
Psilocybin—Mediated Attenuation of Gamma Band Auditory Steady-State Responses (ASSR) Is Driven by the Intensity of Cognitive and Emotional Domains of Psychedelic Experience

 ,
,  , , ,
, , , {kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Approval
2.3. Experimental Design
2.4. Psilocybin Dosage
2.5. Psychological and Physiological Measures
2.6. Auditory Stimulation
2.7. EEG Recording
2.8. Data Analysis
2.8.1. EEG Data Pre-Processing
2.8.2. Statistical Evaluation
3. Results
3.1. Psilocin Pharmacokinetics
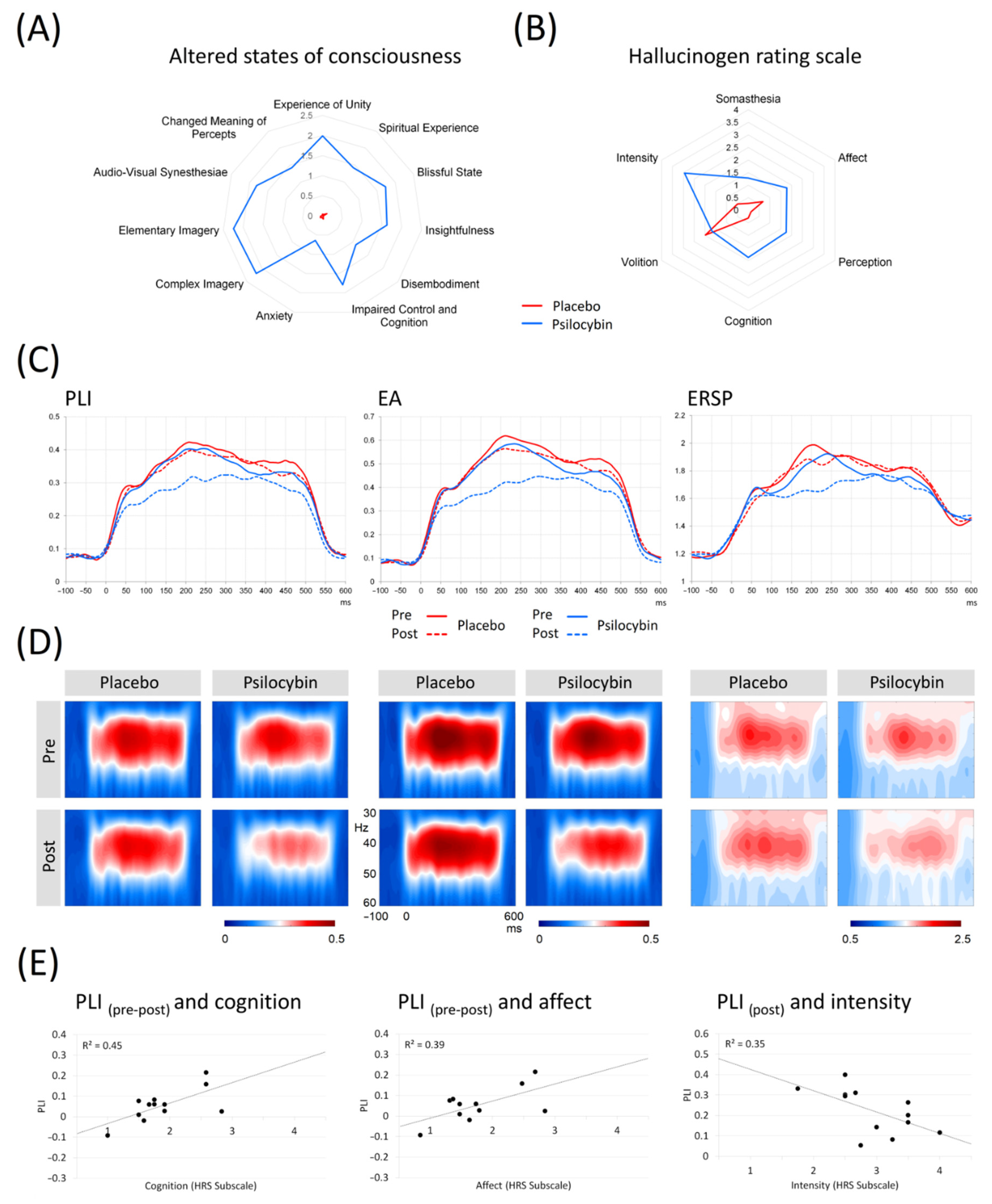
3.2. Effects of Psilocybin on Subjective Experience and Psychopathology
3.3. Vital Signs
3.4. 40 Hz Auditory Steady-State Response
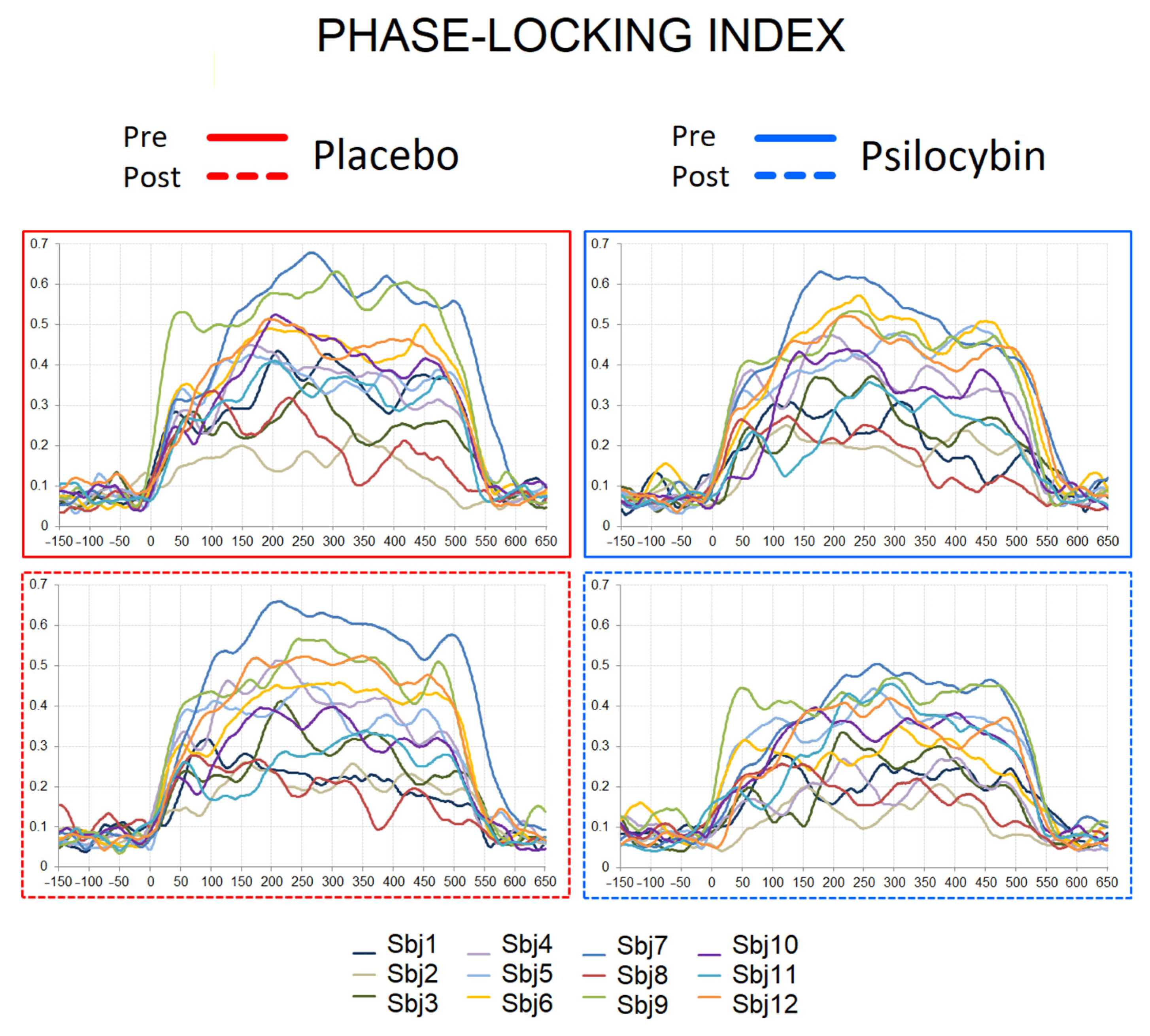
3.4.1. Phase-Locking Index (PLI)
3.4.2. Evoked Amplitude (EA)
3.4.3. Event-Related Spectral Perturbation (ERSP)
3.5. ASSR Correlations with Psychometric Measures and Psilocin Plasma Levels
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nutt, D. Psychedelic drugs—A new era in psychiatry? Dialog-Clin. Neurosci. 2019, 21, 139–147. [Google Scholar] [CrossRef]
- Li, N.-X.; Hu, Y.-R.; Chen, W.-N.; Zhang, B. Dose effect of psilocybin on primary and secondary depression: A preliminary systematic review and meta-analysis. J. Affect. Disord. 2021, 296, 26–34. [Google Scholar] [CrossRef] [PubMed]
- Więckiewicz, G.; Stokłosa, I.; Piegza, M.; Gorczyca, P.; Pudlo, R. Lysergic Acid Diethylamide, Psilocybin and Dimethyltryptamine in Depression Treatment: A Systematic Review. Pharmaceuticals 2021, 14, 793. [Google Scholar] [CrossRef] [PubMed]
- Studerus, E.; Gamma, A.; Kometer, M.; Vollenweider, F.X. Prediction of Psilocybin Response in Healthy Volunteers. PLoS ONE 2012, 7, e30800. [Google Scholar] [CrossRef]
- Meinhardt, M.W.; Pfarr, S.; Fouquet, G.; Rohleder, C.; Meinhardt, M.L.; Barroso-Flores, J.; Hoffmann, R.; Jeanblanc, J.; Paul, E.; Wagner, K.; et al. Psilocybin targets a common molecular mechanism for cognitive impairment and increased craving in alcoholism. Sci. Adv. 2021, 7, eabh2399. [Google Scholar] [CrossRef]
- Vollenweider, F.X.; Preller, K.H. Psychedelic drugs: Neurobiology and potential for treatment of psychiatric disorders. Nat. Rev. Neurosci. 2020, 21, 611–624. [Google Scholar] [CrossRef]
- Doss, M.K.; Považan, M.; Rosenberg, M.D.; Sepeda, N.D.; Davis, A.K.; Finan, P.H.; Smith, G.S.; Pekar, J.J.; Barker, P.B.; Griffiths, R.R.; et al. Psilocybin therapy increases cognitive and neural flexibility in patients with major depressive disorder. Transl. Psychiatry 2021, 11, 1–10. [Google Scholar] [CrossRef]
