
An Item Response Theory Analysis of the Wisconsin Card Sorting Test in Normal Aging, Alzheimer’s Disease and Parkinson’s Disease: Neurophysiological Approach


 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics
2.2. Study Population and Clinical Characteristics
2.3. Instruments
2.4. Data Analysis
- Pi(θ) is probability of hitting an item for a value of θ;
- Bi is difficulty index of item i.
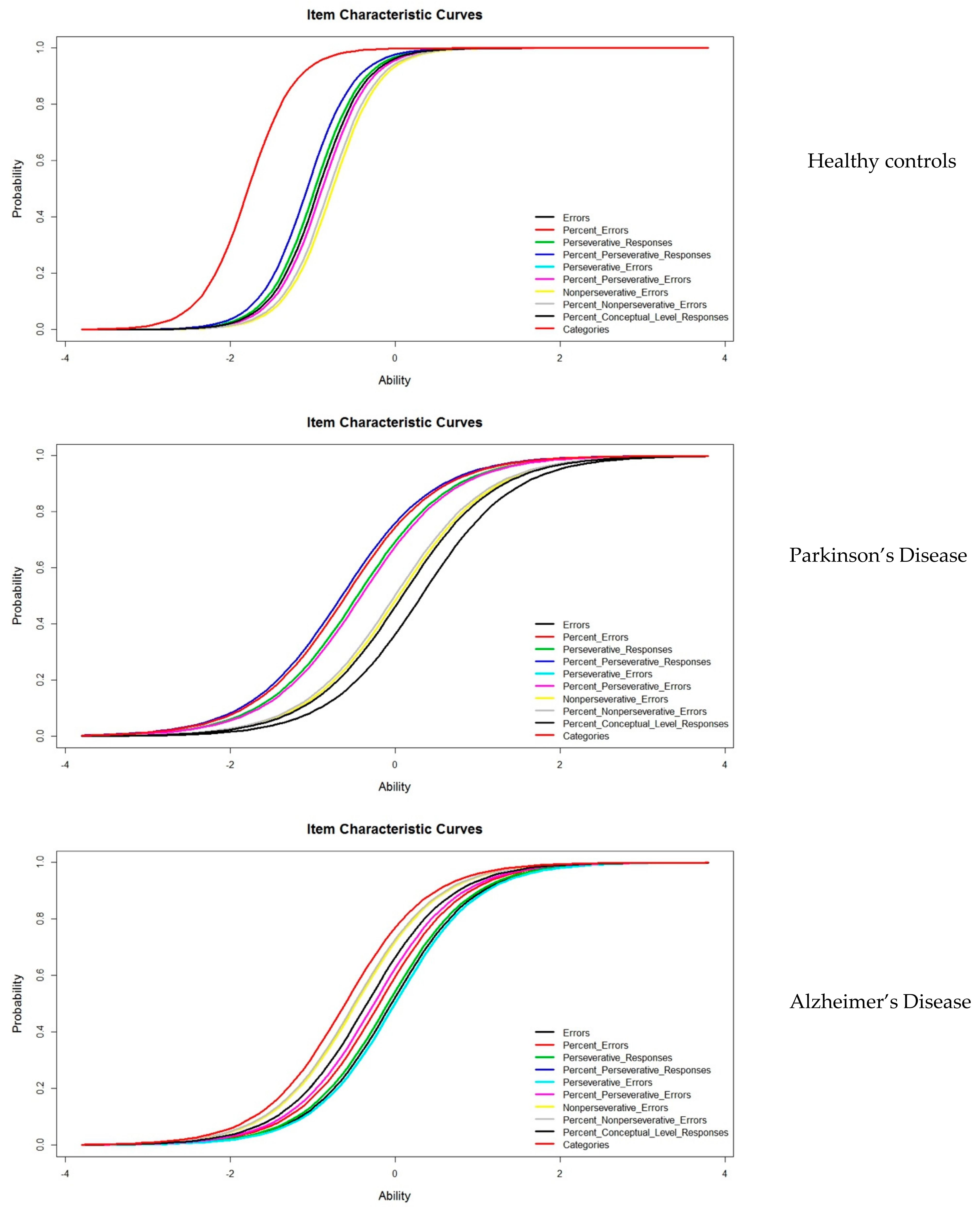
3. Results
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Elliott, R. Executive functions and their disorders. Br. Med. Bull. 2003, 65, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Cristofori, I.; Zimmerman, S.; Grafman, J. Executive Functions. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2019; pp. 197–219. [Google Scholar]
- Spaniol, M.; Danielsson, H. A meta-analysis of the executive function components inhibition, shifting, and attention in intellectual disabilities. J. Intellect. Disabil. Res. 2021, 66, 9–31. [Google Scholar] [CrossRef] [PubMed]
- Hildebrandt, S. Executive Functions. In Neuropsychology for Occupational Therapists: Cognition in Occupational Performance; Wiley: Hoboken, NJ, USA, 2017; pp. 165–176. [Google Scholar] [CrossRef]
- Zink, N.; Lenartowicz, A.; Markett, S. A new era for executive function research: On the transition from centralized to distributed executive functioning. Neurosci. Biobehav. Rev. 2021, 124, 235–244. [Google Scholar] [CrossRef] [PubMed]
- Ishihara, T.; Drollette, E.S.; Ludyga, S.; Hillman, C.H.; Kamijo, K. The effects of acute aerobic exercise on executive function: A systematic review and meta-analysis of individual participant data. Neurosci. Biobehav. Rev. 2021, 128, 258–269. [Google Scholar] [CrossRef] [PubMed]
- Blair, C. Developmental Science and Executive Function. Curr. Dir. Psychol. Sci. 2016, 25, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Hamasaki, A.; Akazawa, N.; Yoshikawa, T.; Myoenzono, K.; Tagawa, K.; Maeda, S. Age-Related Declines in Executive Function and Cerebral Oxygenation Hemodynamics. Tohoku J. Exp. Med. 2018, 245, 245–250. [Google Scholar] [CrossRef] [Green Version]
- Jaul, E.; Barron, J. Age-Related Diseases and Clinical and Public Health Implications for the 85 Years Old and Over Population. Front. Public Health 2017, 5, 335. [Google Scholar] [CrossRef] [Green Version]
- Bettio, L.; Rajendran, L.; Gil-Mohapel, J. The effects of aging in the hippocampus and cognitive decline. Neurosci. Biobehav. Rev. 2017, 79, 66–86. [Google Scholar] [CrossRef]
