
Therapeutic Vitamin D Supplementation Following COVID-19 Diagnosis: Where Do We Stand?—A Systematic Review

 , ,
, , 
 , , , ,
, , , , 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol
2.2. Literature Search
2.3. Inclusion and Exclusion Criteria
2.4. Data Extraction
2.5. Quality Assesment
3. Results
3.1. Search Results
3.2. Study Characteristics
3.3. Interventions
3.4. Length of Hospital Stay
3.5. Need for Intubation and ICU Admission
3.6. Mortality
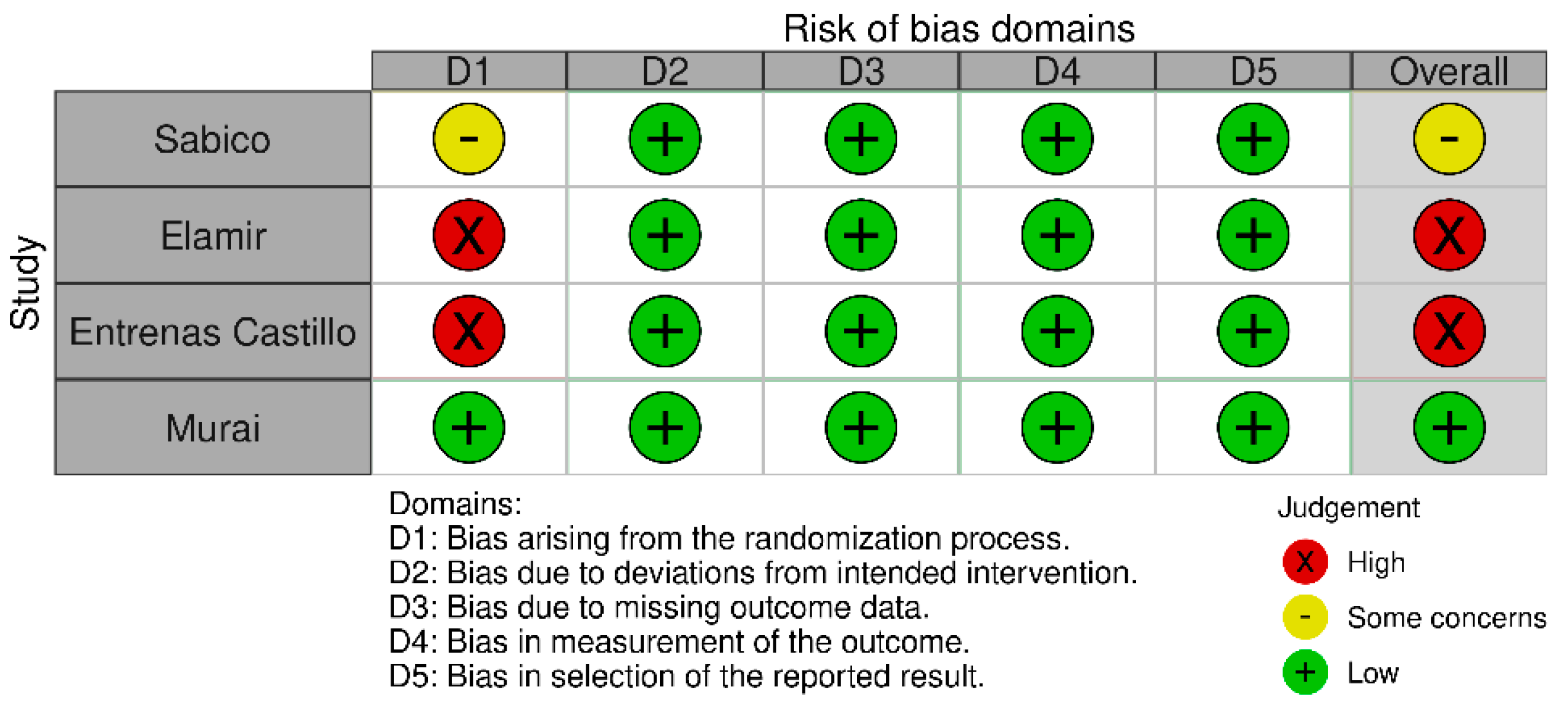
3.7. Quality Assessment and Risk of Bias
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 4 December 2021).
