
Improving the Safety of DIEP Flap Transplantation: Detailed Perforator Anatomy Study Using Preoperative CTA †

 , ,
, ,  ,
,  ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Diameter and Branching of Perforators
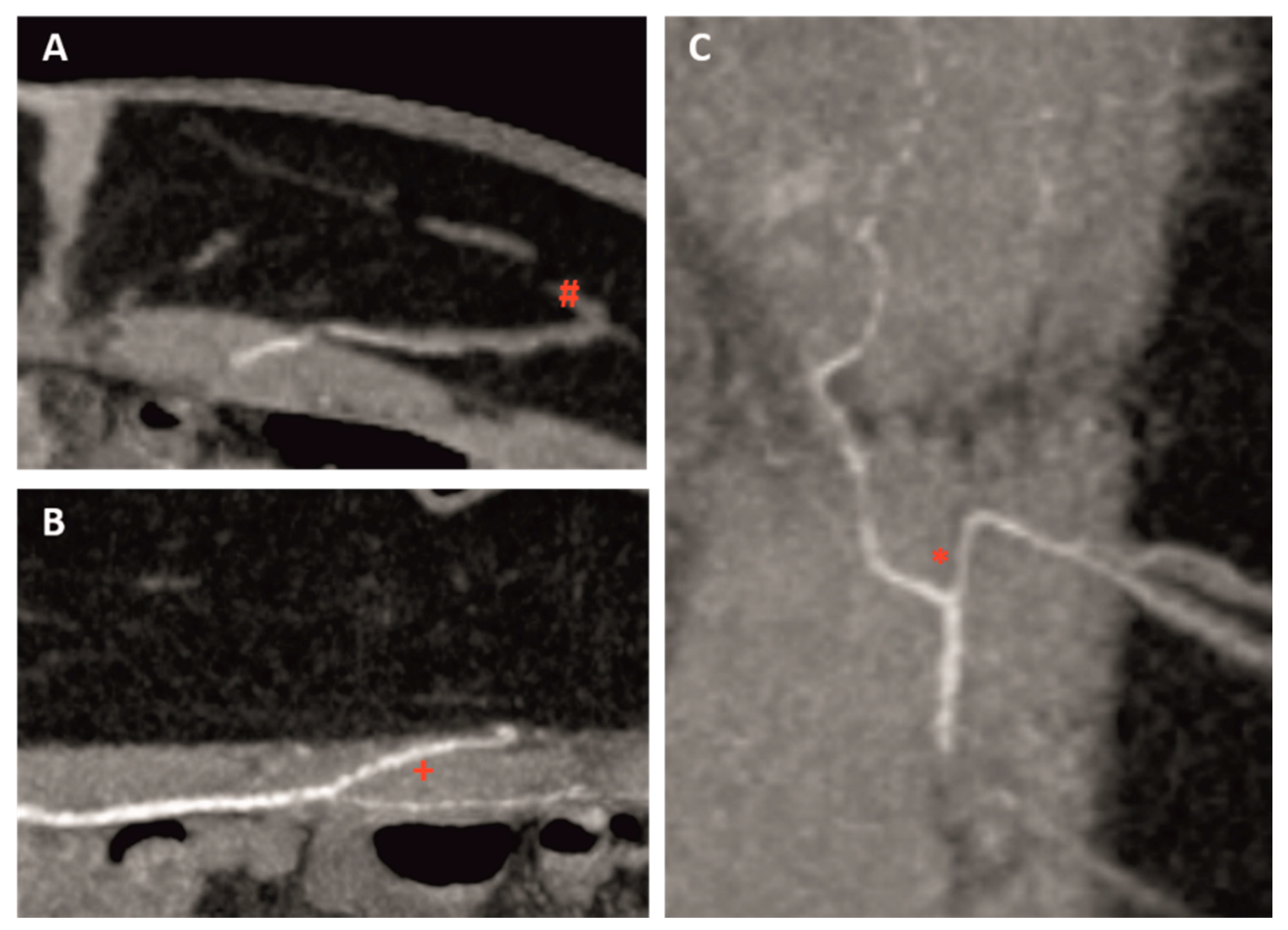
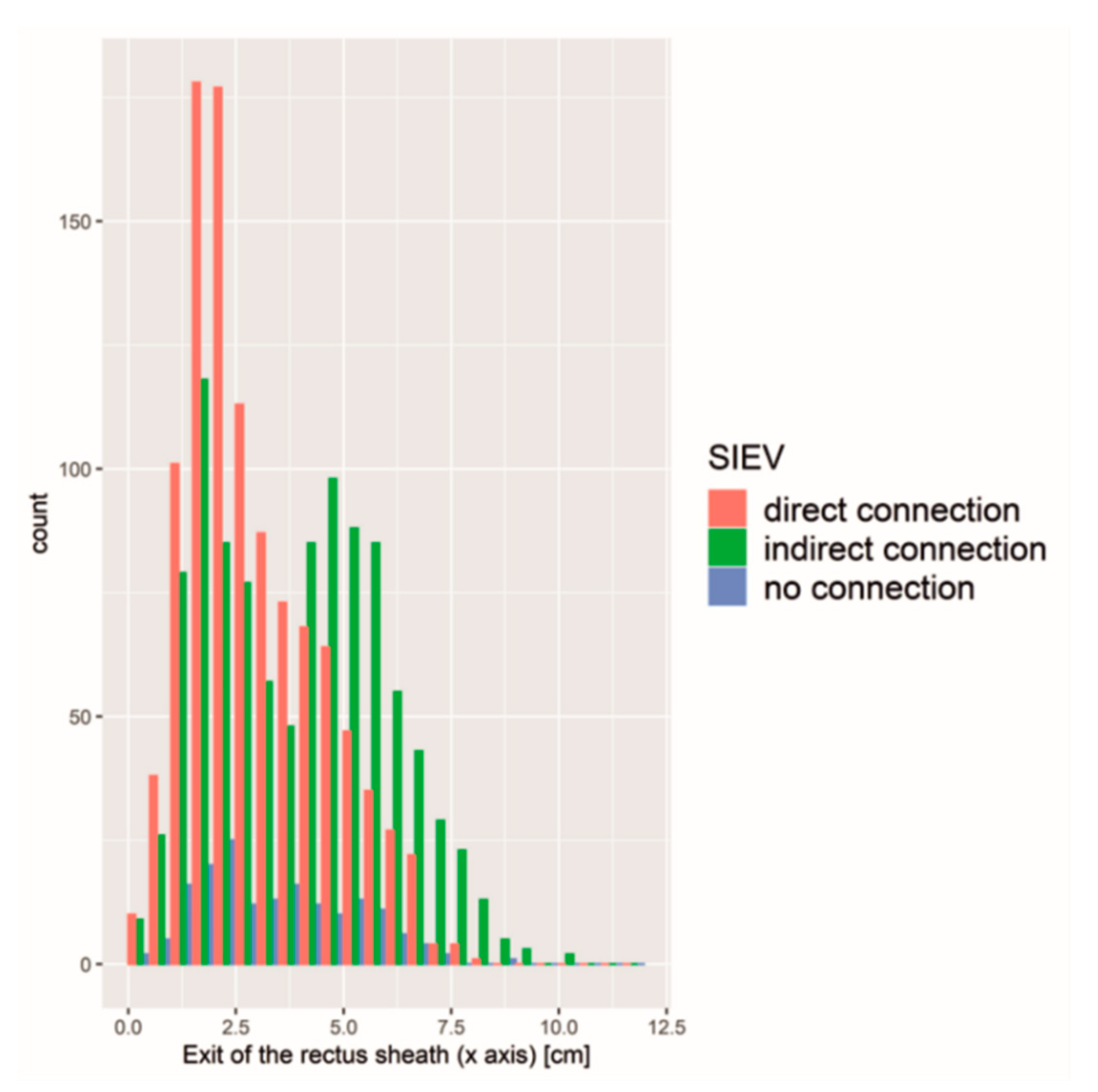
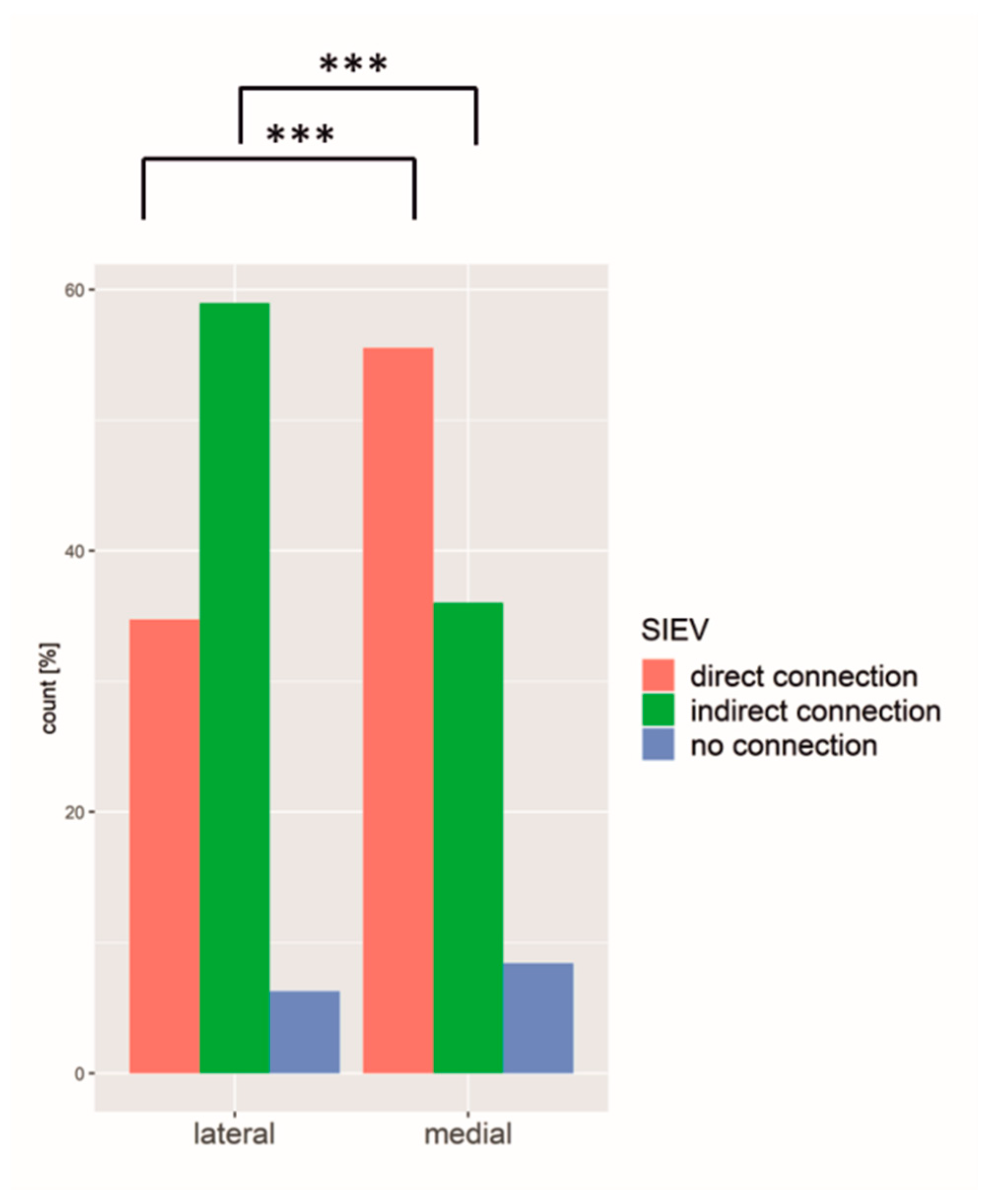
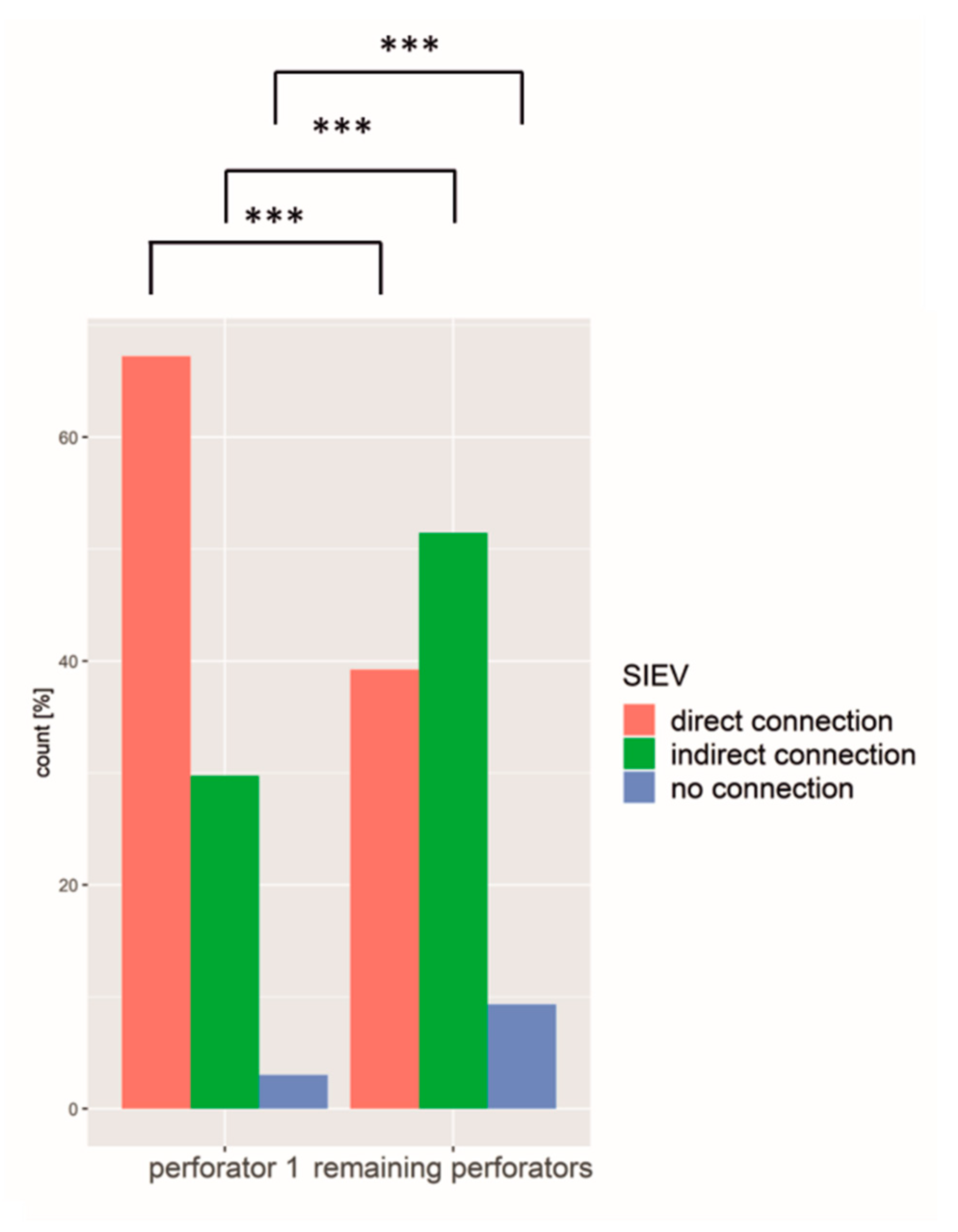
3.2. SIEV
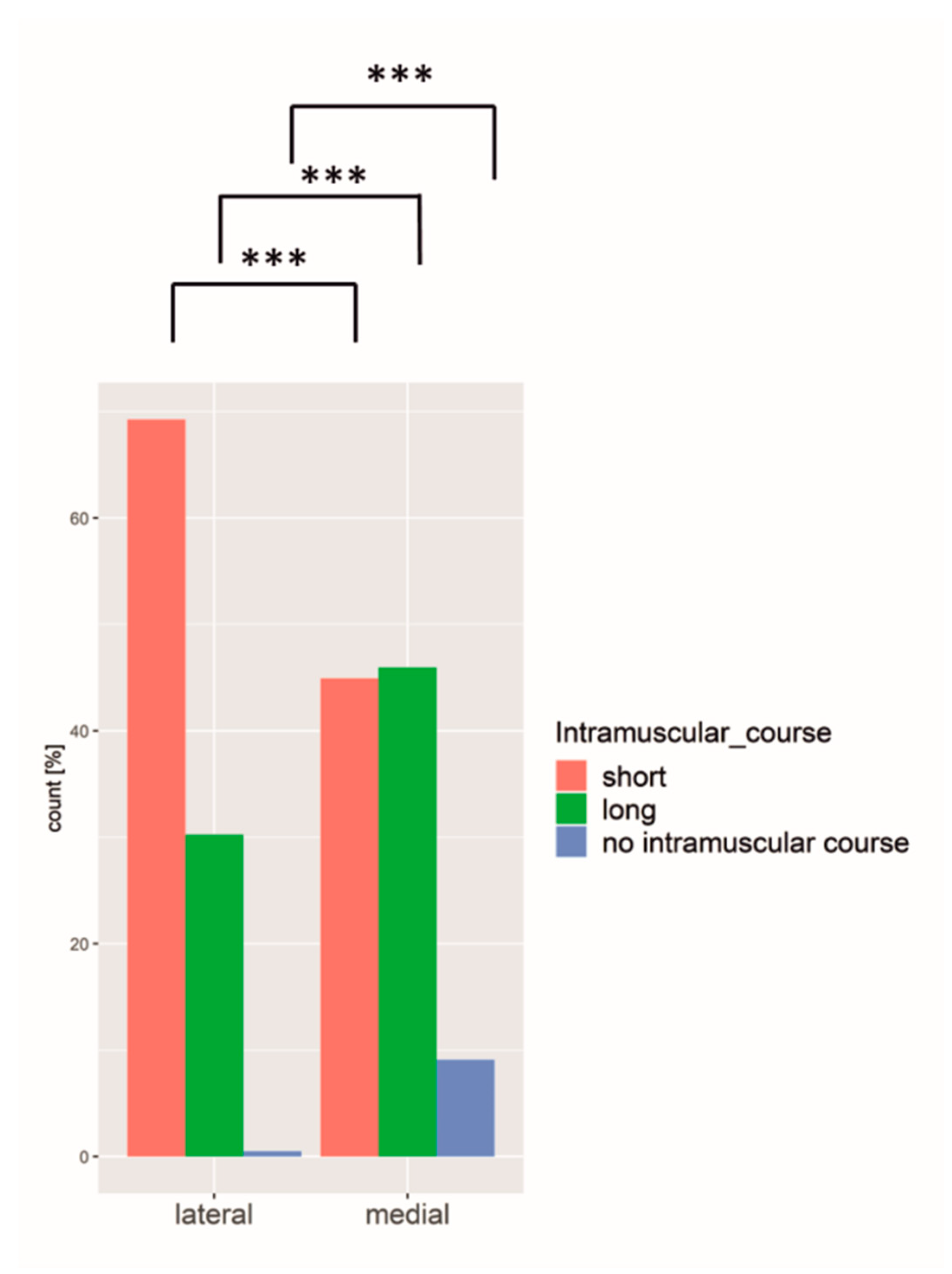
3.3. Intramuscular Course
3.4. Largest Perforator (No 1)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Robert Koch Institut. Krebs in Deutschland für 2015/2016. Available online: https://www.krebsdaten.de/Krebs/DE/Content/Publikationen/Krebs_in_Deutschland/kid_2019/krebs_in_deutschland_2019.pdf;jsessionid=ADE676158568FB2E31DD9F4EC7162474.2_cid372?__blob=publicationFile (accessed on 1 March 2020).
