
Cognitive Performance and Health-Related Quality of Life in Patients with Neuromyelitis Optica Spectrum Disorder

 , , , , , , , , ,
, , , , , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Cognitive Functions
2.3. Patient-Centred Measures
2.4. Statistical Analysis
3. Results
3.1. Demographic, Clinical and Patient-Centred Measures of the Cohort
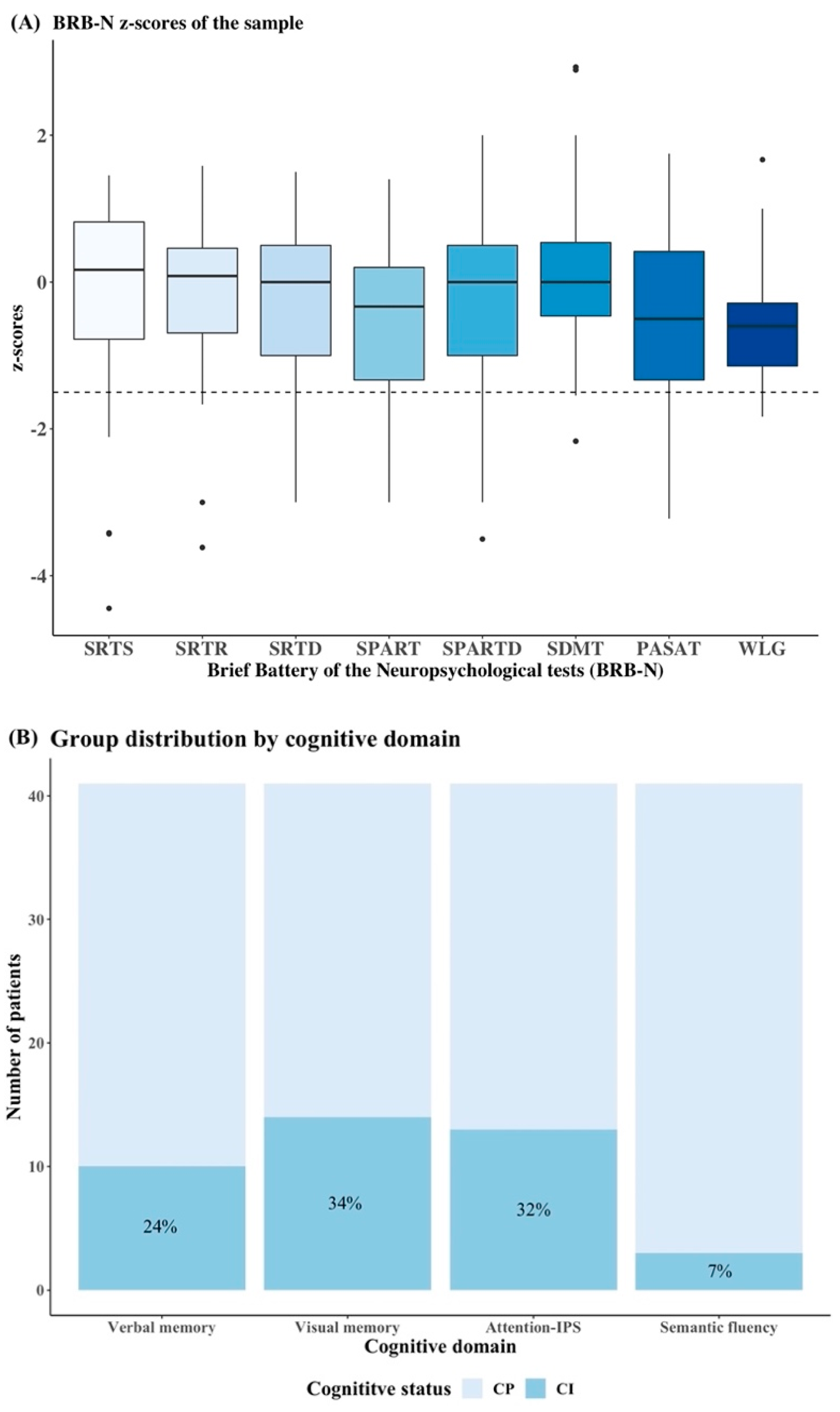
3.2. Cognitive Characteristics in NMOSD Patients
3.3. Association between Cognition, Demographic, Clinical and Patient-Centred Measures
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Oertel, F.C.; Schließeit, J.; Brandt, A.U.; Paul, F. Cognitive Impairment in Neuromyelitis Optica Spectrum Disorders: A Review of Clinical and Neuroradiological Features. Front. Neurol. 2019, 10, 608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weinshenker, B.G.; Wingerchuk, D.M. Neuromyelitis Spectrum Disorders. Mayo Clin. Proc. 2017, 92, 663–679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lennon, V.A.; Wingerchuk, D.M.; Kryzer, T.J.; Pittock, S.J.; Lucchinetti, C.F.; Fujihara, K.; Nakashima, I.; Weinshenker, B.G. A Serum Autoantibody Marker of Neuromyelitis Optica: Distinction from Multiple Sclerosis. Lancet 2004, 364, 2106–2112. [Google Scholar] [CrossRef]
- Wingerchuk, D.M.; Banwell, B.; Bennett, J.L.; Cabre, P.; Carroll, W.; Chitnis, T.; de Seze, J.; Fujihara, K.; Greenberg, B.; Jacob, A.; et al. International Consensus Diagnostic Criteria for Neuromyelitis Optica Spectrum Disorders. Neurology 2015, 85, 177–189. [Google Scholar] [CrossRef]
- Eizaguirre, M.B.; Alonso, R.; Vanotti, S.; Garcea, O. Cognitive Impairment in Neuromyelitis Optica Spectrum Disorders: What Do We Know? Mult. Scler. Relat. Disord. 2017, 18, 225–229. [Google Scholar] [CrossRef]
- Blanc, F.; Zéphir, H.; Lebrun, C.; Labauge, P.; Castelnovo, G.; Fleury, M.; Sellal, F.; Tranchant, C.; Dujardin, K.; Vermersch, P.; et al. Cognitive Functions in Neuromyelitis Optica. Arch. Neurol. 2008, 65, 84–88. [Google Scholar] [CrossRef] [Green Version]
- Moghadasi, A.N.; Mirmosayyeb, O.; Mohammadi, A.; Sahraian, M.A.; Ghajarzadeh, M. The Prevalence of Cognitive Impairment in Patients with Neuromyelitis Optica Spectrum Disorders (NMOSD): A Systematic Review and Meta-Analysis. Mult. Scler. Relat. Disord. 2021, 49, 102757. [Google Scholar] [CrossRef]
- Czarnecka, D.; Oset, M.; Karlińska, I.; Stasiołek, M. Cognitive Impairment in NMOSD—More Questions than Answers. Brain Behav. 2020, 10, e01842. [Google Scholar] [CrossRef]
- Beekman, J.; Keisler, A.; Pedraza, O.; Haramura, M.; Gianella-Borradori, A.; Katz, E.; Ratchford, J.N.; Barron, G.; Cook, L.J.; Behne, J.M.; et al. Neuromyelitis Optica Spectrum Disorder: Patient Experience and Quality of Life. Neurol. Neuroimmunol. Neuroinflamm. 2019, 6, e580. [Google Scholar] [CrossRef] [Green Version]
