
Whole Brain Hemodynamic Response Based on Synchrony Analysis of Brain Signals for Effective Application of HD-tDCS in Stroke Patients: An fNIRS Study

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Protocol
2.3. HD-tDCS
2.4. fNIRS Data Acquisition
2.5. Cortical Hemodynamic Response Analysis
3. Results
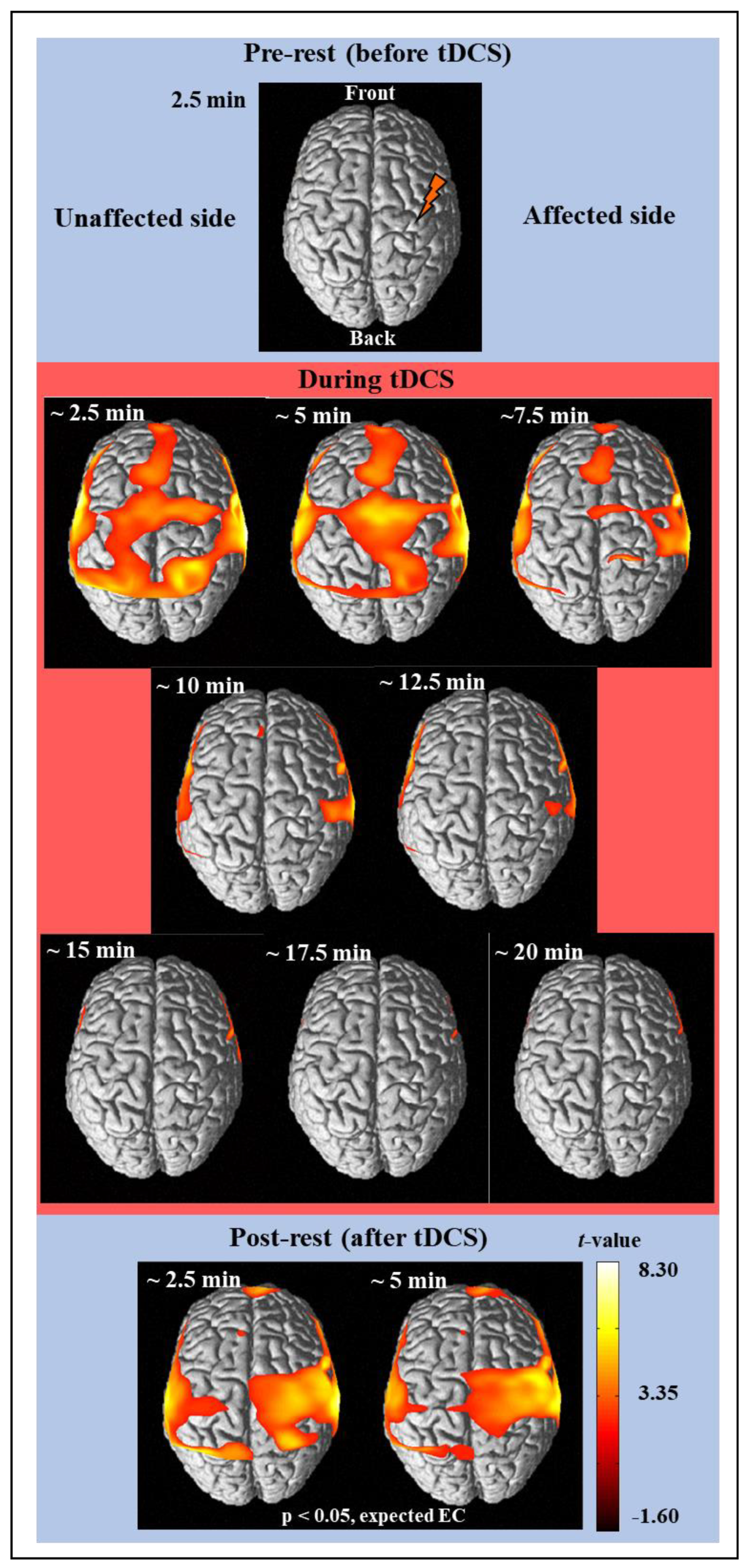
3.1. Activation Analysis Results Using NIRS-SPM
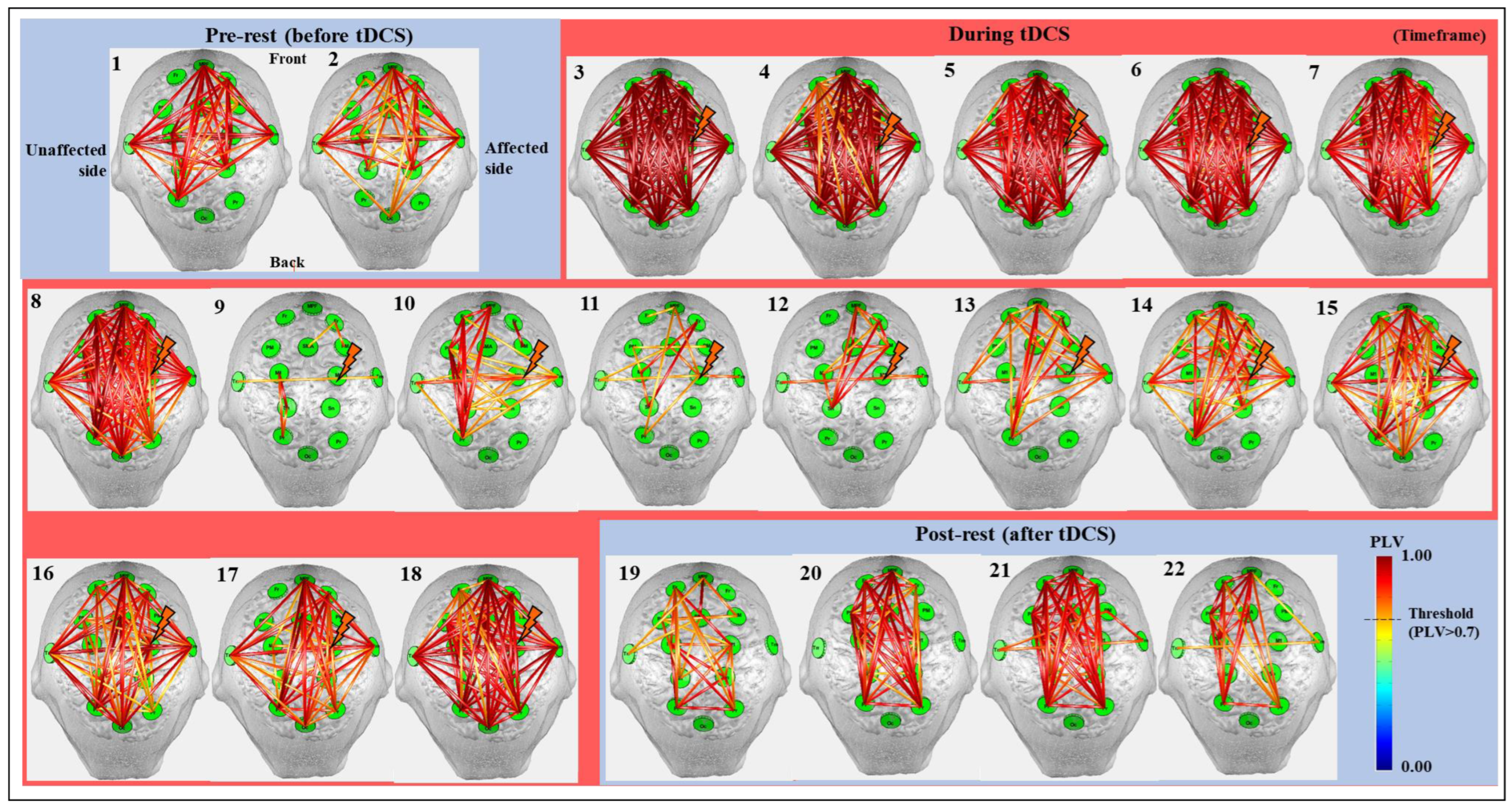
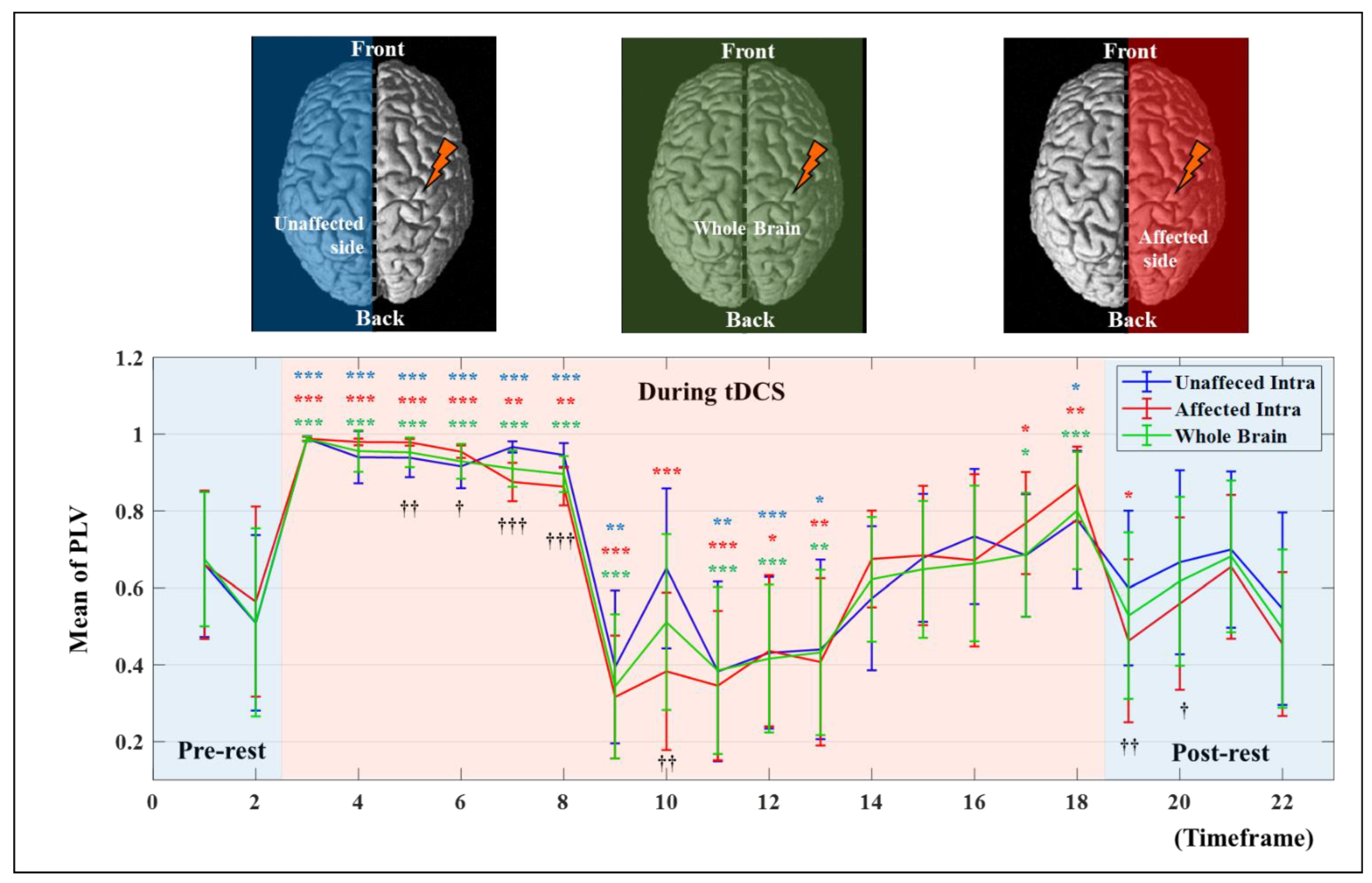
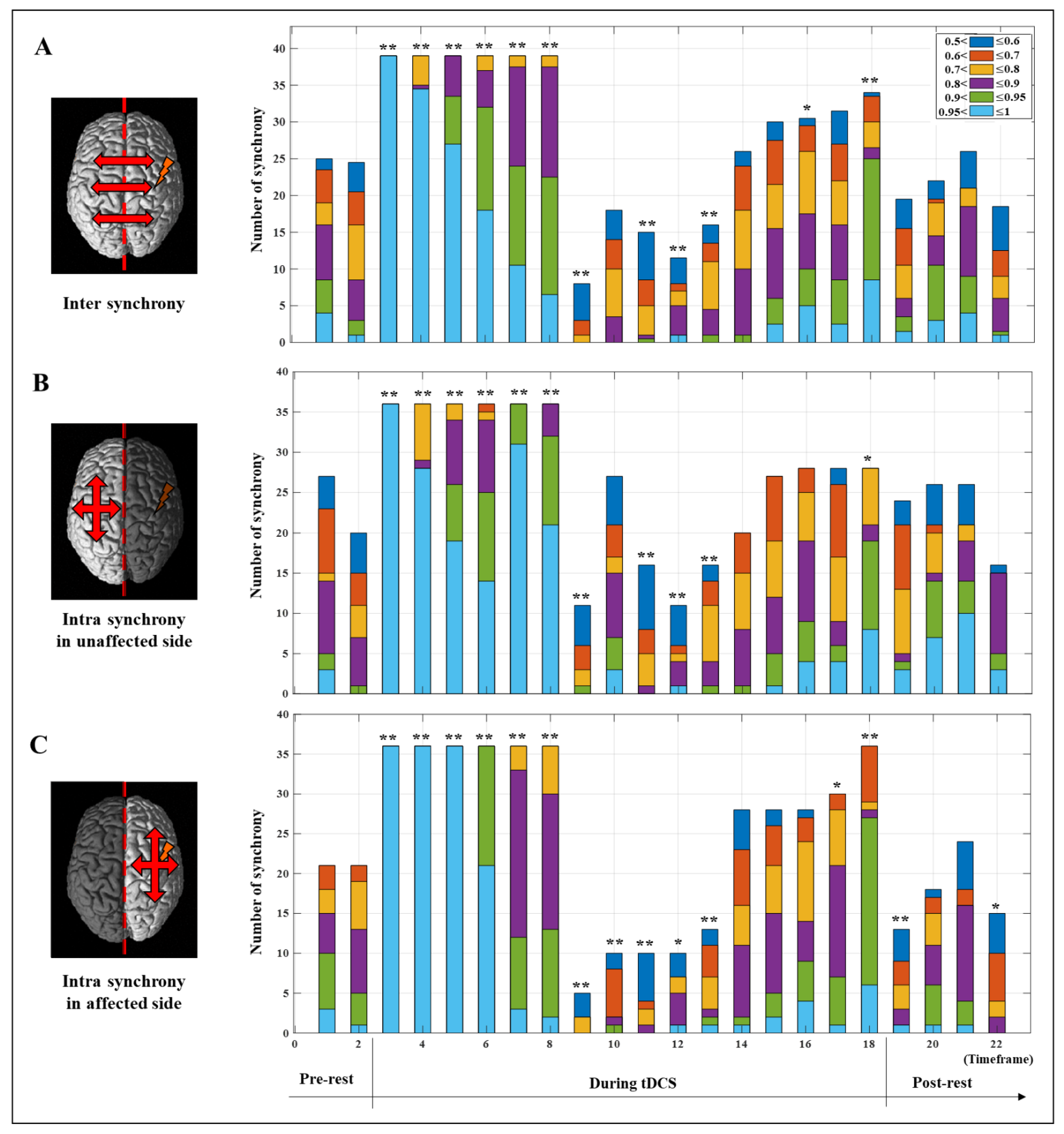
3.2. Synchrony Analysis Results Using OptoNet II®
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Li, S. Spasticity, motor recovery, and neural plasticity after stroke. Front. Neurol. 2017, 8, 120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iosa, M.; Morone, G.; Fusco, A.; Bragoni, M.; Coiro, P.; Multari, M.; Venturiero, V.; De Angelis, D.; Pratesi, L.; Paolucci, S. Seven capital devices for the future of stroke rehabilitation. Stroke Res. Treat. 2012, 2012, 187965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langhorne, P.; Coupar, F.; Pollock, A. Motor recovery after stroke: A systematic review. Lancet Neurol. 2009, 8, 741–754. [Google Scholar] [CrossRef]
- Nitsche, M.A.; Paulus, W. Excitability changes induced in the human motor cortex by weak transcranial direct current stimulation. J. Physiol. 2000, 527, 633–639. [Google Scholar] [CrossRef] [PubMed]
- Dubljević, V.; Saigle, V.; Racine, E. The rising tide of tDCS in the media and academic literature. Neuron 2014, 82, 731–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simonsmeier, B.A.; Grabner, R.H.; Hein, J.; Krenz, U.; Schneider, M. Electrical brain stimulation (tES) improves learning more than performance: A meta-analysis. Neurosci. Biobehav. Rev. 2018, 84, 171–181. [Google Scholar] [CrossRef] [PubMed]
- Imburgio, M.J.; Orr, J.M. Effects of prefrontal tDCS on executive function: Methodological considerations revealed by meta-analysis. Neuropsychologia 2018, 117, 156–166. [Google Scholar] [CrossRef] [PubMed]