- Francies, F.Z.; Hull, R.; Khanyile, R.; Dlamini, Z. Breast cancer in low-middle income countries: Abnormality in splicing and lack of targeted treatment options. Am. J. Cancer Res. 2020, 10, 1568–1591. [Google Scholar] [PubMed]
- Chen, K.; Lu, P.; Beeraka, N.M.; Sukocheva, O.A.; Madhunapantula, S.V.; Liu, J.; Sinelnikov, M.Y.; Nikolenko, V.N.; Bulygin, K.V.; Mikhaleva, L.M.; et al. Mitochondrial mutations and mitoepigenetics: Focus on regulation of oxidative stress-induced responses in breast cancers. Semin. Cancer Biol. 2020, in press. [CrossRef]
- Alderman, A.K.; Wilkins, E.G.; Lowery, J.C.; Kim, M.; Davis, J.A. Determinants of patient satisfaction in postmastectomy breast reconstruction. Plast. Reconstr. Surg. 2000, 106, 769–776. [Google Scholar] [CrossRef]
- Steiner, D.; Horch, R.E.; Ludolph, I.; Schmitz, M.; Beier, J.P.; Arkudas, A. Interdisciplinary Treatment of Breast Cancer After Mastectomy With Autologous Breast Reconstruction Using Abdominal Free Flaps in a University Teaching Hospital-A Standardized and Safe Procedure. Front. Oncol. 2020, 10, 177. [Google Scholar] [CrossRef]
- Allen, R.J.; Treece, P. Deep inferior epigastric perforator flap for breast reconstruction. Ann. Plast. Surg. 1994, 32, 32–38. [Google Scholar] [CrossRef]
- Chen, K.; Zhang, J.; Beeraka, N.M.; Sinelnikov, M.Y.; Zhang, X.; Cao, Y.; Lu, P. Robot-Assisted Minimally Invasive Breast Surgery: Recent Evidence with Comparative Clinical Outcomes. J. Clin. Med. 2022, 11, 1827. [Google Scholar] [CrossRef]
- Ludolph, I.; Horch, R.E.; Harlander, M.; Arkudas, A.; Bach, A.D.; Kneser, U.; Schmitz, M.; Taeger, C.D.; Beier, J.P. Is there a Rationale for Autologous Breast Reconstruction in Older Patients? A Retrospective Single Center Analysis of Quality of life, Complications and Comorbidities after DIEP or ms-TRAM Flap Using the BREAST-Q. Breast J. 2015, 21, 588–595. [Google Scholar] [CrossRef]
- Steiner, D.; Horch, R.E.; Ludolph, I.; Arkudas, A. Successful free flap salvage upon venous congestion in bilateral breast reconstruction using a venous cross-over bypass: A case report. Microsurgery 2020, 40, 74–78. [Google Scholar] [CrossRef]
- Fritschen, U.V.; Grill, B.; Wagner, J.; Schuster, H.; Sukhova, I.; Giunta, R.E.; Heitmann, C.; Andree, C.; Horch, R.E.; Kneser, U.; et al. Quality assurance in breast reconstruction—Establishment of a prospective national online registry for microsurgical breast reconstructions. Handchir. Mikrochir. Plast. Chir. 2020, 52, 58–66. [Google Scholar] [CrossRef]
- Cai, A.; Suckau, J.; Arkudas, A.; Beier, J.P.; Momeni, A.; Horch, R.E. Autologous Breast Reconstruction with Transverse Rectus Abdominis Musculocutaneous (TRAM) or Deep Inferior Epigastric Perforator (DIEP) Flaps: An Analysis of the 100 Most Cited Articles. Med. Sci. Monit. 2019, 25, 3520–3536. [Google Scholar] [CrossRef] [PubMed]
- Hauck, T.; Horch, R.E.; Schmitz, M.; Arkudas, A. Secondary breast reconstruction after mastectomy using the DIEP flap. Surg. Oncol. 2018, 27, 513. [Google Scholar] [CrossRef] [PubMed]
- Eisenhardt, S.U.; Momeni, A.; von Fritschen, U.; Horch, R.E.; Stark, G.B.; Bannasch, H.; Harder, Y.; Heitmann, C.; Kremer, T.; Rieger, U.M.; et al. Breast reconstruction with the free TRAM or DIEP flap—What is the current standard? Consensus Statement of the German Speaking Working Group for Microsurgery of the Peripheral Nerves and Vessels. Handchir. Mikrochir. Plast. Chir. 2018, 50, 248–255, Erratum in Handchir. Mikrochir. Plast. Chir. 2018, 50, E1. [Google Scholar] [CrossRef]
