
Comparison of Adalimumab to Other Targeted Therapies in Rheumatoid Arthritis: Results from Systematic Literature Review and Meta-Analysis

 ,
, 


Abstract
:1. Introduction
2. Methods
2.1. Data Source, Studies Selection and Data Extraction
2.2. Statistical Analysis and Data Evaluations
3. Results
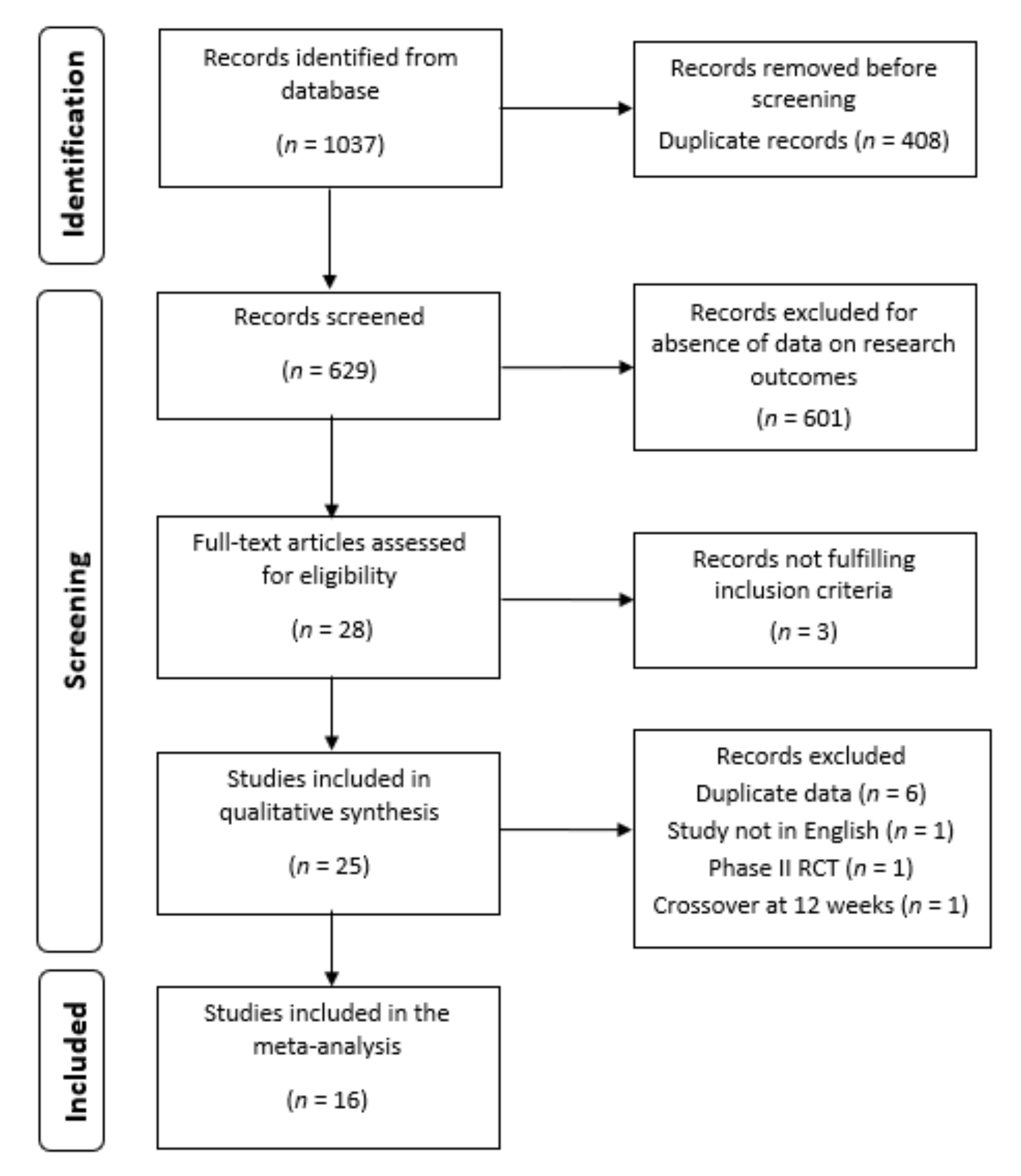
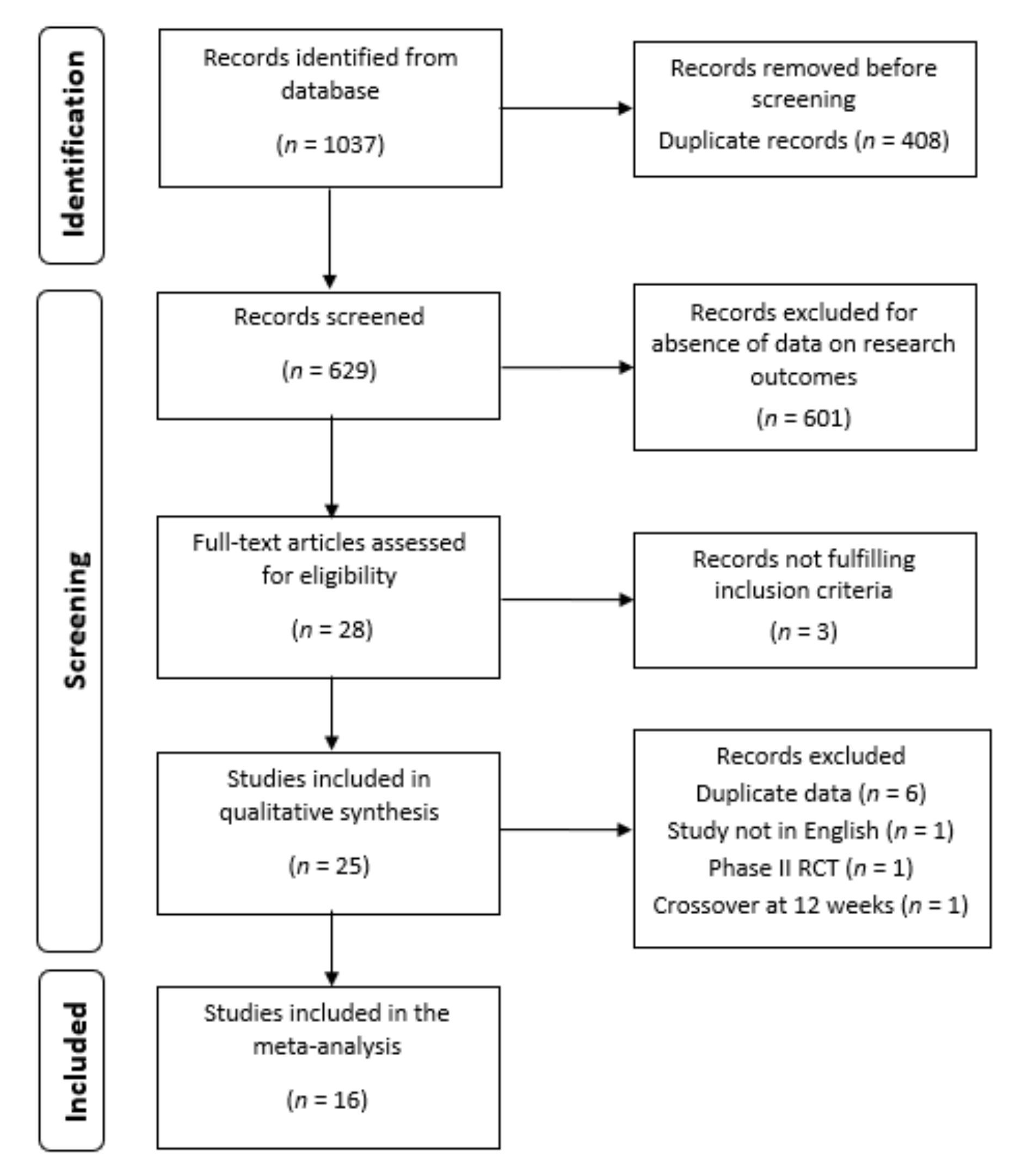
3.1. Studies Selection
3.2. Drug Efficacy and Safety Data
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Smolen, J.S.; Aletaha, D.; Barton, A.; Burmester, G.R.; Emery, P.; Firestein, G.S.; Kavanaugh, A.; McInnes, I.B.; Solomon, D.H.; Strand, V.; et al. Rheumatoid arthritis. Nat. Rev. Dis. Primer 2018, 4, 18001. [Google Scholar] [CrossRef] [PubMed]
- Burmester, G.R.; Pope, J.E. Novel treatment strategies in rheumatoid arthritis. Lancet 2017, 389, 2338–2348. [Google Scholar] [CrossRef]
- Atzeni, F.; Benucci, M.; Sallì, S.; Bongiovanni, S.; Boccassini, L.; Sarzi-Puttini, P. Different effects of biological drugs in rheumatoid arthritis. Autoimmun. Rev. 2013, 12, 575–579. [Google Scholar] [CrossRef] [PubMed]
- Silvagni, E.; Sakellariou, G.; Bortoluzzi, A.; Giollo, A.; Ughi, N.; Vultaggio, L.; Scirè, C.A. One year in review 2021: Novelties in the treatment of rheumatoid arthritis. Clin. Exp. Rheumatol. 2021, 39, 705–720. [Google Scholar]
- Smolen, J.S.; Landewé, R.B.M.; Bijlsma, J.W.J.; Burmester, G.R.; Dougados, M.; Kerschbaumer, A.; McInnes, I.B.; Sepriano, A.; Van Vollenhoven, R.F.; De Wit, M.; et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann. Rheum. Dis. 2020, 79, 685–699. [Google Scholar] [CrossRef] [Green Version]
- Favalli, E.G.; Bugatti, S.; Biggioggero, M.; Caporali, R. Treatment comparison in rheumatoid arthritis: Head-to-head trials and innovative study designs. Biomed. Res. Int. 2014, 2014, 831603. [Google Scholar] [CrossRef]
- Reddy, V.; Cohen, S. Role of Janus Kinase inhibitors in rheumatoid arthritis treatment. Curr. Opin. Rheumatol. 2021, 33, 300–306. [Google Scholar] [CrossRef]
- Venerito, V.; Lopalco, G.; Cacciapaglia, F.; Fornaro, M.; Iannone, F. A Bayesian mixed treatment comparison of efficacy of biologics and small molecules in early rheumatoid arthritis. Clin. Rheumatol. 2019, 38, 1309–1317. [Google Scholar] [CrossRef]