- COVID-19 Treatment Guidelines Panel Coronavirus Disease 2019 (COVID-19) Treatment Guidelines. Available online: https://www.covid19treatmentguidelines.nih.gov/ (accessed on 18 February 2022).
- Holick, M.F.; MacLaughlin, J.A.; Clark, M.B.; Holick, S.A.; Potts, J.T.; Anderson, R.R.; Blank, I.H.; Parrish, J.A.; Elias, P. Photosynthesis of Previtamin D3 in Human Skin and the Physiologic Consequences. Science 1980, 210, 203–205. [Google Scholar] [CrossRef] [PubMed]
- Bikle, D.D. Vitamin D Metabolism, Mechanism of Action, and Clinical Applications. Chem. Biol. 2014, 21, 319–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nurminen, V.; Seuter, S.; Carlberg, C. Primary Vitamin D Target Genes of Human Monocytes. Front. Physiol. 2019, 10, 194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlberg, C. Vitamin D: A Micronutrient Regulating Genes. Curr. Pharm. Des. 2019, 25, 1740–1746. [Google Scholar] [CrossRef] [PubMed]
- Pike, J.W.; Meyer, M.B. The Vitamin D Receptor: New Paradigms for the Regulation of Gene Expression by 1,25-Dihydroxyvitamin D3. Endocrinol. Metab. Clin. N. Am. 2010, 39, 255–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Endocrine Society Evaluation, Treatment, and Prevention of Vitamin D Deficiency: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [Green Version]
- Marino, R.; Misra, M. Extra-Skeletal Effects of Vitamin D. Nutrients 2019, 11, 1460. [Google Scholar] [CrossRef] [Green Version]
- Aygun, H. Vitamin D Can Prevent COVID-19 Infection-Induced Multiple Organ Damage. Naunyn. Schmiedebergs Arch. Pharmacol. 2020, 393, 1157–1160. [Google Scholar] [CrossRef]
- Mercola, J.; Grant, W.B.; Wagner, C.L. Evidence Regarding Vitamin D and Risk of COVID-19 and Its Severity. Nutrients 2020, 12, 3361. [Google Scholar] [CrossRef] [PubMed]
- Dimitrov, V.; White, J.H. Species-Specific Regulation of Innate Immunity by Vitamin D Signaling. J. Steroid Biochem. Mol. Biol. 2016, 164, 246–253. [Google Scholar] [CrossRef]
- Peterson, C.A.; Heffernan, M.E. Serum Tumor Necrosis Factor-Alpha Concentrations Are Negatively Correlated with Serum 25(OH)D Concentrations in Healthy Women. J. Inflamm. Lond. Engl. 2008, 5, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cantorna, M.T.; Snyder, L.; Lin, Y.-D.; Yang, L. Vitamin D and 1,25(OH)2D Regulation of T Cells. Nutrients 2015, 7, 3011–3021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talmor, Y.; Bernheim, J.; Klein, O.; Green, J.; Rashid, G. Calcitriol Blunts Pro-Atherosclerotic Parameters through NFkappaB and P38 in Vitro. Eur. J. Clin. Investig. 2008, 38, 548–554. [Google Scholar] [CrossRef] [PubMed]
- Fisher, S.A.; Rahimzadeh, M.; Brierley, C.; Gration, B.; Doree, C.; Kimber, C.E.; Plaza Cajide, A.; Lamikanra, A.A.; Roberts, D.J. The Role of Vitamin D in Increasing Circulating T Regulatory Cell Numbers and Modulating T Regulatory Cell Phenotypes in Patients with Inflammatory Disease or in Healthy Volunteers: A Systematic Review. PLoS ONE 2019, 14, e0222313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, G.; Wu, D.; Guo, W.; Cao, Y.; Huang, D.; Wang, H.; Wang, T.; Zhang, X.; Chen, H.; Yu, H.; et al. Clinical and Immunological Features of Severe and Moderate Coronavirus Disease 2019. J. Clin. Investig. 2020, 130, 2620–2629. [Google Scholar] [CrossRef] [Green Version]