- Barrett, F.S.; Carbonaro, T.M.; Hurwitz, E.; Johnson, M.W.; Griffiths, R.R. Double-blind comparison of the two hallucinogens psilocybin and dextromethorphan: Effects on cognition. Psychopharmacologia. 2018, 235, 2915–2927. [Google Scholar] [CrossRef]
- Bravermanová, A.; Viktorinová, M.; Tylš, F.; Novák, T.; Androvičová, R.; Korčák, J.; Horáček, J.; Balíková, M.; Griškova-Bulanova, I.; Danielová, D.; et al. Psilocybin disrupts sensory and higher order cognitive processing but not pre-attentive cognitive processing—study on P300 and mismatch negativity in healthy volunteers. Psychopharmacology 2018, 235, 491–503. [Google Scholar] [CrossRef]
- Kometer, M.; Cahn, B.R.; Andel, D.; Carter, O.L.; Vollenweider, F.X. The 5-HT2A/1A Agonist Psilocybin Disrupts Modal Object Completion Associated with Visual Hallucinations. Biol. Psychiatry 2011, 69, 399–406. [Google Scholar] [CrossRef] [Green Version]
- Kometer, M.; Schmidt, A.; Jäncke, L.; Vollenweider, F.X. Activation of Serotonin 2A Receptors Underlies the Psilocybin-Induced Effects on α Oscillations, N170 Visual-Evoked Potentials, and Visual Hallucinations. J. Neurosci. 2013, 33, 10544–10551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Umbricht, D.S.; Vollenweider, F.X.; Schmid, L.; Grübel, C.; Skrabo, A.; Huber, T.; Koller, R. Effects of the 5-HT2A Agonist Psilocybin on Mismatch Negativity Generation and AX-Continuous Performance Task: Implications for the Neuropharmacology of Cognitive Deficits in Schizophrenia. Neuropsychopharmacology 2003, 28, 170–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kometer, M.; Schmidt, A.; Bachmann, R.; Studerus, E.; Seifritz, E.; Vollenweider, F.X. Psilocybin biases facial recognition, goal-directed behavior, and mood state toward positive relative to negative emotions through different serotonergic subreceptors. Biol Psychiatry 2012, 72, 898–906. [Google Scholar] [CrossRef] [PubMed]
- Vejmola, Č.; Tylš, F.; Piorecká, V.; Koudelka, V.; Kadeřábek, L.; Novák, T.; Páleníček, T. Psilocin, LSD, mescaline, and DOB all induce broadband desynchronization of EEG and disconnection in rats with robust translational validity. Transl. Psychiatry 2021, 11, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Başar, E. A review of gamma oscillations in healthy subjects and in cognitive impairment. Int. J. Psychophysiol. 2013, 90, 99–117. [Google Scholar] [CrossRef]
- Isomura, S.; Onitsuka, T.; Tsuchimoto, R.; Nakamura, I.; Hirano, S.; Oda, Y.; Oribe, N.; Hirano, Y.; Ueno, T.; Kanba, S. Differentiation between major depressive disorder and bipolar disorder by auditory steady-state responses. J. Affect. Disord. 2016, 190, 800–806. [Google Scholar] [CrossRef]
