1. Introduction
Syncopes are defined as a transient complete loss of consciousness (TLOC) caused by temporary cerebral hypoperfusion, with a rapid onset and short duration, and a spontaneous full recovery [
1]. This condition represents a very common phenomenon with a lifetime prevalence of 30–50% [
1]. The incidence of recurrent syncopes is high, with approximately 20% in 24 months [
2]. In the study by Zimmermann et al., the highest predictive value for the recurrence of syncope was a history of more than three syncopes. More importantly, according to this dataset, patients with three or more syncopes had an unfavorable outcome (i.e., death or major adverse cardiovascular events (MACEs)) [
2]. Barbic et al. showed a risk of a syncope relapse after an initial syncope, leading to presentation in an emergency department of over 20% in 5 years [
3]. Solbiati et al. reported in a review including 25 studies that the risk for a short-term (10 days) incidence for major cardiac events and death was approximately 10% [
4].
The diagnostic approach to elucidate the origin of syncope includes the implantation of implantable loop recorders (ILRs) to be able to correlate paroxysmal ECG abnormalities detected with the loop recorders with clinical symptomatology. For this reason, ILRs have proven their superiority over conventional diagnostic tools such as external loop recorders and Holter ECGs [
5,
6,
7,
8]. Solbiati et al. performed a systematic review including 49 studies examining the diagnostic yield of ILRs [
9]. The authors underlined that an underlying cause could be found in approximately 50% of patients with unexplained syncopes. In approximately half of these patients, arrhythmia could be identified as the reason underlying the high diagnostic value of these devices. These results have led to a class IA indication for ILR implantation in most patients with unexplained syncopes. In the 2018 ESC Guidelines on diagnosis and management of syncope, if no high-risk circumstances exist (severe structural heart diseases or sudden onset with palpitation immediately followed by syncope), recommend the implantation of a pacemaker or ICD instead [
1]. This is further important as subjective heart racing often occurs in the temporal context of syncope and to that effect, harmless and dangerous reasons for these symptoms have to be distinguished. Sinus tachycardia is the most important reason for subjective heart racing, and psychological factors may play a significant role in the offspring, symptom maintenance and treatment efficacy. This knowledge has led to the development of psychocardiology as its own sub-specialty with its own specialized therapies [
10]. More importantly, heart racing can also hint at a ventricular arrhythmia origin, which puts patients at serious risk.
In clinical routine, patients with unclear syncopes are often young and present with anxiety and/or depressive symptoms. Linzer et al. reported that syncope itself causes psychosocial impairment comparable to chronic active diseases, such as severe rheumatoid arthritis, independent from comorbid diseases or age [
11]. Kouakam reported a very high prevalence of up to 50% for underlying psychiatric comorbidities in patients referred for repetitive unexplained syncopes, especially for anxiety disorders [
12]. The authors further reported a 1.7% higher risk for recurrent syncopes during a three-year follow-up of patients with a respective psychiatric disorder. Similar results were reported by Ventura et al., who found even higher rates of psychiatric disorders in 81% of participants of a small cohort of patients presenting with recurrent syncopes [
13]. Patients were offered psychotherapeutic treatment after a diagnostic set-up, which was ultimately refused by most patients. Interestingly, patients who received treatment were free of recurrent syncopes during the follow-up, while patients who refused treatment experienced further syncopes, indicating the need for psychological interventions in this respect. A similar observation was reported by Magnavita et al., who showed that the risk for syncope was higher in patients with occupational distress, a low sleep quality and poor mental health. The authors reasoned that health promotion interventions could reduce syncopes via reducing sleep quality and reducing (work-associated) stressors [
14].
Yet, our clinical observation is that syncopes often stop after ILR implantation or their frequency of occurrence is reduced. This suggests that the recurrence of syncope may be influenced by psychological factors, such as anxiety, depression, personality traits, quality of life, social comparison or trust in medical personnel or devices. Against this background, we aimed at evaluating psychological factors in patients with implantable loop recorders to examine the extent to which they predict syncopes of cardiac or non-cardiac origin.