- López-Castro, J. Coronavirus Disease-19 Pandemic and Vitamin D: So Much for so Little? Rev. Investig. Clin. Organo Hosp. Enferm. Nutr. 2021, 73, 408. [Google Scholar] [CrossRef] [PubMed]
- Sieiro-Santos, C.; López-Castro, J. Post-Coronavirus Disease Syndrome and Disseminated Microthrombosis: The Role of the von Willebrand Factor and Antiphospholipid Antibodies. Clinics 2021, 76, e2784. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef]
- Imai, Y.; Kuba, K.; Rao, S.; Huan, Y.; Guo, F.; Guan, B.; Yang, P.; Sarao, R.; Wada, T.; Leong-Poi, H.; et al. Angiotensin-Converting Enzyme 2 Protects from Severe Acute Lung Failure. Nature 2005, 436, 112–116. [Google Scholar] [CrossRef]
- Vaidya, A.; Forman, J.P.; Hopkins, P.N.; Seely, E.W.; Williams, J.S. 25-Hydroxyvitamin D Is Associated with Plasma Renin Activity and the Pressor Response to Dietary Sodium Intake in Caucasians. J. Renin-Angiotensin-Aldosterone Syst. 2011, 12, 311–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forman, J.P.; Williams, J.S.; Fisher, N.D.L. Plasma 25-Hydroxyvitamin D and Regulation of the Renin-Angiotensin System in Humans. Hypertension 2010, 55, 1283–1288. [Google Scholar] [CrossRef] [Green Version]
- Xu, J.; Yang, J.; Chen, J.; Luo, Q.; Zhang, Q.; Zhang, H. Vitamin D Alleviates Lipopolysaccharide-induced Acute Lung Injury via Regulation of the Renin-angiotensin System. Mol. Med. Rep. 2017, 16, 7432–7438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jevalikar, G.; Mithal, A.; Singh, A.; Sharma, R.; Farooqui, K.J.; Mahendru, S.; Dewan, A.; Budhiraja, S. Lack of Association of Baseline 25-Hydroxyvitamin D Levels with Disease Severity and Mortality in Indian Patients Hospitalized for COVID-19. Sci. Rep. 2021, 11, 6258. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological Index For Non-Randomized Studies (MINORS): Development And Validation of A New Instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Annweiler, G.; Corvaisier, M.; Gautier, J.; Dubée, V.; Legrand, E.; Sacco, G.; Annweiler, C. Vitamin D Supplementation Associated to Better Survival in Hospitalized Frail Elderly COVID-19 Patients: The GERIA-COVID Quasi-Experimental Study. Nutrients 2020, 12, 3377. [Google Scholar] [CrossRef] [PubMed]
- Sabico, S.; Enani, M.A.; Sheshah, E.; Aljohani, N.J.; Aldisi, D.A.; Alotaibi, N.H.; Alshingetti, N.; Alomar, S.Y.; Alnaami, A.M.; Amer, O.E.; et al. Effects of a 2-Week 5000 IU vs. 1000 IU Vitamin D3 Supplementation on Recovery of Symptoms in Patients with Mild to Moderate Covid-19: A Randomized Clinical Trial. Nutrients 2021, 13, 2170. [Google Scholar] [CrossRef]