- Buch, E.R.; Santarnecchi, E.; Antal, A.; Born, J.; Celnik, P.A.; Classen, J.; Gerloff, C.; Hallett, M.; Hummel, F.C.; Nitsche, M.A. Effects of tDCS on motor learning and memory formation: A consensus and critical position paper. Clin. Neurophysiol. 2017, 128, 589–603. [Google Scholar] [CrossRef] [Green Version]
- Pixa, N.H.; Pollok, B. Effects of tDCS on bimanual motor skills: A brief review. Front. Behav. Neurosci. 2018, 12, 63. [Google Scholar] [CrossRef]
- Angius, L.; Hopker, J.; Mauger, A.R. The ergogenic effects of transcranial direct current stimulation on exercise performance. Front. Physiol. 2017, 8, 90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fenton, B.W.; Palmieri, P.A.; Boggio, P.; Fanning, J.; Fregni, F. A preliminary study of transcranial direct current stimulation for the treatment of refractory chronic pelvic pain. Brain Stimul. 2009, 2, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Fagerlund, A.J.; Hansen, O.A.; Aslaksen, P.M. Transcranial direct current stimulation as a treatment for patients with fibromyalgia: A randomized controlled trial. Pain 2015, 156, 62–71. [Google Scholar] [CrossRef] [PubMed]
- Palm, U.; Schiller, C.; Fintescu, Z.; Obermeier, M.; Keeser, D.; Reisinger, E.; Pogarell, O.; Nitsche, M.; Möller, H.-J.; Padberg, F. Transcranial direct current stimulation in treatment resistant depression: A randomized double-blind, placebo-controlled study. Brain Stimul. 2012, 5, 242–251. [Google Scholar] [CrossRef] [PubMed]
- Kaski, D.; Dominguez, R.; Allum, J.; Islam, A.; Bronstein, A. Combining physical training with transcranial direct current stimulation to improve gait in Parkinson’s disease: A pilot randomized controlled study. Clin. Rehabil. 2014, 28, 1115–1124. [Google Scholar] [CrossRef] [PubMed]