2. Methods
To investigate the association between psychological factors and recurrent syncopes in patients with implantable loop recorders, we included patients being implanted between January 2018 and November 2021 at our tertiary care center after extensive conservative diagnostic measures, as well as an invasive electrophysiological study, not revealing a cardiac cause of syncope in a retrospective manner. In patients with a typical anamnesis for reflex syncope or orthostatic hypotension, we performed a head-up tilt test. A carotid sinus massage was not regularly performed. Indication for implantation was a single high-risk syncope or multiple unexplained syncopes not cleared up by the diagnostic set-up mentioned before. All ILRs were implanted with a class I or IIa indication according to the current guidelines. Further inclusion criteria were an age over 18 years, availability and willingness for a telephone interview to be performed, good knowledge and understanding of the German language and a complete dataset. Exclusion criteria were insufficient language skills, a mental disability (impossibility of informed consent) and a prior explantation of the ILR without arrhythmia detection leading to ICD or pacemaker implantation. Following approval by the local ethics committee (reference number: 2021-087-f-S), data on patient characteristics and underlying medical history were extracted from patient records. After that, a standardized telephone interview was performed with patients who had given informed consent. The battery consisted of the following validated psychometric tools:
2.1. Patient Health Questionnaire (PHQ-9)
The PHQ-9 is a module for the diagnosis of depressive disorders from the Patient Health Questionnaire (PHQ-D), and uses 9 items to assess the presence and severity of depressive symptoms over the last 2 weeks on a 4-point Likert scale [
15,
16].
2.2. Generalized Anxiety Disorder Scale (GAD-7)
The GAD-7 is a brief assessment tool used to evaluate anxiety, and has been used in clinical as well as general populations extensively [
17,
18]. The questionnaire assesses feelings of anxiety and how often they occurred over the last 2 weeks on a 4-point Likert scale.
2.3. Trust in Medical Professionals
The scale used in this trial was a 5-item version, which measures the trust patients put in their physicians [
19]. Answers were given on a 5-point Likert scale.
2.4. Modified Florida Patient Acceptance Scale (FPAS)
The FPAS was initially developed for patients with implantable cardioverter-defibrillators, and has been used to assess the acceptance of the implanted device and the extent to which it influences daily life. As the items do not focus on specific functions of ICDs, we used a modified version, replacing ICD with the more general term “device”, meaning the ILR. The FPAS initially used 18 items, of which 3 were eliminated in the course of use as the discriminatory power between different psychological constructs was not high enough. Therefore, the version used in our trial comprised 15 items reflecting 4 factors (return to life, device-related distress, positive appraisal and body image concerns), which were answered on a 5-point Likert scale.
2.5. Short Version of the Iowa–Netherlands Comparison Orientation Measure (INCOM)
To assess the tendency by patients to compare themselves with others, we used the validated short form of the INCOM, which contains 6 items [
20]. The scale differentiates between two comparisons of abilities and comparisons of opinions.
2.6. Big Five Inventory (BIF-10)
The BIF-10 allows for the measuring of personality traits with only 10 items. As can be concluded from its name, it was theoretically founded on the five-factor model of personality, also known as the Big Five or OCEAN model (O—openness; C—conscientiousness; E—extraversion; A—agreeableness; N—neuroticism), and each factor was assessed with two items [
21].
2.7. Short-Form Health Survey (SF-12)
The SF-12 is a non-disease-specific questionnaire using 12 items to assess up to 8 dimensions of health and quality of life (physical functioning, social functioning, role limitation (physical), role limitation (emotional), bodily pain, general health, vitality and mental health) and was developed as a short form of the SF-36, extracting the most specific item(s) for the respective dimension [
22].
2.8. Statistical Analysis
Categorical variables were expressed as frequencies with percentages, while continuous variables were expressed as means with standard deviations (SDs). Chi-square-test or Fisher’s exact test were used to compare categorical variables and Mann–Whitney U test for continuous variables between patients from different groups. Therefore, we divided the patients into three groups: patients with recurrent syncopes of then-proven arrhythmic cause (group 1), patients with recurrent syncopes without arrhythmic correlation (group 2) or patients without recurrent syncopes (group 3). Multi-variable logistic regression analysis was used to examine which psychological or demographic characteristics were independently associated with recurrent syncopes without pathological ECG findings during follow-up.
