
Clinical Predictors for Procedural Stroke and Implications for Embolic Protection Devices during TAVR: Results from the Multicenter Transcatheter Aortic Valve Replacement In-Hospital Stroke (TASK) Study

 , , ,
, , ,  , ,
, ,
Abstract
:1. Introduction
2. Methods
3. Statistical Analysis
4. Results
4.1. Peri-Procedural Cerebrovascular Events
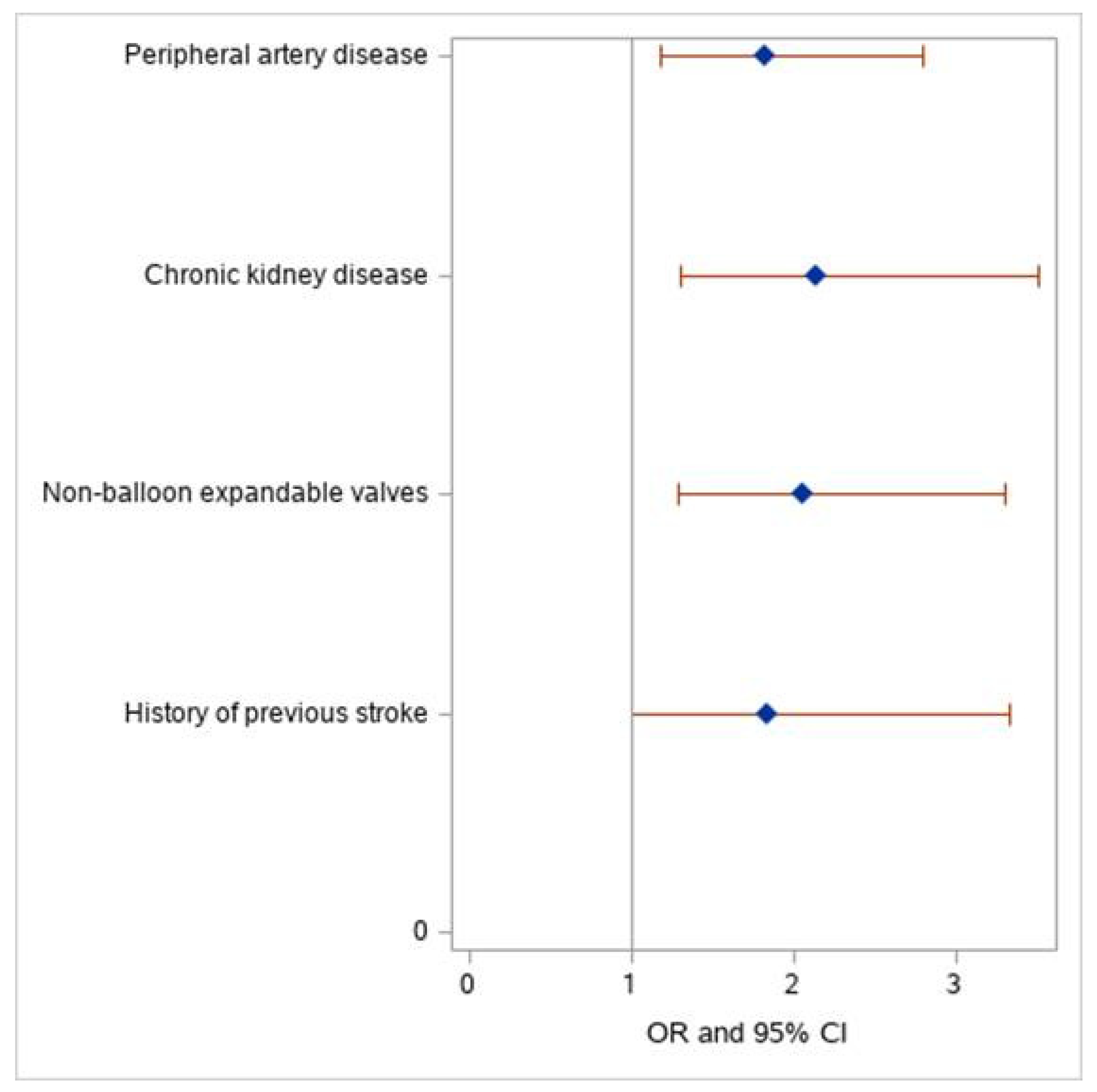
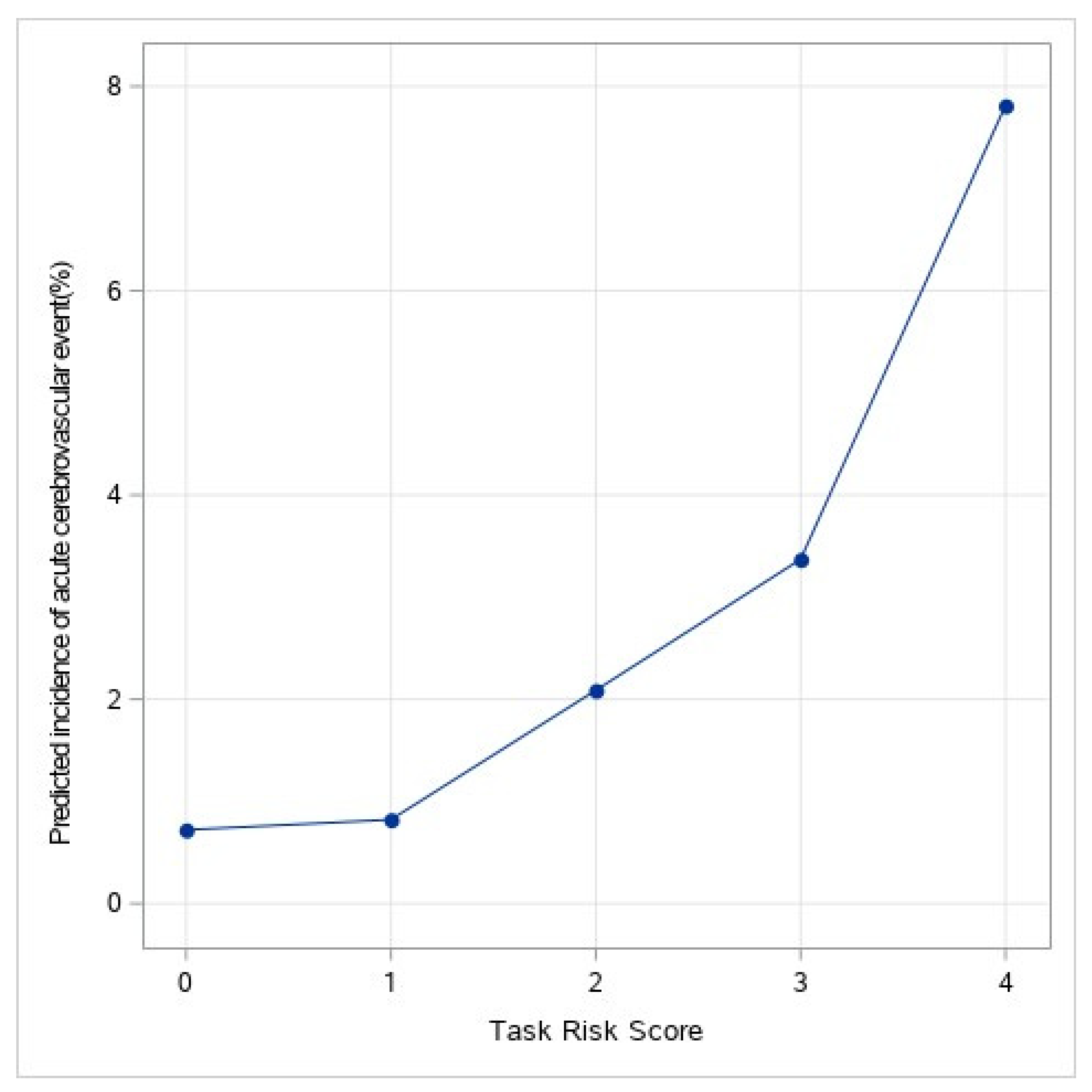
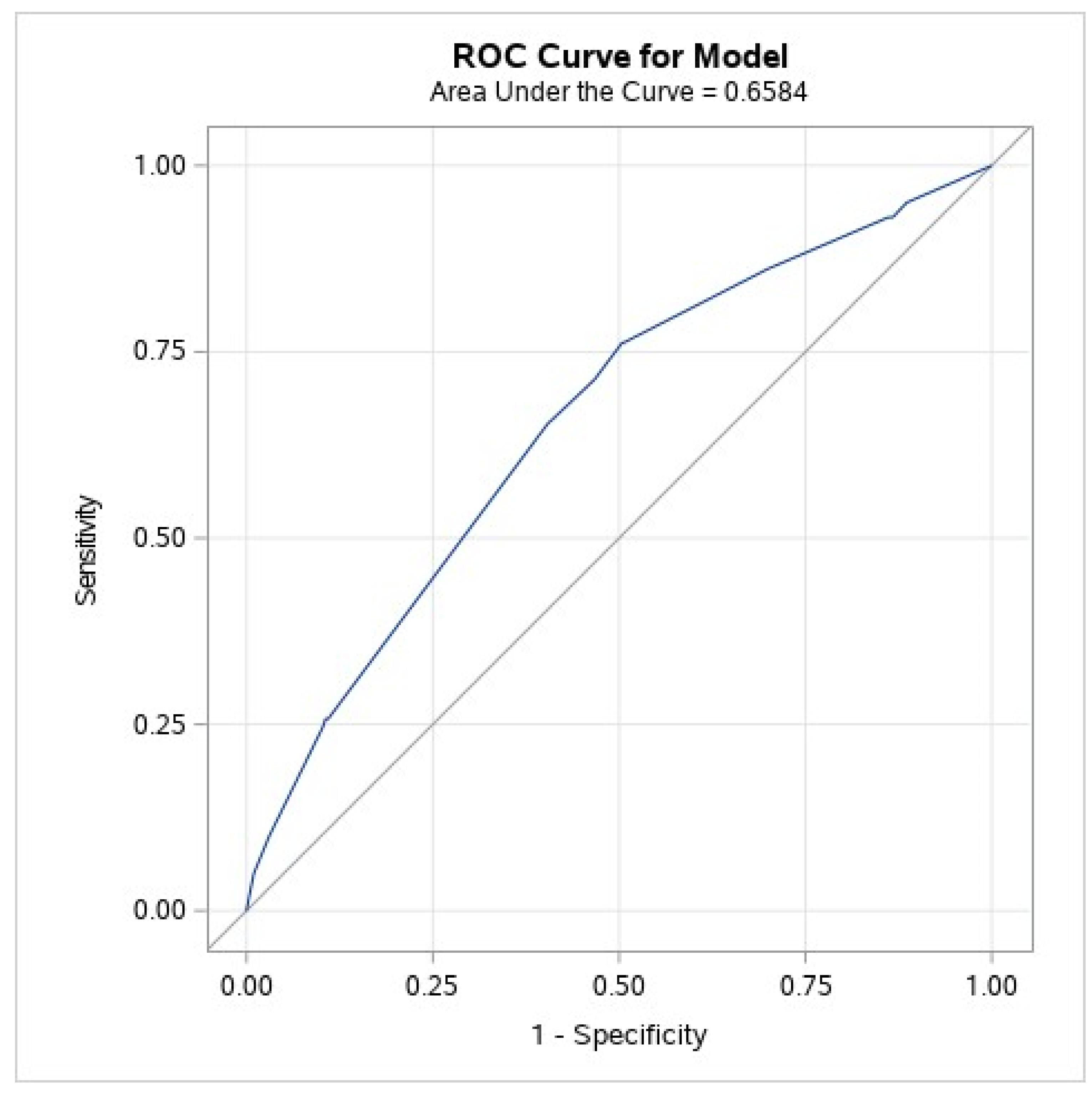
4.2. TASK Score Derivation and Validation
4.3. Prognostic Value of Peri-Procedural Cerebrovascular Events
5. Discussion
6. Limitations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| TAVR | transcatheter aortic valve replacement |
| TASK | Transcatheter Aortic valve replacement in-hoSpital stroKe study |
| OR | odds ratio |
| CI | confidence interval |
Appendix A
Appendix A.1. Statistical Analysis
Appendix A.2. TASK Score Derivation
References
- Popma, J.J.; Deeb, G.M.; Yakubov, S.J.; Mumtaz, M.; Gada, H.; O’Hair, D.; Bajwa, T.; Heiser, J.C.; Merhi, W.; Kleiman, N.S.; et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1706–1715. [Google Scholar] [CrossRef]
- Mack, M.J.; Leon, M.B.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Russo, M.; Kapadia, S.R.; Malaisrie, S.C.; Cohen, D.J.; Pibarot, P.; et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N. Engl. J. Med. 2019, 380, 1695–1705. [Google Scholar] [CrossRef] [PubMed]
- Eggebrecht, H.; Schmermund, A.; Voigtländer, T.; Kahlert, P.; Erbel, R.; Mehta, R.H. Risk of stroke after transcatheter aortic valve implantation (TAVI): A meta-analysis of 10,037 published patients. EuroIntervention 2012, 8, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Kapadia, S.R.; Kodali, S.; Makkar, R.; Mehran, R.; Lazar, R.M.; Zivadinov, R.; Dwyer, M.G.; Jilaihawi, H.; Virmani, R.; Anwaruddin, S.; et al. Protection Against Cerebral Embolism During Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2017, 69, 367–377. [Google Scholar] [CrossRef] [PubMed]
