1. Introduction
Osteogenesis imperfecta (OI) is a rare genetic collagen disease characterized by bone fragility and ligamentous laxity [
1,
2]. Surgical fixation of brittle bones is difficult and is associated with a high rate of complications. The Fassier–Duval (FD) telescoping nail was developed to provide stability during long bone growth, and, currently, it is the most commonly used intramedullary device worldwide [
3,
4,
5]. However, the surgical revision rate is still high [
4,
6,
7]. The aim of this study was to review the results of OI patients treated with the FD nail at our institution and discuss a surgical strategy to decrease the FD nail revision rate.
2. Materials and Methods
We retrospectively reviewed all patients with a diagnosis of OI who were treated at our institution between 2015 and 2020. OI patients with at least one FD nail implant procedure performed in one lower extremity long bone were included. The exclusion criteria were those with a follow-up duration less than one year, incomplete radiograph images, and an FD nail implanted in an upper extremity long bone. The following data were collected: age at first surgery, sex, Sillence classification of OI, usage of bisphosphonate treatment, location of nail implant, nail diameter, revision timing, and failure mode.
The Sillence classification, defined as type I to type IV based on clinical finding, is currently most widely referenced [
8]. The phenotype of OI in our study was proven by molecular genetic examinations [
1,
9,
10] and confirmed by our pediatric geneticists.
With regards to the FD nail technique, the infrapatellar approach was used to apply tibial FD nails, while the antegrade approach was used for femur nails. For the tibial FD nails, a short threaded male component without cross-pin fixation was chosen for distal fixation, while a short or long threaded nail was chosen according to the thickness of the epiphysis in the distal femur. The FD nails were available in five diameters: 3.2, 4.0, 4.8, 5.6, and 6.4 mm [
11].
Serial X-ray images were examined for bone healing and implant failure. Nail failure was defined as: (1) migration of the male component (distally dislodged; the male nail tip had been pulled out of the epiphysis); (2) migration of the female component (proximal protrusion out of the anchorage; the female component had become dislodged); (3) refracture of the bone; (4) nail bending; and (5) delayed union. Delayed union was defined as failure to reach bony union by 6 months.
3. Results
The final cohort consisted of seven patients (three females and four males) with twenty lower limb long bones involved (ten femurs and ten tibiae). According to Sillence classification, six patients were classified as having type III OI, and one patient with type IV OI. The average age at first surgery was 5.4 years (range 1.5–11 years). The average nail diameter was 4.2 mm (range 3.2–6.4 mm). Among the 20 affected limbs, 11 required revision surgery, for a revision rate of 55%. The average interval between previous FD nail insertion and revision surgery was 2.4 years (range 0.8–3.25 years). Patient demographics and mode of nail failure are described in
Table 1. All patients received regular intravenous bisphosphonate treatment with pamidronate disodium at a dose of 30 mg/m
2, once every month. The treatment was stopped after surgery but resumed post-operatively after 3 months.
Among the causes of FD nail failure, migration of the male component (femur: 1, tibia: 4), migration of the female component (femur: 3), nail bending (femur: 3), refracture of the bone (femur: 2), and delayed union (tibia: 3) are described in
Table 2.
4. Discussion
Osteogenesis imperfecta (OI) is a rare genetic collagen disease characterized by bone fragility and ligamentous laxity [
1,
2]. Typical surgical interventions include realignment osteotomies and intramedullary fixation. However, internal fixation with nontelescoping intramedullary nails requires frequent revision due to patient growth [
3]. Telescoping intramedullary nails have superior probability of survival and decreased revision rate compared with static implants [
12,
13,
14]. Since 2001, the FD telescopic system has been used in the treatment of OI, congenital pseudarthrosis of the tibia, and, also, other various skeletal dysplasias [
3,
4,
5]. The FD telescopic nail has the advantage over regular nails [
15,
16] of being inserted through one incision without arthrotomy [
14,
17], however, complications can still occur, with a complication rate ranging from 0% to 53% [
4,
6,
7].
In a review of the literature, the main reasons for revision surgery were migration of the male/female component, refracture/nail bending, and delayed union [
7,
18,
19]. In our series, migration of the female component and nail bending were common reasons for failure in the femur, while migration of the male component and delayed union were common reasons for failure in the tibia, which is described in
Table 2.