- Breitling, C.; Zaehle, T.; Dannhauer, M.; Bonath, B.; Tegelbeckers, J.; Flechtner, H.-H.; Krauel, K. Improving interference control in ADHD patients with transcranial direct current stimulation (tDCS). Front. Cell. Neurosci. 2016, 10, 72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghafoor, U.; Kim, S.; Hong, K.-S. Selectivity and longevity of peripheral-nerve and machine interfaces: A review. Front. Neurorobotics 2017, 11, 59. [Google Scholar] [CrossRef] [Green Version]
- Wei, Y.; Gu, K.; Cui, X.; Hao, C.; Wang, H.; Chang, Y. Strategies for feet massage robot to position the pelma acupoints with model predictive and real-time optimization. Int. J. Control Autom. Syst. 2016, 14, 628–636. [Google Scholar] [CrossRef]
- Hong, K.-S.; Aziz, N.; Ghafoor, U. Motor-commands decoding using peripheral nerve signals: A review. J. Neural Eng. 2018, 15, 031004. [Google Scholar] [CrossRef] [Green Version]
- Horvath, J.C.; Carter, O.; Forte, J.D. No significant effect of transcranial direct current stimulation (tDCS) found on simple motor reaction time comparing 15 different simulation protocols. Neuropsychologia 2016, 91, 544–552. [Google Scholar] [CrossRef]
- Pellicciari, M.C.; Brignani, D.; Miniussi, C. Excitability modulation of the motor system induced by transcranial direct current stimulation: A multimodal approach. Neuroimage 2013, 83, 569–580. [Google Scholar] [CrossRef] [Green Version]
- Polanía, R.; Nitsche, M.A.; Paulus, W. Modulating functional connectivity patterns and topological functional organization of the human brain with transcranial direct current stimulation. Hum. Brain Mapp. 2011, 32, 1236–1249. [Google Scholar] [CrossRef] [PubMed]
- Stagg, C.; O’shea, J.; Kincses, Z.; Woolrich, M.; Matthews, P.; Johansen-Berg, H. Modulation of movement-associated cortical activation by transcranial direct current stimulation. Eur. J. Neurosci. 2009, 30, 1412–1423. [Google Scholar] [CrossRef] [PubMed]