- Stortecky, S.; Windecker, S.; Pilgrim, T.; Heg, D.; Buellesfeld, L.; Khattab, A.A.; Huber, C.; Gloekler, S.; Nietlispach, F.; Mattle, H.; et al. Cerebrovascular accidents complicating transcatheter aortic valve implantation: Frequency, timing and impact on outcomes. EuroIntervention 2012, 88, 62–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tay, E.L.W.; Gurvitch, R.; Wijesinghe, N.; Nietlispach, F.; Nielispach, F.; Wood, D.; Cheung, A.; Ye, J.; Lichtenstein, S.V.; Carere, R.; et al. A high-risk period for cerebrovascular events exists after transcatheter aortic valve implantation. JACC. Cardiovasc. Interv. 2011, 4, 1290–1297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosmans, J.; Bleiziffer, S.; Gerckens, U.; Wenaweser, P.; Brecker, S.; Tamburino, C.; Linke, A. The Incidence and Predictors of Early- and Mid-Term Clinically Relevant Neurological Events After Transcatheter Aortic Valve Replacement in Real-World Patients. J. Am. Coll. Cardiol. 2015, 66, 209–217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kappetein, A.P.; Head, S.J.; Généreux, P.; Piazza, N.; van Mieghem, N.M.; Blackstone, E.H.; Brott, T.G.; Cohen, D.J.; Cutlip, D.E.; van Es, G.-A.; et al. Updated standardized endpoint definitions for transcatheter aortic valve implantation: The Valve Academic Research Consortium-2 consensus document†. Eur. Heart J. 2012, 33, 2403–2418. [Google Scholar] [CrossRef]
- Muralidharan, A.; Thiagarajan, K.; Van Ham, R.; Gleason, T.G.; Mulukutla, S.; Schindler, J.T.; Jeevanantham, V.; Thirumala, P.D. Meta-Analysis of Perioperative Stroke and Mortality in Transcatheter Aortic Valve Implantation. Am. J. Cardiol. 2016, 118, 1031–1045. [Google Scholar] [CrossRef]