- Klimova, B.; Valis, M.; Kuca, K. Cognitive decline in normal aging and its prevention. Clin. Interv. Aging 2017, 2017, 903–910. [Google Scholar] [CrossRef] [Green Version]
- Roheger, M.; Kalbe, E.; Liepelt-Scarfone, I. Progression of Cognitive Decline in Parkinson’s Disease. J. Park. Dis. 2018, 8, 183–193. [Google Scholar] [CrossRef] [Green Version]
- Lange, F.; Brückner, C.; Knebel, A.; Seer, C.; Kopp, B. Executive dysfunction in Parkinson’s disease: A meta-analysis on the Wisconsin Card Sorting Test literature. Neurosci. Biobehav. Rev. 2018, 93, 38–56. [Google Scholar] [CrossRef] [PubMed]
- Aarsland, D.; Creese, B.; Politis, M.; Chaudhuri, K.R.; Ffytche, D.H.; Weintraub, D.; Ballard, C. Cognitive decline in Parkinson disease. Nat. Rev. Neurol. 2017, 13, 217–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rouch, I.; Padovan, C.; Boublay, N.; Pongan, E.; Laurent, B.; Trombert-Paviot, B.; Krolak-Salmon, P.; Dorey, J. Association between executive function and the evolution of behavioral disorders in Alzheimer’s disease. Int. J. Geriatr. Psychiatry 2020, 35, 1043–1050. [Google Scholar] [CrossRef] [PubMed]
- Michalon, S.; Serveaux, J.-P.; Allain, P. Frontal functions and activities of daily living in Alzheimer’s disease. Gériatrie Psychol. Neuropsychiatr. Viellissement 2018, 16, 321–328. [Google Scholar] [CrossRef] [PubMed]
- Butha, A.M. HHS Public Access. Physiol. Behav. 2017, 176, 139–148. [Google Scholar]
- Kirova, A.-M.; Bays, R.B.; Lagalwar, S. Working Memory and Executive Function Decline across Normal Aging, Mild Cognitive Impairment, and Alzheimer’s Disease. BioMed Res. Int. 2015, 2015, 748212. [Google Scholar] [CrossRef] [Green Version]
- Grant, D.; Berg, E. A behavioral analysis of degree of reinforcement and ease of shifting to new responses in a Weigel-type card-sorting problem. J. Exp. Psychol. 1948, 34, 404–411. [Google Scholar] [CrossRef]
- Berg, E.A. A Simple Objective Technique for Measuring Flexibility in Thinking. J. Gen. Psychol. 1948, 39, 15–22. [Google Scholar] [CrossRef]
- Chiu, E.-C.; Lee, S.-C. Test-retest reliability of the Wisconsin Card Sorting Test in people with schizophrenia. Disabil. Rehabil. 2021, 43, 996–1000. [Google Scholar] [CrossRef]
- Axelrod, B.N.; Goldman, R.S.; Woodard, J.L. Interrater reliability in scoring the Wisconsin card sorting test. Clin. Neuropsychol. 1992, 6, 143–155. [Google Scholar] [CrossRef]
