
Adaptive Radiotherapy in Head and Neck Cancer Using Volumetric Modulated Arc Therapy



Abstract
:1. Introduction
2. Patients and Methods
2.1. Patient Characteristics
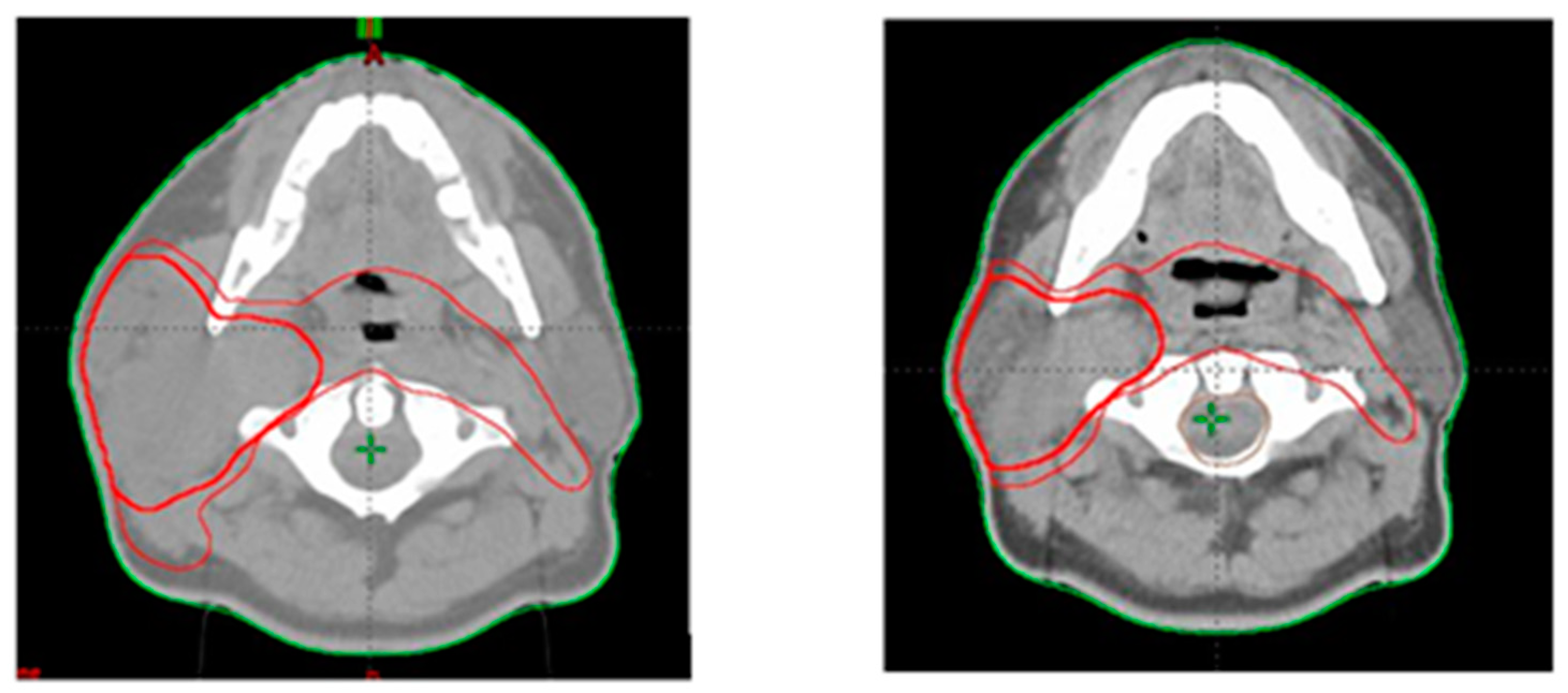
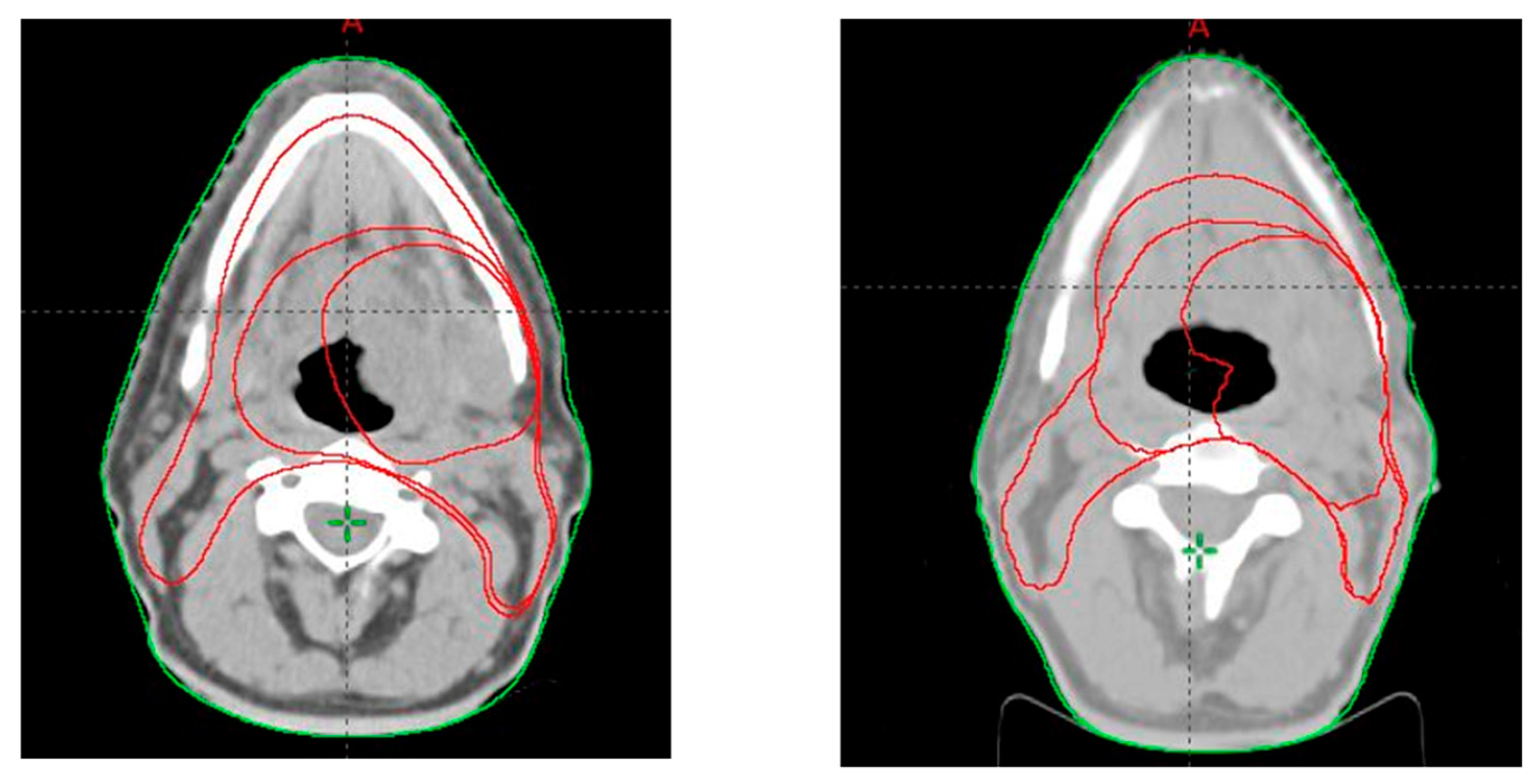
2.2. Target Volume Delineation
2.3. Treatment Planning
2.4. Statistical Analysis
3. Results
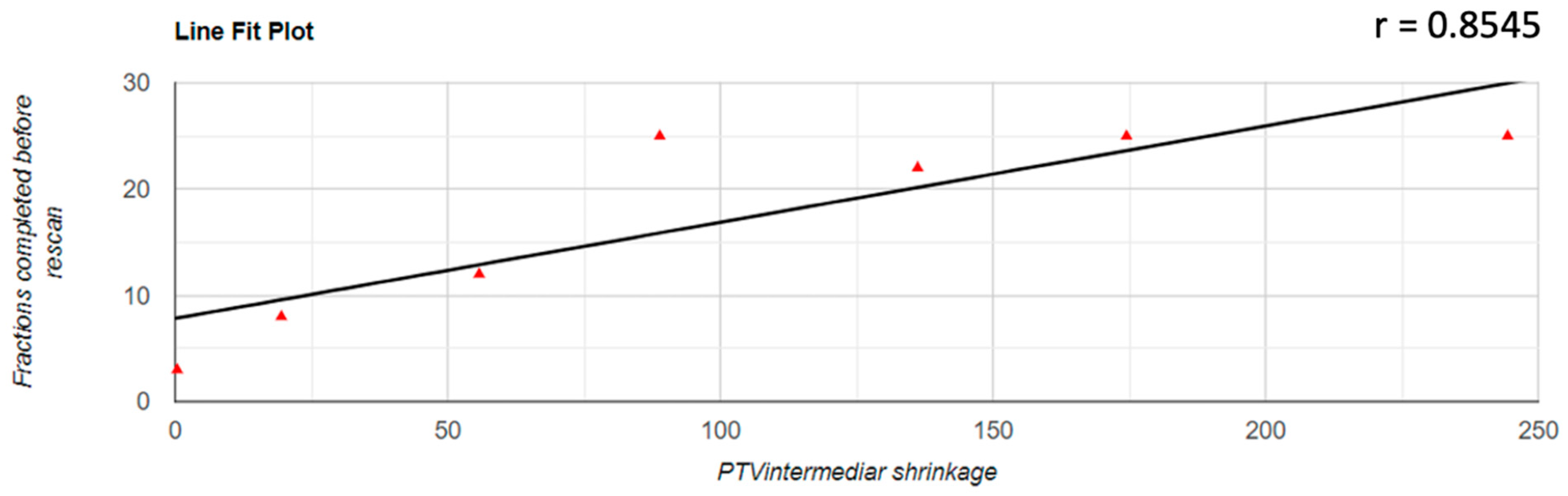
3.1. PTV Shrinkage
3.2. Parotid Glands Shrinkage
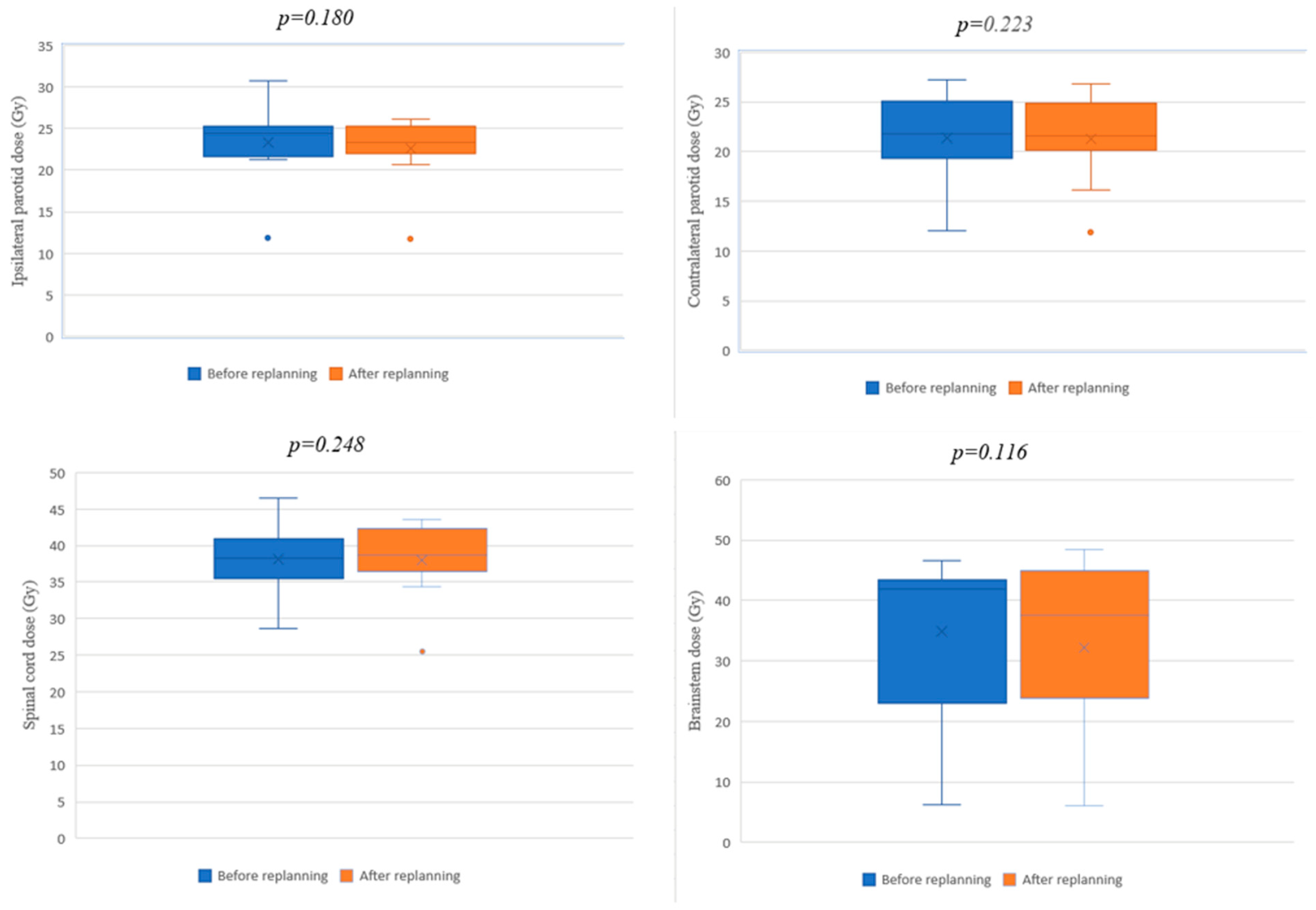
3.3. Dosimetry of Organs at Risk
3.4. Acute Toxicities
4. Discussions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Ghosh, A.; Gupta, S.; Johny, D.; Bhosale, V.V.; Negi, M.P.S. A Study to Assess the Dosimetric Impact of the Anatomical Changes Occurring in the Parotid Glands and Tumour Volume during Intensity Modulated Radiotherapy using Simultaneous Integrated Boost (IMRT-SIB) in Head and Neck Squamous Cell Cancers. Cancer Med. 2021, 10, 5175–5190. [Google Scholar] [CrossRef] [PubMed]
- Ho, K.F.; Marchant, T.; Moore, C.; Webster, G.; Rowbottom, C.; Penington, H.; Lee, L.; Yap, B.; Sykes, A.; Slevin, N. Monitoring dosimetric impact of weight loss with kilovoltage (KV) cone beam CT (CBCT) during parotid-sparing IMRT and concurrent chemotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, e375–e382. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, V.; Patel, P.; Gurjar, O.P.; Gupta, K.L. Impact of repeat computerized tomography replans in the radiation therapy of head and neck cancers. J. Med. Phys. 2014, 39, 164–168. [Google Scholar] [CrossRef] [PubMed]
- Burela, N.; Soni, T.P.; Patni, N.; Natarajan, T. Adaptive intensity-modulated radiotherapy in head-and-neck cancer: A volumetric and dosimetric study. J. Cancer Res. Ther. 2019, 15, 533–538. [Google Scholar] [CrossRef] [PubMed]