- Nazif, T.M.; Moses, J.; Sharma, R.; Dhoble, A.; Rovin, J.; Brown, D.; Horwitz, P.; Makkar, R.; Stoler, R.; Forrest, J.; et al. Randomized Evaluation of TriGuard 3 Cerebral Embolic Protection After Transcatheter Aortic Valve Replacement: REFLECT II. JACC Cardiovasc. Interv. 2021, 14, 515–527. [Google Scholar] [CrossRef]
- Van Mieghem, N.M.; Van Gils, L.; Ahmad, H.; Van Kesteren, F.; Van Der Werf, H.W.; Brueren, G.; Storm, M.; Lenzen, M.; Daemen, J.; Van Den Heuvel, A.F.M.; et al. Filter-based cerebral embolic protection with transcatheter aortic valve implantation: The randomised MISTRAL-C trial. EuroIntervention 2016, 12, 499–507. [Google Scholar] [CrossRef] [PubMed]
- Haussig, S.; Mangner, N.; Dwyer, M.G.; Lehmkuhl, L.; Lücke, C.; Woitek, F.; Holzhey, D.M.; Mohr, F.W.; Gutberlet, M.; Zivadinov, R.; et al. Effect of a Cerebral Protection Device on Brain Lesions Following Transcatheter Aortic Valve Implantation in Patients With Severe Aortic Stenosis. JAMA 2016, 316, 592. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, Y.; Howard, J.P. Meta-Analysis of Usefulness of Cerebral Embolic Protection During Transcatheter Aortic Valve Implantation. Am. J. Cardiol. 2021, 146, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Lansky, A.J.; Schofer, J.; Tchetche, D.; Stella, P.; Pietras, C.G.; Parise, H.; Abrams, K.; Forrest, J.K.; Cleman, M.; Reinöhl, J.; et al. A prospective randomized evaluation of the TriGuardTM HDH embolic deflection device during transcatheter aortic valve implantation: Results from the DEFLECT III trial. Eur. Heart J. 2015, 36, 2070–2078. [Google Scholar] [CrossRef] [PubMed]
- Sobieski, M.A., II; Pappas, P.S.; Tatooles, A.J.; Slaughter, M.S. Embol-X Intra-Aortic Filtration System: Capturing Particulate Emboli in the Cardiac Surgery Patient. J. Extra. Corpor. Technol. 2005, 37, 222. [Google Scholar]
- Gasior, T.; Mangner, N.; Bijoch, J.; Wojakowski, W. Cerebral embolic protection systems for transcatheter aortic valve replacement. J. Interv. Cardiol. 2018, 31, 891–898. [Google Scholar] [CrossRef] [Green Version]