Musielak, B.J. et al. [
7] reported that the risk factors for FD nail failure were a patient age younger than 5 years and an FD nail diameter smaller than 4 mm. However, few studies have described the possible reasons for nail failure in OI patients. According to Holmes et al. [
20], one of the most important reasons leading to implant migration is the position of the distal end of the nail in relation to the center of the epiphysis. They reported a 12% increase in failure rate per 10% increase in deviation from the center for both anteroposterior and lateral radiographs.
However, we still experienced failures where a nail in a fairly central position became dislodged or the bone refractured. Therefore, we suggest that not only the position of the nail but also the depth of the purchase and the overall mechanical axis alignment are important, along with a central nail position and bowing correction. According to our failure cases, the main principles for the FD nail should be purchase, nail position, and bowing.
4.1. Principle 1: Enough Depth of Nail Purchase in Distal and Proximal Epiphysis
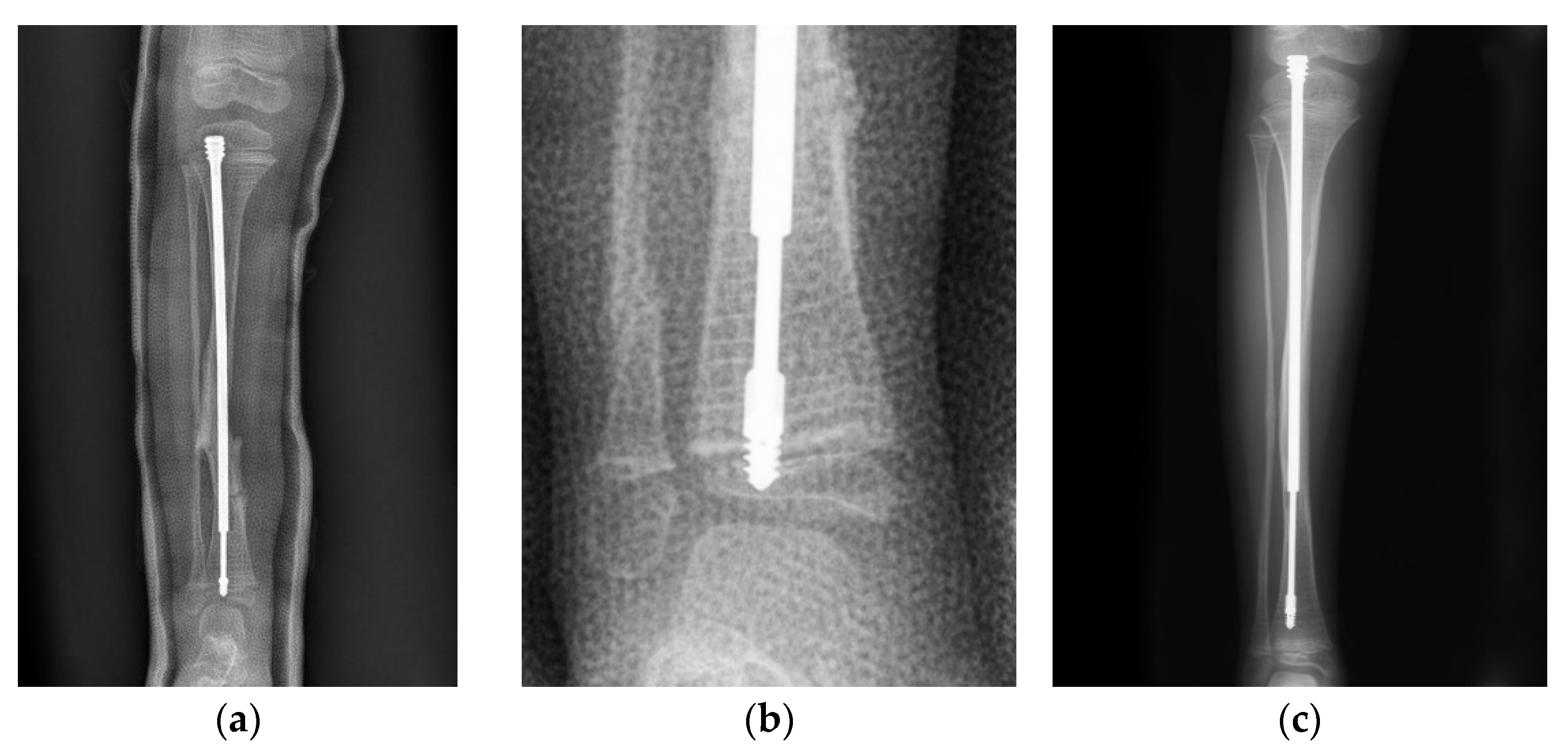
In a case of a 4-year-old female with type III OI (
Figure 1), the position of the male component was quite central in the distal epiphysis on both anteroposterior and lateral views. However, there was insufficient purchase of the male component tip (
Figure 1a). If the threads end just around the physis instead of beyond it (
Figure 1b), distal dislodgement would occur along with growth of the limb (
Figure 1c). However, this raises the question of how to ensure sufficient depth of the male implant intraoperatively. We suggest the following steps: First, center the male component at the center of the distal epiphysis as far as possible so that the thickest epiphysis is purchased. The thread of the male component needs to be fully submerged into the epiphysis, and the flange of the nail must exceed the physis, or at least stop at the level of the physis. If the distal epiphysis of the tibia is small, the tip of the nail may reach the subchondral area to ensure that the whole thread goes through the physis (
Figure 2). Since the distal epiphysis of the femur is larger than the distal epiphysis of the tibia, there is a relatively lower risk of distal dislodgement in the femur (tibia 4, femur 1 in our series) due to sufficient distal purchase.