- Huang, W.; ZhangBao, J.; Chang, X.; Wang, L.; Zhao, C.; Lu, J.; Wang, M.; Ding, X.; Xu, Y.; Zhou, L.; et al. Neuromyelitis Optica Spectrum Disorder in China: Quality of Life and Medical Care Experience. Mult. Scler. Relat. Disord. 2020, 46, 102542. [Google Scholar] [CrossRef]
- Meca-Lallana, J.E.; Prefasi, D.; Pérez-Miralles, F.; Forero, L.; Sepúlveda, M.; Calles, C.; Martínez-Ginés, M.L.; González-Suárez, I.; Boyero, S.; Romero-Pinel, L.; et al. Perception of Stigma in Patients with Neuromyelitis Optica Spectrum Disorder. Patient Prefer. Adherence 2021, 15, 713–719. [Google Scholar] [CrossRef] [PubMed]
- Kurtzke, J.F. Rating Neurologic Impairment in Multiple Sclerosis: An Expanded Disability Status Scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benedict, R.H.B.; Fishman, I.; McClellan, M.M.; Bakshi, R.; Weinstock-Guttman, B. Validity of the Beck Depression Inventory-Fast Screen in Multiple Sclerosis. Mult. Scler. 2003, 9, 393–396. [Google Scholar] [CrossRef] [PubMed]
- Fisk, J.D.; Doble, S.E. Construction and Validation of a Fatigue Impact Scale for Daily Administration (D-FIS). Qual. Life Res. 2002, 11, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.M.; Leo, G.J.; Bernardin, L.; Unverzagt, F. Cognitive Dysfunction in Multiple Sclerosis. I. Frequency, Patterns, and Prediction. Neurology 1991, 41, 685–691. [Google Scholar] [CrossRef]
- Sepulcre, J.; Vanotti, S.; Hernández, R.; Sandoval, G.; Cáceres, F.; Garcea, O.; Villoslada, P. Cognitive Impairment in Patients with Multiple Sclerosis Using the Brief Repeatable Battery-Neuropsychology Test. Mult. Scler. 2006, 12, 187–195. [Google Scholar] [CrossRef]
- Hobart, J.; Lamping, D.; Fitzpatrick, R.; Riazi, A.; Thompson, A. The Multiple Sclerosis Impact Scale (MSIS-29): A New Patient-Based Outcome Measure. Brain 2001, 124, 962–973. [Google Scholar] [CrossRef]
- Pavot, W.; Diener, E.; Colvin, C.R.; Sandvik, E. Further Validation of the Satisfaction with Life Scale: Evidence for the Cross-Method Convergence of Well-Being Measures. J. Personal. Assess. 1991, 57, 149–161. [Google Scholar] [CrossRef]
- Green, R.; Kalina, J.; Ford, R.; Pandey, K.; Kister, I. SymptoMScreen: A Tool for Rapid Assessment of Symptom Severity in MS Across Multiple Domains. Appl. Neuropsychol. Adult 2017, 24, 183–189. [Google Scholar] [CrossRef]
- Molina, Y.; Choi, S.W.; Cella, D.; Rao, D. The Stigma Scale for Chronic Illnesses 8-Item Version (SSCI-8): Development, Validation and Use across Neurological Conditions. Int. J. Behav. Med. 2013, 20, 450–460. [Google Scholar] [CrossRef]