- Blondeel, P.N. One hundred free DIEP flap breast reconstructions: A personal experience. Br. J. Plast. Surg. 1999, 52, 104–111. [Google Scholar] [CrossRef] [PubMed]
- Casey, W.J., 3rd; Chew, R.T.; Rebecca, A.M.; Smith, A.A.; Collins, J.M.; Pockaj, B.A. Advantages of preoperative computed tomography in deep inferior epigastric artery perforator flap breast reconstruction. Plast. Reconstr. Surg. 2009, 123, 1148–1155. [Google Scholar] [CrossRef]
- Salgarello, M.; Pagliara, D.; Rossi, M.; Visconti, G.; Barone-Adesi, L. Postoperative Monitoring of Free DIEP Flap in Breast Reconstruction with Near-Infrared Spectroscopy: Variables Affecting the Regional Oxygen Saturation. J. Reconstr. Microsurg. 2018, 34, 383–388. [Google Scholar] [CrossRef]
- Chen, K.; Beeraka, N.M.; Sinelnikov, M.Y.; Zhang, J.; Song, D.; Gu, Y.; Li, J.; Reshetov, I.V.; Startseva, O.I.; Liu, J.; et al. Patient Management Strategies in Perioperative, Intraoperative, and Postoperative Period in Breast Reconstruction With DIEP-Flap: Clinical Recommendations. Front. Surg. 2022, 9, 729181. [Google Scholar] [CrossRef]
- Rozen, W.M.; Ashton, M.W.; Stella, D.L.; Phillips, T.J.; Grinsell, D.; Taylor, G.I. The accuracy of computed tomographic angiography for mapping the perforators of the deep inferior epigastric artery: A blinded, prospective cohort study. Plast. Reconstr. Surg. 2008, 122, 1003–1009. [Google Scholar] [CrossRef]
- Taylor, G.I.; Doyle, M.; McCarten, G. The Doppler probe for planning flaps: Anatomical study and clinical applications. Br. J. Plast. Surg. 1990, 43, 1–16. [Google Scholar] [CrossRef]
- Ahn, C.Y.; Narayanan, K.; Shaw, W.W. In vivo anatomic study of cutaneous perforators in free flaps using magnetic resonance imaging. J. Reconstr. Microsurg. 1994, 10, 157–163. [Google Scholar] [CrossRef]
- Masia, J.; Clavero, J.A.; Larranaga, J.R.; Alomar, X.; Pons, G.; Serret, P. Multidetector-row computed tomography in the planning of abdominal perforator flaps. J. Plast. Reconstr. Aesthet. Surg. 2006, 59, 594–599. [Google Scholar] [CrossRef] [PubMed]
- Alonso-Burgos, A.; Garcia-Tutor, E.; Bastarrika, G.; Cano, D.; Martinez-Cuesta, A.; Pina, L.J. Preoperative planning of deep inferior epigastric artery perforator flap reconstruction with multislice-CT angiography: Imaging findings and initial experience. J. Plast. Reconstr. Aesthet. Surg. 2006, 59, 585–593. [Google Scholar] [CrossRef] [PubMed]
- Rozen, W.M.; Stella, D.L.; Ashton, M.W.; Phillips, T.J.; Taylor, G.I. Three-dimensional CT angiography: A new technique for imaging microvascular anatomy. Clin. Anat. 2007, 20, 1001–1003. [Google Scholar] [CrossRef]
- Rozen, W.M.; Phillips, T.J.; Ashton, M.W.; Stella, D.L.; Gibson, R.N.; Taylor, G.I. Preoperative imaging for DIEA perforator flaps: A comparative study of computed tomographic angiography and doppler ultrasound. Plast. Reconstr. Surg. 2008, 121, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Bailey, S.H.; Saint-Cyr, M.; Wong, C.; Mojallal, A.; Zhang, K.; Ouyang, D.; Arbique, G.; Trussler, A.; Rohrich, R.J. The single dominant medial row perforator DIEP flap in breast reconstruction: Three-dimensional perforasome and clinical results. Plast. Reconstr. Surg. 2010, 126, 739–751. [Google Scholar] [CrossRef] [PubMed]
- Ghattaura, A.; Henton, J.; Jallali, N.; Rajapakse, Y.; Savidge, C.; Allen, S.; Searle, A.E.; Harris, P.A.; James, S.E. One hundred cases of abdominal-based free flaps in breast reconstruction. The impact of preoperative computed tomographic angiography. J. Plast. Reconstr. Aesthet. Surg. 2010, 63, 1597–1601. [Google Scholar] [CrossRef]