Migration of the male component is common in the tibia due to an almost empty epiphysis [
18,
19]. For the male component, short thread screws are designed to anchor the epiphysis and resist a pulling out force due to growth [
15]. A keyhole over the screw thread adds strength to the distal fixation. The fixation-wire with a diameter ranging from 0.7 mm to 1.1 mm for the corresponding nail can increase more anchorage [
11], however, it was relatively difficult to facilitate targeting the keyhole with such a small fixation-wire. In addition, non-threaded (LON) male components with peg fixation and larger keyhole (1.5 mm) [
11] are not currently available in Taiwan. Thus, we could only follow the principles mentioned above to ensure maximal distal fixation.
Moreover, loss of fixation in the proximal femur is also related to insufficient purchase, which can be subdivided into two situations: (1) the nail entry point is not precisely over the tip of the greater trochanter and (2) insufficient depth of the thread of the female component. Proximal femoral fixation is challenging in younger children due to a partially ossified greater trochanter [
18].
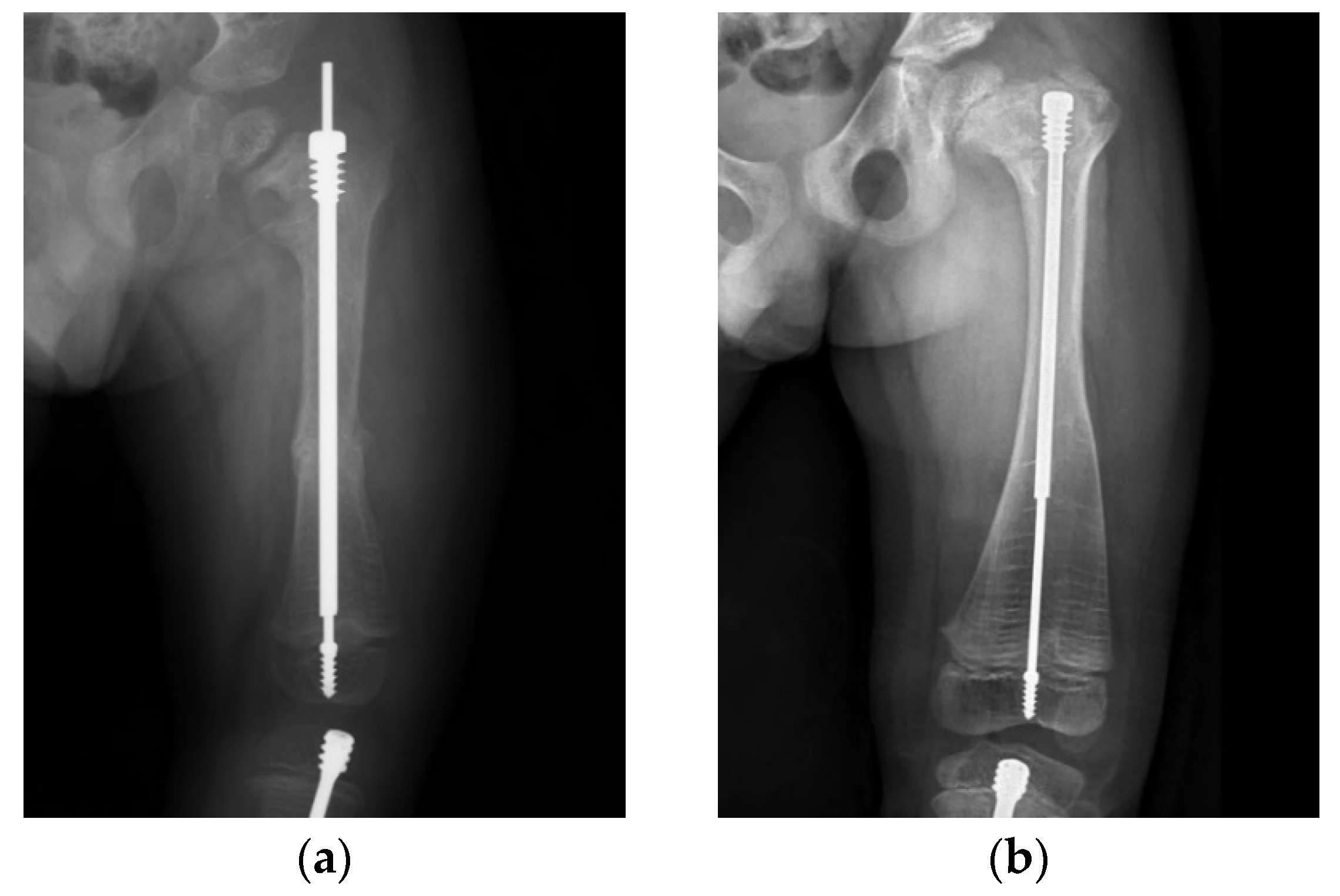
Another of our cases involved a boy who received double osteotomies and fixation with an FD nail in his right femur at the age of 1.5 years (
Figure 3). The proximal osteotomy segment was too small to align and the greater trochanter had not ossified, so it was difficult to find the most suitable entry point under the c-arm (
Figure 3a). During follow-up, we found that the female thread had become much more distal and anterior (
Figure 3b). In the following revision, due to concerns over damaging the apophysis of the femur and iatrogenic greater trochanter epiphysiodesis, with resulting sequela of valgus deformity, insufficient depth of the female component may have occurred, resulting in its proximal protrusion (
Figure 3c,d). The importance of the entry point and adequate purchase of the proximal femur cannot be over-emphasized (
Figure 3e).
4.2. Principle 2: The Nail Must Be Placed in the Center of the Epiphysis on Both Anteroposterior and Lateral Views
An 11-year-old boy with type IV OI (
Figure 4) underwent revision surgery with an FD nail due to implant malposition. When the distal tip of a nail is not placed in the center of the joint, the mechanical axis may become deviated, possibly leading to refracture or nail bending (