2.9. Follow-Up
The follow-up duration was approximately 2 years (710 ± 430 days). Patients were scheduled for telemetric monitoring of the ILR every three months, and in case of the occurrence of an arrhythmia transmitted by the ILR or a symptom activation of the patient, at our clinic. In-person aftercare was performed every year, including anamnesis, clinical examination, 12-lead ECG and ILR interrogation.
3. Results
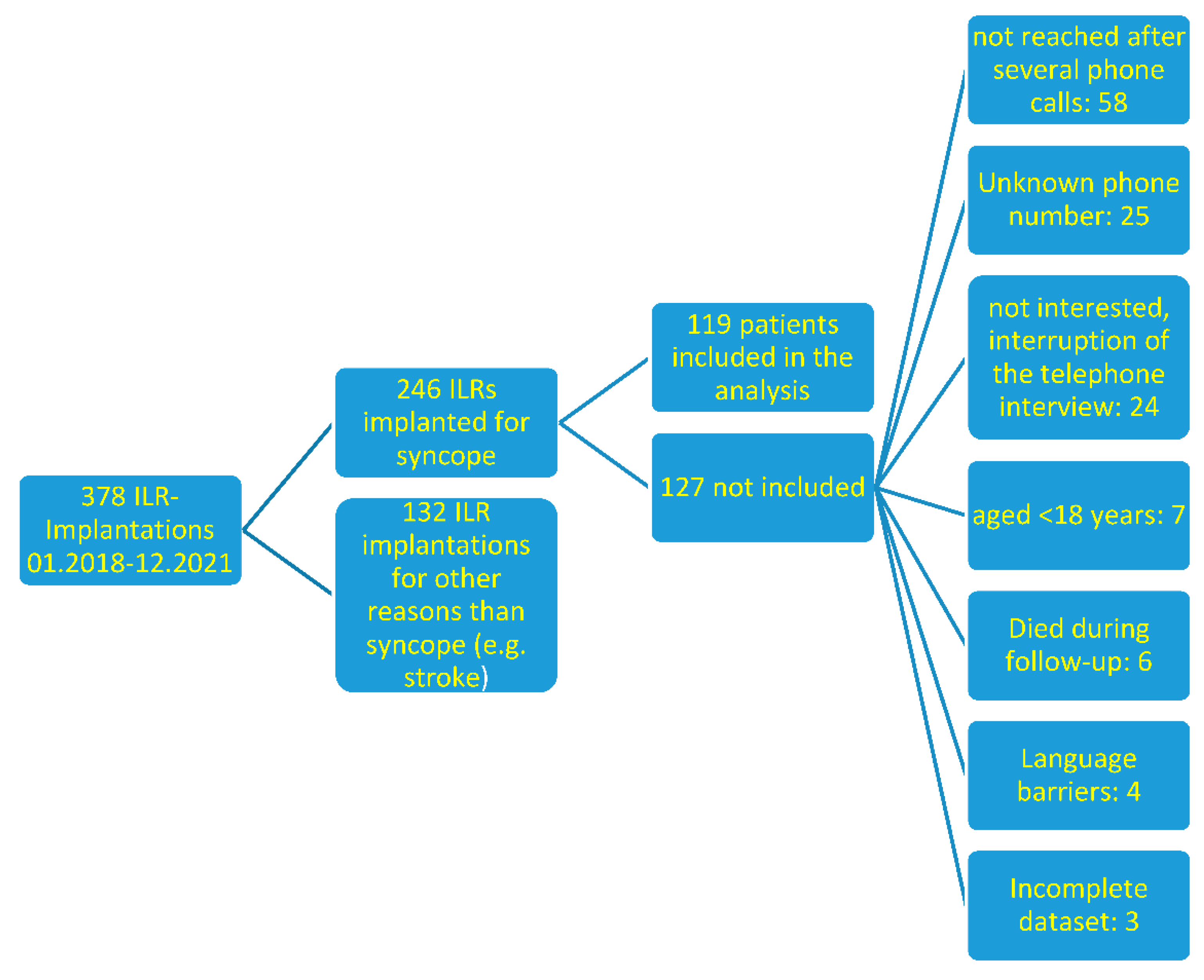
After screening our clinical device implantation registry for implanted loop recorders between January 2018 and December 2021, we identified 378 patients that were possibly suitable for study inclusion. In total, 119 patients were reached out to for a telephone interview and agreed to participate in the study. For detailed information about the patient selection process, please see
Figure 1.