- Bhide, S.A.; Davies, M.; Burke, K.; McNair, H.A. Weekly volume and dosimetric changes during chemoradiotherapy with intensity-modulated radiation therapy for head and neck cancer: A prospective observational study. Int. J. Radiat. Oncol. Biol. Phys. 2010, 6, 1360–1368. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.; Langen, K.M.; Lu, W.; Haimerl, J.; Schnarr, E.; Ruchala, K.J.; Olivera, G.H.; Meeks, S.L.; Kupelian, P.A.; Shellenberger, T.D.; et al. Assessment of parotid gland dose changes during head and neck cancer radiotherapy using daily megavoltage computed tomography and deformable image registration. Int. J. Radiat. Oncol. Biol. Phys. 2008, 71, 1563–1571. [Google Scholar] [CrossRef]
- Sanguineti, G.; Ricchetti, F.; Wu, B.; McNutt, T.; Fiorino, C. Parotid gland shrinkage during IMRT predicts the time to Xerostomia resolution. Radiat. Oncol. 2015, 10, 19. [Google Scholar] [CrossRef] [Green Version]
- Beyzadeoglu, M.; Ozyigit, G.; Selek, U. (Eds.) Radiation Therapy for Head and Neck Cancers: A Case-Based Review; Springer International Publishing: Berlin/Heidelberg, Germany, 2015. [Google Scholar]
- Castelli, J.; Simon, A.; Lafond, C.; Perichon, N.; Rigaud, B.; Chajon, E.; De Bari, B.; Ozsahin, M.; Bourhis, J.; De Crevoisier, R. Adaptive radiotherapy for head and neck cancer. Acta Oncol. 2018, 57, 1284–1292. [Google Scholar] [CrossRef] [Green Version]
- Chen, A.M.; Yu, Y.; Daly, M.E.; Farwell, D.G.; Benedict, S.H.; Purdy, J.A. Long-term experience with reduced planning target volume margins and intensity-modulated radiotherapy with daily image-guidance for head and neck cancer. Head Neck 2014, 36, 1766–1772. [Google Scholar] [CrossRef]