- Güven, M.; Gültekin, H. The Effect of High-Dose Parenteral Vitamin D3 on COVID-19-Related Inhospital Mortality in Critical COVID-19 Patients during Intensive Care Unit Admission: An Observational Cohort Study. Eur. J. Clin. Nutr. 2021, 75, 1383–1388. [Google Scholar] [CrossRef]
- Nogues, X.; Ovejero, D.; Pineda-Moncusí, M.; Bouillon, R.; Arenas, D.; Pascual, J.; Ribes, A.; Guerri-Fernandez, R.; Villar-Garcia, J.; Rial, A.; et al. Calcifediol Treatment and COVID-19-Related Outcomes. J. Clin. Endocrinol. Metab. 2021, 106, e4017–e4027. [Google Scholar] [CrossRef]
- Elamir, Y.M.; Amir, H.; Lim, S.; Rana, Y.P.; Lopez, C.G.; Feliciano, N.V.; Omar, A.; Grist, W.P.; Via, M.A. A Randomized Pilot Study Using Calcitriol in Hospitalized COVID-19 Patients. Bone 2022, 154, 116175. [Google Scholar] [CrossRef]
- Entrenas Castillo, M.; Entrenas Costa, L.M.; Vaquero Barrios, J.M.; Alcalá Díaz, J.F.; López Miranda, J.; Bouillon, R.; Quesada Gomez, J.M. Effect of Calcifediol Treatment and Best Available Therapy vs. Best Available Therapy on Intensive Care Unit Admission and Mortality among Patients Hospitalized for COVID-19: A Pilot Randomized Clinical Study. J. Steroid Biochem. Mol. Biol. 2020, 203, 105751. [Google Scholar] [CrossRef] [PubMed]
- Alcala-Diaz, J.F.; Limia-Perez, L.; Gomez-Huelgas, R.; Martin-Escalante, M.D.; Cortes-Rodriguez, B.; Zambrana-Garcia, J.L.; Entrenas-Castillo, M.; Perez-Caballero, A.I.; López-Carmona, M.D.; Garcia-Alegria, J.; et al. Calcifediol Treatment and Hospital Mortality Due to COVID-19: A Cohort Study. Nutrients 2021, 13, 1760. [Google Scholar] [CrossRef] [PubMed]
- Murai, I.H.; Fernandes, A.L.; Sales, L.P.; Pinto, A.J.; Goessler, K.F.; Duran, C.S.C.; Silva, C.B.R.; Franco, A.S.; Macedo, M.B.; Dalmolin, H.H.H.; et al. Effect of a Single High Dose of Vitamin D3 on Hospital Length of Stay in Patients With Moderate to Severe COVID-19. JAMA 2021, 325, 1053–1060. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.W.; Ho, L.P.; Kalimuddin, S.; Cherng, B.P.Z.; Teh, Y.E.; Thien, S.Y.; Wong, H.M.; Tern, P.J.W.; Chandran, M.; Chay, J.W.M.; et al. Cohort Study to Evaluate the Effect of Vitamin D, Magnesium, and Vitamin B12 in Combination on Progression to Severe Outcomes in Older Patients with Coronavirus (COVID-19). Nutrition 2020, 79–80, 111017. [Google Scholar] [CrossRef] [PubMed]
- Soliman, A.R.; Abdelaziz, T.S.; Fathy, A. Impact of Vitamin D Therapy on the Progress COVID-19: Six Weeks Follow-Up Study of Vitamin D Deficient Elderly Diabetes Patients. Proc. Singap. Healthc. 2021, 201010582110414. [Google Scholar] [CrossRef]
- Arteh, J.; Narra, S.; Nair, S. Prevalence of Vitamin D Deficiency in Chronic Liver Disease. Dig. Dis. Sci. 2010, 55, 2624–2628. [Google Scholar] [CrossRef]
- Kim, S.M.; Choi, H.J.; Lee, J.P.; Kim, D.K.; Oh, Y.K.; Kim, Y.S.; Lim, C.S. Prevalence of Vitamin D Deficiency and Effects of Supplementation with Cholecalciferol in Patients with Chronic Kidney Disease. J. Ren. Nutr. Off. J. Counc. Ren. Nutr. Natl. Kidney Found. 2014, 24, 20–25. [Google Scholar] [CrossRef]