- Kopp, B.; Lange, F.; Steinke, A. The Reliability of the Wisconsin Card Sorting Test in Clinical Practice. Assessment 2021, 28, 248–263. [Google Scholar] [CrossRef] [PubMed]
- Muñiz, J. Las Teoría de los Tests: TCT y TRI. Pap. Psicólogo 2010, 31, 57–66. Available online: http://www.papelesdelpsicologo.es/pdf/1796.pdf (accessed on 12 December 2021).
- Rasch, G. Studies in Mathematical Psychology: I. Probabilistic Models for Some Intelligence and Attainment Tests; Copenhagen Danmarks pædagogiske Institut V. 44; Copenhagen Danmarks pædagogiske Institut: København, Denmark, 1960. [Google Scholar]
- Muñiz, J. Introducción a la Teoría de Respuesta a los Ítems; Piramide: Madrid, Spain, 1997. [Google Scholar]
- Lobo, A.; Escobar, V.; Ezquerra, J.; Seva Díaz, A. “El Mini Examen Cognoscitivo” (Un test sencillo y práctico para detectar alteraciones intelectuales en pacientes médicos). Revista de Psiquiatria Y Psicologia Medica 1980, 14, 39–57. [Google Scholar]
- Postuma, R.B.; Berg, D.; Stern, M.; Poewe, W.; Olanow, C.W.; Oertel, W.; Obeso, J.; Marek, K.; Litvan, I.; Lang, A.E.; et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov. Disord. 2015, 30, 1591–1601. [Google Scholar] [CrossRef]
- Hoehn, M.M.; Yahr, M.D. Parkinsonism: Onset, progression, and mortality. Neurology 1967, 50, 318. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Publishing: Arlington, TA, USA, 2013. [Google Scholar]
- Boada, M.; Berthier, M.; Martinez, M. Evidencia Científica en Enfermedad de Alzheimer. In Manual de Actuación; International Marketing and Comunication: Madrid, Spain, 2008. [Google Scholar]
- Oldfield, R.C. The assessment and analysis of handedness: The Edinburgh inventory. Neuropsychologia 1971, 9, 97–113. [Google Scholar] [CrossRef]
- Heaton, R.; Chelune, G.; Talley, J.; Kay, G.; Curtiss, G. Wisconsin Card Sorting Test Manual: Revised and Expanded; Psychological Assessment Resources Inc.: Odessa, FL, USA, 1993. [Google Scholar]
- Kopp, B.; Maldonado, N.; Scheffels, J.F.; Hendel, M.; Lange, F. A Meta-Analysis of Relationships between Measures of Wisconsin Card Sorting and Intelligence. Brain Sci. 2019, 9, 349. [Google Scholar] [CrossRef] [Green Version]
- Reise, S.P.; Henson, J.M. A Discussion of Modern Versus Traditional Psychometrics as Applied to Personality Assessment Scales. J. Pers. Assess. 2003, 81, 93–103. [Google Scholar] [CrossRef]
- Prieto, G.; Delgado, A.R.; Perea, M.V.; Ladera, V. Scoring Neuropsychological Tests Using the Rasch Model: An Illustrative Example with the Rey-Osterrieth Complex Figure. Clin. Neuropsychol. 2010, 24, 45–56. [Google Scholar] [CrossRef]