- Stauch, Z.; Zoller, W.; Tedrick, K.; Walston, S.; Christ, D.; Hunzeker, A.; Lenards, N.; Culp, L.; Gamez, M.E.; Blakaj, D. An evaluation of adaptive planning by assessing the dosimetric impact of weight loss throughout the course of radiotherapy in bilateral treatment of head and neck cancer patients. Med. Dosim. 2020, 45, 52–59. [Google Scholar] [CrossRef]
- Thomson, D.J.; Beasley, W.J.; Garcez, K.; Lee, L.W.; Sykes, A.J.; Rowbottom, C.G.; Slevin, N.J. Relative plan robustness of step-and-shoot vs rotational intensity–modulated radiotherapy on repeat computed tomographic simulation for weight loss in head and neck cancer. Med. Dosim. 2016, 41, 154–158. [Google Scholar] [CrossRef] [PubMed]
- Barker, J.L., Jr.; Garden, A.S.; Kian Ang, K.; O’Daniel, J.C.; Wang, H.; Court, L.E.; Morrison, W.H.; Rosenthal, D.I.; Chao, K.S.C.; Tucker, S.L.; et al. Quantification of volumetric and geometric changes occurring during fractionated radiotherapy for head-and-neck cancer using an integrated CT/linear accelerator system. Int. J. Radiat. Oncol. Biol. Phys. 2004, 59, 960–970. [Google Scholar] [CrossRef] [PubMed]
- Jensen, A.D.; Nill, S.; Huber, P.E.; Bendl, R.; Debus, J.; Münter, M.W. A Clinical Concept for Interfractional Adaptive Radiation Therapy in the Treatment of Head and Neck Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 590–596. [Google Scholar] [CrossRef] [PubMed]
- Hansen, E.K.; Bucci, M.K.; Quivey, J.M.; Weinberg, V.; Xia, P. Repeat CT imaging and replanning during the course of IMRT for head-and-neck cancer. Int. J. Radiat. Oncol. Biol. Phys. 2006, 64, 355–362. [Google Scholar] [CrossRef]