- Rosson, G.D.; Williams, C.G.; Fishman, E.K.; Singh, N.K. 3D CT angiography of abdominal wall vascular perforators to plan DIEAP flaps. Microsurgery 2007, 27, 641–646. [Google Scholar] [CrossRef]
- Rozen, W.M.; Ashton, M.W. Improving outcomes in autologous breast reconstruction. Aesthetic Plast. Surg. 2009, 33, 327–335. [Google Scholar] [CrossRef]
- Salgarello, M.; Pagliara, D.; Visconti, G.; Barone-Adesi, L. Tissue Oximetry Monitoring for Free Deep Inferior Epigastric Perforator Flap Viability: Factors to be Considered toward Optimizing Postoperative Outcome. J. Reconstr. Microsurg. 2018, 34, e4. [Google Scholar] [CrossRef]
- Rozen, W.M.; Ashton, M.W.; Grinsell, D. The branching pattern of the deep inferior epigastric artery revisited in-vivo: A new classification based on CT angiography. Clin. Anat. 2010, 23, 87–92. [Google Scholar] [CrossRef]
- Rozen, W.M.; Garcia-Tutor, E.; Alonso-Burgos, A.; Acosta, R.; Stillaert, F.; Zubieta, J.L.; Hamdi, M.; Whitaker, I.S.; Ashton, M.W. Planning and optimising DIEP flaps with virtual surgery: The Navarra experience. J. Plast. Reconstr. Aesthet. Surg. 2010, 63, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Schrogendorfer, K.F.; Nickl, S.; Keck, M.; Lumenta, D.B.; Loewe, C.; Gschwandtner, M.; Haslik, W.; Nedomansky, J. Viability of five different pre- and intraoperative imaging methods for autologous breast reconstruction. Eur. Surg. 2016, 48, 326–333. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Masia, J.; Kosutic, D.; Clavero, J.A.; Larranaga, J.; Vives, L.; Pons, G. Preoperative computed tomographic angiogram for deep inferior epigastric artery perforator flap breast reconstruction. J. Reconstr. Microsurg. 2010, 26, 21–28. [Google Scholar] [CrossRef]
- Cina, A.; Barone-Adesi, L.; Rinaldi, P.; Cipriani, A.; Salgarello, M.; Masetti, R.; Bonomo, L. Planning deep inferior epigastric perforator flaps for breast reconstruction: A comparison between multidetector computed tomography and magnetic resonance angiography. Eur. Radiol. 2013, 23, 2333–2343. [Google Scholar] [CrossRef]
- Karunanithy, N.; Rose, V.; Lim, A.K.; Mitchell, A. CT angiography of inferior epigastric and gluteal perforating arteries before free flap breast reconstruction. Radiographics 2011, 31, 1307–1319. [Google Scholar] [CrossRef] [PubMed]
- Mohan, A.T.; Saint-Cyr, M. Anatomic and physiological fundamentals for autologous breast reconstruction. Gland. Surg. 2015, 4, 116–133. [Google Scholar] [CrossRef] [PubMed]
- Wong, C.; Saint-Cyr, M.; Arbique, G.; Becker, S.; Brown, S.; Myers, S.; Rohrich, R.J. Three- and four-dimensional computed tomography angiographic studies of commonly used abdominal flaps in breast reconstruction. Plast. Reconstr. Surg. 2009, 124, 18–27. [Google Scholar] [CrossRef]
- Pellegrin, A.; Stocca, T.; Belgrano, M.; Bertolotto, M.; Pozzi-Mucelli, F.; Marij Arnez, Z.; Cova, M.A. Preoperative vascular mapping with multislice CT of deep inferior epigastric artery perforators in planning breast reconstruction after mastectomy. Radiol. Med. 2013, 118, 732–743. [Google Scholar] [CrossRef]
- Kelly, J.A.; Pacifico, M.D. Lateralising paraumbilical medial row perforators: Dangers and pitfalls in DIEP FLAP planning: A systematic review of 1116 DIEP flaps. J. Plast. Reconstr. Aesthet. Surg. 2014, 67, 383–388. [Google Scholar] [CrossRef]