- Kahlert, P.; Knipp, S.C.; Schlamann, M.; Thielmann, M.; Al-Rashid, F.; Weber, M.; Johansson, U.; Wendt, D.; Jakob, H.G.; Forsting, M.; et al. Silent and Apparent Cerebral Ischemia After Percutaneous Transfemoral Aortic Valve Implantation. Circulation 2010, 121, 870–878. [Google Scholar] [CrossRef] [Green Version]
- Nombela-Franco, L.; Webb, J.G.; de Jaegere, P.P.; Toggweiler, S.; Nuis, R.-J.; Dager, A.E.; Amat-Santos, I.J.; Cheung, A.; Ye, J.; Binder, R.K.; et al. Timing, Predictive Factors, and Prognostic Value of Cerebrovascular Events in a Large Cohort of Patients Undergoing Transcatheter Aortic Valve Implantation. Circulation 2012, 126, 3041–3053. [Google Scholar] [CrossRef]
- Butala, N.M.; Makkar, R.; Secemsky, E.A.; Gallup, D.; Marquis-Gravel, G.; Kosinski, A.S.; Vemulapalli, S.; Valle, J.A.; Bradley, S.M.; Chakravarty, T.; et al. Cerebral Embolic Protection and Outcomes of Transcatheter Aortic Valve Replacement: Results from the TVT Registry. Circulation 2021, 143, 2229–2240. [Google Scholar] [CrossRef]
- Giustino, G.; Sorrentino, S.; Mehran, R.; Faggioni, M.; Dangas, G. Cerebral Embolic Protection During TAVR: A Clinical Event Meta-Analysis. J. Am. Coll. Cardiol. 2017, 69, 465–466. [Google Scholar] [CrossRef]
- Armijo, G.; Nombela-Franco, L.; Tirado-Conte, G. Cerebrovascular Events After Transcatheter Aortic Valve Implantation. Front. Cardiovasc. Med. 2018, 5, 104. [Google Scholar] [CrossRef]
- Fink, N.; Segev, A.; Kornowski, R.; Finkelstein, A.; Assali, A.; Rozenbaum, Z.; Vaknin-Assa, H.; Halkin, A.; Fefer, P.; Ben-Shoshan, J.; et al. Balloon dilatation and outcome among patients undergoing trans-femoral aortic valve replacement. Int. J. Cardiol. 2017, 230, 537–541. [Google Scholar] [CrossRef] [PubMed]