- Bindman, L.J.; Lippold, O.; Redfearn, J. The action of brief polarizing currents on the cerebral cortex of the rat (1) during current flow and (2) in the production of long-lasting after-effects. J. Physiol. 1964, 172, 369–382. [Google Scholar] [CrossRef] [PubMed]
- Brunoni, A.R.; Nitsche, M.A.; Bolognini, N.; Bikson, M.; Wagner, T.; Merabet, L.; Edwards, D.J.; Valero-Cabre, A.; Rotenberg, A.; Pascual-Leone, A. Clinical research with transcranial direct current stimulation (tDCS): Challenges and future directions. Brain Stimul. 2012, 5, 175–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bao, S.-C.; Wong, W.-W.; Leung, T.W.H.; Tong, K.-Y. Cortico-muscular coherence modulated by high-definition transcranial direct current stimulation in people with chronic stroke. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 27, 304–313. [Google Scholar] [CrossRef] [PubMed]
- Nikolin, S.; Loo, C.K.; Bai, S.; Dokos, S.; Martin, D.M. Focalised stimulation using high definition transcranial direct current stimulation (HD-tDCS) to investigate declarative verbal learning and memory functioning. Neuroimage 2015, 117, 11–19. [Google Scholar] [CrossRef]
- Villringer, A.; Dirnagl, U. Coupling of brain activity and cerebral blood flow: Basis of functional neuroimaging. Cerebrovasc. Brain Metab. Rev. 1995, 7, 240–276. [Google Scholar]
- Hoshi, Y. Functional near-infrared optical imaging: Utility and limitations in human brain mapping. Psychophysiology 2003, 40, 511–520. [Google Scholar] [CrossRef]
- Ye, J.C.; Tak, S.; Jang, K.E.; Jung, J.; Jang, J. NIRS-SPM: Statistical parametric mapping for near-infrared spectroscopy. Neuroimage 2009, 44, 428–447. [Google Scholar] [CrossRef]
- Huppert, T.J.; Diamond, S.G.; Franceschini, M.A.; Boas, D.A. HomER: A review of time-series analysis methods for near-infrared spectroscopy of the brain. Appl. Opt. 2009, 48, D280–D298. [Google Scholar] [CrossRef] [Green Version]
- Aarabi, A.; Wallois, F.; Grebe, R. Does spatiotemporal synchronization of EEG change prior to absence seizures? Brain Res. 2008, 1188, 207–221. [Google Scholar] [CrossRef] [PubMed]