- Zhao, L.; Wan, Q.; Zhou, Y.; Deng, X.; Xie, C.; Wu, S. The role of replanning in fractionated intensity modulated radiotherapy for nasopharyngeal carcinoma. Radiother. Oncol. 2011, 98, 23–27. [Google Scholar] [CrossRef]
- Castelli, J.; Simon, A.; Louvel, G.; Henry, O.; Chajon, E.; Nassef, M.; Haigron, P.; Cazoulat, G.; Ospina, J.D.; Jegoux, F.; et al. Impact of head and neck cancer adaptive radiotherapy to spare the parotid glands and decrease the risk of xerostomia. Radiat. Oncol. 2015, 10, 6. [Google Scholar] [CrossRef]
- Robar, J.L.; Day, A.; Clancey, J.; Kelly, R.; Yewondwossen, M.; Hollenhorst, H.; Rajaraman, M.; Rajaraman, M.; Wilke, D. Spatial and dosimetric variability of organs at risk in head-and-neck intensity-modulated radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2007, 68, 1121–1130. [Google Scholar] [CrossRef]
- van Timmeren, J.E.; Chamberlain, M.; Bogowicz, M.; Ehrbar, S.; Dal Bello, R.; Schüler, H.G.; Krayenbuehl, J.; Wilke, L.; Andratschke, N.; Guckenberger, M.; et al. MR-Guided Adaptive Radiotherapy for Head and Neck Cancer: Prospective Evaluation of Migration and Anatomical Changes of the Major Salivary Glands. Cancers 2021, 13, 5404. [Google Scholar] [CrossRef]
- Castadot, P.; Lee, J.A.; Geets, X.; Grégoire, V. Adaptive radiotherapy of head and neck cancer. Semin. Radiat. Oncol. 2010, 20, 84–93. [Google Scholar] [CrossRef]
- Vásquez Osorio, E.M.; Hoogeman, M.S.; Al-Mamgani, A.; Teguh, D.N.; Levendag, P.C.; Heijmen, B.J. Local anatomic changes in parotid and submandibular glands during radiotherapy for oropharynx cancer and correlation with dose, studied in detail with nonrigid registration. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 875–882. [Google Scholar] [CrossRef]
