
Anxiety Is a Mediator between Heart Rate Variability and Quality of Life in Chronic Obstructive Pulmonary Disease

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measurements
2.3. The Experimental Procedure
2.4. Data Processing and Statistical Analysis
3. Results
3.1. Participants’ Characteristics
3.2. Differences in Depression, Anxiety, Quality of Life, Spirometry, and HRV Indices between the HC and COPD Groups
3.3. Correlations between HRV Indices, Depression, Anxiety, Quality of Life, and Spirometry in Participants with COPD
3.4. HRV Indices, Depression, Anxiety, and Spirometry in Predicting SGRQ
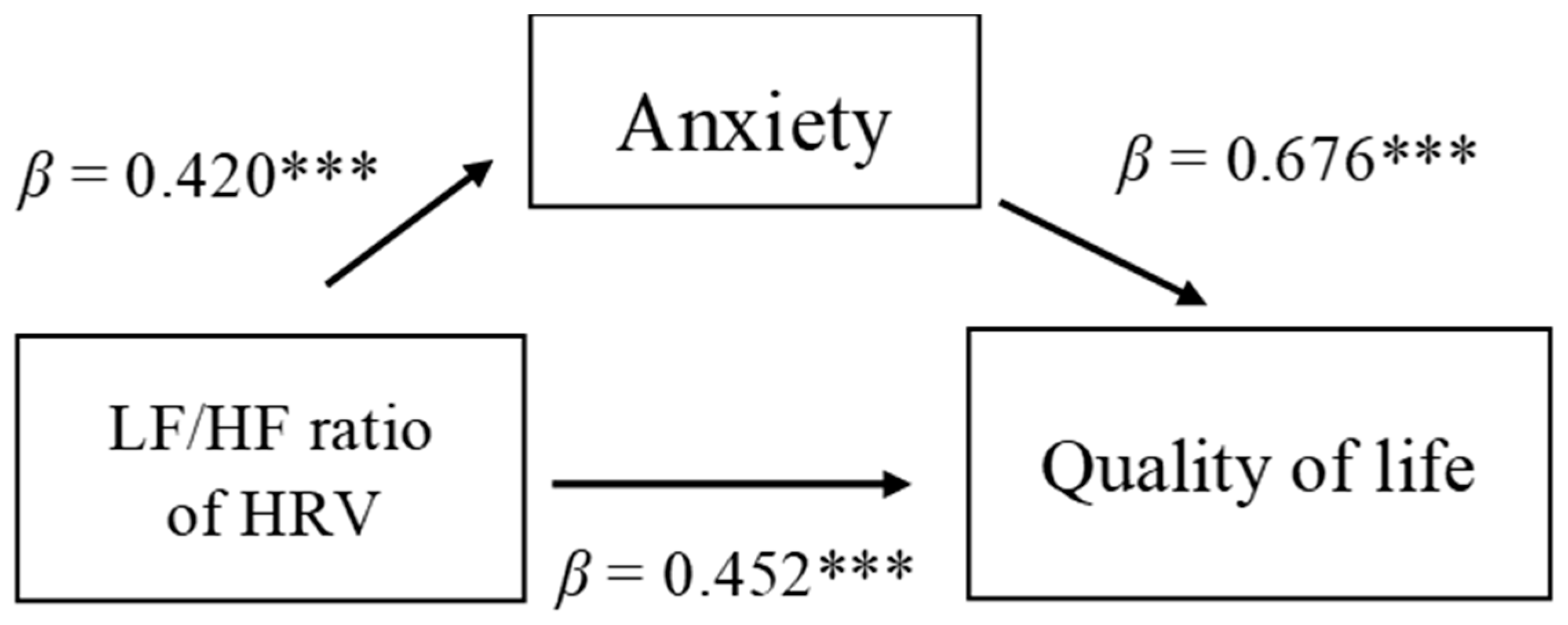
3.5. Anxiety Was a Mediator between Sympathetic Activation and Quality of Life
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Global Initiative for Chronic Obstructive Lung Disease. 2022 Report: Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. Available online: https://goldcopd.org/2022-gold-reports-2/ (accessed on 25 February 2022).