- Song, G.G.; Lee, Y.H. Relative efficacy and safety of secukinumab and guselkumab for the treatment of active psoriatic arthritis: A network meta-analysis. Int. J. Clin. Pharmacol. Ther. 2021, 59, 433–441. [Google Scholar] [CrossRef]
- Head, S.J.; Kaul, S.; Bogers, A.J.J.C.; Kappetein, A.P. Non-inferiority study design: Lessons to be learned from cardiovascular trials. Eur. Heart J. 2012, 33, 1318–1324. [Google Scholar] [CrossRef] [Green Version]
- Caporali, R.; Doria, A.; Ferraccioli, G.F.; Meroni, P.L.; Zavaglia, D.; Iannone, F. Unmet Needs in the Treatment of RA in the Era of Jak-i: IDRA (Italian Delphi Rheumatoid Arthritis) Consensus. BioMed Res. Int. 2018, 2018, 3878953. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Ward, M.M.; Guthrie, L.C.; Alba, M.I. Brief report: Rheumatoid arthritis response criteria and patient-reported improvement in arthritis activity: Is an American College of Rheumatology twenty percent response meaningful to patients? Arthritis Rheumatol. 2014, 66, 2339–2343. [Google Scholar] [CrossRef]
- Mack, M.E.; Hsia, E.; Aletaha, D. Comparative Assessment of the Different American College of Rheumatology/European League Against Rheumatism Remission Definitions for Rheumatoid Arthritis for Their Use as Clinical Trial End Points. Arthritis Rheumatol. 2017, 69, 518–528. [Google Scholar] [CrossRef] [Green Version]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Fleischmann, R.; Weinblatt, M.; Ahmad, H.; Maldonado, M.A.; Alemao, E.; Ye, J.; Schiff, M. Efficacy of Abatacept and Adalimumab in Patients with Early Rheumatoid Arthritis With Multiple Poor Prognostic Factors: Post Hoc Analysis of a Randomized Controlled Clinical Trial (AMPLE). Rheumatol. Ther. 2019, 6, 559–571. [Google Scholar] [CrossRef] [Green Version]
- Schiff, M.; Weinblatt, M.E.; Valente, R.; van der Heijde, D.; Citera, G.; Elegbe, A.; Maldonado, M.; Fleischmann, R. Head-to-head comparison of subcutaneous abatacept versus adalimumab for rheumatoid arthritis: Two-year efficacy and safety findings from AMPLE trial. Ann. Rheum. Dis. 2014, 73, 86–94. [Google Scholar] [CrossRef] [Green Version]
- Fleischmann, R.M.; Genovese, M.C.; Enejosa, J.V.; Mysler, E.; Bessette, L.; Peterfy, C.; Durez, P.; Ostor, A.; Li, Y.; Song, I.H. Safety and effectiveness of upadacitinib or ada-limumab plus methotrexate in patients with rheumatoid arthritis over 48 weeks with switch to alternate therapy in patients with insufficient response. Ann. Rheum. Dis. 2019, 78, 1454–1462. [Google Scholar] [CrossRef] [Green Version]
