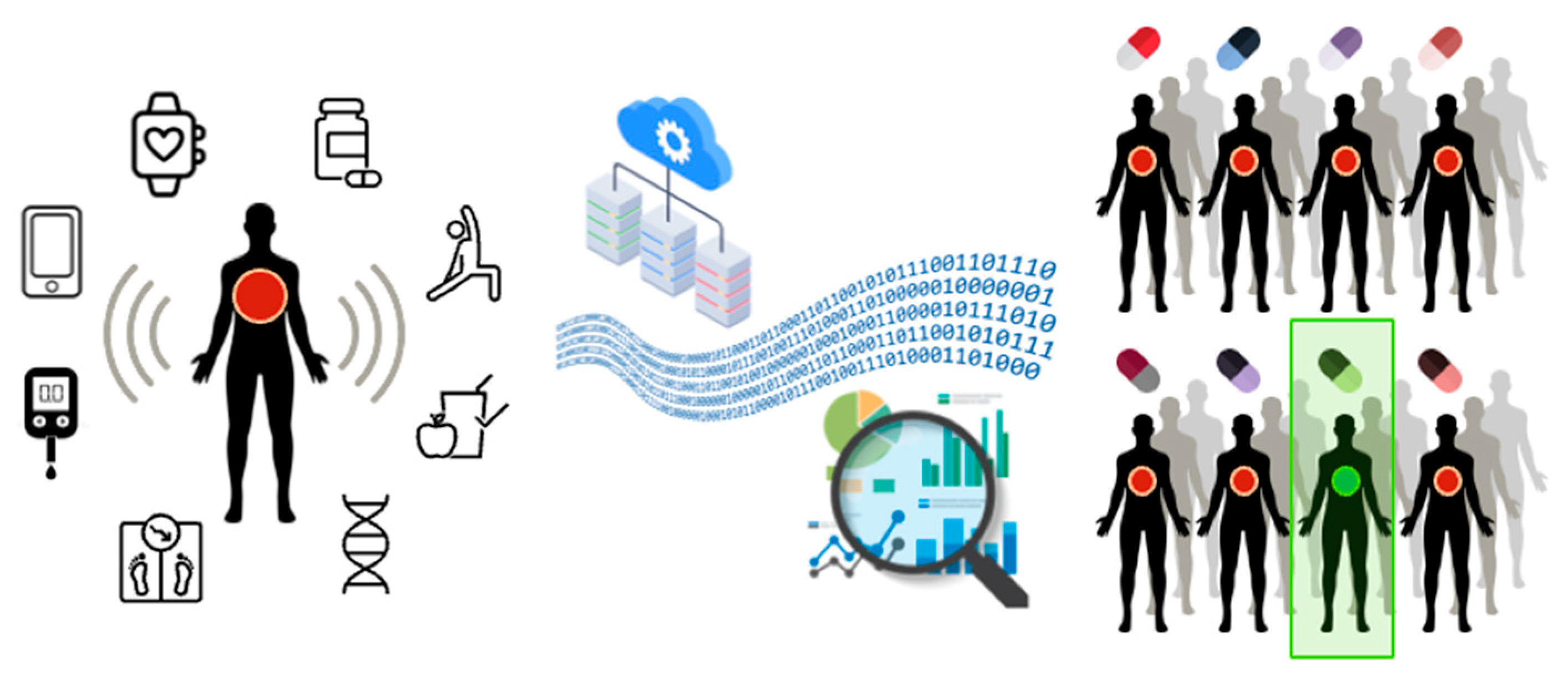
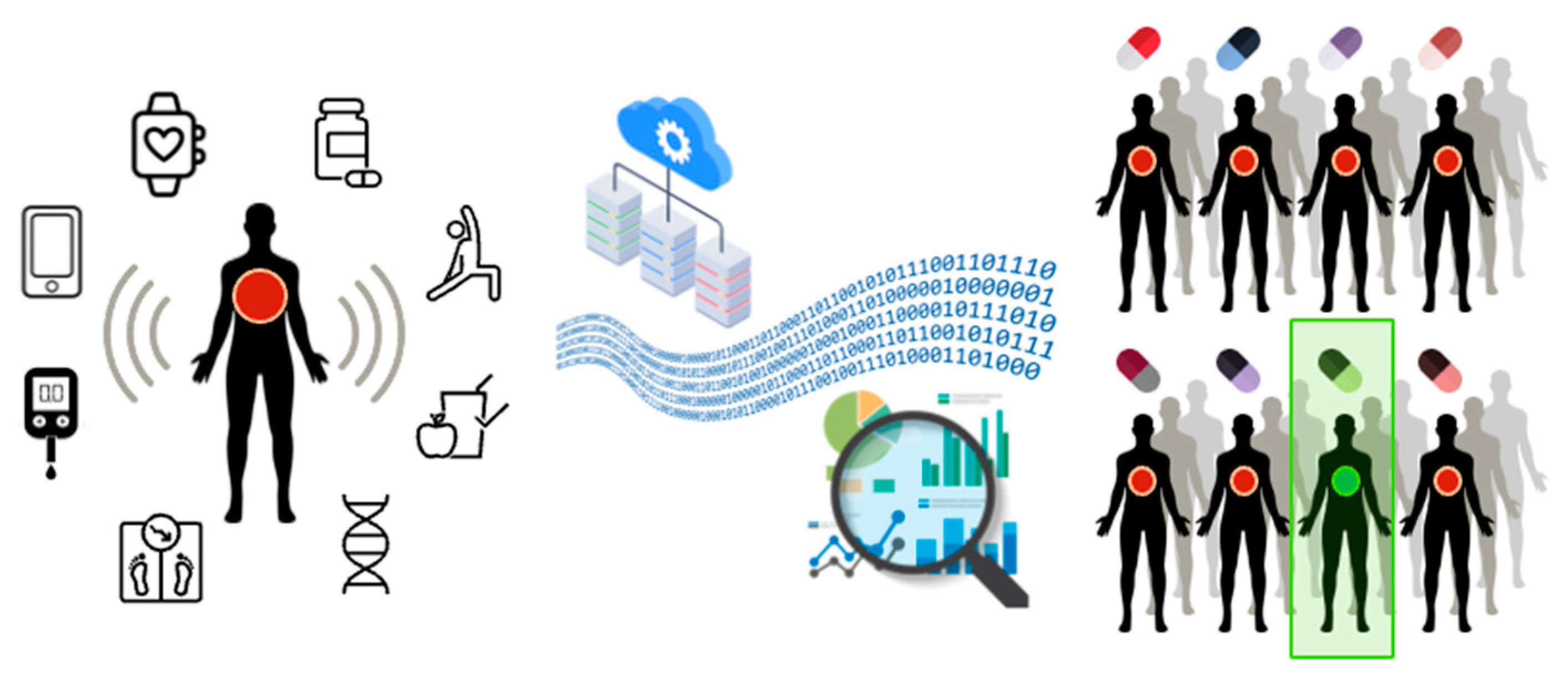
2.1.1. Data Generation for DT Implementation
2.1.2. Technology for DT Implementation
2.2. Current Applications of DTs in Healthcare
2.2.1. Precision Medicine and Support to Medical Decision Making
2.2.2. Clinical Trials Design
2.2.3. Optimizing Hospital Operations
3. Open Issues and Challenges
3.1. Ethical Issues and Policy Considerations
3.2. Technical Limitations
3.3. Social Barriers
4. Discussion
4.1. Use of DTs in Clinical Trials
4.2. Equity Issues
4.3. Social Issues Related to the Affordability of DTs
4.4. Social Issues Related to the Potential Replacement of Clinicians
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barricelli, B.R.; Casiraghi, E.; Fogli, D. A survey on digital twin: Definitions, characteristics, applications, and design implications. IEEE Access 2019, 7, 167653–167671. [Google Scholar] [CrossRef]