- Wang, M.X.; Gwee, S.X.W.; Pang, J. Micronutrients Deficiency, Supplementation and Novel Coronavirus Infections-A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 1589. [Google Scholar] [CrossRef]
- Rawat, D.; Roy, A.; Maitra, S.; Shankar, V.; Khanna, P.; Baidya, D.K. Vitamin D Supplementation and COVID-19 Treatment: A Systematic Review and Meta-Analysis. Diabetes Metab. Syndr. 2021, 15, 102189. [Google Scholar] [CrossRef]
- Szarpak, L.; Rafique, Z.; Gasecka, A.; Chirico, F.; Gawel, W.; Hernik, J.; Kaminska, H.; Filipiak, K.J.; Jaguszewski, M.J.; Szarpak, L. A Systematic Review and Meta-Analysis of Effect of Vitamin D Levels on the Incidence of COVID-19. Cardiol. J. 2021, 28, 647–654. [Google Scholar] [CrossRef]
- Batista, K.S.; Cintra, V.M.; Lucena, P.A.F.; Manhães-de-Castro, R.; Toscano, A.E.; Costa, L.P.; Queiroz, M.E.B.S.; de Andrade, S.M.; Guzman-Quevedo, O.; de S Aquino, J. The Role of Vitamin B12 in Viral Infections: A Comprehensive Review of Its Relationship with the Muscle-Gut-Brain Axis and Implications for SARS-CoV-2 Infection. Nutr. Rev. 2022, 80, 561–578. [Google Scholar] [CrossRef] [PubMed]
- Vahedian-Azimi, A.; Abbasifard, M.; Rahimi-Bashar, F.; Guest, P.C.; Majeed, M.; Mohammadi, A.; Banach, M.; Jamialahmadi, T.; Sahebkar, A. Effectiveness of Curcumin on Outcomes of Hospitalized COVID-19 Patients: A Systematic Review of Clinical Trials. Nutrients 2022, 14, 256. [Google Scholar] [CrossRef] [PubMed]
- Shokri-Mashhadi, N.; Kazemi, M.; Saadat, S.; Moradi, S. Effects of Select Dietary Supplements on the Prevention and Treatment of Viral Respiratory Tract Infections: A Systematic Review of Randomized Controlled Trials. Expert Rev. Respir. Med. 2021, 15, 805–821. [Google Scholar] [CrossRef]
- Abioye, A.I.; Bromage, S.; Fawzi, W. Effect of Micronutrient Supplements on Influenza and Other Respiratory Tract Infections among Adults: A Systematic Review and Meta-Analysis. BMJ Glob. Health 2021, 6, e003176. [Google Scholar] [CrossRef]
- Jolliffe, D.A.; Camargo, C.A.; Sluyter, J.D.; Aglipay, M.; Aloia, J.F.; Ganmaa, D.; Bergman, P.; Borzutzky, A.; Damsgaard, C.T.; Dubnov-Raz, G.; et al. Vitamin D Supplementation to Prevent Acute Respiratory Infections: Systematic Review and Meta-Analysis of Aggregate Data from Randomised Controlled Trials. medRxiv 2020. [Google Scholar] [CrossRef]
- Crafa, A.; Cannarella, R.; Condorelli, R.A.; Mongioì, L.M.; Barbagallo, F.; Aversa, A.; La Vignera, S.; Calogero, A.E. Influence of 25-Hydroxy-Cholecalciferol Levels on SARS-CoV-2 Infection and COVID-19 Severity: A Systematic Review and Meta-Analysis. EClinicalMedicine 2021, 37, 100967. [Google Scholar] [CrossRef] [PubMed]
- Teshome, A.; Adane, A.; Girma, B.; Mekonnen, Z.A. The Impact of Vitamin D Level on COVID-19 Infection: Systematic Review and Meta-Analysis. Front. Public Health 2021, 9, 624559. [Google Scholar] [CrossRef]
- Wang, Z.; Joshi, A.; Leopold, K.; Jackson, S.; Christensen, S.; Nayfeh, T.; Mohammed, K.; Creo, A.; Tebben, P.; Kumar, S. Association of Vitamin D Deficiency with COVID-19 Infection Severity: Systematic Review and Meta-Analysis. Clin. Endocrinol. 2021, 93, 281–287. [Google Scholar] [CrossRef]