- Pavelka, K.; Szekanecz, Z.; Damjanov, N.; Anić, B.; Tomšič, M.; Mazurov, V.; Maksimovic, M.; Nagy, O.; Świerkot, J.; Petranova, T.; et al. Upadacitinib versus placebo or adalimumab with back-ground methotrexate in patients with rheumatoid arthritis and an inadequate response to methotrexate: A subgroup analysis of a phase III randomized controlled trial in Central and Eastern European patients. Drugs Context 2020, 9, 2020. [Google Scholar] [CrossRef]
- Fautrel, B.; Kirkham, B.; Pope, J.E.; Takeuchi, T.; Gaich, C.; Quebe, A.; Zhu, B.; de la Torre, I.; De Leonardis, F.; Taylor, P.C. Effect of Baricitinib and Adalimumab in Reducing Pain and Improving Function in Patients with Rheumatoid Arthritis in Low Disease Activity: Exploratory Analyses from RA-BEAM. J. Clin. Med. 2019, 8, 1394. [Google Scholar] [CrossRef] [Green Version]
- Best, J.H.; Vlad, S.C.; Pei, J. Comparative Cost per Response for 4 Clinical Endpoints with Tocilizumab Monotherapy vs. Adalimumab Monotherapy in a Head-to-Head Randomized Double-Blind Superiority Trial (ADACTA) in Patients with Rheumatoid Arthritis. Rheumatol. Ther. 2020, 7, 165–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleischmann, R.; Cutolo, M.; Genovese, M.C.; Lee, E.B.; Kanik, K.S.; Sadis, S.; Connell, C.A.; Gruben, D.; Krishnaswami, S.; Wallenstein, G.; et al. Phase IIb dose-ranging study of the oral JAK inhibitor tofacitinib (CP-690,550) or adalimumab monotherapy versus placebo in patients with active rheumatoid arthritis with an inadequate response to disease-modifying antirheumatic drugs. Arthritis Rheum. 2012, 64, 617–629. [Google Scholar] [CrossRef] [PubMed]
- Bernal Rivera, L.; Guerrero Aznar, M.D.; Monzón Moreno, A.; Beltrán García, M.; Hernández Cruz, B.; Colmenero, M.A. Effectiveness and safety of adalimumab and etanercept for rheumatoid arthritis in a third-level hospital. Farm. Hosp. 2006, 30, 223–229. [Google Scholar] [CrossRef]