- Light, G.A.; Hsu, J.L.; Hsieh, M.H.; Meyer-Gomes, K.; Sprock, J.; Swerdlow, N.R.; Braff, D.L. Gamma Band Oscillations Reveal Neural Network Cortical Coherence Dysfunction in Schizophrenia Patients. Biol. Psychiatry 2006, 60, 1231–1240. [Google Scholar] [CrossRef]
- Parker, D.A.; Hamm, J.P.; McDowell, J.E.; Keedy, S.K.; Gershon, E.S.; Ivleva, E.I.; Pearlson, G.D.; Keshavan, M.S.; Tamminga, C.A.; Sweeney, J.A.; et al. Auditory steady-state EEG response across the schizo-bipolar spectrum. Schizophr. Res. 2019, 209, 218–226. [Google Scholar] [CrossRef]
- Spencer, K.M.; Salisbury, D.F.; Shenton, M.E.; McCarley, R.W. γ-Band Auditory Steady-State Responses Are Impaired in First Episode Psychosis. Biol. Psychiatry 2008, 64, 369–375. [Google Scholar] [CrossRef] [Green Version]
- Thuné, H.; Recasens, M.; Uhlhaas, P.J. The 40-Hz Auditory Steady-State Response in Patients With Schizophrenia. JAMA Psychiatry 2016, 73, 1145. [Google Scholar] [CrossRef]
- Ahmed, S.; Lepock, J.R.; Mizrahi, R.; Bagby, R.M.; Gerritsen, C.J.; Korostil, M.; Light, G.A.; Kiang, M. Decreased Gamma Auditory Steady-State Response Is Associated With Impaired Real-World Functioning in Unmedicated Patients at Clinical High Risk for Psychosis. Clin. EEG Neurosci. 2020, 52, 400–405. [Google Scholar] [CrossRef] [PubMed]
- Tada, M.; Nagai, T.; Kirihara, K.; Koike, S.; Suga, M.; Araki, T.; Kobayashi, T.; Kasai, K. Differential Alterations of Auditory Gamma Oscillatory Responses between Pre-Onset High-Risk Individuals and First-Episode Schizophrenia. Cereb. Cortex 2016, 26, 1027–1035. [Google Scholar] [CrossRef] [PubMed]
- Parciauskaite, V.; Bjekic, J.; Griskova-Bulanova, I. Gamma-Range Auditory Steady-State Responses and Cognitive Performance: A Systematic Review. Brain Sci. 2021, 11, 217. [Google Scholar] [CrossRef] [PubMed]
- Gao, M.; Rejaei, D.; Liu, H. Ketamine use in current clinical practice. Acta Pharmacol. Sin. 2016, 37, 865–872. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plourde, G.; Baribeau, J.; Bonhomme, V. Ketamine increases the amplitude of the 40-Hz auditory steady-state response in humans. Br. J. Anaesth. 1997, 78, 524–529. [Google Scholar] [CrossRef] [PubMed]
- Sivarao, D.V.; Chen, P.; Senapati, A.; Yang, Y.; Fernandes, A.; Benitex, Y.; Whiterock, V.; Li, Y.-W.; Ahlijanian, M.K. 40 Hz Auditory Steady-State Response Is a Pharmacodynamic Biomarker for Cortical NMDA Receptors. Neuropsychopharmacology 2016, 41, 2232–2240. [Google Scholar] [CrossRef] [Green Version]
- Geyer, M.A.; Vollenweider, F.X. Serotonin research: Contributions to understanding psychoses. Trends Pharmacol. Sci. 2008, 29, 445–453. [Google Scholar] [CrossRef]