- Salvi, S.S.; Barnes, P.J. Chronic obstructive pulmonary disease in non-smokers. Lancet 2009, 374, 733–743. [Google Scholar] [CrossRef]
- Varmaghani, M.; Dehghani, M.; Heidari, E.; Sharifi, F.; Moghaddam, S.S.; Farzadfar, F. Global prevalence of chronic obstructive pulmonary disease: Systematic review and meta-analysis. East. Mediterr. Health J. 2019, 25, 47–57. [Google Scholar] [CrossRef]
- Cheng, S.L.; Chan, M.C.; Wang, C.C.; Lin, C.H.; Wang, H.C.; Hsu, J.Y.; Hang, L.W.; Chang, C.J.; Perng, D.W.; Yu, C.J. COPD in Taiwan: A national epidemiology survey. Int. J. Chron. Obstruct. Pulmon. Dis. 2015, 10, 2459. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Barnes, P.J. Immunology of asthma and chronic obstructive pulmonary disease. Nat. Rev. Immunol. 2008, 8, 183–192. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.F.; Adcock, I.M. Multifaceted mechanisms in COPD: Inflammation, immunity, and tissue repair and destruction. Eur. Respir. J. 2008, 31, 1334–1356. [Google Scholar] [CrossRef] [PubMed]
- Leap, J.; Arshad, O.; Cheema, T.; Balaan, M. Pathophysiology of COPD. Crit. Care. Nurs. Q. 2021, 44, 2–8. [Google Scholar] [CrossRef] [PubMed]
- Mohammed, J.; Meeus, M.; Derom, E.; Da Silva, H.; Calders, P. Evidence for autonomic function and its influencing factors in subjects with COPD: A systematic review. Respir. Care 2015, 60, 1841–1851. [Google Scholar] [CrossRef]
- van Gestel, A.J.; Steier, J. Autonomic dysfunction in patients with chronic obstructive pulmonary disease (COPD). J. Thorac. Dis. 2010, 2, 215. [Google Scholar] [CrossRef]
- Carvalho, T.D.; Pastre, C.M.; de Godoy, M.F.; Fereira, C.; Pitta, F.O.; de Abreu, L.C.; Ramos, E.M.C.; Valenti, V.E.; Vanderlei, L.C.M. Fractal correlation property of heart rate variability in chronic obstructive pulmonary disease. Int. J. Chron. Obstruct. Pulmon. Dis. 2011, 6, 23. [Google Scholar] [CrossRef][Green Version]
- Gunduz, H.; Talay, F.; Arinc, H.; Ozyildirim, S.; Akdemir, R.; Yolcu, M.; Kanat, M.; Uyan, C. Heart rate variability and heart rate turbulence in patients with chronic obstructive pulmonary disease. Cardiol. J. 2009, 16, 553–559. [Google Scholar]
- Mohammed, J.; Derom, E.; de Backer, T.; de Wandele, I.; Calders, P. Cardiac autonomic function and reactivity tests in physically active subjects with moderately severe COPD. COPD 2018, 15, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Rossi, R.C.; Vanderlei, F.M.; Bernardo, A.F.; Souza, N.M.D.; Goncalves, A.C.C.R.; Ramos, E.M.C.; Pastre, C.M.; de Abreu, L.C.; Vanderlei, L.C.M. Effect of pursed-lip breathing in patients with COPD: Linear and nonlinear analysis of cardiac autonomic modulation. COPD 2014, 11, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Vanzella, L.M.; Bernardo, A.F.B.; Carvalho, T.D.D.; Vanderlei, F.M.; Silva, A.K.F.D.; Vanderlei, L.C.M. Complexity of autonomic nervous system function in individuals with COPD. J. Bras. Pneumol. 2018, 44, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Zupanic, E.; Zivanovic, I.; Kalisnik, J.M.; Avbelj, V.; Lainscak, M. The effect of 4-week rehabilitation on heart rate variability and QTc interval in patients with chronic obstructive pulmonary disease. COPD 2014, 11, 659–669. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.L.; Chen, G.Y.; Kuo, C.D. Hypoxemia and autonomic nervous dysfunction in patients with chronic obstructive pulmonary disease. Respir. Med. 2006, 100, 1547–1553. [Google Scholar] [CrossRef]