- Ashendorf, L.; McCaffrey, R.J. Exploring Age-Related Decline on the Wisconsin Card Sorting Test. Clin. Neuropsychol. 2008, 22, 262–272. [Google Scholar] [CrossRef]
- Hartman, M.; Bolton, E.; Fehnel, S.E. Accounting for age differences on the Wisconsin Card Sorting Test: Decreased working memory, not inflexibility. Psychol. Aging 2001, 16, 385–399. [Google Scholar] [CrossRef] [PubMed]
- Head, D.; Kennedy, K.; Rodrigue, K.; Raz, N. Age differences in perseveration: Cognitive and neuroanatomical mediators of performance on the Wisconsin Card Sorting Test. Neuropsychologia 2009, 47, 1200–1203. [Google Scholar] [CrossRef] [Green Version]
- García, E.; Fidalgo, A. Análisis de los Ítems; Muralla, L., Ed.; Centro Virtual Cervantes: Madrid, Spain, 2009. [Google Scholar]
- Asún, R.; Zúñiga, C. Ventajas de los modelos politómicos de teoría de respuesta al ítem en la medición de actitudes sociales. Psykhe 2008, 17, 103–115. [Google Scholar] [CrossRef] [Green Version]
- Hambleton, R.K.; Swaminathan, H.; Rogers, H.J. Fundamentals of Item Response Theory, 1st ed.; Sage: Beverly Hills, CA, USA, 1991. [Google Scholar]
- Tanner, J.A.; Rabinovici, G.D. Relationship Between Tau and Cognition in the Evolution of Alzheimer’s Disease: New Insights from Tau PET. J. Nucl. Med. 2021, 62, 612–613. [Google Scholar] [CrossRef] [PubMed]
- Sperling, R.; Mormino, E.; Johnson, K. The Evolution of Preclinical Alzheimer’s Disease: Implications for Prevention Trials. Neuron 2014, 84, 608–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alexoudi, A.; Gatzonis, S. Parkinson’s disease pathogenesis, evolution and alternative pathways: A review. Rev. Neurol. 2018, 174, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Embretson, S.; Reise, S. Item Response Theory for Psychologist; LEA: Mahwah, NJ, USA, 2000. [Google Scholar]
- Mungas, D.; Reed, B.R. Application of item response theory for development of a global functioning measure of dementia with linear measurement properties. Stat. Med. 2000, 19, 1631–1644. [Google Scholar] [CrossRef]

{kind=link}
| Control (n = 86) | PD (n = 77) | AD (n = 155) | Sign. | |
|---|---|---|---|---|
| Age, years | 70.71 ± 7.54 | 71.81 ± 7.26 | 74.75 ± 7.66 | <0.0001 |
| Female gender % | 52 | 55 | 67 | n.s. |
| Education, years | 7.86 ± 3.506 | 7.31 ± 3.63 | 6.94 ± 3.19 | n.s. |
| MMSE | 33.45 ± 1.46 | 30.72 ± 4.29 | 26.16 ± 5.59 | <0.0001 |
| Healthy Controls | Parkinson’s Disease | Alzheimer’s Disease | ||||