- Soisson, E.; Guerrieri, P.; Balasubramanian, S.; Ahamad, A.; Moran, J.M.; Joiner, M.C.; Dominello, M.; Burmeister, J. Three discipline collaborative radiation therapy special debate: All head and neck cancer patients with intact tumors/nodes should have scheduled adaptive replanning performed at least once during the course of radiotherapy. J. Appl. Clin. Med. Phys. 2019, 20, 7–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwartz, D.L.; Garden, A.S.; Thomas, J.; Chen, Y.; Zhang, Y.; Lewin, J.; Chambers, M.S.; Dong, L. Adaptive radiotherapy for head-and-neck cancer: Initial clinical outcomes from a prospective trial. Int. J. Radiat. Oncol. Biol. Phys. 2011, 83, 986–993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maheshwari, G.; Dhanawat, A.; Kumar, H.S.; Sharma, N.; Jakhar, S.L. Clinical and dosimetric impact of adaptive intensity-modulated radiotherapy in locally advanced head-and-neck cancer. J. Cancer Res. Ther. 2020, 16, 600–604. [Google Scholar] [PubMed]
- Zhang, Y.; Plautz, T.E.; Hao, Y.; Kinchen, C.; Li, X.A. Texture-based, automatic contour validation for online adaptive replanning: A feasibility study on abdominal organs. Med. Phys. 2019, 46, 4010–4020. [Google Scholar] [CrossRef] [PubMed]
- Gensheimer, M.F.; Le, Q.T. Adaptive radiotherapy for head and neck cancer: Are we ready to put it into routine clinical practice? Oral Oncol. 2018, 86, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Cuccia, F.; Figlia, V.; Palmeri, A.; Verderame, F.; Casto, A.L.; Mannino, M.; Ferrera, G. Helical Tomotherapy® is a Safe and Feasible Technique for Total Scalp Irradiation. Rare Tumors 2017, 9, 6942. [Google Scholar] [CrossRef]