- Kantrowitz, J.T. Targeting Serotonin 5-HT2A Receptors to Better Treat Schizophrenia: Rationale and Current Approaches. CNS Drugs 2020, 34, 947–959. [Google Scholar] [CrossRef]
- Stahl, S.M. Beyond the dopamine hypothesis of schizophrenia to three neural networks of psychosis: Dopamine, serotonin, and glutamate. CNS Spectr. 2018, 23, 187–191. [Google Scholar] [CrossRef]
- Švob Štrac, D.; Pivac, N.; Mück-Šeler, D. The serotonergic system and cognitive function. Transl. Neurosci. 2016, 7, 35–49. [Google Scholar] [CrossRef] [Green Version]
- Butcher, J.N.; Graham, J.R.; Fowler, R.D. Special Series: The Mmpi-2*. J. Pers. Assess. 1991, 57, 203–204. [Google Scholar] [CrossRef] [PubMed]
- Sheehan, D.V.; Lecrubier, Y.; Sheehan, K.H.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G.C. The Mini-International Neuropsychiatric Interview (M.I.N.I): The development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 1998, 59 (Suppl. S20), 22–33. [Google Scholar] [PubMed]
- Johnson, M.; Richards, W.; Griffiths, R. Human hallucinogen research: Guidelines for safety. J. Psychopharmacol. 2008, 22, 603–620. [Google Scholar] [CrossRef] [Green Version]
- Nichols, D.E. Psychedelics. Pharmacol. Rev. 2016, 68, 264–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tylš, F.; Páleníček, T.; Kaderábek, L.; Lipski, M.; Kubešová, A.; Horácek, J. Sex differences and serotonergic mechanisms in the behavioural effects of psilocin. Behav. Pharmacol. 2016, 27, 309–320. [Google Scholar] [CrossRef] [PubMed]
- Overall, J.E.; Hollister, L.E.; Pichot, P. Major Psychiatric Disorders: A Four-Dimensional Model. Arch. Gen. Psychiatry 1967, 16, 146–151. [Google Scholar] [CrossRef]
- Strassman, R.J.; Qualls, C.R.; Uhlenhuth, E.H.; Kellner, R. Dose-Response Study of N,N-Dimethyltryptamine in Humans: II. Subjective Effects and Preliminary Results of a New Rating Scale. Arch. Gen. Psychiatry 1994, 51, 98–108. [Google Scholar] [CrossRef]
- Studerus, E.; Gamma, A.; Vollenweider, F.X. Psychometric Evaluation of the Altered States of Consciousness Rating Scale (OAV). PLoS ONE 2010, 5, e12412. [Google Scholar] [CrossRef]
- Dittrich, A. The standardized psychometric assessment of altered states of consciousness (ASCs) in humans. Pharmacopsychiatry 1998, 31 (Suppl. S2), 80–84. [Google Scholar] [CrossRef]
- Tylš, F.; Páleníček, T.; Horáček, J. Psilocybin–Summary of knowledge and new perspectives. Eur. Neuropsychopharmacol. 2014, 24, 342–356. [Google Scholar] [CrossRef]
- Perrin, F.; Pernier, J.; Bertrand, O.; Echallier, J. Spherical splines for scalp potential and current density mapping. Electroencephalogr. Clin. Neurophysiol. 1989, 72, 184–187. [Google Scholar] [CrossRef]