- Tanaka, Y.; Fautrel, B.; Keystone, E.C.; Ortmann, R.A.; Xie, L.; Zhu, B.; Issa, M.; Patel, H.; Gaich, C.L.; de Bono, S.; et al. Clinical outcomes in patients switched from adalimumab to baricitinib due to non-response and/or study design: Phase III data in patients with rheumatoid arthritis. Ann. Rheum. Dis. 2019, 78, 890–898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jamshidi, A.; Gharibdoost, F.; Vojdanian, M.; Soroosh, S.G.; Soroush, M.; Ahmadzadeh, A.; Nazarinia, M.A.; Mousavi, M.; Karimzadeh, H.; Shakibi, M.R.; et al. A phase III, randomized, two-armed, dou-ble-blind, parallel, active controlled, and non-inferiority clinical trial to compare efficacy and safety of biosimilar adalimumab (CinnoRA®) to the reference product (Humira®) in patients with active rheumatoid arthritis. Arthritis Res. Ther. 2017, 19, 168. [Google Scholar] [CrossRef] [PubMed]
- Fleischmann, R.M.; Alten, R.; Pileckyte, M.; Lobello, K.; Hua, S.Y.; Cronenberger, C.; Alvarez, D.; Bock, A.E.; Sewell, K.L. A comparative clinical study of PF-06410293, a candidate adalimumab biosimilar, and adalimumab reference product (Humira®) in the treatment of active rheumatoid arthritis. Arthritis Res. Ther. 2018, 20, 178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Genovese, M.C.; Glover, J.; Greenwald, M.; Porawska, W.; El Khouri, E.C.; Dokoupilova, E.; Vargas, J.I.; Stanislavchuk, M.; Kellner, H.; Baranova, E.; et al. FKB327, an adalimumab biosimilar, versus the reference product: Results of a randomized, Phase III, double-blind study, and its open-label extension. Arthritis Res. Ther. 2019, 21, 281. [Google Scholar] [CrossRef] [Green Version]
- Sinha, S.; Ghosh, B.; Bandyopadhyay, S.; Fatima, F.; Bandi, V.K.; Thakur, P.; Reddy, B.; Chary, S.; Talluri, L.; Gupta, A.; et al. Comparative evaluation of efficacy, pharmacodynamics, and safety of Hetero’s adalimumab (Mabura®, Hetero Biopharma Ltd.) and reference adalimumab (Humira®, Abbvie Inc.) in patients with active rheumatoid arthritis on concomitant methotrexate therapy. BMC Rheumatol. 2020, 4, 24. [Google Scholar] [CrossRef]
- Van Vollenhoven, R.F.; Fleischmann, R.; Cohen, S.; Lee, E.B.; García Meijide, J.A.; Wagner, S.; Forejtova, S.; Zwillich, S.H.; Gruben, D.; Koncz, T.; et al. Tofacitinib or adalimumab versus placebo in rheumatoid arthritis. N. Engl. J. Med. 2012, 367, 508–519. [Google Scholar] [CrossRef] [Green Version]
- Fleischmann, R.; Mysler, E.; Hall, S.; Kivitz, A.J.; Moots, R.J.; Luo, Z.; DeMasi, R.; Soma, K.; Zhang, R.; Takiya, L.; et al. Efficacy and safety of tofacitinib monotherapy, tofacitinib with methotrexate, and adalimumab with methotrexate in patients with rheumatoid arthritis (ORAL Strategy): A phase 3b/4, double-blind, head-to-head, randomised controlled trial. Lancet 2017, 390, 457–468. [Google Scholar] [CrossRef]