The follow-up duration was approximately 2 years (710 ± 430 days), and the gender ratio was approximately 50/50%. The mean patient age was 54.8 ± 18.6 years. Most patients had no evidence of structural heart disease (84%), and normal LV function (92%). A detailed description of patient characteristics is shown in
Table 1.
Levels of depressive (5.7 ± 4.5 of a maximum of 36 points) and anxious (4.3 ± 4.1 of a maximum of 28 points) symptoms were recorded with the questionnaires mentioned above. Trust in the medical professionals (18.8 ± 3.8 of possible 25 points) and in the ILR as a device was very high (68.0 ± 7.1 of possible 75 points). There were no relevant body image concerns induced by the ILR (9.9/10 points, lowest score 7/10) and most patients appreciated the ILR as a potential contribution to achieving or restoring a better health status (17.2 ± 2.7 of possible 20 points).
To examine our hypothesis that psychological factors as well as patient characteristics had a predictive value on the recurrence of arrhythmic or psychogenic syncope, we performed linear regression analyses using the recurrence of each syncope type as the dependent variable. There were only two significant factors associated with arrhythmic syncope during follow-up using the variables analyzed. One was the presence of a known structural heart disease at the time of implantation (p = 0.04), and the other one was a low level of neuroticism in the BF-10 questionnaire (p = 0.02). An association with a low perception of physical functioning reached borderline significance (p = 0.07). Concerning the occurrence of non-arrhythmic syncopes, the only significantly associated variable was physical functioning (p = 0.02). Two variables reached borderline significance—a low physical role function (p = 0.06) and a high value for cooperation (p = 0.09). The social comparison orientation and present quality of life did not significantly predict the recurrence of syncope.
In a comparison of three patient groups (patients with recurrent syncopes proven to be arrhythmic (group one), patients with recurrent syncopes without arrhythmic cause (group two) and patients without recurrence (group three)), we showed that levels for anxiety and depressive symptoms were significantly higher in group one than in group two. In addition to that, levels of neuroticism were also higher and quality of life was lower in group two compared to patients from group one. For a more detailed presentation of all results of this analysis, please look at
Table 2,
Table 3 and
Table 4.
4. Discussion
In our study, we found a significantly higher level of anxious and depressive symptoms in patients with recurrent syncopes of non-arrhythmic origin and a worse quality of life. However, we did not find single factors serving as possible future predictors of these non-arrhythmic syncopes during the regression analysis, except for the presence of structural heart disease before implantation. This factor was associated with a later arrhythmia in the ILRs, leading to the implantation of either a pacemaker or an ICD, which is in line with existing data [
2]. There were no other factors with significant association.
Concerning non-arrhythmic syncopes, a low subjective perception of physical functioning and physical role functioning showed a significant association with the occurrence of non-arrhythmic syncopes during follow-up. This is relevant, as patients suffering from an arrhythmic syncope were exposed to higher levels of structural heart disease and hypertension and, therefore, probably had higher levels of physical impairment than the aforementioned group. Furthermore, patients with non-arrhythmic syncopes had higher levels of anxiety or depressive symptoms than patients with arrhythmic syncopes. Furthermore, non-arrhythmic recurrent syncope was associated with a worse quality of life.