- Górska, U.; Binder, M. Low and medium frequency auditory steady-state responses decrease during NREM sleep. Int. J. Psychophysiol. 2019, 135, 44–54. [Google Scholar] [CrossRef] [PubMed]
- Griskova, I.; Morup, M.; Parnas, J.; Ruksenas, O.; Arnfred, S.M. The amplitude and phase precision of 40 Hz auditory steady-state response depend on the level of arousal. Exp. Brain Res. 2007, 183, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Iber, C.; Ancoli-Israel, S.; Chesson, A.; Quan, S. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications. Am. Acad. Sleep Med. 2007, 176, 16–30. [Google Scholar]
- Mørup, M.; Hansen, L.K.; Arnfred, S.M. ERPWAVELAB: A toolbox for multi-channel analysis of time–frequency transformed event related potentials. J. Neurosci. Methods 2007, 161, 361–368. [Google Scholar] [CrossRef]
- Makeig, S. Auditory event-related dynamics of the EEG spectrum and effects of exposure to tones. Electroencephalogr. Clin. Neurophysiol. 1993, 86, 283–293. [Google Scholar] [CrossRef]
- Griskova-Bulanova, I.; Hubl, D.; van Swam, C.; Dierks, T.; Koenig, T. Early- and late-latency gamma auditory steady-state response in schizophrenia during closed eyes: Does hallucination status matter? Clin. Neurophysiol. 2016, 127, 2214–2221. [Google Scholar] [CrossRef] [Green Version]
- Griskova-Bulanova, I.; Dapsys, K.; Melynyte, S.; Voicikas, A.; Maciulis, V.; Andruskevicius, S.; Korostenskaja, M. 40 Hz auditory steady-state response in schizophrenia: Sensitivity to stimulation type (clicks versus flutter amplitude-modulated tones). Neurosci. Lett. 2018, 662, 152–157. [Google Scholar] [CrossRef]
- Tada, M.; Kirihara, K.; Koshiyama, D.; Fujioka, M.; Usui, K.; Uka, T.; Komatsu, M.; Kunii, N.; Araki, T.; Kasai, K. Gamma-Band Auditory Steady-State Response as a Neurophysiological Marker for Excitation and Inhibition Balance: A Review for Understanding Schizophrenia and Other Neuropsychiatric Disorders. Clin. EEG Neurosci. 2019, 51, 234–243. [Google Scholar] [CrossRef]
- Love, J.; Selker, R.; Verhagen, J.; Marsman, M.; Gronau, Q.F.; Jamil, T.; Smira, M.; Epskamp, S.; Wild, A.; Ly, A.; et al. Software to Sharpen Your Stats. APS Obs. 2015, 28, 27–29. [Google Scholar]
- Parciauskaite, V.; Voicikas, A.; Jurkuvenas, V.; Tarailis, P.; Kraulaidis, M.; Pipinis, E.; Griskova-Bulanova, I. 40-Hz auditory steady-state responses and the complex information processing: An exploratory study in healthy young males. PLoS ONE 2019, 14, e0223127. [Google Scholar] [CrossRef] [PubMed]