- Stein, P.K.; Nelson, P.; Rottman, J.N.; Howard, D.; Ward, S.M.; Kleiger, R.E.; Senior, R.M. Heart rate variability reflects severity of COPD in PiZ α1-antitrypsin deficiency. Chest 1998, 113, 327–333. [Google Scholar] [CrossRef]
- Zareifopoulos, N.; Bellou, A.; Spiropoulou, A.; Spiropoulos, K. Prevalence, contribution to disease burden and management of comorbid depression and anxiety in chronic obstructive pulmonary disease: A narrative review. COPD 2019, 16, 406–417. [Google Scholar] [CrossRef]
- Atlantis, E.; Fahey, P.; Cochrane, B.; Smith, S. Bidirectional associations between clinically relevant depression or anxiety and COPD: A systematic review and meta-analysis. Chest 2013, 144, 766–777. [Google Scholar] [CrossRef]
- Tantucci, C.; Bottone, D.; Levi, G.; Uccelli, S.; Venturoli, N.; Magri, R.; Garrafa, E.; Pini, L. Respiratory function, autonomic dysfunction, and systemic inflammation are closely linked in patients with COPD and tidal flow limitation: An exploratory study. Respir. Physiol. Neurobiol. 2021, 284, 103565. [Google Scholar] [CrossRef]
- van Gestel, A.J.; Kohler, M.; Steier, J.; Teschler, S.; Russi, E.W.; Teschler, H. Cardiac autonomic dysfunction and health-related quality of life in patients with chronic obstructive pulmonary disease. Respirology 2011, 16, 939–946. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Beck depression inventory–II. San Antonio 1996, 78, 490–498. [Google Scholar] [CrossRef]
- Beck, A.T.; Epstein, N.; Brown, G.; Steer, R.A. An inventory for measuring clinical anxiety: Psychometric properties. J. Consult. Clin. Psychol. 1988, 56, 893–897. [Google Scholar] [CrossRef] [PubMed]
- Jones, P.W.; Quirk, F.H.; Baveystock, C.M.; Littlejohns, P. A self-complete measure of health status for chronic airflow limitation. Am. Rev. Respir. Dis. 1992, 145, 1321–1327. [Google Scholar] [CrossRef]
- Chen, H.Y. Beck Depression Inventory Version II (Chinese Version); Chinese Behavioral Science Corporation: Taipei, Taiwan, 2000. [Google Scholar]
- Lu, M.L.; Che, H.H.; Chang, S.W.; Shen, W.W. Reliability and validity of the Chinese version of the beck depression inventory–II. Taiwan J. Psychiatry 2002, 16, 301–309. [Google Scholar]
- Lin, Y.J. Beck Anxiety Inventory (Chinese Version); Chinese Behavioral Science Corporation: Taipei, Taiwan, 2000. [Google Scholar]
- Che, H.H.; Lu, M.M.; Chen, H.C.; Chang, S.W.; Lee, Y.G. Validation of the Chinese version of the beck anxiety inventory. Formos. J. Med. 2006, 10, 447–454. [Google Scholar] [CrossRef]
- David, T.W.; Scudds, R.J.; Scudds, R.A. Reliability and validity of a Hong Kong Chinese version of the St George’s Respiratory Questionnaire in patients with COPD. Hong Kong Physiother. J. 2004, 22, 33–39. [Google Scholar] [CrossRef]
- Chen, H.W. Validity and Reliability of the Chinese Version of the St. George’s Respiratory Questionnaire for COPD Patients. Master’s Thesis, National Defense Medical Center, Taipei, Taiwan, 2010. Available online: https://hdl.handle.net/11296/cw4v4m (accessed on 14 March 2022).
