
Effects of Artificial Extraoral Markers on Accuracy of Three-Dimensional Dentofacial Image Integration: Smartphone Face Scan versus Stereophotogrammetry



Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Pimentel, W.; Teixeira, M.L.; Costa, P.P.; Jorge, M.Z.; Tiossi, R. Predictable outcomes with porcelain laminate veneers: A clinical report. J. Prosthodont. 2016, 25, 335–340. [Google Scholar] [CrossRef]
- Charavet, C.; Bernard, J.C.; Gaillard, C.; Le Gall, M. Benefits of Digital Smile Design (DSD) in the conception of a complex orthodontic treatment plan: A case report-proof of concept. Int. Orthod. 2019, 17, 573–579. [Google Scholar] [CrossRef]
- Lin, W.-S.; Harris, B.T.; Phasuk, K.; Llop, D.R.; Morton, D. Integrating a facial scan, virtual smile design, and 3D virtual patient for treatment with CAD-CAM ceramic veneers: A clinical report. J. Prosthet. Dent. 2018, 119, 200–205. [Google Scholar] [CrossRef]
- Galibourg, A.; Brenes, C. Virtual smile design tip: From 2D to 3D design with free software. J. Prosthet. Dent. 2019, 121, 863–864. [Google Scholar] [CrossRef] [Green Version]
- Kovacs, L.; Zimmermann, A.; Brockmann, G.; Gühring, M.; Baurecht, H.; Papadopulos, N.; Schwenzer-Zimmerer, K.; Sader, R.; Biemer, E.; Zeilhofer, H. Three-dimensional recording of the human face with a 3D laser scanner. Plast. Reconstr. Aesthet. Surg. 2006, 59, 1193–1202. [Google Scholar] [CrossRef]
- Kook, M.-S.; Jung, S.; Park, H.-J.; Oh, H.-K.; Ryu, S.-Y.; Cho, J.-H.; Lee, J.-S.; Yoon, S.-J.; Kim, M.-S.; Shin, H.-K. A comparison study of different facial soft tissue analysis methods. J. Craniomaxillofac. Surg. 2014, 42, 648–656. [Google Scholar] [CrossRef]
- Li, Z.; Liang, Y.; Schenck, T.L.; Frank, K.; Giunta, R.E.; Koban, K.C. Investigating the Reliability of Novel Nasal Anthropometry Using Advanced Three-Dimensional Digital Stereophotogrammetry. J. Pers. Med. 2022, 12, 60. [Google Scholar] [CrossRef]
- Berssenbrügge, P.; Berlin, N.F.; Kebeck, G.; Runte, C.; Jung, S.; Kleinheinz, J.; Dirksen, D. 2D and 3D analysis methods of facial asymmetry in comparison. J. Craniomaxillofac. Surg. 2014, 42, e327–e334. [Google Scholar] [CrossRef]
- Gibelli, D.; Dolci, C.; Cappella, A.; Sforza, C. Reliability of optical devices for three-dimensional facial anatomy description: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2020, 49, 1092–1106. [Google Scholar] [CrossRef]
- de Menezes, M.; Rosati, R.; Ferrario, V.F.; Sforza, C. Accuracy and reproducibility of a 3-dimensional stereophotogrammetric imaging system. J. Oral Maxillofac. Surg. 2010, 68, 2129–2135. [Google Scholar] [CrossRef]
- Tzou, C.J.; Artner, N.M.; Pona, I.; Hold, A.; Placheta, E.; Kropatsch, W.G.; Frey, M. Comparison of three-dimensional surface-imaging systems. J. Craniofac. Surg. 2019, 30, 1869–1872. [Google Scholar] [CrossRef]
- Germec-Cakan, D.; Canter, H.I.; Nur, B.; Arun, T. Comparison of facial soft tissue measurements on three-dimensional images and models obtained with different methods. J. Craniofac. Surg. 2010, 21, 1393–1399. [Google Scholar] [CrossRef]
- Bakirman, T.; Gumusay, M.U.; Reis, H.C.; Selbesoglu, M.O.; Yosmaoglu, S.; Yaras, M.C.; Seker, D.Z.; Bayram, B. Comparison of low cost 3D structured light scanners for face modeling. Appl. Opt. 2017, 56, 985–992. [Google Scholar] [CrossRef]