- Voicikas, A.; Niciute, I.; Ruksenas, O.; Griskova-Bulanova, I. Effect of attention on 40 Hz auditory steady-state response depends on the stimulation type: Flutter amplitude modulated tones versus clicks. Neurosci. Lett. 2016, 629, 215–220. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, B.F.; Vohs, J.L.; Krishnan, G.P.; Rass, O.; Hetrick, W.P.; Morzorati, S.L. Chapter 6-The auditory steady-state response (ASSR): A translational biomarker for schizophrenia. In Supplements to Clinical Neurophysiology; Başar, E., Başar-Eroĝlu, C., Özerdem, A., Rossini, P.M., Yener, G.G., Eds.; Elsevier: Amsterdam, The Netherlands, 2013; Volume 62, pp. 101–112. [Google Scholar]
- Kozono, N.; Honda, S.; Tada, M.; Kirihara, K.; Zhao, Z.; Jinde, S.; Uka, T.; Yamada, H.; Matsumoto, M.; Kasai, K.; et al. Auditory Steady State Response; nature and utility as a translational science tool. Sci. Rep. 2019, 9, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vohs, J.L.; Chambers, R.A.; Krishnan, G.P.; O’Donnell, B.F.; Berg, S.; Morzorati, S.L. GABAergic modulation of the 40 Hz auditory steady-state response in a rat model of schizophrenia. Int. J. Neuropsychopharmacol. 2010, 13, 487–497. [Google Scholar] [CrossRef] [Green Version]
- Vohs, J.L.; Chambers, R.A.; O’Donnell, B.F.; Krishnan, G.P.; Morzorati, S.L. Auditory steady state responses in a schizophrenia rat model probed by excitatory/inhibitory receptor manipulation. Int. J. Psychophysiol. 2012, 86, 136–142. [Google Scholar] [CrossRef] [Green Version]
- Puig, M.V.; Watakabe, A.; Ushimaru, M.; Yamamori, T.; Kawaguchi, Y. Serotonin Modulates Fast-Spiking Interneuron and Synchronous Activity in the Rat Prefrontal Cortex through 5-HT1A and 5-HT2A Receptors. J. Neurosci. 2010, 30, 2211–2222. [Google Scholar] [CrossRef]
- Akhmetshina, D.; Zakharov, A.; Vinokurova, D.; Nasretdinov, A.; Valeeva, G.; Khazipov, R. The serotonin reuptake inhibitor citalopram suppresses activity in the neonatal rat barrel cortex in vivo. Brain Res. Bull. 2016, 124, 48–54. [Google Scholar] [CrossRef]
- Méndez, P.; Pazienti, A.; Szabó, G.; Bacci, A. Direct Alteration of a Specific Inhibitory Circuit of the Hippocampus by Antidepressants. J. Neurosci. 2012, 32, 16616–16628. [Google Scholar] [CrossRef] [Green Version]
- Cortes-Briones, J.; Skosnik, P.D.; Mathalon, D.; Cahill, J.; Pittman, B.; Williams, A.; Sewell, R.A.; Ranganathan, M.; Roach, B.; Ford, J.; et al. Δ9-THC Disrupts Gamma (γ)-Band Neural Oscillations in Humans. Neuropsychopharmacology 2015, 40, 2124–2134. [Google Scholar] [CrossRef] [Green Version]
- Albrecht, M.A.; Price, G.; Lee, J.; Iyyalol, R.; Martin-Iverson, M.T. Dexamphetamine selectively increases 40 Hz auditory steady state response power to target and nontarget stimuli in healthy humans. J. Psychiatry Neurosci. 2013, 38, 24–32. [Google Scholar] [CrossRef] [Green Version]