- Thapa, N.; Maharjan, M.; Shrestha, T.M.; Gauchan, S.; Pun, P.; Thapa, Y.B. Anxiety and depression among patients with chronic obstructive pulmonary disease and general population in rural Nepal. BMC Psychiatry 2017, 17, 397. [Google Scholar] [CrossRef] [PubMed]
- Fu, P.K. The Prevalence of Depressive Disorder and Its Effect on Acute Exacerbation and Mortality in Patients with Chronic Obstructive Pulmonary Disease (COPD). Master’s Thesis, National Taiwan University, Taipei, Taiwan, 2015. [Google Scholar] [CrossRef]
- Hsieh, M.H.; Lee, C.T.C.; Tsai, P.J.; Tsai, C.J.; Liao, Y.T.; Chen, V.C.H.; Stewart, R. Chronic obstructive pulmonary disease and anxiety disorders: A nationwide population-based study in Taiwan. Gen. Hosp. Psychiatry 2016, 42, 1–6. [Google Scholar] [CrossRef]
- Matte, D.L.; Pizzichini, M.M.; Hoepers, A.T.; Diaz, A.P.; Karloh, M.; Dias, M.; Pizzichini, E. Prevalence of depression in COPD: A systematic review and meta-analysis of controlled studies. Respir. Med. 2016, 117, 154–161. [Google Scholar] [CrossRef]
- Willgoss, T.G.; Yohannes, A.M. Anxiety disorders in patients with COPD: A systematic review. Respir. Care 2013, 58, 858–866. [Google Scholar] [CrossRef]
- Snène, H.; Rafrafi, R.; Salah, N.; Blibech, H.; Mehiri, N.; Louzir, B. Anxiety and depression in Tunisian patients with COPD. Tunis. Med. 2021, 99, 623–631. [Google Scholar] [PubMed]
- Pooler, A.; Beech, R. Examining the relationship between anxiety and depression and exacerbations of COPD which result in hospital admission: A systematic review. Int. J. Chron. Obstruct. Pulmon. Dis. 2014, 9, 315. [Google Scholar] [CrossRef] [PubMed]
- Vikjord, S.A.A.; Brumpton, B.M.; Mai, X.M.; Vanfleteren, L.; Langhammer, A. The association of anxiety and depression with mortality in a COPD cohort. The HUNT study, Norway. Respir. Med. 2020, 171, 106089. [Google Scholar] [CrossRef] [PubMed]
- Dua, R.; Das, A.; Kumar, A.; Kumar, S.; Mishra, M.; Sharma, K. Association of comorbid anxiety and depression with chronic obstructive pulmonary disease. Lung India 2018, 35, 31. [Google Scholar] [CrossRef] [PubMed]
- Hynninen, M.J.; Pallesen, S.; Nordhus, I.H. Factors affecting health status in COPD patients with co-morbid anxiety or depression. Int. J. Chron. Obstruct. Pulmon. Dis. 2007, 2, 323. [Google Scholar]
- Hernández-Pérez, A.; Vargas-Núñez, I.; Moreno-Jiménez, B.; Pérez-Padilla, R.; Ramírez-Venegas, A. Affective comorbidity associated with symptoms, lung function, and differences between patients with COPD for biomass and tobacco smoke Exposure. J. Clin. Psychol. Med. Settings 2021, 29, 310–317. [Google Scholar] [CrossRef]