- Wickramasinghe, N.; Jayaraman, P.P.; Zelcer, J.; Forkan, A.R.M.; Ulapane, N.; Kaul, R.; Vaughan, S. A vision for leveraging the concept of digital twins to support the provision of personalised cancer care. IEEE Internet Comput. 2021, 1. [Google Scholar] [CrossRef]
- Glaessgen, E.; Stargel, D. The Digital Twin Paradigm for Future NASA and U.S. Air Force Vehicles. In Proceedings of the 53rd AIAA/ASME/ASCE/AHS/ASC Structures, Structural Dynamics, and Materials Conference 20th AIAA/ASME/AHS Adaptive Structures Conference 14th AIAA, Honolulu, HI, USA, 23–26 April 2012; p. 1818. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Zhang, L.; Yang, Y.; Zhou, L.; Ren, L.; Wang, F.; Liu, R.; Pang, Z.; Deen, M.J. A Novel Cloud-Based Framework for the Elderly Healthcare Services Using Digital Twin. IEEE Access 2019, 7, 49088–49101. [Google Scholar] [CrossRef]
- Grieves, M. Digital Twin: Manufacturing Excellence through Virtual Factory Replication. 2014. Available online: https://www.researchgate.net/publication/275211047_Digital_Twin_Manufacturing_Excellence_through_Virtual_Factory_Replication (accessed on 22 December 2021).