- Carhart-Harris, R.L.; Erritzoe, D.; Williams, T.; Stone, J.M.; Reed, L.J.; Colasanti, A.; Tyacke, R.J.; Leech, R.; Malizia, A.L.; Murphy, K.; et al. Neural correlates of the psychedelic state as determined by fMRI studies with psilocybin. Proc. Natl. Acad. Sci. USA 2012, 109, 2138–2143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koshiyama, D.; Miyakoshi, M.; Joshi, Y.B.; Nakanishi, M.; Tanaka-Koshiyama, K.; Sprock, J.; Light, G.A. Source decomposition of the frontocentral auditory steady-state gamma band response in schizophrenia patients and healthy subjects. Psychiatry Clin. Neurosci. 2021, 75, 172–179. [Google Scholar] [CrossRef] [PubMed]
- Euston, D.R.; Gruber, A.J.; McNaughton, B.L. The Role of Medial Prefrontal Cortex in Memory and Decision Making. Neuron 2012, 76, 1057–1070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carhart-Harris, R.L. The entropic brain-revisited. Neuropharmacology 2018, 142, 167–178. [Google Scholar] [CrossRef]
- Molina, J.L.; Thomas, M.L.; Joshi, Y.B.; Hochberger, W.C.; Koshiyama, D.; Nungaray, J.A.; Cardoso, L.; Sprock, J.; Braff, D.L.; Swerdlow, N.R.; et al. Gamma oscillations predict pro-cognitive and clinical response to auditory-based cognitive training in schizophrenia. Transl. Psychiatry 2020, 10, 405. [Google Scholar] [CrossRef]
- Cromheeke, S.; Mueller, S.C. Probing emotional influences on cognitive control: An ALE meta-analysis of cognition emotion interactions. Brain Struct. Funct. 2014, 219, 995–1008. [Google Scholar] [CrossRef] [Green Version]
- Carhart-Harris, R.; Nutt, D. Serotonin and brain function: A tale of two receptors. J. Psychopharmacol. 2017, 31, 1091–1120. [Google Scholar] [CrossRef] [Green Version]
- Carhart-Harris, R.L.; Leech, R.; Hellyer, P.J.; Shanahan, M.; Feilding, A.; Tagliazucchi, E.; Chialvo, D.R.; Nutt, D. The entropic brain: A theory of conscious states informed by neuroimaging research with psychedelic drugs. Front. Hum. Neurosci. 2014, 8, 20. [Google Scholar] [CrossRef] [Green Version]
- Hirano, Y.; Oribe, N.; Onitsuka, T.; Kanba, S.; Nestor, P.G.; Hosokawa, T.; Levin, M.; Shenton, M.E.; McCarley, R.W.; Spencer, K.M. Auditory Cortex Volume and Gamma Oscillation Abnormalities in Schizophrenia. Clin. EEG Neurosci. 2020, 51, 244–251. [Google Scholar] [CrossRef]
- Roach, B.J.; D’Souza, D.C.; Ford, J.M.; Mathalon, D.H. Test-retest reliability of time-frequency measures of auditory steady-state responses in patients with schizophrenia and healthy controls. NeuroImage Clin. 2019, 23, 101878. [Google Scholar] [CrossRef]