- Weinblatt, M.E.; Schiff, M.; Valente, R.; van der Heijde, D.; Citera, G.; Zhao, C.; Maldonado, M.; Fleischmann, R. Head-to-head comparison of subcutaneous abatacept versus adalimumab for rheumatoid arthritis: Findings of a phase IIIb, multinational, prospective, randomized study. Arthritis Rheum. 2013, 65, 28–38. [Google Scholar] [CrossRef]
- Smolen, J.S.; Burmester, G.-R.; Combe, B.; Curtis, J.R.; Hall, S.; Haraoui, B.; van Vollenhoven, R.; Cioffi, C.; Ecoffet, C.; Gervitz, L.; et al. Head-to-head comparison of certolizumab pegol versus adalimumab in rheumatoid arthritis: 2-year efficacy and safety results from the randomised EXXELERATE study. Lancet 2016, 388, 2763–2774. [Google Scholar] [CrossRef]
- Taylor, P.C.; Keystone, E.C.; van der Heijde, D.; Weinblatt, M.E.; Del Carmen Morales, L.; Reyes Gonzaga, J.; Yakushin, S.; Ishii, T.; Emoto, K.; Beattie, S.; et al. Baricitinib versus Placebo or Adalimumab in Rheumatoid Arthritis. N. Engl. J. Med. 2017, 376, 652–662. [Google Scholar] [CrossRef]
- Fleischmann, R.; Pangan, A.L.; Song, I.-H.; Mysler, E.; Bessette, L.; Peterfy, C.; Durez, P.; Ostor, A.J.; Li, Y.; Zhou, Y.; et al. Upadacitinib Versus Placebo or Adalimumab in Patients With Rheumatoid Arthritis and an Inadequate Response to Methotrexate: Results of a Phase III, Double-Blind, Randomized Controlled Trial. Arthritis Rheumatol. 2019, 71, 1788–1800. [Google Scholar] [CrossRef]
- Combe, B.; Kivitz, A.; Tanaka, Y.; van der Heijde, D.; Simon, J.A.; Baraf, H.S.B.; Kumar, U.; Matzkies, F.; Bartok, B.; Ye, L.; et al. Filgotinib versus placebo or adalimumab in patients with rheumatoid arthritis and inadequate response to methotrexate: A phase III randomised clinical trial. Ann. Rheum. Dis. 2021, 80, 848–858. [Google Scholar] [CrossRef]
- Cohen, S.; Genovese, M.C.; Choy, E.; Perez-Ruiz, F.; Matsumoto, A.; Pavelka, K.; Pablos, J.L.; Rizzo, W.; Hrycaj, P.; Zhang, N.; et al. Efficacy and safety of the biosimilar ABP 501 compared with adalimumab in patients with moderate to severe rheumatoid arthritis: A randomised, double-blind, phase III equivalence study. Ann. Rheum. Dis. 2017, 76, 1679–1687. [Google Scholar] [CrossRef]