In addition to that, we needed to consider that other psychological factors that we did not examine in our study may play a significant role in the recurrence and risk for syncope. Ferguson showed in different cohorts that fainting and vasovagal syncope had a negative association to intellect, but a positive correlation to perceived threat and the fear of loss. Emotional stability was negatively correlated with the risk of fainting [
23]. In our cohort, personality traits, apart from neuroticism, were not associated with the recurrence of syncope or the type of underlying origin, which may also have been due to the small number of patients included. These syncopes might be possibly addressed by psychological interventions, so that a thorough identification of possible stressors and risk factors is mandatory in the assessment of syncopes, in line with the results by Magnavita et al. described in the introduction [
14].
In a retrospective analysis, Walsh et al. showed in more than 1400 patients referred to a syncope unit that a history of psychiatric disorders was associated with a later diagnosis of psychogenic pseudosyncope (PPS) [
24]. Similar results were reported in the Irish Longitudinal Study of Aging (TILDA) [
25], where the authors identified the fear of falling as a major contributor to quality of life and a significant predictor of syncopes, once again underlining the possible potential of psychotherapeutic interventions in the treatment of patients with recurrent syncope [
25]. A small pilot trial from Brazil revealed an improvement in quality of life and a reduction in syncope recurrence in a randomized design, further emphasizing the meaningfulness of the approach [
26]. In our trial, we assessed many different psychological factors and underlying psychometric concepts for the possible prediction of psychogenic factors leading to syncopes, and could identify an association in non-arrhythmic syncopes to psychological findings such as higher anxiety and depression. These findings might help to improve risk stratification concerning the probability of arrhythmic or non-arrhythmic syncopes. The identification of psychogenic syncopes remains of high importance to provide early diagnosis and organize qualified therapeutic support for these patients. It is, however, very important to underline one of the main results of this study, that a psychogenic syncope still remains a diagnosis by exclusion and that all patients, regardless of underlying psychological pathologies, may not be pre-judged, but have to be carefully examined for underlying causes such as arrhythmias. This is illustrated by the fact that no less than one-fifth of the patients with an ILR were in need of a pacemaker or ICD during a follow-up of approximately two years. The use of the ILR was definitely a strength of this study, as it guaranteed a correct differentiation between different reasons for syncope.
5. Limitations
On the other hand, the design was retrospective. The patients were not consecutively included, but depended on their willingness to perform a telephone interview. Furthermore, psychological factors could, for the sake of the study design, only be associated with the later occurrence of arrhythmic or non-arrhythmic syncope, but not serve as true predictors. In addition to that, the trial used a cohort design without a control group to be compared to, which also has to be taken into account when looking at the results.
For an early identification of PPS, a detailed history, optimally supported by an observer, is helpful [
27]. However, in our study, we did not use more elaborated diagnostic measures such as video recording during the tilt test, in order to further support the finding of PPS, so that we could discriminate only between syncopes of arrhythmic or non-arrhythmic origin and no other entities within the non-arrhythmic ones.
In addition to that, the number of patients could be too low, leading to statistical power issues and also the possibly of false negative results.
6. Conclusions
Future studies should apply longitudinal and prospective designs, maybe also with placebo-controlled designs (reveal implantation vs. sham procedure), to examine potential predictors of non-arrhythmic syncopes and potential facilitators of risk stratification concerning the origin of syncope and the role of ILRs on the psychologic well-being. Equally important are studies examining the role of psychotherapeutic interventions, which may help patients with syncopes with elevated levels of psychopathology. Therefore, the identification of the cause of syncope remains an important challenge that is facilitated by an accurate multi-disciplinary clinical approach and by the correct use of new diagnostic tools, including ILR, as suggested by the recent guidelines. However, the possible underlying psychological mechanisms should also be evaluated during the diagnostic work-up of syncopes and addressed, if necessary, in an equally structured manner.
Author Contributions
Conceptualization K.W. and N.M.; methodology K.W., N.M., J.K. and L.E.; software K.W. and S.S.; validation K.W., D.W., B.R., F.R. and F.K.W.; formal analysis K.W., J.K. and N.M.; investigation K.W., S.S., J.W. and C.E.; resources K.W. and C.E.; data curation K.W., D.W., F.K.W. and J.W.; writing—original draft preparation K.W., J.K., L.E. and N.M.; writing—review and editing K.W., J.K. and N.M.; visualization K.W. and S.S.; supervision J.K., L.E. and N.M.; project administration K.W. and N.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the local Ethics Committee (protocol code 2021-087-f-S, approved 18 March 2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Additional and raw data can be obtained from the corresponding author under
kevin.willy@ukmuenster.de upon reasonable request.