- Park, S.C.; Saiphoklang, N.; Jung, D.; Gomez, D.; Phillips, J.E.; Dolezal, B.A.; Tashkin, D.P.; Barjaktarevic, U.; Cooper, C.B. Use of a wearable biosensor to study heart rate variability in chronic obstructive pulmonary disease and its relationship to disease severity. Sensors 2022, 22, 2264. [Google Scholar] [CrossRef]
- Baron, R.M.; Kenny, D.A. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- Yohannes, A.M.; Junkes-Cunha, M.; Smith, J.; Vestbo, J. Management of dyspnea and anxiety in chronic obstructive pulmonary disease: A critical review. J. Am. Med. Dir. Assoc. 2017, 18, 1096.e1–1096.e17. [Google Scholar] [CrossRef]
- Li, Z.; Liu, S.; Wang, L.; Smith, L. Mind–body exercise for anxiety and depression in copd patients: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2020, 17, 22. [Google Scholar] [CrossRef]


{kind=link}
| COPD Group (n = 96) | HC Group (n = 34) | t/x2 | p | |
|---|---|---|---|---|
| Age, mean (years) | 66.25 ± 8.69 | 61.38 ± 7.56 | −2.90 ** | 0.004 |
| Sex, male/female (%) | 86/10 (90%/10%) | 18/16 (53%/47%) | 21.07 *** | <0.001 |
| ANCOVA a | COPD group (n = 96) | HC group (n = 34) | F | p |
| Total BDI-II score | 5.35 ± 7.98 | 2.03 ± 2.43 | 4.10 ** | 0.008 |
| Total BAI score | 4.12 ± 7.52 | 1.33 ± 1.59 | 1.62 | 0.188 |
| Total SGRQ score | 20.29 ± 17.93 | 3.52 ± 5.36 | 8.40 *** | <0.001 |
| Spirometry_FEV1(L) | 1.64 ± 0.61 | 2.36 ± 0.51 | 32.15 *** | <0.001 |
| FVC(L) | 2.63 ± 0.77 | 2.85 ± 0.57 | 19.57 *** | <0.001 |
| FEV1/Predicted (%) | 59.02 ± 19.11 | 90.58 ± 17.31 | 61.52 *** | <0.001 |
| FEV1/FVC (%) | 61.77 ± 11.69 | 82.79 ± 9.32 | 59.69 *** | <0.001 |
| Breathing rate (breaths/min) | 17.63 ± 4.31 | 16.47 ± 3.65 | 1.51 | 0.222 |
| Heart rate (beats/min) | 76.05 ± 12.78 | 71.86 ± 8.77 | 1.28 | 0.284 |
| SpO2 (%) | 95.95 ± 1.70 | 96.65 ± 1.43 | 0.795 | 0.374 |
| SBP (mmHg) | 129.77 ± 13.42 | 125.76 ± 14.63 | 0.43 | 0.515 |
| DBP (mmHg) | 77.45 ± 10.84 | 76.74 ± 10.79 | 0.89 | 0.348 |
| HRV_SDNN (ms) | 21.17 ± 9.17 | 26.19 ± 9.51 | 5.49 * | 0.021 |
| LF (ms2/Hz) | 28.19 ± 38.70 | 47.76 ± 52.95 | 3.03 * | 0.032 |
| HF (ms2/Hz) | 41.86 ± 53.83 | 62.59 ± 64.21 | 2.86 | 0.093 |
| LF/HF ratio | 1.32 ± 1.44 | 1.26 ± 1.25 | 0.006 | 0.939 |
| COPD (n = 96) | HC (n =34) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| SDNN | LF | HF | LF/HF Ratio | SGRQ | SDNN | LF | HF | LF/HF Ratio | SGRQ | |
| Total BDI-II score | −0.017 | −0.038 | −0.125 | 0.312 ** | 0.370 ** | 0.136 | 0.246 | 0.186 | 0.119 | 0.299 |
| Total BAI score | −0.182 | −0.033 | −0.138 | 0.420 *** | 0.676 *** | 0.044 | 0.013 | 0.042 | 0.038 | 0.349 |
| Total SGRQ score | −0.085 | −0.075 | −0.121 | 0.467 *** | 1.00 | −0.142 | −0.104 | −0.225 | −0.235 | 1 |