- Nicosia, L.; Sicignano, G.; Rigo, M.; Figlia, V.; Cuccia, F.; De Simone, A.; Giaj-Levra, N.; Mazzola, R.; Naccarato, S.; Ricchetti, F.; et al. Daily dosimetric variation between image-guided volumetric modulated arc radiotherapy and MR-guided daily adaptive radio-therapy for prostate cancer stereotactic body radiotherapy. Acta Oncol. 2021, 60, 215–221. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex | Age (Years) | Tumor Location | Staging | Concomitant Chemotherapy |
|---|---|---|---|---|
| M | 57 | Pyriform sinus | T4N2bM0 | Yes |
| M | 68 | Larynx | T2N2M0 | Yes |
| M | 48 | Rhinopharynx | TxN3M0 | Yes |
| M | 50 | Rhinopharynx | T2N3M0 | Yes |
| M | 33 | Nasopharynx | T3N2M0 | No |
| F | 68 | Rhinopharynx | T4cN2M0 | No |
| F | 55 | Rhinopharynx | T2N2M0 | Yes |
| F | 62 | Tongue | T3N3M0 | Yes |
| M | 52 | Rhinopharynx | T3N2M0 | No |
| M | 50 | Rhinopharynx | T2N0M0 | Yes |
| M | 76 | Hypopharynx | T2N2M0 | Yes |
| M | 65 | Hypopharynx | T4N3M0 | No |
| M | 47 | Rhinopharynx | T2N1M0 | Yes |
| Organ | Dose-Volume Index | Objective |
|---|---|---|
| PTV | D95% | V95% |
| Dmax | <108% | |
| Parotid glands (single) | Dmean | <26 Gy |
| V50% | <30 Gy | |
| Spinal cord | Dmax | <45 Gy |
| Brainstem | Dmax | <54 Gy |
| PTV Low (cm3) | PTV Intermediate (cm3) | PTV High (cm3) | Fractions Completed before Rescanning | |||
|---|---|---|---|---|---|---|
| Initial | Replanning | Initial | Replanning | Initial | Replanning | |
| 587.9 | 574 | - | - | 72.1 | 71.8 | 8 |
| 577.9 | 571.8 | 360.2 | 340.7 | 204 | 183.3 | 8 |
| 1032.8 | 828.9 | - | - | 317.6 | 220.5 | 21 |
| 1028.8 | 898.7 | 896 | 759.8 | 300 | 187.5 | 22 |