- Thut, G.; Veniero, D.; Romei, V.; Miniussi, C.; Schyns, P.; Gross, J. Rhythmic TMS causes local entrainment of natural oscillatory signatures. Curr. Biol. 2011, 21, 1176–1185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varotto, G.; Visani, E.; Franceschetti, S.; Sparacino, G.; Panzica, F. Spectral and coherence analysis of EEG during intermittent photic stimulation in patients with photosensitive epilepsy. Int. J. Bioelectromagn. 2009, 11, 189–193. [Google Scholar]
- Yilmaz, I. Landslide susceptibility mapping using frequency ratio, logistic regression, artificial neural networks and their comparison: A case study from Kat landslides (Tokat—Turkey). Comput. Geosci. 2009, 35, 1125–1138. [Google Scholar] [CrossRef]
- Lachaux, J.P.; Rodriguez, E.; Martinerie, J.; Varela, F.J. Measuring phase synchrony in brain signals. Hum. Brain Mapp. 1999, 8, 194–208. [Google Scholar] [CrossRef] [Green Version]
- Lee, G.; Park, J.-S.; Jung, Y.-J. OptoNet: A MATLAB-based toolbox for cortical network analyses using functional near-infrared spectroscopy. Opt. Eng. 2019, 59, 061602. [Google Scholar] [CrossRef]
- Lee, G.; Park, J.-S.; Lee, J.; Kim, J.; Jung, Y.-J.; Kim, Y.-H. OptoNet II: An Advanced MATLAB-Based Toolbox for Functional Cortical Connectivity Analysis with Surrogate Tests Using fNIRS. IEEE Access 2020, 9, 15983–15991. [Google Scholar] [CrossRef]
- Tzourio-Mazoyer, N.; Landeau, B.; Papathanassiou, D.; Crivello, F.; Etard, O.; Delcroix, N.; Mazoyer, B.; Joliot, M. Automated anatomical labeling of activations in SPM using a macroscopic anatomical parcellation of the MNI MRI single-subject brain. Neuroimage 2002, 15, 273–289. [Google Scholar] [CrossRef]
- Penny, W.D.; Friston, K.J.; Ashburner, J.T.; Kiebel, S.J.; Nichols, T.E. Statistical Parametric Mapping: The Analysis of Functional Brain Images; Elsevier: Amsterdam, The Netherlands, 2011. [Google Scholar]