- McFadden, K.L.; Steinmetz, S.E.; Carroll, A.M.; Simon, S.T.; Wallace, A.; Rojas, D.C. Test-Retest Reliability of the 40 Hz EEG Auditory Steady-State Response. PLoS ONE 2014, 9, e85748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, H.R.M.; Gross, J.; Uhlhaas, P.J. MEG—measured auditory steady-state oscillations show high test–retest reliability: A sensor and source-space analysis. NeuroImage 2015, 122, 417–426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamata, T.; Nishikawa, M.; Katagi, M.; Tsuchihashi, H. Optimized glucuronide hydrolysis for the detection of psilocin in human urine samples. J. Chromat. B. 2003, 796, 421–427. [Google Scholar] [CrossRef]
- Martin, R.; Schürenkamp, J.; Pfeiffer, H.; Lehr, M.; Köhler, H. Synthesis, hydrolysis and stability of psilocin glucuronide. Forens. Sci. Intern. 2014, 237, 1–6. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Viktorin, V.; Griškova-Bulanova, I.; Voicikas, A.; Dojčánová, D.; Zach, P.; Bravermanová, A.; Andrashko, V.; Tylš, F.; Korčák, J.; Viktorinová, M.; et al. Psilocybin—Mediated Attenuation of Gamma Band Auditory Steady-State Responses (ASSR) Is Driven by the Intensity of Cognitive and Emotional Domains of Psychedelic Experience. J. Pers. Med. 2022, 12, 1004. https://doi.org/10.3390/jpm12061004
Viktorin V, Griškova-Bulanova I, Voicikas A, Dojčánová D, Zach P, Bravermanová A, Andrashko V, Tylš F, Korčák J, Viktorinová M, et al. Psilocybin—Mediated Attenuation of Gamma Band Auditory Steady-State Responses (ASSR) Is Driven by the Intensity of Cognitive and Emotional Domains of Psychedelic Experience. Journal of Personalized Medicine. 2022; 12(6):1004. https://doi.org/10.3390/jpm12061004
Chicago/Turabian StyleViktorin, Vojtěch, Inga Griškova-Bulanova, Aleksandras Voicikas, Dominika Dojčánová, Peter Zach, Anna Bravermanová, Veronika Andrashko, Filip Tylš, Jakub Korčák, Michaela Viktorinová, and et al. 2022. "Psilocybin—Mediated Attenuation of Gamma Band Auditory Steady-State Responses (ASSR) Is Driven by the Intensity of Cognitive and Emotional Domains of Psychedelic Experience" Journal of Personalized Medicine 12, no. 6: 1004. https://doi.org/10.3390/jpm12061004
APA StyleViktorin, V., Griškova-Bulanova, I., Voicikas, A., Dojčánová, D., Zach, P., Bravermanová, A., Andrashko, V., Tylš, F., Korčák, J., Viktorinová, M., Koudelka, V., Hájková, K., Kuchař, M., Horáček, J., Brunovský, M., & Páleníček, T. (2022). Psilocybin—Mediated Attenuation of Gamma Band Auditory Steady-State Responses (ASSR) Is Driven by the Intensity of Cognitive and Emotional Domains of Psychedelic Experience. Journal of Personalized Medicine, 12(6), 1004. https://doi.org/10.3390/jpm12061004