| 881.9 | 719.2 | - | - | 229.1 | 193.5 | 19 |
| 871.2 | 757.3 | - | - | 489.2 | 397.8 | 9 |
| 764.4 | 764.4 | 342.2 | 253.3 | 159.8 | 93.5 | 25 |
| 586.4 | 527.6 | 236.8 | 181 | 50.7 | 34.3 | 12 |
| 1058.9 | 1058.9 | 711.4 | 467 | 80 | 77.5 | 25 |
| 726.4 | 701.5 | - | - | 171 | 170 | 13 |
| 479.8 | 480.3 | 164.6 | 164.2 | 34.3 | 34.1 | 3 |
| 634.6 | 595 | - | - | 231.9 | 184.7 | 17 |
| 904.4 | 664 | 390 | 215.5 | 165 | 43.8 | 25 |
| Mean Value | ||||||
| 779.646 | 703.2 | 443.028 | 340.214 | 192.669 | 145.562 | |
| p Value | ||||||
| 0.007 | 0.021 | 0.003 | ||||
| Ipsilateral Parotid (cm3) | Ipsilateral Parotid (Replanning) (cm3) | Contralateral Parotid (cm3) | Contralateral Parotid (Replanning) (cm3) |
|---|---|---|---|
| 32 | 32.7 | 25.3 | 28.9 |
| 19.5 | 18.8 | 14.6 | 14.5 |
| - | - | 43.1 | 26.8 |
| 30.7 | 31.9 | 26.1 | 25.5 |
| 26.1 | 18.7 | 23.1 | 18.3 |
| - | - | 17.6 | 24.6 |
| 36.8 | 33.4 | 33.4 | 24 |
| 10 | 16.5 | 18.9 | 12.3 |
| 35.5 | 22.2 | 34.2 | 14.5 |
| 18.2 | 18 | 18.3 | 17.6 |
| 26 | 27.2 | 29.2 | 28.7 |
| 18.7 | 13.8 | 12.5 | 12.5 |
| 32.3 | 18.4 | 27.8 | 20.9 |
| Mean Value | |||
| 25.98 | 22.23 | 24.93 | 20.7 |
| p Value | |||
| 0.067 | 0.033 | ||
| Ipsilateral Parotid (Gy) | Ipsilateral Parotid Replan (Gy) | Contralateral Parotid (Gy) | Contralateral Parotid Replan (Gy) | Spinal Cord (Gy) | Spinal Cord Replan (Gy) | Brainstem (Gy) | Brainstem Replan (Gy) |
|---|---|---|---|---|---|---|---|
| 11.826 | 11.719 | 12.03 | 11.912 | 28.597 | 25.508 | 11.34 | 12.178 |
| 21.599 | 20.61 | 16.285 | 16.144 | 34.380 | 34.301 | 6.284 | 6.149 |
| - | - | 20.907 | 21.297 | 40.905 | 42.26 | 42.974 | 46.24 |
| 22.169 | 23.33 | 19.273 | 20.658 | 40.042 | 40.873 | 44.675 | 48.464 |