- Morais, G.A.Z.; Balardin, J.B.; Sato, J.R. fNIRS optodes’ location decider (fOLD): A toolbox for probe arrangement guided by brain regions-of-interest. Sci. Rep. 2018, 8, 3341. [Google Scholar] [CrossRef] [Green Version]
- Bhutta, M.R.; Woo, S.-W.; Khan, M.J.; Hong, K.-S. Effect of anodal tDCS on human prefrontal cortex observed by fNIRS. In Proceedings of the 2016 6th IEEE International Conference on Biomedical Robotics and Biomechatronics (BioRob), Singapore, 26–29 June 2016; pp. 957–961. [Google Scholar]
- Yan, J.; Wei, Y.; Wang, Y.; Xu, G.; Li, Z.; Li, X. Use of functional near-infrared spectroscopy to evaluate the effects of anodal transcranial direct current stimulation on brain connectivity in motor-related cortex. J. Biomed. Opt. 2015, 20, 046007. [Google Scholar] [CrossRef]
- Takai, H.; Tsubaki, A.; Sugawara, K.; Miyaguchi, S.; Oyanagi, K.; Matsumoto, T.; Onishi, H.; Yamamoto, N. Effect of transcranial direct current stimulation over the primary motor cortex on cerebral blood flow: A time course study using near-infrared spectroscopy. In Oxygen Transport to Tissue XXXVII; Springer: Berlin/Heidelberg, Germany, 2016; pp. 335–341. [Google Scholar]
- Stephens, J.A.; Berryhill, M.E. Older adults improve on everyday tasks after working memory training and neurostimulation. Brain Stimul. 2016, 9, 553–559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borragán, G.; Gilson, M.; Guerrero-Mosquera, C.; Di Ricci, E.; Slama, H.; Peigneux, P. Transcranial direct current stimulation does not counteract cognitive fatigue, but induces sleepiness and an inter-hemispheric shift in brain oxygenation. Front. Psychol. 2018, 9, 2351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, J.; Liu, H.; Alexandrakis, G. Modulating the resting-state functional connectivity patterns of language processing areas in the human brain with anodal transcranial direct current stimulation applied over the Broca’s area. Neurophotonics 2018, 5, 025002. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.; Dawidziuk, A.; Darzi, A.W.; Singh, H.; Leff, D.R. Systematic review of combined functional near-infrared spectroscopy and transcranial direct-current stimulation studies. Neurophotonics 2020, 7, 020901. [Google Scholar] [CrossRef] [PubMed]
- Dutta, A.; Jacob, A.; Chowdhury, S.R.; Das, A.; Nitsche, M.A. EEG-NIRS based assessment of neurovascular coupling during anodal transcranial direct current stimulation-a stroke case series. J. Med. Syst. 2015, 39, 36. [Google Scholar] [CrossRef]
- Jindal, U.; Sood, M.; Chowdhury, S.R.; Das, A.; Kondziella, D.; Dutta, A. Corticospinal excitability changes to anodal tDCS elucidated with NIRS-EEG joint-imaging: An ischemic stroke study. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 3399–3402. [Google Scholar]
- Li, H.; Zhu, N.; Klomparens, E.A.; Xu, S.; Wang, M.; Wang, Q.; Wang, J.; Song, L. Application of functional near-infrared spectroscopy to explore the neural mechanism of transcranial direct current stimulation for post-stroke depression. Neurol. Res. 2019, 41, 714–721. [Google Scholar] [CrossRef]
- Narita, Z.; Noda, T.; Setoyama, S.; Sueyoshi, K.; Inagawa, T.; Sumiyoshi, T. The effect of transcranial direct current stimulation on psychotic symptoms of schizophrenia is associated with oxy-hemoglobin concentrations in the brain as measured by near-infrared spectroscopy: A pilot study. J. Psychiatr. Res. 2018, 103, 5–9. [Google Scholar] [CrossRef]
- Dias, I.A.; Hazime, F.A.; Lopes, D.A.; da Silva, C.S.; Baptista, A.F.; da Silva, B.A.K. Effects of transcranial direct current stimulation on heart rate variability: A systematic review protocol. JBI Evid. Synth. 2020, 18, 1313–1319. [Google Scholar] [CrossRef]
- Verma, R.; Jha, A.; Singh, S. Functional near-infrared spectroscopy to probe tDCS-induced cortical functioning changes in tinnitus. J. Int. Adv. Otol. 2019, 15, 321. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | n = 26 |