| Spirometry_FEV1 | −0.061 | 0.094 | −0.088 | 0.162 | −0.171 | 0.101 | −0.031 | 0.097 | 0.104 | −0.065 |
| FVC | −0.005 | 0.099 | −0.048 | 0.134 | −0.142 | −0.026 | −0.148 | −0.054 | −0.073 | −0.083 |
| FEV1/Predicted | −0.030 | 0.079 | −0.018 | 0.052 | −0.205 | 0.350 * | 0.113 | 0.327 | 0.419 * | −0.203 |
| FEV1/FVC | −0.145 | 0.023 | −0.097 | 0.099 | −0.168 | 0.255 | 0.263 | 0.291 | 0.322 | 0.010 |
| Model 1 | Model 2 | |||||
|---|---|---|---|---|---|---|
| β | t | p | β | t | p | |
| Model 1 | ||||||
| Age | −0.097 | −0.810 | 0.421 | 0.019 | 0.213 | 0.832 |
| Sex | 0.058 | 0.484 | 0.630 | 0.007 | 0.080 | 0.937 |
| Model 2 | ||||||
| BDI-II | 0.024 | 0.244 | 0.808 | |||
| BAI | 0.585 *** | 5.925 | <0.001 | |||
| LF/HF ratio | 0.231 * | 2.445 | 0.017 | |||
| FEV1/predicted | −0.251 ** | −2.977 | 0.004 | |||
| R2 | 0.012 | 0.566 *** | ||||
| F | 0.425 | 14.117 | ||||
| P | 0.656 | <0.001 | ||||
| ΔR2 | 0.554 *** | |||||
| ΔF | 20.271 | |||||
| ΔP | <0.001 | |||||
| BAI | SGRQ | |||
|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | |
| LF/HF ratio | 0.420 *** | 0.452 *** | 0.228 ** | |
| BAI | 0.676 *** | 0.533 *** | ||
| R2 | 0.176 | 0.219 | 0.457 | 0.498 |
| ΔR2 | 0.279 | |||
| F | 19.695 *** | 19.752 *** | 58.954 *** | 34.234 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, D.-W.; Chang, L.-H.; Yang, P.-C.; Kuo, T.-Y.; Tsai, D.-L.; Chen, H.-C.; Yuan, H.-L.; Chen, P.-S.; Chen, S.-C.; Lin, I.-M. Anxiety Is a Mediator between Heart Rate Variability and Quality of Life in Chronic Obstructive Pulmonary Disease. J. Pers. Med. 2022, 12, 960. https://doi.org/10.3390/jpm12060960
Wu D-W, Chang L-H, Yang P-C, Kuo T-Y, Tsai D-L, Chen H-C, Yuan H-L, Chen P-S, Chen S-C, Lin I-M. Anxiety Is a Mediator between Heart Rate Variability and Quality of Life in Chronic Obstructive Pulmonary Disease. Journal of Personalized Medicine. 2022; 12(6):960. https://doi.org/10.3390/jpm12060960
Chicago/Turabian StyleWu, Da-Wei, Li-Hsin Chang, Po-Chou Yang, Tzu-Yu Kuo, Dong-Lin Tsai, Huang-Chi Chen, Hui-Lan Yuan, Pei-Shih Chen, Szu-Chia Chen, and I-Mei Lin. 2022. "Anxiety Is a Mediator between Heart Rate Variability and Quality of Life in Chronic Obstructive Pulmonary Disease" Journal of Personalized Medicine 12, no. 6: 960. https://doi.org/10.3390/jpm12060960
APA StyleWu, D.-W., Chang, L.-H., Yang, P.-C., Kuo, T.-Y., Tsai, D.-L., Chen, H.-C., Yuan, H.-L., Chen, P.-S., Chen, S.-C., & Lin, I.-M. (2022). Anxiety Is a Mediator between Heart Rate Variability and Quality of Life in Chronic Obstructive Pulmonary Disease. Journal of Personalized Medicine, 12(6), 960. https://doi.org/10.3390/jpm12060960