- Pennington, D.G.; Rome, P.; Kitchener, P. Predicting results of DIEP flap reconstruction: The flap viability index. J. Plast. Reconstr. Aesthet. Surg. 2012, 65, 1490–1495. [Google Scholar] [CrossRef]
- Kuekrek, H.; Muller, D.; Paepke, S.; Dobritz, M.; Machens, H.G.; Giunta, R.E. [Preoperative CT angiography for planning free perforator flaps in breast reconstruction]. Handchir. Mikrochir. Plast. Chir. 2011, 43, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Mu, D.; Yang, Y.; Li, W.; Lin, Y.; Li, H.; Luan, J. Predicting the Feasibility of Utilizing SIEA Flap for Breast Reconstruction with Preoperative BMI and Computed Tomography Angiography (CTA) Data. Aesthetic Plast. Surg. 2020, 45, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Pusic, A.L.; Klassen, A.F.; Scott, A.M.; Klok, J.A.; Cordeiro, P.G.; Cano, S.J. Development of a new patient-reported outcome measure for breast surgery: The BREAST-Q. Plast. Reconstr. Surg. 2009, 124, 345–353. [Google Scholar] [CrossRef] [PubMed]
- Cohen, W.A.; Mundy, L.R.; Ballard, T.N.; Klassen, A.; Cano, S.J.; Browne, J.; Pusic, A.L. The BREAST-Q in surgical research: A review of the literature 2009–2015. J. Plast. Reconstr. Aesthet. Surg. 2016, 69, 149–162. [Google Scholar] [CrossRef]
- Pagliara, D.; Albanese, R.; Storti, G.; Barone-Adesi, L.; Salgarello, M. Patient-reported Outcomes in Immediate and Delayed Breast Reconstruction with Deep Inferior Epigastric Perforator Flap. Plast. Reconstr. Surg. Glob. Open 2018, 6, e1666. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| DIEA Branching | |
| Branching pattern | Type 0-IV according to Moon and Taylor classification (modified by Rozen et al.) |
| Branching pattern point | Localization on the x- and y-axis |
| Perforator | Sorted by diameter |
| Diameter | At the exit of the rectus sheath |
| Entrance of the perforator into the DIEA branch | Localization on the x- and y-axis |
| Medial/lateral | |
| Intramuscular course | Short (<1.5 cm), long (>1.5 cm), no intramuscular course (medially around the rectus muscle) |
| Exit of the rectus sheath | Localization on the x- and y-axis |
| SIEV | Direct connection, indirect connection, no connection to upper fat compartment |
| Subcutaneous fat | Thickness 3 cm to the right and left of the umbilicus |
| General information |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frank, K.; Ströbel, A.; Ludolph, I.; Hauck, T.; May, M.S.; Beier, J.P.; Horch, R.E.; Arkudas, A. Improving the Safety of DIEP Flap Transplantation: Detailed Perforator Anatomy Study Using Preoperative CTA. J. Pers. Med. 2022, 12, 701. https://doi.org/10.3390/jpm12050701
Frank K, Ströbel A, Ludolph I, Hauck T, May MS, Beier JP, Horch RE, Arkudas A. Improving the Safety of DIEP Flap Transplantation: Detailed Perforator Anatomy Study Using Preoperative CTA. Journal of Personalized Medicine. 2022; 12(5):701. https://doi.org/10.3390/jpm12050701
Chicago/Turabian StyleFrank, Katharina, Armin Ströbel, Ingo Ludolph, Theresa Hauck, Matthias S. May, Justus P. Beier, Raymund E. Horch, and Andreas Arkudas. 2022. "Improving the Safety of DIEP Flap Transplantation: Detailed Perforator Anatomy Study Using Preoperative CTA" Journal of Personalized Medicine 12, no. 5: 701. https://doi.org/10.3390/jpm12050701
APA StyleFrank, K., Ströbel, A., Ludolph, I., Hauck, T., May, M. S., Beier, J. P., Horch, R. E., & Arkudas, A. (2022). Improving the Safety of DIEP Flap Transplantation: Detailed Perforator Anatomy Study Using Preoperative CTA. Journal of Personalized Medicine, 12(5), 701. https://doi.org/10.3390/jpm12050701