|---|---|---|---|---|---|---|
| Difficulty | Std Error | Difficulty | Std Error | Difficulty | Std Error | |
| Errors | −0.9733 | 0.1380 | 0.3179 | 1.5232 | −0.0441 | 0.1353 |
| % Errors | −1.0681 | 0.1435 | −0.0044 | −0.0215 | −0.1934 | 0.1354 |
| Perseverative Responses | −0.9732 | 0.1380 | −0.4579 | −2.2028 | −0.0868 | 0.1352 |
| % Perseverative Responses | −1.0681 | 0.1435 | −0.6481 | −3.0218 | −0.3431 | 0.1368 |
| Perseverative Errors | −0.8840 | 0.1336 | −0.4116 | −1.9914 | −0.0014 | 0.1355 |
| % Perseverative Errors | −0.8839 | 0.1336 | −0.4116 | −1.9914 | −0.2570 | 0.1358 |
| Nonperseverative Errors | −0.7583 | 0.1293 | 0.0409 | 0.2007 | −0.4735 | 0.1390 |
| % Nonperseverative Errors | −0.7992 | 0.1304 | −0.0044 | −0.0214 | −0.4955 | 0.1395 |
| % Conceptual Level Responses | −0.9279 | 0.1357 | 0.0863 | 0.4228 | −0.3432 | 0.1368 |
| Categories | −1.7806 | 0.2394 | −0.5996 | −2.8216 | −0.6075 | 0.1424 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Rodríguez, J.L.; Juárez-Vela, R.; Santolalla-Arnedo, I.; Ruiz de Viñaspre-Hernandez, R.; Sánchez-González, J.L. An Item Response Theory Analysis of the Wisconsin Card Sorting Test in Normal Aging, Alzheimer’s Disease and Parkinson’s Disease: Neurophysiological Approach. J. Pers. Med. 2022, 12, 539. https://doi.org/10.3390/jpm12040539
Sánchez-Rodríguez JL, Juárez-Vela R, Santolalla-Arnedo I, Ruiz de Viñaspre-Hernandez R, Sánchez-González JL. An Item Response Theory Analysis of the Wisconsin Card Sorting Test in Normal Aging, Alzheimer’s Disease and Parkinson’s Disease: Neurophysiological Approach. Journal of Personalized Medicine. 2022; 12(4):539. https://doi.org/10.3390/jpm12040539
Chicago/Turabian StyleSánchez-Rodríguez, Juan Luis, Raúl Juárez-Vela, Iván Santolalla-Arnedo, Regina Ruiz de Viñaspre-Hernandez, and Juan Luis Sánchez-González. 2022. "An Item Response Theory Analysis of the Wisconsin Card Sorting Test in Normal Aging, Alzheimer’s Disease and Parkinson’s Disease: Neurophysiological Approach" Journal of Personalized Medicine 12, no. 4: 539. https://doi.org/10.3390/jpm12040539
APA StyleSánchez-Rodríguez, J. L., Juárez-Vela, R., Santolalla-Arnedo, I., Ruiz de Viñaspre-Hernandez, R., & Sánchez-González, J. L. (2022). An Item Response Theory Analysis of the Wisconsin Card Sorting Test in Normal Aging, Alzheimer’s Disease and Parkinson’s Disease: Neurophysiological Approach. Journal of Personalized Medicine, 12(4), 539. https://doi.org/10.3390/jpm12040539