- Weinblatt, M.E.; Baranauskaite, A.; Niebrzydowski, J.; Dokoupilova, E.; Zielinska, A.; Jaworski, J.; Racewicz, A.; Pileckyte, M.; Jedrychowicz-Rosiak, K.; Cheong, S.Y.; et al. Phase III Randomized Study of SB5, an Adalimumab Biosimilar, Versus Reference Adalimumab in Patients With Moderate-to-Severe Rheumatoid Arthritis. Arthritis Rheumatol. 2018, 70, 40–48. [Google Scholar] [CrossRef]
- Cohen, S.B.; Alonso-Ruiz, A.; Klimiuk, P.A.; Lee, E.C.; Peter, N.; Sonderegger, I.; Assudani, D. Similar efficacy, safety and immunogenicity of adalimumab biosimilar BI 695501 and Humira reference product in patients with moderately to severely active rheumatoid arthritis: Results from the phase III randomised VOLTAIRE-RA equivalence study. Ann. Rheum. Dis. 2018, 77, 914–921. [Google Scholar] [CrossRef]
- Gabay, C.; Emery, P.; van Vollenhoven, R.; Dikranian, A.; Alten, R.; Pavelka, K.; Klearman, M.; Musselman, D.; Agarwal, S.; Green, J.; et al. Tocilizumab monotherapy versus adalimumab monotherapy for treatment of rheumatoid arthritis (ADACTA): A randomised, double-blind, controlled phase 4 trial. Lancet 2013, 381, 1541–1550. [Google Scholar] [CrossRef]
- Burmester, G.R.; Lin, Y.; Patel, R.; van Adelsberg, J.; Mangan, E.K.; Graham, N.M.H.; van Hoogstraten, H.; Bauer, D.; Ignacio Vargas, J.; Lee, E.B. Efficacy and safety of sarilumab monotherapy versus adalimumab monotherapy for the treatment of patients with active rheumatoid arthritis (MONARCH): A randomised, double-blind, parallel-group phase III trial. Ann. Rheum. Dis. 2017, 76, 840–847. [Google Scholar] [CrossRef]
- Lee, Y.H.; Song, G.G. Comparative efficacy and safety of adalimumab biosimilars and adalimumab in patients with rheumatoid arthritis presenting an insufficient response to methotrexate: A network meta-analysis. Z. Rheumatol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H.; Song, G.G. Comparative efficacy and safety of infliximab and its biosimilars in patients with rheumatoid arthritis presenting an insufficient response to methotrexate: A network meta-analysis. Z. Rheumatol. 2021. [Google Scholar] [CrossRef]