- Schwartz, S.M.; Wildenhaus, K.; Bucher, A.; Byrd, B. Digital Twins and the Emerging Science of Self: Implications for Digital Health Experience Design and “Small” Data. Front. Comput. Sci. 2020, 2, 31. [Google Scholar] [CrossRef]
- SDA Bocconi LIFT Lab. LIFT Radar 2021. Available online: https://www.sdabocconi.it/en/faculty-research/labs-and-research-centers/lift-lab/activities (accessed on 22 December 2021).
- IEEE Computer Society. IEEE Computer Society’s Top 12 Technology Trends for 2020. 2019. Available online: https://www.prnewswire.com/news-releases/ieee-computer-societys-top-12-technology-trends-for-2020-300971863.html (accessed on 22 December 2021).
- Voigt, I.; Inojosa, H.; Dillenseger, A.; Haase, R.; Akgün, K.; Ziemssen, T. Digital Twins for Multiple Sclerosis. Front. Immunol. 2021, 12, 669811. [Google Scholar] [CrossRef] [PubMed]
- Raden, N. Digital Twins for Personalized Medicine—A Critical Assessment. 2020. Available online: https://diginomica.com/digital-twins-personalized-medicine-critical-assessment (accessed on 22 December 2021).
- CBinsights. 5 Ways Digital Twins Could Improve Healthcare. 2020. Available online: https://www.cbinsights.com/research/digital-twins-technology-healthcare/ (accessed on 22 December 2021).
- Corral-Acero, J.; Margara, F.; Marciniak, M.; Rodero, C.; Loncaric, F.; Feng, Y.; Gilbert, Y.; Fernandes, J.F.; Bukhari, H.A.; Wajdan, A.; et al. The ‘Digital Twin’ to enable the vision of precision cardiology. Eur. Heart J. 2020, 41, 4556–4564. [Google Scholar] [CrossRef] [PubMed]
- Elayan, H.; Aloqaily, M.; Guizani, M. Digital Twin for Intelligent Context-Aware IoT Healthcare Systems. IEEE Internet Things J. 2021, 8, 16749–16757. [Google Scholar] [CrossRef]
- Tao, F.; Sui, F.; Liu, A.; Qi, Q.; Zhang, M.; Song, B.; Guo, Z.; Lu, S.C.-Y.; Nee, A.Y.C. Digital twin-driven product design framework. Int. J. Prod. Res. 2019, 57, 3935–3953. [Google Scholar] [CrossRef] [Green Version]
- Boulos, M.K.; Zhang, P. Digital Twins: From Personalised Medicine to Precision Public Health. J. Pers. Med. 2021, 11, 745. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Lu, R.; Guan, Y.; Zhang, S.; Shao, J. Towards Private Similarity Query based Healthcare Monitoring over Digital Twin Cloud Platform. In Proceedings of the 2021 IEEE/ACM 29th International Symposium on Quality of Service (IWQOS), Tokyo, Japan, 25–28 June 2021; pp. 1–10. [Google Scholar] [CrossRef]
- Erol, T.; Mendi, A.F.; Dogan, D. The Digital Twin Revolution in Healthcare. In Proceedings of the 2020 4th International Symposium on Multidisciplinary Studies and Innovative Technologies (ISMSIT), Istanbul, Turkey, 22–24 October 2020; pp. 1–7. Available online: https://ieeexplore.ieee.org/document/9255249 (accessed on 22 December 2021).