- Heinze, G.; Wallisch, C.; Dunkler, D. Variable selection—A review and recommendations for the practicing statistician. Biom. J. 2018, 60, 431–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, R.A. Introducing the GLMSELECT Procedure for Model Selection. In Proceedings of the Thirty-First Annual SAS Users Group International Conference, San Francisco, CA, USA, 26–29 March 2006. [Google Scholar]
- Smith, G.C.S.; Seaman, S.R.; Wood, A.M.; Royston, P.; White, I.R. Correcting for Optimistic Prediction in Small Data Sets. Am. J. Epidemiol. 2014, 180, 318–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Entire Cohort | Peri-Procedural Cerebrovascular Event | Odds Ratio | Confidence Interval | p-Value | |
|---|---|---|---|---|---|---|
| N = 8779 | Yes N = 127 | No N = 8652 | ||||
| Baseline characteristics | ||||||
| Age (mean ± SD) | 82 ± 6.6 | 82.1 ± 6.8 | 83.1 ± 6.5 | 1.02 | 0.99–1.05 | 0.12 |
| Female gender (%) | 4546 (52) | 72 (57) | 4474 (52) | 1.22 | 0.86–1.74 | 0.27 |
| Low body weight * (%) | 3414 (40) | 65 (52) | 3349 (40) | 1.60 | 1.12–2.28 | 0.009 |
| Ischemic heart disease (%) | 2697 (31) | 39 (31) | 2658 (31) | 0.95 | 0.67–1.44 | 0.95 |
| Chronic kidney disease ** (%) | 5458 (68) | 101 (82) | 5357 (68) | 2.16 | 1.36–3.43 | <0.001 |
| Stroke history (%) | 620 (7) | 14 (11) | 606 (7) | 1.60 | 0.91–2.8 | 0.10 |
| Diabetes mellitus (%) | 2586 (30) | 35 (28) | 2551 (30) | 0.9 | 0.61–1.33 | 0.60 |
| Hypertension (%) | 6088 (80) | 79 (81) | 6009 (80) | 1.06 | 0.64–1.78 | 0.81 |
| Atrial fibrillation (%) | 2607 (32) | 35 (29) | 2572 (32) | 0.85 | 0.57–1.26 | 0.43 |
| Chronic obstructive pulmonary disease (%) | 1296 (17) | 17 (16) | 1279 (17) | 0.97 | 0.58–1.65 | 0.92 |
| Peripheral vascular disease (%) | 1462 (19) | 35 (29) | 1427 (19) | 1.76 | 1.19–2.62 | 0.005 |
| Baseline medications | ||||||
| Aspirin (%) | 5646 (64) | 66 (68) | 4478 (62) | 1.29 | 0.84–1.98 | 0.24 |
| P2Y12 inhibitor (%) | 1966 (30) | 33 (35) | 1933 (30) | 1.26 | 0.82–1.93 | 0.28 |
| Oral anti-coagulant (%) | 1689 (26) | 19 (20) | 1670 (26) | 0.72 | 0.44–1.20 | 0.21 |