Conflicts of Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
- Brignole, M.; Moya, A.; De Lange, F.J.; Deharo, J.-C.; Elliott, P.M.; Fanciulli, A.; Fedorowski, A.; Furlan, R.; Kenny, R.A.; Martínez, A.M.; et al. 2018 ESC Guidelines for the diagnosis and management of syncope. Eur. Heart J. 2018, 39, 1883–1948. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, T.; du Fay de Lavallaz, J.; Nestelberger, T.; Gualandro, D.M.; Strebel, I.; Badertscher, P.; Lopez-Ayala, P.; Widmer, V.; Freese, M.; Miró, O.; et al. Incidence, characteristics, determinants, and prognostic impact of recurrent syncope. Europace 2020, 22, 1885–1895. [Google Scholar] [CrossRef] [PubMed]
- Barbic, F.; Dipaola, F.; Casazza, G.; Borella, M.; Minonzio, M.; Solbiati, M.; Raj, S.R.; Sheldon, R.; Quinn, J.; Costantino, G.; et al. Syncope in a Working-Age Population: Recurrence Risk and Related Risk Factors. J. Clin. Med. 2019, 8, 150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Solbiati, M.; Casazza, G.; Dipaola, F.; Rusconi, A.M.; Cernuschi, G.; Barbic, F.; Montano, N.; Sheldon, R.S.; Furlan, R.; Costantino, G. Syncope recurrence and mortality: A systematic review. Europace 2015, 17, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Krahn, A.D.; Klein, G.J.; Yee, R.; Skanes, A.C. Randomized assessment of syncope trial: Conventional diagnostic testing versus a prolonged monitoring strategy. Circulation 2001, 104, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Podoleanu, C.; DaCosta, A.; Defaye, P.; Taieb, J.; Galley, D.; Bru, P.; Maury, P.; Mabo, P.; Boveda, S.; Cellarier, G.; et al. Early use of an implantable loop recorder in syncope evaluation: A randomized study in the context of the French healthcare system (FRESH study). Arch. Cardiovasc. Dis. 2014, 107, 546–552. [Google Scholar] [CrossRef] [Green Version]
- Sulke, N.; Sugihara, C.; Hong, P.; Patel, N.; Freemantle, N. The benefit of a remotely monitored implantable loop recorder as a first line investigation in unexplained syncope: The EaSyAS II trial. Europace 2016, 18, 912–918. [Google Scholar] [CrossRef]
- Farwell, D.J.; Freemantle, N.; Sulke, N. The clinical impact of implantable loop recorders in patients with syncope. Eur. Heart J. 2006, 27, 351–356. [Google Scholar] [CrossRef] [Green Version]
- Solbiati, M.; Casazza, G.; Dipaola, F.; Barbic, F.; Caldato, M.; Montano, N.; Furlan, R.; Sheldon, R.S.; Costantino, G. The diagnostic yield of implantable loop recorders in unexplained syncope: A systematic review and meta-analysis. Int. J. Cardiol. 2017, 231, 170–176. [Google Scholar] [CrossRef]
- Kahl, K.G.; Stapel, B.; Correll, C.U. Psychological and Psychopharmacological Interventions in Psychocardiology. Front. Psychiatry 2022, 13, 831359. [Google Scholar] [CrossRef] [PubMed]
- Linzer, M.; Pontinen, M.; Gold, D.T.; Divine, G.W.; Felder, A.; Brooks, W.B. Impairment of physical and psychosocial function in recurrent syncope. J. Clin. Epidemiol. 1991, 44, 1037–1043. [Google Scholar] [CrossRef]
- Kouakam, C.; Lacroix, D.; Klug, D.; Baux, P.; Marquié, C.; Kacet, S. Prevalence and prognostic significance of psychiatric disorders in patients evaluated for recurrent unexplained syncope. Am. J. Cardiol. 2002, 89, 530–535. [Google Scholar] [CrossRef]
- Ventura, R.; Maas, R.; Rüppel, R.; Stuhr, U.; Schuchert, A.; Meinertz, T.; Nienaber, C.A. Psychiatric conditions in patients with recurrent unexplained syncope. Europace 2001, 3, 311–316. [Google Scholar] [CrossRef]