- Gevaux, L.; Adnet, C.; Séroul, P.; Clerc, R.; Trémeau, A.; Perrot, J.L.; Hébert, M. Three-dimensional maps of human skin properties on full face with shadows using 3-D hyperspectral imaging. J. Biomed. Opt. 2019, 24, 066002. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.M.; Kim, M.S.; Lee, G.J.; Jang, H.J.; Song, Y.M. Miniaturized 3D Depth Sensing-Based Smartphone Light Field Camera. Sensors 2020, 20, 2129. [Google Scholar] [CrossRef] [Green Version]
- Jeon, B.; Jeong, B.; Jee, S.; Huang, Y.; Kim, Y.; Park, G.H.; Kim, J.; Wufuer, M.; Jin, X.; Kim, S.W. A facial recognition mobile app for patient safety and biometric identification: Design, development, and validation. JMIR mHealth uHealth 2019, 7, e11472. [Google Scholar] [CrossRef]
- Elbashti, M.E.; Sumita, Y.I.; Aswehlee, A.M.; Seelaus, R. Smartphone Application as a Low-Cost Alternative for Digitizing Facial Defects: Is It Accurate Enough for Clinical Application? Int. J. Prosthodont. 2019, 32, 541–543. [Google Scholar] [CrossRef]
- Lo Russo, L.; Salamini, A.; Troiano, G.; Guida, L. Digital dentures: A protocol based on intraoral scans. J. Prosthet. Dent. 2021, 125, 597–602. [Google Scholar] [CrossRef]
- Liu, C.-H.; Lin, I.-C.; Lu, J.-J.; Cai, D. A Smartphone App for Improving Clinical Photography in Emergency Departments: Comparative Study. JMIR mHealth uHealth 2019, 7, e14531. [Google Scholar] [CrossRef]
- Granata, S.; Giberti, L.; Vigolo, P.; Stellini, E.; Di Fiore, A. Incorporating a facial scanner into the digital workflow: A dental technique. J. Prosthet. Dent. 2019, 123, 781–785. [Google Scholar] [CrossRef]
- Revilla-León, M.; Meyer, M.J.; Barrington, J.J.; Sones, A.; Umorin, M.P.; Taleghani, M.; Zandinejad, A. Perception of occlusal plane that is nonparallel to interpupillary and commissural lines but with the maxillary dental midline ideally positioned. J. Prosthet. Dent. 2019, 122, 482–490. [Google Scholar] [CrossRef]
- Hong, S.-J.; Noh, K. Setting the sagittal condylar inclination on a virtual articulator by using a facial and intraoral scan of the protrusive interocclusal position: A dental technique. J. Prosthet. Dent. 2021, 125, 392–395. [Google Scholar] [CrossRef] [PubMed]
- Park, J.-M.; Oh, K.C.; Shim, J.-S. Integration of intraoral digital scans with a 3D facial scan for anterior tooth rehabilitation. J. Prosthet. Dent. 2019, 121, 394–397. [Google Scholar] [CrossRef] [PubMed]
- Rangel, F.A.; Maal, T.J.J.; Bergé, S.J.; van Vlijmen, O.J.C.; Plooij, J.M.; Schutyser, F.; Kuijpers-Jagtman, A.M. Integration of digital dental casts in 3-dimensional facial photographs. Am. J. Orthod. Dentofac. Orthop 2008, 134, 820–826. [Google Scholar] [CrossRef] [PubMed]
- Revilla-León, M.; Raney, L.; Piedra-Cascón, W.; Barrington, J.; Zandinejad, A.; Özcan, M. Digital workflow for an esthetic rehabilitation using a facial and intraoral scanner and an additive manufactured silicone index: A dental technique. J. Prosthet. Dent. 2020, 123, 564–570. [Google Scholar] [CrossRef]