- van Houten, H. How a Virtual Heart Could Save Your Real One. 2018. Available online: https://www.philips.com/a-w/about/news/archive/blogs/innovation-matters/20181112-how-a-virtual-heart-could-save-your-real-one.html (accessed on 22 December 2021).
- The Stanford Virtual Heart–Revolutionizing Education on Congenital Heart Defects. Available online: https://www.stanfordchildrens.org/en/innovation/virtual-reality/stanford-virtual-heart (accessed on 22 December 2021).
- Swedish Digital Twin Consortium. Available online: https://www.sdtc.se/-digital-twins (accessed on 22 December 2021).
- James, L. Digital twins will revolutionise healthcare: Digital twin technology has the potential to transform healthcare in a variety of ways – improving the diagnosis and treatment of patients, streamlining preventative care and facilitating new approaches for hospital planning. Eng. Technol. 2021, 16, 50–53. [Google Scholar] [CrossRef]
- Erö, C.; Gewaltig, M.-O.; Keller, D.; Markram, H. A Cell Atlas for the Mouse Brain. Front. Neuroinf. 2018, 12, 84. [Google Scholar] [CrossRef] [PubMed]
- Laubenbacher, R.; Sluka, J.P.; Glazier, J.A. Using digital twins in viral infection. Science 2021, 371, 1105–1106. [Google Scholar] [CrossRef] [PubMed]
- Croatti, A.; Gabellini, M.; Montagna, S.; Ricci, A. On the Integration of Agents and Digital Twins in Healthcare. J. Med. Syst. 2020, 44, 161. [Google Scholar] [CrossRef] [PubMed]
- Shamanna, P.; Saboo, B.; Damodharan, S.; Mohammed, J.; Mohamed, M.; Poon, T.; Kleinman, N.; Thajudeen, M. Reducing HbA1c in type 2 diabetes using digital twin technology-enabled precision nutrition: A retrospective analysis. Diabetes Ther. 2020, 11, 2703–2714. [Google Scholar] [CrossRef] [PubMed]
- Unlearn, A.I. AI Driven Approaches to Trial Design Innovation Enabling Faster, More Efficient Trials with Digital Twins. Available online: https://www.unlearn.ai/solutions#digital-twin (accessed on 22 December 2021).
- Popa, E.O.; van Hilten, M.; Oosterkamp, E.; Bogaardt, M.-J. The use of digital twins in healthcare: Socio-ethical benefits and socio-ethical risks. Life Sci. Soc. Policy 2021, 17, 6. [Google Scholar] [CrossRef] [PubMed]
- Reis, L.; Maier, C.; Mattke, J.; Creutzenberg, M.; Weitzel, T. Addressing User Resistance Would Have Prevented a Healthcare AI Project Failure. MIS Q. Exec. 2020, 19, 279–296. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Target Organ/Disease | Reference (Company, Journal etc.) | Description |
|---|---|---|
| Heart [1] | Living Heart Project, Dassault Systèmes | The Living Heart Project is the first DT organ considering all aspects of the heart’s functionality, such as blood flow, mechanics, and electrical impulses. The 3D model of the organ has built with a 2D scan of the heart. The Living Heart Model on the 3DEXPERIENCE platform can be used to create new ways to design and test new devices and drug treatments. For instance, physicians can run hypothetical scenarios like adding a pacemaker or reversing the heart chambers to predict the outcome of treatment on the patient. |
| Heart [12] | CardioInsight, Medtronic | The CardioInsight Noninvasive 3D Mapping System collects chest electrocardiogram (ECG) signals and combines these signals with computerized tomography (CT) scan data to produce and display simultaneous 3-D cardiac maps. The mapping system enables physicians to characterize abnormal rhythms of the heart through a personalized heart model. |
| Heart [1] | Siemens Healthineers | Another heart DT has been developed by Siemens Healthineers and used for research purposes by Cardiologists of the Heidelberg University Hospital (HUH) in Germany. Although the first study is still in the data evaluation process, preliminary results are promising. Siemens Healthineers developed the DT model by exploiting a massive database containing more than 250 million annotated images, reports, and operational data. The AI-based DT model enables digital heart design based on patient data with the same conditions of the given patient (size, ejection fraction, and muscle contraction). |