- Magnavita, N.; Di Prinzio, R.R.; Arnesano, G.; Cerrina, A.; Gabriele, M.; Garbarino, S.; Gasbarri, M.; Iuliano, A.; Labella, M.; Matera, C.; et al. Association of Occupational Distress and Low Sleep Quality with Syncope, Presyncope, and Falls in Workers. Int. J. Environ. Res. Public Health 2021, 18, 12283. [Google Scholar] [CrossRef] [PubMed]
- Gilbody, S.; Richards, D.; Brealey, S.; Hewitt, C. Screening for Depression in Medical Settings with the Patient Health Questionnaire (PHQ): A Diagnostic Meta-Analysis. J. Gen. Intern. Med. 2007, 22, 1596–1602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Löwe, B.; Kroenke, K.; Herzog, W.; Gräfe, K. Measuring depression outcome with a brief self-report instrument: Sensitivity to change of the Patient Health Questionnaire (PHQ-9). J. Affect. Disord. 2004, 81, 61–66. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Lowe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Löwe, B.; Decker, O.; Müller, S.; Brähler, E.; Schellberg, D.; Herzog, W.; Herzberg, P.Y. Validation and Standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the General Population. Med. Care 2008, 46, 266–274. [Google Scholar] [CrossRef]
- Dugan, E.; Trachtenberg, F.; Hall, M.A. Development of abbreviated measures to assess patient trust in a physician, a health insurer, and the medical profession. BMC Health Serv. Res. 2005, 5, 64. [Google Scholar] [CrossRef] [Green Version]
- Schneider, S.M.; Schupp, J. Individual Differences in Social Comparison and its Consequences for Life Satisfaction: Introducing a Short Scale of the Iowa–Netherlands Comparison Orientation Measure. Soc. Indic. Res. 2014, 115, 767–789. [Google Scholar] [CrossRef]
- Rammstedt, B. The 10-Item Big Five Inventory—Norm values and investigation of sociodemographic effects based on a German population representative sample. Eur. J. Psychol. Assess. 2007, 23, 193–201. [Google Scholar] [CrossRef]
- Ware, J.E.; Kosinski, M.; Keller, S.D. A 12-item short-form health survey—Construction of scales and preliminary tests of reliability and validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferguson, E. Intellect and Somatic Health: Associations with Hypochondriacal Concerns, Perceived Threat and Fainting. Psychother. Psychosom. 2001, 70, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Walsh, K.E.; Baneck, T.; Page, R.L.; Brignole, M.; Hamdan, M.H. Psychogenic pseudosyncope: Not always a diagnosis of exclusion. Pacing Clin. Electrophysiol. 2018, 41, 480–486. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, K.; Ward, M.; Romero Ortuno, R.; Kenny, R.A. Syncope, Fear of Falling and Quality of Life Among Older Adults: Findings From the Irish Longitudinal Study on Aging (TILDA). Front. Cardiovasc. Med. 2020, 7, 7. [Google Scholar] [CrossRef] [PubMed]
- de Barros e Silva, R.L.A.; Volich, R.M.; de Barros e Silva, P.G.M.; da Costa Darrieux, F.C.; Scanavacca, M.I.; Hachul, D.T. Effect of psychotherapy on recurrence of events and quality of life in patients with vasovagal syncope. Sci Rep. 2022, 12, 5745. [Google Scholar] [CrossRef] [PubMed]
- Alciati, A.; Shiffer, D.; Dipaola, F.; Barbic, F.; Furlan, R. Psychogenic Pseudosyncope: Clinical Features, Diagnosis and Management. J. Atr. Fibrillat. 2020, 13, 2399. [Google Scholar]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 


{kind=link}