- Mangano, F.; Mangano, C.; Margiani, B.; Admakin, O. Combining Intraoral and Face Scans for the Design and Fabrication of Computer-Assisted Design/Computer-Assisted Manufacturing (CAD/CAM) Polyether-Ether-Ketone (PEEK) Implant-Supported Bars for Maxillary Overdentures. Scanning 2019, 2019, 4274715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mai, H.-N.; Lee, D.-H. Accuracy of Mobile Device–Compatible 3D Scanners for Facial Digitization: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2020, 22, e22228. [Google Scholar] [CrossRef] [PubMed]
- Mai, H.N.; Lee, D.H. A digital technique to replicate edentulous arches with functional borders and accurate maxillomandibular relationship for digital complete denture. J. Prosthodont. 2020, 29, 356–359. [Google Scholar] [CrossRef] [PubMed]
- Maal, T.J.J.; Plooij, J.M.; Rangel, F.A.; Mollemans, W.; Schutyser, F.A.C.; Bergé, S.J. The accuracy of matching three-dimensional photographs with skin surfaces derived from cone-beam computed tomography. Int. J. Oral Maxillofac. Surg. 2008, 37, 641–646. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.-j.; Xiong, Y.-x.; Wang, Y. Three-dimensional accuracy of facial scan for facial deformities in clinics: A new evaluation method for facial scanner accuracy. PLoS ONE 2017, 12, e0169402. [Google Scholar] [CrossRef]
- Xiao, Z.; Liu, Z.; Gu, Y. Integration of digital maxillary dental casts with 3D facial images in orthodontic patients: A three-dimensional validation study. Angle Orthod. 2019, 90, 397–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ritschl, L.M.; Wolff, K.-D.; Erben, P.; Grill, F.D. Simultaneous, radiation-free registration of the dentoalveolar position and the face by combining 3D photography with a portable scanner and impression-taking. Head Face Med. 2019, 15, 28. [Google Scholar] [CrossRef] [PubMed]
- Mai, H.-N.; Lee, D.-H. The Effect of Perioral Scan and Artificial Skin Markers on the Accuracy of Virtual Dentofacial Integration: Stereophotogrammetry Versus Smartphone Three-Dimensional Face-Scanning. Int. J. Environ. Res. Public Health 2021, 18, 229. [Google Scholar] [CrossRef] [PubMed]
- Michaeli, J.G.; DeGroff, M.C.; Roxas, R.C. Error Aggregation in the Reengineering Process from 3D Scanning to Printing. Scanning 2017, 2017, 1218541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amornvit, P.; Sanohkan, S. The Accuracy of Digital Face Scans Obtained from 3D Scanners: An In Vitro Study. Int. J. Environ. Res. Public Health 2019, 16, 5061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, K.; Shim, H. Robust approach to reconstructing transparent objects using a time-of-flight depth camera. Opt. Express 2017, 25, 2666–2676. [Google Scholar] [CrossRef]
- Revilla-León, M.; Campbell, H.E.; Meyer, M.J.; Umorin, M.; Sones, A.; Zandinejad, A. Esthetic dental perception comparisons between 2D- and 3D-simulated dental discrepancies. J. Prosthet. Dent. 2020, 124, 763–773. [Google Scholar] [CrossRef]
- Kattadiyil, M.T.; Goodacre, C.J.; Naylor, W.P.; Maveli, T.C. Esthetic smile preferences and the orientation of the maxillary occlusal plane. J. Prosthet. Dent. 2012, 108, 354–361. [Google Scholar] [CrossRef]
- Ker, A.; Chan, R.; Fields, H.W.; Beck, M.; Rosenstiel, S. Esthetics and smile characteristics from the layperson’s perspective: A computer-based survey study. J. Am. Dent. Assoc. 2008, 139, 1318–1327. [Google Scholar] [CrossRef]