Figure 4a). In this patient, deviated alignment and a bowed femur caused an imbalance in mechanical stress, which led to a proximal femur refracture. Restoration of the alignment and bowing correction to avoid further implant failure were performed with a pediatric nail after physeal closure (
Figure 4b).
First, c-arm positioning intra-operatively cannot be over-emphasized to obtain the true AP and true lateral view of the affected limb. We prefer using the supine position or fracture table during both tibia and femur interventions, thus changing the projection radiation instead of changing the limb position. It is important to try to identify the entry point as precisely as possible. This is especially difficult for proximal femur entry because of the non-ossified small greater trochanter in young children under a non-open and percutaneous approach. The open approach is a possible solution; however, more tissue damage is a concern. Thus, we still use the percutaneous approach under fluoroscopy and accept the possible deviation rather than risk possible damage from the open approach. After a straight and rigid guide-wire or reamer has been inserted from the correct entry point, the wire will eventually meet the area of deformity, or CORA. We use a multiple percutaneous drilling technique for osteoclasis at the CORA and straighten the limb as the guidewire passes through, which realigns the deformed bone and minimizes surgical trauma.
4.3. Principle 3: Bowing of the Bone Is Related to Delayed Union and Refracture, and Correction Is Warranted
A 4-year-old male with type III OI presented as a classic model of insufficient depth of purchase and excessive bowing of the tibia (
Figure 5). When axial force is applied to the limbs with excessive bowing, there will be an uneven force on the concave and convex sides, leading to delayed union (
Figure 5a–c). Correction of the bowing with adequate osteotomy (or osteoclasis) before FD nail insertion is crucial (
Figure 5d,e).
These principles may help to guide treatment and avoid complications. Six years after surgery, a male patient with type III OI (
Figure 6) still maintained good nail telescoping without implant failure. We emphasize that sufficient depth of purchase is important to avoid migration of both the male and female components of the FD nail. A central nail position in the epiphysis ensures balanced alignment of the mechanical axis. Correcting excessive bowing cannot be over-emphasized. Following these principles, it is possible to avoid most implant-related complications during the long course of treatment for OI patients.