- Stewart, A.L.; Hays, R.D.; Ware, J.E. The MOS Short-Form General Health Survey. Med. Care 1988, 26, 724–735. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-H.; Park, E.Y.; Park, B.; Hyun, J.-W.; Park, N.Y.; Joung, A.; Lee, S.H.; Kim, H.J. Multimodal Magnetic Resonance Imaging in Relation to Cognitive Impairment in Neuromyelitis Optica Spectrum Disorder. Sci. Rep. 2017, 7, 9180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.-H.; Kwak, K.; Jeong, I.H.; Hyun, J.-W.; Jo, H.-J.; Joung, A.; Yu, E.-S.; Kim, J.-H.; Lee, S.H.; Yun, S.; et al. Cognitive Impairment Differs between Neuromyelitis Optica Spectrum Disorder and Multiple Sclerosis. Mult. Scler. 2016, 22, 1850–1858. [Google Scholar] [CrossRef]
- Vanotti, S.; Cores, E.V.; Eizaguirre, B.; Melamud, L.; Rey, R.; Villa, A. Cognitive Performance of Neuromyelitis Optica Patients: Comparison with Multiple Sclerosis. Arq. Neuropsiquiatr. 2013, 71, 357–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saji, E.; Arakawa, M.; Yanagawa, K.; Toyoshima, Y.; Yokoseki, A.; Okamoto, K.; Otsuki, M.; Akazawa, K.; Kakita, A.; Takahashi, H.; et al. Cognitive Impairment and Cortical Degeneration in Neuromyelitis Optica. Ann. Neurol. 2013, 73, 65–76. [Google Scholar] [CrossRef]
- Yabalak, A.; Altunrende, B.; Demir, G.A. Cognitive Impairment in Neuromyelitis Optica. Noro Psikiyatr. Ars. 2021, 58, 200–205. [Google Scholar] [CrossRef]
- Salama, S.; Marouf, H.; Reda, M.I.; Mansour, A.R.; ELKholy, O.; Levy, M. Cognitive Functions in Egyptian Neuromyelitis Optica Spectrum Disorder. Clin. Neurol. Neurosurg. 2020, 189, 105621. [Google Scholar] [CrossRef]
- Zhang, N.; Li, Y.J.; Fu, Y.; Shao, J.H.; Luo, L.L.; Yang, L.; Shi, F.D.; Liu, Y. Cognitive Impairment in Chinese Neuromyelitis Optica. Mult. Scler. 2015, 21, 1839–1846. [Google Scholar] [CrossRef]
- Moore, P.; Methley, A.; Pollard, C.; Mutch, K.; Hamid, S.; Elsone, L.; Jacob, A. Cognitive and Psychiatric Comorbidities in Neuromyelitis Optica. J. Neurol. Sci. 2016, 360, 4–9. [Google Scholar] [CrossRef]
- Liu, Y.; Fu, Y.; Schoonheim, M.M.; Zhang, N.; Fan, M.; Su, L.; Shen, Y.; Yan, Y.; Yang, L.; Wang, Q.; et al. Structural MRI Substrates of Cognitive Impairment in Neuromyelitis Optica. Neurology 2015, 85, 1491–1499. [Google Scholar] [CrossRef]
- Bo, M.; Niegowska, M.; Arru, G.; Sechi, E.; Mariotto, S.; Mancinelli, C.; Farinazzo, A.; Alberti, D.; Gajofatto, A.; Ferrari, S.; et al. Mycobacterium Avium Subspecies Paratuberculosis and Myelin Basic Protein Specific Epitopes Are Highly Recognized by Sera from Patients with Neuromyelitis Optica Spectrum Disorder. J. Neuroimmunol. 2018, 318, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Slavin, Y.N.; Bo, M.; Caggiu, E.; Sechi, G.; Arru, G.; Bach, H.; Sechi, L.A. High Levels of Antibodies against PtpA and PknG Secreted by Mycobacterium Avium Ssp. Paratuberculosis Are Present in Neuromyelitis Optica Spectrum Disorder and Multiple Sclerosis Patients. J. Neuroimmunol. 2018, 323, 49–52. [Google Scholar] [CrossRef] [PubMed]