- Thomas, J.L.; Hayes, C.; Zawaideh, S. The effect of axial midline angulation on dental esthetics. Angle Orthod. 2003, 73, 359–364. [Google Scholar] [CrossRef]
- Joda, T.; Gallucci, G.O. The virtual patient in dental medicine. Clin. Oral Implants Res. 2015, 26, 725–726. [Google Scholar] [CrossRef] [PubMed]
- Janson, G.; Branco, N.C.; Fernandes, T.M.F.; Sathler, R.; Garib, D.; Lauris, J.R.P. Influence of orthodontic treatment, midline position, buccal corridor and smile arc on smile attractiveness: A systematic review. Angle Orthod. 2011, 81, 153–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shyagali, T.R.; Chandralekha, B.; Bhayya, D.P.; Kumar, S.; Balasubramanyam, G. Are ratings of dentofacial attractiveness influenced by dentofacial midline discrepancies? Aust. Orthod. J. 2008, 24, 91–95. [Google Scholar] [PubMed]
- Batwa, W.; Hunt, N.P.; Petrie, A.; Gill, D. Effect of occlusal plane on smile attractiveness. Angle Orthod. 2012, 82, 218–223. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Face-Scanning System | Tooth-Based Matching Mean (SD) | Marker-Based Matching Mean (SD) | p |
|---|---|---|---|---|
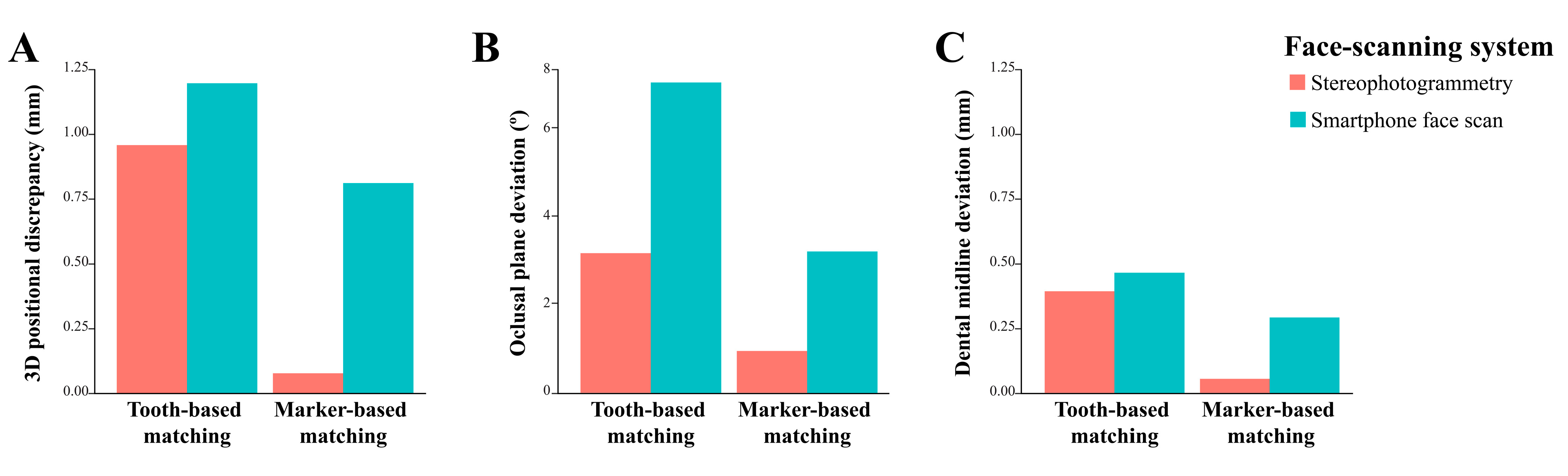
| Three-dimensional positional discrepancy (mm) | Stereophotogrammetry | 0.959 (0.043) a,1 | 0.078 (0.041) b,1 | 0.008 |
| Smartphone face scan | 1.197 (0.106) a,2 | 0.812 (0.065) b,2 | 0.008 | |
| p | 0.016 | 0.008 | ||
| Occlusal angle deviation (degrees) | Stereophotogrammetry | 3.187 (0.147) a,1 | 0.955 (0.350) b,1 | 0.008 |
| Smartphone face scan | 7.087 (0.608) a,2 | 3.225 (0.242) b,2 | 0.008 | |
| p | 0.008 | 0.008 | ||
| Dental midline deviation (mm) | Stereophotogrammetry | 0.393 (0.257) a,1 | 0.054 (0.074) b,1 | 0.032 |
| Smartphone face scan | 0.466 (0.031) a,1 | 0.292 (0.178) a,2 | 0.151 | |
| p | 0.690 | 0.032 |
| Outcome Variable | Source | Sum of Squares | df | Mean Square | F | p * |
|---|---|---|---|---|---|---|
| Three-dimensional positional discrepancy | Face-scanning system × image-matching method | 6.984 | 3 | 2.328 | 440.965 | <0.001 |
| Occlusal plane deviation | 184.681 | 3 | 64.894 | 408.234 | <0.001 | |
| Dental midline deviation | 0.965 | 3 | 0.322 | 11.102 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mai, H.-N.; Lee, D.-H. Effects of Artificial Extraoral Markers on Accuracy of Three-Dimensional Dentofacial Image Integration: Smartphone Face Scan versus Stereophotogrammetry. J. Pers. Med. 2022, 12, 490. https://doi.org/10.3390/jpm12030490
Mai H-N, Lee D-H. Effects of Artificial Extraoral Markers on Accuracy of Three-Dimensional Dentofacial Image Integration: Smartphone Face Scan versus Stereophotogrammetry. Journal of Personalized Medicine. 2022; 12(3):490. https://doi.org/10.3390/jpm12030490
Chicago/Turabian StyleMai, Hang-Nga, and Du-Hyeong Lee. 2022. "Effects of Artificial Extraoral Markers on Accuracy of Three-Dimensional Dentofacial Image Integration: Smartphone Face Scan versus Stereophotogrammetry" Journal of Personalized Medicine 12, no. 3: 490. https://doi.org/10.3390/jpm12030490
APA StyleMai, H.-N., & Lee, D.-H. (2022). Effects of Artificial Extraoral Markers on Accuracy of Three-Dimensional Dentofacial Image Integration: Smartphone Face Scan versus Stereophotogrammetry. Journal of Personalized Medicine, 12(3), 490. https://doi.org/10.3390/jpm12030490