All patients received regular intravenous bisphosphonate treatment with pamidronate disodium at a dose of 30 mg/m
2, once every month. The treatment was stopped after surgery but was resumed post-operatively after 3 months. Pamidronate is a bisphosphonate, and it has been shown to increase bone mineral density (BMD) and decrease fracture rate, thereby substantially improving functional status [
21,
22]. During the first pamidronate infusion, a few patients had low-grade fever. These patients received acetaminophen prior to subsequent pamidronate infusions, and the fever did not recur. No other associated adverse effects were observed.
5. Limitation
Osteogenesis imperfecta is a rare disease, and one of the limitations of this study is the small number of cases treated at a single center with two pediatric orthopedic surgeons. A larger number of patients from multiple centers with a longer follow-up duration in future studies will be greatly beneficial to clarify the treatment of choice. This surgical strategy could be considered as a proposed study method in further collaborations with other medical institutes for a larger number of cases and, possibly, as a prospective series. Optimal and evidence-based treatments are still being studied. In addition, wire fixation of the male component in the distal tibia could not be performed, as this implant type is not currently available in Taiwan, which may have led to a higher dislodgment rate in the distal tibia. Further studies are warranted to investigate the effect of implant selection on the revision rate.
6. Conclusions
Surgery for OI patients is challenging. Orthopedic surgeons should aim to minimize complication and revision rates with the FD nail. In the femur, migration of the female component and nail bending were common reasons for failure in our series, while migration of the male component and delayed union were common in the tibia. According to our experience of using the FD telescoping nail, the key factors are sufficient depth of purchase, center–center nail position, and adequate osteotomy to correct bowing.
Author Contributions
Conceptualization, Y.-C.H., C.-Y.Y. and S.-C.L.; methodology, Y.-C.H. and C.-Y.Y.; software, Y.-C.H. and K.-Y.C.; validation, Y.-C.H., H.-Y.L., S.-P.L., K.-Y.C., C.-Y.Y. and S.-C.L.; formal analysis, Y.-C.H. and C.-Y.Y.; investigation, Y.-C.H. and C.-Y.Y.; resources, H.-Y.L., S.-P.L., K.-Y.C., C.-Y.Y. and S.-C.L.; data curation, Y.-C.H. and K.-Y.C.; writing—original draft preparation, Y.-C.H.; writing—review and editing, C.-Y.Y. and S.-C.L.; visualization, H.-Y.L., S.-P.L., K.-Y.C., C.-Y.Y. and S.-C.L.; supervision, H.-Y.L., S.-P.L., K.-Y.C., C.-Y.Y. and S.-C.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of MacKay Memorial Hospital (protocol code 22MMHIS176e and date of approval 11 May 2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
All of the data are registered at MacKay Memorial Hospital, Taipei, Taiwan.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Marini, J.C.; Blissett, A.R. New genes in bone development: What’s new in osteogenesis imperfecta. J. Clin. Endocrinol. Metab. 2013, 98, 3095–3103. [Google Scholar] [CrossRef] [PubMed]
- Forlino, A.; Marini, J.C. Osteogenesis imperfecta. Lancet 2016, 387, 1657–1671. [Google Scholar] [CrossRef]
- Esposito, P.; Plotkin, H. Surgical treatment of osteogenesis imperfecta: Current concepts. Curr. Opin. Pediatr. 2008, 20, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Ruck, J.; Dahan-Oliel, N.; Montpetit, K.; Rauch, F.; Fassier, F. Fassier-Duval femoral rodding in children with osteogenesis imperfecta receiving bisphosphonates: Functional outcomes at one year. J. Child. Orthop. 2011, 5, 217–224. [Google Scholar] [CrossRef] [PubMed]
- Fassier, F.; Duval, P. New concept for telescoping rodding in osteogenesis imperfecta: Preliminary results. In Proceedings of the Annual Meeting of the Pediatric Orthopaedic Society of North America (POSNA), Cancun, Mexico, 1–5 May 2001; p. 101. [Google Scholar]