| Baseline Echocardiography | ||||||
| AVA (cm2) (mean ± SD) | 0.73 ± 0.2 | 0.74 ± 0.2 | 0.72 ± 0.2 | 0.83 | 0.34–2.03 | 0.68 |
| Ejection fraction (mean ± SD) | 54 ± 12 | 54 ± 12 | 54 ± 12 | 1.00 | 0.99–1.01 | 0.75 |
| Mean gradient (mmHg) (mean ± SD) | 45 ± 16 | 45 ± 14 | 45 ± 16 | 0.99 | 0.99–1.01 | 0.84 |
| Procedural data | ||||||
| Conscious sedation (%) | 2675 (31) | 37 (29) | 2638 (31) | 0.92 | 0.63–1.35 | 0.67 |
| Self-expandable valve | 4516 (52) | 71 (56) | 4445 (52) | 1.35 | 0.91–2.00 | 0.136 |
| Balloon expandable valve | 2878 (37) | 26 (24) | 2852 (37) | 0.53 | 0.34–0.83 | 0.005 |
| Mechanical expandable valve | 451 (6) | 13 (12) | 438 (6) | 2.23 | 1.24–4.01 | 0.001 |
| Balloon pre-dilatation | 4358 (50) | 68 (53) | 4290 (50) | 1.14 | 0.80–1.62 | 0.46 |
| Balloon post-dilatation | 1414 (19) | 22 (19) | 1392 (19) | 0.94 | 0.62–1.57 | 0.98 |
| In-hospital events | ||||||
| Myocardial infarction (%) | 41 (0.5) | 3 (2.6) | 38 (0.5) | 5.4 | 1.65–17.8 | 0.005 |
| Any cerebrovascular event (%) | 203 (2.3) | 127 (100) | 77 (0.9) | - | - | <0.001 |
| 24 hr cardiovascular event (%) | 127 (1.4) | 127 (100) | 0 (0) | - | - | <0.001 |
| New atrial fibrillation (%) | 600 (8) | 9 (8) | 591 (8) | 1.03 | 0.52–2.05 | 0.934 |
| Life-threatening/major bleeding (%) | 606 (7) | 12 (10) | 594 (7) | 1.42 | 0.78–2.59 | 0.251 |
| In-hospital mortality (%) | 867 (1.2) | 10 (7.9) | 97 (1.1) | 7.54 | 3.83–14.82 | <0.001 |
| Observed Stroke Incidence (%) | Odds Ratio | Confidence Interval | p-Value | |
|---|---|---|---|---|
| Very-low risk = 0 points (n = 692) | 0.7 | 1.00 | - | - |
| Low risk = 1 point (n = 2310) | 0.8 | 1.14 | 0.42–3.06 | 0.79 |
| Intermediate risk = 2 points (n = 2442) | 2.1 | 2.93 | 1.16–7.37 | 0.022 |