|---|---|
| Age (years) | |
| Mean ± SD | 59.4 ± 12.8 |
| Sex (n) | |
| Male | 20 |
| Female | 6 |
| Stroke type (n) | |
| Infarction | 13 |
| Hemorrhage | 13 |
| Lesion location (n) | |
| Supratentoria | |
| Cortical | |
| MCA territory (Lt./Rt.) | 1 (0/1) |
| Subcortical | |
| CR (Lt./Rt.) | 3 (0/3) |
| BG (Lt./Rt.) | 10 (5/5) |
| CR + BG (Lt./Rt.) | 1 (1/0) |
| Thalamus (Lt./Rt.) | 5 (3/2) |
| Infratentorial | |
| Pons (Lt./Rt.) | 5 (5/0) |
| Medullar (Lt./Rt.) | 1 (0/1) |
| Duration (months) | |
| Mean ± SD | 40.1 ± 29.4 |
| FMA upper extremity score | |
| Mean ± SD | 47.6 ± 10.2 |
| FMA total score | |
| Mean ± SD | 69.3 ± 14.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, G.; Lee, J.; Kim, J.; Kim, H.; Chang, W.H.; Kim, Y.-H. Whole Brain Hemodynamic Response Based on Synchrony Analysis of Brain Signals for Effective Application of HD-tDCS in Stroke Patients: An fNIRS Study. J. Pers. Med. 2022, 12, 432. https://doi.org/10.3390/jpm12030432
Lee G, Lee J, Kim J, Kim H, Chang WH, Kim Y-H. Whole Brain Hemodynamic Response Based on Synchrony Analysis of Brain Signals for Effective Application of HD-tDCS in Stroke Patients: An fNIRS Study. Journal of Personalized Medicine. 2022; 12(3):432. https://doi.org/10.3390/jpm12030432
Chicago/Turabian StyleLee, Gihyoun, Jungsoo Lee, Jinuk Kim, Heegoo Kim, Won Hyuk Chang, and Yun-Hee Kim. 2022. "Whole Brain Hemodynamic Response Based on Synchrony Analysis of Brain Signals for Effective Application of HD-tDCS in Stroke Patients: An fNIRS Study" Journal of Personalized Medicine 12, no. 3: 432. https://doi.org/10.3390/jpm12030432
APA StyleLee, G., Lee, J., Kim, J., Kim, H., Chang, W. H., & Kim, Y.-H. (2022). Whole Brain Hemodynamic Response Based on Synchrony Analysis of Brain Signals for Effective Application of HD-tDCS in Stroke Patients: An fNIRS Study. Journal of Personalized Medicine, 12(3), 432. https://doi.org/10.3390/jpm12030432