- Sterian, A.G.; Ulici, A. Revision Rates for Osteogenesis Imperfecta Patients Treated with Telescopic Nails. A follow-up Study After a 7-year Experience. J. Med. Life 2020, 13, 543–547. [Google Scholar] [CrossRef] [PubMed]
- Musielak, B.J.; Wozniak, L.; Sulko, J.; Oberc, A.; Jozwiak, M. Problems, Complications, and Factors Predisposing to Failure of Fassier-Duval Rodding in Children With Osteogenesis Imperfecta: A Double-center Study. J. Pediatr. Orthop. 2021, 41, e347–e352. [Google Scholar] [CrossRef] [PubMed]
- Sillence, D.O.; Senn, A.; Danks, D.M. Genetic heterogeneity in osteogenesis imperfecta. J. Med. Genet. 1979, 16, 101–116. [Google Scholar] [CrossRef] [PubMed]
- Byers, P.H.; Krakow, D.; Nunes, M.E.; Pepin, M. Genetic evaluation of suspected osteogenesis imperfecta (OI). Genet. Med. 2006, 8, 383–388. [Google Scholar] [CrossRef] [PubMed]
- Palomo, T.; Vilaça, T.; Lazaretti-Castro, M. Osteogenesis imperfecta: Diagnosis and treatment. Curr. Opin. Endocrinol. Diabetes Obes. 2017, 24, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Fassier, F.; Duval, P. Fassier-Duval Telescopic IM System Surgical Technique; Pega Medical: Laval, QC, Canada, 2009; pp. 1–19. [Google Scholar]
- Nicholas, R.W.; James, P. Telescoping intramedullary stabilization of the lower extremities for severe osteogenesis imperfecta. J. Pediatr. Orthop. 1990, 10, 219–223. [Google Scholar] [CrossRef] [PubMed]
- El-Adl, G.; Khalil, M.A.; Enan, A.; Mostafa, M.F.; El-Lakkany, M.R. Telescoping versus non-telescoping rods in the treatment of osteogenesis imperfecta. Acta Orthop. Belg. 2009, 75, 200–208. [Google Scholar] [PubMed]
- Spahn, K.M.; Mickel, T.; Carry, P.M.; Brazell, C.J.; Whalen, K.; Georgopoulos, G.; Miller, N.H. Fassier-Duval Rods are Associated With Superior Probability of Survival Compared With Static Implants in a Cohort of Children With Osteogenesis Imperfecta Deformities. J. Pediatr. Orthop. 2019, 39, e392–e396. [Google Scholar] [CrossRef] [PubMed]
- Fassier, A. Telescopic rodding in children: Technical progression from Dubow-Bailey to Fassier-Duval™. Orthop. Traumatol. Surg. Res. 2021, 107, 102759. [Google Scholar] [CrossRef] [PubMed]
- Yong, B.; De Wouters, S.; Howard, A. Complications of Elongating Intramedullary Rods in the Treatment of Lower Extremity Fractures for Osteogenesis Imperfecta: A Meta-Analysis of 594 Patients in 40 Years. J. Pediatr. Orthop. 2022, 42, e301–e308. [Google Scholar] [CrossRef] [PubMed]
- Sułko, J.; Oberc, A. Advantages and Complications Following Fassier-Duval Intramedullary Rodding in Children. Pilot Study. Ortop. Traumatol. Rehabil. 2015, 17, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Cox, I.; Al Mouazzen, L.; Bleibleh, S.; Moldovan, R.; Bintcliffe, F.; Bache, C.E.; Thomas, S. Combined two-centre experience of single-entry telescopic rods identifies characteristic modes of failure. Bone Jt. J. 2020, 102, 1048–1055. [Google Scholar] [CrossRef] [PubMed]
- Fassier, F.R. Osteogenesis Imperfecta-Who Needs Rodding Surgery? Curr. Osteoporos. Rep. 2021, 19, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Holmes, K.; Gralla, J.; Brazell, C.; Carry, P.; Tong, S.; Miller, N.H.; Georgopoulos, G. Fassier-Duval Rod Failure: Is It Related to Positioning in the Distal Epiphysis? J. Pediatr. Orthop. 2020, 40, 448–452. [Google Scholar] [CrossRef] [PubMed]
- Bajpai, A.; Kabra, M.; Gupta, N.; Sharda, S.; Ghosh, M. Intravenous pamidronate therapy in osteogenesis imperfecta: Response to treatment and factors influencing outcome. J. Pediatr. Orthop. 2007, 27, 225–227. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.Y.; Lin, S.P.; Chuang, C.K.; Chen, M.R.; Chang, C.Y. Intravenous pamidronate therapy in Taiwanese patients with osteogenesis imperfecta. Pediatr. Neonatol. 2008, 49, 161–165. [Google Scholar] [CrossRef][Green Version]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}