| High risk = 3–4 points (n = 687) | 3.8 | 5.40 | 2.06–14.16 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berkovitch, A.; Segev, A.; Maor, E.; Sedaghat, A.; Finkelstein, A.; Saccocci, M.; Kornowski, R.; Latib, A.; De La Torre Hernandez, J.M.; Søndergaard, L.; et al. Clinical Predictors for Procedural Stroke and Implications for Embolic Protection Devices during TAVR: Results from the Multicenter Transcatheter Aortic Valve Replacement In-Hospital Stroke (TASK) Study. J. Pers. Med. 2022, 12, 1056. https://doi.org/10.3390/jpm12071056
Berkovitch A, Segev A, Maor E, Sedaghat A, Finkelstein A, Saccocci M, Kornowski R, Latib A, De La Torre Hernandez JM, Søndergaard L, et al. Clinical Predictors for Procedural Stroke and Implications for Embolic Protection Devices during TAVR: Results from the Multicenter Transcatheter Aortic Valve Replacement In-Hospital Stroke (TASK) Study. Journal of Personalized Medicine. 2022; 12(7):1056. https://doi.org/10.3390/jpm12071056
Chicago/Turabian StyleBerkovitch, Anat, Amit Segev, Elad Maor, Alexander Sedaghat, Ariel Finkelstein, Matteo Saccocci, Ran Kornowski, Azeem Latib, Jose M. De La Torre Hernandez, Lars Søndergaard, and et al. 2022. "Clinical Predictors for Procedural Stroke and Implications for Embolic Protection Devices during TAVR: Results from the Multicenter Transcatheter Aortic Valve Replacement In-Hospital Stroke (TASK) Study" Journal of Personalized Medicine 12, no. 7: 1056. https://doi.org/10.3390/jpm12071056
APA StyleBerkovitch, A., Segev, A., Maor, E., Sedaghat, A., Finkelstein, A., Saccocci, M., Kornowski, R., Latib, A., De La Torre Hernandez, J. M., Søndergaard, L., Mylotte, D., Van Royen, N., Zaman, A. G., Robert, P., Sinning, J.-M., Steinvil, A., Maisano, F., Orvin, K., Iannopollo, G., ... Barbash, I. M. (2022). Clinical Predictors for Procedural Stroke and Implications for Embolic Protection Devices during TAVR: Results from the Multicenter Transcatheter Aortic Valve Replacement In-Hospital Stroke (TASK) Study. Journal of Personalized Medicine, 12(7), 1056. https://doi.org/10.3390/jpm12071056