| Brain [17] | Blue Brain Project, EPFL and Hewlett Packard Enterprise | Hewlett Packard Enterprise, partnering with Ecole Polytechnique Fédérale de Lausannes (EPFL), builds a DT of brain called the Blue Brain Project. The project is one of the sub-projects of the Human Brain Project and aims to build biologically detailed digital reconstructions (computer models) and simulations of the mouse brain. In 2018, researchers published the first 3D cell atlas for the entire mouse brain [22]. |
| Human air-way system [1] | Oklahoma State University’s Computational Biofluidics and Biomechanics Laboratory | Researchers developed a prototype of human DT, named ‘‘virtual human V1.0”, with the high-resolution human respiratory system covering the entire conducting and respiratory zones, lung lobes, and body shell. The project aims to study and increase the success rate of cancer-destroying drugs in targeting tumor-only locations. |
| Brain aneurysm and surrounding blood vessels [1] | Sim&Cure | Sim&Cure developed a DT to treat aneurysms, which are enlarged blood vessels that can result in clots or strokes. DT of the aneurysm and the surrounding blood vessels (represented by a 3D model) allow brain surgeons to run simulations and understand the interactive relationship between the implant and the aneurysm. Although preliminary trials have shown promising results, further evaluation is required. |
| Multiple Sclerosis (MS) [9] | Frontiers in Immunology (journal) | Multiple sclerosis, also called the ‘disease of a thousand faces’, has high complexity, multidimensionality, and heterogeneity in disease progression and treatment options among patients. This results in extensive data to study the disease. Human DTs are promising in the case of precision medicine for people with MS (pwMS), allowing healthcare professionals to handle this big data, monitor the patient effectively, and provide more personalized treatment and care. |
| Viral Infection [23] | Science (journal) | Human DTs can predict the viral infection or immune response of a patient infected with a virus by integrating known human physiology and immunology with population and individual clinical data into AI-based models. |
| Trauma Management [24] | Journal of Medical Systems (journal) | Trauma management is highly critical among time-dependent pathologies. DTs can participate from the pre-hospital phase, where the physician provides the patient first aid and transfers them to the hospital emergency department, to the operative phase, where the trauma team assists the patient in hospital emergency. Although there is no real implementation yet, a system prototype has been developed. |
| Diabetes [25] | Diabetes (journal) | Human DT can also participate in diabetes management. California-based start-up Twin Health has applied DTs by modeling patient metabolism. The DT model tracks nutrition, sleep, and step changes and monitors patients’ blood sugar levels, liver function, weight, and more. Ongoing clinical trials show that daily precision nutrition guidance based on a continuous glucose monitoring system (CGM), food intake data, and machine learning algorithms can benefit patients with type 2 diabetes. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Armeni, P.; Polat, I.; De Rossi, L.M.; Diaferia, L.; Meregalli, S.; Gatti, A. Digital Twins in Healthcare: Is It the Beginning of a New Era of Evidence-Based Medicine? A Critical Review. J. Pers. Med. 2022, 12, 1255. https://doi.org/10.3390/jpm12081255
Armeni P, Polat I, De Rossi LM, Diaferia L, Meregalli S, Gatti A. Digital Twins in Healthcare: Is It the Beginning of a New Era of Evidence-Based Medicine? A Critical Review. Journal of Personalized Medicine. 2022; 12(8):1255. https://doi.org/10.3390/jpm12081255
Chicago/Turabian StyleArmeni, Patrizio, Irem Polat, Leonardo Maria De Rossi, Lorenzo Diaferia, Severino Meregalli, and Anna Gatti. 2022. "Digital Twins in Healthcare: Is It the Beginning of a New Era of Evidence-Based Medicine? A Critical Review" Journal of Personalized Medicine 12, no. 8: 1255. https://doi.org/10.3390/jpm12081255
APA StyleArmeni, P., Polat, I., De Rossi, L. M., Diaferia, L., Meregalli, S., & Gatti, A. (2022). Digital Twins in Healthcare: Is It the Beginning of a New Era of Evidence-Based Medicine? A Critical Review. Journal of Personalized Medicine, 12(8), 1255. https://doi.org/10.3390/jpm12081255