- Ben-Eltriki, M.; Hopefl, R.; Wright, J.M.; Deb, S. Association between Vitamin D Status and Risk of Developing Severe COVID-19 Infection: A Meta-Analysis of Observational Studies. J. Am. Coll. Nutr. 2021, 1–11, Ahead of print. [Google Scholar] [CrossRef]
- Ghasemian, R.; Shamshirian, A.; Heydari, K.; Malekan, M.; Alizadeh-Navaei, R.; Ebrahimzadeh, M.A.; Ebrahimi Warkiani, M.; Jafarpour, H.; Razavi Bazaz, S.; Rezaei Shahmirzadi, A.; et al. The Role of Vitamin D in the Age of COVID-19: A Systematic Review and Meta-analysis. Int. J. Clin. Pract. 2021, 75, e14675. [Google Scholar] [CrossRef]
- Sánchez-Zuno, G.A.; González-Estevez, G.; Matuz-Flores, M.G.; Macedo-Ojeda, G.; Hernández-Bello, J.; Mora-Mora, J.C.; Pérez-Guerrero, E.E.; García-Chagollán, M.; Vega-Magaña, N.; Turrubiates-Hernández, F.J.; et al. Vitamin D Levels in COVID-19 Outpatients from Western Mexico: Clinical Correlation and Effect of Its Supplementation. J. Clin. Med. 2021, 10, 2378. [Google Scholar] [CrossRef] [PubMed]
- Rastogi, A.; Bhansali, A.; Khare, N.; Suri, V.; Yaddanapudi, N.; Sachdeva, N.; Puri, G.D.; Malhotra, P. Short Term, High-Dose Vitamin D Supplementation for COVID-19 Disease: A Randomised, Placebo-Controlled, Study (SHADE Study). Postgrad. Med. J. 2020, 98, 87–90. [Google Scholar] [CrossRef] [PubMed]
- Lakkireddy, M.; Gadiga, S.G.; Malathi, R.D.; Karra, M.L.; Raju, I.S.S.V.P.M.; Ragini; Chinapaka, S.; Baba, K.S.S.S.; Kandakatla, M. Impact of Daily High Dose Oral Vitamin D Therapy on the Inflammatory Markers in Patients with COVID 19 Disease. Sci. Rep. 2021, 11, 10641. [Google Scholar] [CrossRef]
- Pal, R.; Banerjee, M.; Bhadada, S.K.; Shetty, A.J.; Singh, B.; Vyas, A. Vitamin D Supplementation and Clinical Outcomes in COVID-19: A Systematic Review and Meta-Analysis. J. Endocrinol. Investig. 2021, 45, 53–68. [Google Scholar] [CrossRef]
- da Rocha, A.P.; Atallah, A.N.; Aldrighi, J.M.; Pires, A.L.R.; dos Santos Puga, M.E.; Pinto, A.C.P.N. Insufficient Evidence for Vitamin D Use in COVID-19: A Rapid Systematic Review. Int. J. Clin. Pract. 2021, 75, e14649. [Google Scholar] [CrossRef] [PubMed]
- Stroehlein, J.K.; Wallqvist, J.; Iannizzi, C.; Mikolajewska, A.; Metzendorf, M.-I.; Benstoem, C.; Meybohm, P.; Becker, M.; Skoetz, N.; Stegemann, M.; et al. Vitamin D Supplementation for the Treatment of COVID-19: A Living Systematic Review. Cochrane Database Syst. Rev. 2021, 5, CD015043. [Google Scholar] [CrossRef] [PubMed]
- Bassatne, A.; Basbous, M.; Chakhtoura, M.; El Zein, O.; Rahme, M.; El-Hajj Fuleihan, G. The Link between COVID-19 and VItamin D (VIVID): A Systematic Review and Meta-Analysis. Metabolism 2021, 119, 154753. [Google Scholar] [CrossRef]
- Shah, K.; Saxena, D.; Mavalankar, D. Vitamin D Supplementation, COVID-19 and Disease Severity: A Meta-Analysis. QJM Int. J. Med. 2021, 114, 175–181. [Google Scholar] [CrossRef]