| 25.327 | 25.558 | 25.058 | 24.869 | 42.072 | 42.881 | 43.4 | 44.91 |
| - | - | 23.373 | 23.476 | 36.936 | 38.685 | 23.007 | 23.908 |
| 24.449 | 22.862 | 20.663 | 20.127 | 38.33 | 36.427 | 42.685 | 25.035 |
| 21.224 | 23.337 | 21.808 | 21.577 | 38.496 | 37.518 | 41.847 | 24.242 |
| 24.714 | 26.09 | 25.066 | 26.791 | 37.506 | 37.486 | 41.345 | 40.916 |
| 27.419 | 25.239 | 27.222 | 24.991 | 46.546 | 43.62 | 46.641 | 44.17 |
| 25.061 | 24.282 | 23.44 | 22.621 | 35.491 | 38.641 | 40.03 | 37.63 |
| 21.958 | 21.946 | 21.140 | 22.084 | 35.851 | 36.217 | 31.922 | 30.953 |
| 30.687 | 23.632 | 18.935 | 13.486 | 42.210 | 37.26 | 55.44 | 55.133 |
| Mean Value | |||||||
| 23.312 | 22.600 | 21.169 | 20.771 | 38.258 | 37.821 | 36.276 | 33.840 |
| p Value | |||||||
| 0.180 | 0.223 | 0.248 | 0.116 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buciuman, N.; Marcu, L.G. Adaptive Radiotherapy in Head and Neck Cancer Using Volumetric Modulated Arc Therapy. J. Pers. Med. 2022, 12, 668. https://doi.org/10.3390/jpm12050668
Buciuman N, Marcu LG. Adaptive Radiotherapy in Head and Neck Cancer Using Volumetric Modulated Arc Therapy. Journal of Personalized Medicine. 2022; 12(5):668. https://doi.org/10.3390/jpm12050668
Chicago/Turabian StyleBuciuman, Nikolett, and Loredana G. Marcu. 2022. "Adaptive Radiotherapy in Head and Neck Cancer Using Volumetric Modulated Arc Therapy" Journal of Personalized Medicine 12, no. 5: 668. https://doi.org/10.3390/jpm12050668
APA StyleBuciuman, N., & Marcu, L. G. (2022). Adaptive Radiotherapy in Head and Neck Cancer Using Volumetric Modulated Arc Therapy. Journal of Personalized Medicine, 12(5), 668. https://doi.org/10.3390/jpm12050668