- Arru, G.; Sechi, E.; Mariotto, S.; Zarbo, I.R.; Ferrari, S.; Gajofatto, A.; Monaco, S.; Deiana, G.A.; Bo, M.; Sechi, L.A.; et al. Antibody Response against HERV-W in Patients with MOG-IgG Associated Disorders, Multiple Sclerosis and NMOSD. J. Neuroimmunol. 2020, 338, 577110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blanc, F.; Noblet, V.; Jung, B.; Rousseau, F.; Renard, F.; Bourre, B.; Longato, N.; Cremel, N.; Di Bitonto, L.; Kleitz, C.; et al. White Matter Atrophy and Cognitive Dysfunctions in Neuromyelitis Optica. PLoS ONE 2012, 7, e33878. [Google Scholar] [CrossRef] [PubMed]
- Chanson, J.-B.; Zéphir, H.; Collongues, N.; Outteryck, O.; Blanc, F.; Fleury, M.; Vermersch, P.; de Seze, J. Evaluation of Health-Related Quality of Life, Fatigue and Depression in Neuromyelitis Optica. Eur. J. Neurol. 2011, 18, 836–841. [Google Scholar] [CrossRef]

{kind=link}
| NMOSD Cohort (n = 41) | |
|---|---|
| Demographic and clinical data | |
| Age (years) | 44 (39–49) |
| Female, n (%) | 35 (85) |
| Disease duration (years) | 8.1 (3.9–15.5) |
| AQP4-IgG positive, n (%) | 27 (66) |
| EDSS score (range) | 2.0 (0–7.5) |
| Number of relapses | 2.5 (1–4) |
| Current treatment, n (%) | 37 (90) |
| Beck Depression Inventory-Fast Screen (BDI-FS) | 3 (0–6) |
| Fatigue Impact Scale for Daily Use (D-FIS) | 6 (2–18) |
| Patient-centred measures | |
| Physical MSIS-29v2 | 35 (23–49) |
| Psychological MSIS-29v2 | 21 (14–29) |
| Satisfaction with Life Scale (SWLS) | 21 (18–25) |
| SymptoMScreen questionnaire (SyMS) | 16 (8–30) |
| Stigma Scale for Chronic Illness (SSCI-8) | 9 (8–14) |
| MOS Pain Effects Scale (PES) | 15 (9–20) |
| Cognitive z-Score | AQP4-IgG Positive (n = 27) | AQP4-IgG Negative (n = 13) | Corrected p-Value |
|---|---|---|---|
| Verbal memory | |||
| z-score SRTS (storage) | 0.17 (−0.49–0.86) | 0.17 (−0.89–0.54) | 0.952 b |
| z-score SRTR (retrieval) | 0.23 (−0.60–0.50) | −0.25 (−1.08–0.46) | 0.952 b |
| z-score SRTD (delayed) | 0.0 (−1.25–0.50) | −0.50 (−1.0–1.0) | 0.952 b |
| Verbal memory z-score | 0.05 (−0.54–0.66) | −0.04 (−0.62–0.69) | 0.977 b |
| Visual memory | |||
| z-score SPART (storage) | −0.50 (−1.42–0.55) | −0.20 (−0.67–0.17) | 0.952 a |
| z-score SPARTD (delayed) | 0.0 (−1.5–0.5) | −0.50 (−1.0–0.0) | 0.952 a |
| Visual memory z-score | −0.67 (−1.40–0.55) | −0.33 (−0.67–0.08) | 0.952 a |