- Dramé, M.; Cofais, C.; Hentzien, M.; Proye, E.; Coulibaly, P.S.; Demoustier-Tampère, D.; Destailleur, M.-H.; Lotin, M.; Cantegrit, E.; Cebille, A.; et al. Relation between Vitamin D and COVID-19 in Aged People: A Systematic Review. Nutrients 2021, 13, 1339. [Google Scholar] [CrossRef]
- Petrelli, F.; Luciani, A.; Perego, G.; Dognini, G.; Colombelli, P.L.; Ghidini, A. Therapeutic and Prognostic Role of Vitamin D for COVID-19 Infection: A Systematic Review and Meta-Analysis of 43 Observational Studies. J. Steroid Biochem. Mol. Biol. 2021, 211, 105883. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Author, Date of Publication | Study Design | Treatment | Population, Male/Female Ratio, Mean Age, Baseline Vitamin D Levels (ng/mL) | ||
|---|---|---|---|---|---|
| Intervention | Control | Intervention | Control | ||
| Annweiler [28] Nov-2020 | non-randomized clinical trial | 80,000 IU oral vitamin D3 plus standard care | standard care | 16 11/5 85 (IQR = 84–89) NA | 32 19/13 88 (IQR = 84–92) NA |
| Sabico [29] Jun-2021 | randomized controlled trial | 5000 IU oral vitamin D3 | 1,000 IU oral D3 | 36 21/15 46.3 ± 15.2 21.4 ± 1.2 * | 33 13/20 53.5 ± 12.3 25.2 ± 1 * |
| Güven [30] Sep-2021 | observational | 300,000 IU of vitamin D3 IM | NA | 113 69/44 74 (IQR = 60–81) 6.65 (5.06–9.1) | 62 36/26 74 (IQR = 60–81) 7.14 (5.17–8.21) |
| Nogues [31] Sep-2021 | prospective | oral 25(OH)D3 (532 μg on day one plus 266μg on day 3, 7, 15, and 30) plus standard care | standard care | 447 264/183 61.81 ± 15.5 13 (IQR = 8–24) | 391 231/160 62.41 ± 17.2 12 (IQR = 8–19) |
| Elamir [32] Sep-2021 | randomized controlled trial | 0.5 μg 1,25(OH)2D3 daily for 14 days oral plus standard care | standard care | 25 12/13 69 ± 18 NA | 25 13/12 64 ± 16 NA |
| Entrenas-Castillo [33] Oct-2020 | randomized controlled trial | oral 25(OH)D3 (0.532 mg), oral calcifediol (0.266 mg) on day 3 and 7, and then weekly plus standard care | standard care | 50 27/23 53.14 ± 10.77 NA | 26 18/8 52.77 ± 9.35 NA |
| Alcala-Diaz [34] May-2021 | retrospective | oral 25(OH)D3 (0.532 mg), then 0.266 mg on day 3 and 7, and then weekly until discharge or ICU admission plus standard care | standard care | 79 42/37 69 ± 15 NA | 458 275/183 67 ± 16 NA |
| Murai [35] Mar-2021 | randomized controlled trial | single dose of 200,000 IU of oral vitamin D3 | placebo | 119 70/49 56.5 ± 13.8 21.2 ± 10.1 | 118 63/55 56.0 ± 15.0 20.6 ± 8.1 |
| Tan [36] Nov/Dec 2020 | retrospective | 1000 IU/d oral vitamin D3 and 150 mg/d oral magnesium, and 500 mcg/d oral vitamin B12 | NA | 17 11/6 58.4 ± 7 NA | 26 15/11 64.1 ± 7.9 NA |
| Soliman [37] Sep-2021 | prospective | vitamin D3 as a single IM (200,000 IU) injection | placebo | 40 NA 71.30 ± 4.16 10.4 ± 1.3 | 16 NA 70.19 ± 4.57 21.17 ± 3.96 |
| Jevalikar [25] Mar-2021 | prospective | median total dose of 60,000 IU oral vitamin D3 | NA | 128 NA 45.5 ± 18.2 NA | 40 NA 48.8 ± 14.7 NA |
| Author | Length of Hospital Stay (Days), Mean ± SD or Median (IQR) | ICU Admission (n/N,%) | Mechanical Ventilation (n/N,%) | All-Cause Mortality (n/N,%) | ||||
|---|---|---|---|---|---|---|---|---|