| Attention and information processing speed | |||
| z-score SDMT | 0.12 (−0.61–0.54) | 0.0 (−0.29–1.29) | 0.952 a |
| z-score PASAT 3 | −0.50 (−1.29–0.65) | −0.44 (−1.33–0.33) | 0.952 a |
| Attention-IPS z-score | −0.28 (−1.06–0.50) | −0.15 (−0.89–0.70) | 0.952 a |
| Semantic fluency | |||
| z-score WLG | −0.60 (−0.86–−0.18) | −0.6 (−1.17–−0.29) | 0.952 b |
| Semantic fluency z-score | −0.60 (−0.86–−0.18) | −0.6 (−1.17–−0.29) | 0.952 b |
| Global cognition (zBRB-N) | |||
| BRB-N z-score | −0.32 (−0.93–0.21) | −0.17 (−0.97–0.15) | 0.977 a |
| Parameters | β (95% CI) | Corrected p-Value |
|---|---|---|
| Gender | −0.418 (−0.92–0.09) | 0.102 |
| Beck Depression Inventory-Fast Screen (BDI-FS) | 0.654 (0.26–1.05) | 0.002 |
| Fatigue Impact Scale for Daily Use (D-FIS) | −0.388 (−0.72–−0.05) | 0.024 |
| Satisfaction with Life Scale (SWLS) | 0.343 (0.08–0.60) | 0.011 |
| Stigma Scale for Chronic Illness (SSCI-8) | −0.361 (−0.65–−0.07) | 0.016 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lopez-Soley, E.; Meca-Lallana, J.E.; Llufriu, S.; Blanco, Y.; Gómez-Ballesteros, R.; Maurino, J.; Pérez-Miralles, F.; Forero, L.; Calles, C.; Martinez-Gines, M.L.; et al. Cognitive Performance and Health-Related Quality of Life in Patients with Neuromyelitis Optica Spectrum Disorder. J. Pers. Med. 2022, 12, 743. https://doi.org/10.3390/jpm12050743
Lopez-Soley E, Meca-Lallana JE, Llufriu S, Blanco Y, Gómez-Ballesteros R, Maurino J, Pérez-Miralles F, Forero L, Calles C, Martinez-Gines ML, et al. Cognitive Performance and Health-Related Quality of Life in Patients with Neuromyelitis Optica Spectrum Disorder. Journal of Personalized Medicine. 2022; 12(5):743. https://doi.org/10.3390/jpm12050743
Chicago/Turabian StyleLopez-Soley, Elisabet, Jose E. Meca-Lallana, Sara Llufriu, Yolanda Blanco, Rocío Gómez-Ballesteros, Jorge Maurino, Francisco Pérez-Miralles, Lucía Forero, Carmen Calles, María L. Martinez-Gines, and et al. 2022. "Cognitive Performance and Health-Related Quality of Life in Patients with Neuromyelitis Optica Spectrum Disorder" Journal of Personalized Medicine 12, no. 5: 743. https://doi.org/10.3390/jpm12050743
APA StyleLopez-Soley, E., Meca-Lallana, J. E., Llufriu, S., Blanco, Y., Gómez-Ballesteros, R., Maurino, J., Pérez-Miralles, F., Forero, L., Calles, C., Martinez-Gines, M. L., Gonzalez-Suarez, I., Boyero, S., Romero-Pinel, L., Sempere, Á. P., Meca-Lallana, V., Querol, L., Costa-Frossard, L., Sepulveda, M., & Solana, E. (2022). Cognitive Performance and Health-Related Quality of Life in Patients with Neuromyelitis Optica Spectrum Disorder. Journal of Personalized Medicine, 12(5), 743. https://doi.org/10.3390/jpm12050743