| Intervention | Control | Intervention | Control | Intervention | Control | Intervention | Control | |
| Annweiler [28] | NA | NA | all (the study recruited patients already admitted in the ICU) | NA | NA | 3/16, 19% | 10/32, 31% | |
| Sabico [29] | 6 (5–8) | 7 (0–10) | 2/36, 5.6% | 3/33, 9.1% | NA | NA | 1/36, 2.8% | 0/33, 0% |
| Güven [30] | 9 (6–16) | 9 (5–17) | all (the study recruited patients already admitted in the ICU) | 44/113, 39% | 13/62, 21% | 43/113, 38% | 30/62, 48% | |
| Nogues [31] | NA | NA | 20/447, 4.5% | 82/39, 21% | NA | NA | 21/447, 4.7% | 62/391, 16% |
| Elamir [32] | 5.5 ± 3.9 | 9.24 ± 9.4 | 5/25, 20% | 8/25, 32% | 0/25, 0% | 2/25, 8% | 0/25, 0% | 3/25, 12% |
| Entrenas-Castillo [33] | NA | NA | 1/50, 2% | 13/26, 50% | NA | NA | 0/50, 0% | 2/26, 7.7% |
| Alcala-Diaz [34] | NA | NA | NA | NA | 3/79, 3.8% | 26/458, 5.7% | 4/79, 5.1% | 90/458, 20% |
| Murai [35] | 7.0 (4.0–10.0) | 7.0 (5.0–13.0) | 16.0 % (9.9–22.5) | 21.2% (14.2–29.7) | 7.6% (3.5–13.9) | 14.4% (8.6–22.1) | 7.6% (3.5–13.9) | 5.1% (1.9–10.7) |
| Tan [36] | NA | NA | 1/17, 5.9% | 8/26, 31% | NA | NA | 0/17, 0% | 0/26, 0% |
| Soliman [37] | NA | NA | NA | NA | 14/40, 35% | 7/16, 44% | 7/40, 18% | 3/16, 19% |
| Jevalikar [25] | NA | NA | 16/128, 13% | 13/40, 33% | NA | NA | 1/128, 0.8% | 3/40, 7.5% |
| Author | MINORS Score (Out of 24) |
|---|---|
| Annweiler | 18 |
| Guven | 18 |
| Nogues | 19 |
| Alcala Diaz | 17 |
| Tan | 18 |
| Jevalikar | 22 |
| Soliman | 17 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bania, A.; Pitsikakis, K.; Mavrovounis, G.; Mermiri, M.; Beltsios, E.T.; Adamou, A.; Konstantaki, V.; Makris, D.; Tsolaki, V.; Gourgoulianis, K.; et al. Therapeutic Vitamin D Supplementation Following COVID-19 Diagnosis: Where Do We Stand?—A Systematic Review. J. Pers. Med. 2022, 12, 419. https://doi.org/10.3390/jpm12030419
Bania A, Pitsikakis K, Mavrovounis G, Mermiri M, Beltsios ET, Adamou A, Konstantaki V, Makris D, Tsolaki V, Gourgoulianis K, et al. Therapeutic Vitamin D Supplementation Following COVID-19 Diagnosis: Where Do We Stand?—A Systematic Review. Journal of Personalized Medicine. 2022; 12(3):419. https://doi.org/10.3390/jpm12030419
Chicago/Turabian StyleBania, Angelina, Konstantinos Pitsikakis, Georgios Mavrovounis, Maria Mermiri, Eleftherios T. Beltsios, Antonis Adamou, Vasiliki Konstantaki, Demosthenes Makris, Vasiliki Tsolaki, Konstantinos Gourgoulianis, and et al. 2022. "Therapeutic Vitamin D Supplementation Following COVID-19 Diagnosis: Where Do We Stand?—A Systematic Review" Journal of Personalized Medicine 12, no. 3: 419. https://doi.org/10.3390/jpm12030419
APA StyleBania, A., Pitsikakis, K., Mavrovounis, G., Mermiri, M., Beltsios, E. T., Adamou, A., Konstantaki, V., Makris, D., Tsolaki, V., Gourgoulianis, K., & Pantazopoulos, I. (2022). Therapeutic Vitamin D Supplementation Following COVID-19 Diagnosis: Where Do We Stand?—A Systematic Review. Journal of Personalized Medicine, 12(3), 419. https://doi.org/10.3390/jpm12030419