- Song, G.G.; Lee, Y.H. Comparative efficacy and safety of 100 mg and 200 mg filgotinib administered to patients with active rheumatoid arthritis: A Bayesian network meta-analysis of randomized controlled trials. Int. J. Clin. Pharmacol. Ther. 2020, 58, 293–298. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Study | Country | Tot. N. Patients | Agent | N. Patients Each Arm | ACR50 % at 24 Weeks | Drop-Out (%) | Jadad Score |
|---|---|---|---|---|---|---|---|
| Combination therapy with MTX | |||||||
| Jamshidi, 2017 [25] | Iran | 128 | ADAbio | 64 | 76.6 | 4 (6.3) | 3 |
| ADAor | 64 | 75.0 | 4 (6.3) | ||||
| Fleishmann, 2018 [26] | Worldwide | 559 | ADAbio | 286 | 56.3 | 44 (15.4) | 4 |
| ADAor | 273 | 52.7 | 78 (28.6) | ||||
| Genovese, 2019 [27] | Worldwide | 661 | ADAbio | 333 | 48.9 | 34 (10.2) | 4 |
| ADAor | 328 | 49.4 | 35 (10.7) | ||||
| Sinha, 2020 [28] | India | 159 | ADAbio | 107 | 80.4 | 5 (4.7) | 4 |
| ADAor | 52 | 80.8 | 4 (7.7) | ||||
| van Vollenhoven, 2012 [29] | Worldwide | 312 | TOFA | 150 | 40.7 | 54 (36) | 4 |
| ADAor | 162 | 32.1 | 42 (25.9) | ||||
| Fleischmann, 2017 [30] | Worldwide | 762 | TOFA | 376 | 46.0 | 73 (19.4) | 4 |
| ADAor | 386 | 43.8 | 74 (19.2) | ||||
| Weinblatt, 2013 [31] | North and South America | 594 | ABA | 296 | 41.2 | NA | 3 |
| ADAor | 298 | 39.9 | NA | ||||
| Smolen, 2016 [32] | Worldwide | 714 | CTZ | 353 | 64.0 | NA | 3 |
| ADAor | 361 | 62.6 | NA | ||||
| Taylor, 2017 [33] | Worldwide | 817 | BAR | 487 | 50.5 | 24 (4.9) | 4 |
| ADAor | 330 | 45.5 | 7 (2.1) | ||||
| Fleischmann, 2019 [34] | Worldwide | 978 | UPA | 651 | 54.1 | 20 (3.1) | 5 |
| ADAor | 327 | 41.9 | 12 (3.7) | ||||
| Combe, 2021 [35] | Worldwide | 800 | FIL | 475 | 57.9 | 50 (10.5) | 4 |
| ADAor | 325 | 53.8 | 36 (11.1) | ||||
| Monotherapy | |||||||
| Cohen, 2017 [36] | EU, North and Latin America | 496 | ADAbio | 244 | 49.2 | 21 (8.6) | 4 |
| ADAor | 252 | 52.0 | 11 (4.4) | ||||
| Weinblatt, 2018 [37] | EU | 476 | ADAbio | 239 | 38.1 | 17 (7.1) | 4 |
| ADAor | 237 | 39.7 | 19 (8) | ||||
| Cohen, 2018 [38] | Asia, EU, USA, Latin America | 593 | ADAbio | 298 | 36.9 | 26 (8.7) | 3 |
| ADAor | 295 | 35.9 | 26 (8.8) | ||||
| Gabay, 2013 [39] | North and South America, Australasia, EU | 325 | TCZ | 163 | 47.2 | 24 (14.7) | 4 |
| ADAor | 162 | 27.8 | 28 (17.3) | ||||
| Burmester, 2017 [40] | Worldwide | 369 | SARI | 184 | 45.7 | 19 (10.3) | 4 |
| ADAor | 185 | 29.7 | 28 (15.1) |
| SUCRA | |
|---|---|
| Combination therapy with MTX | |
| Upadacitinib 15 mg qd | 0.8871 |
| Baricitinib 4 mg qd | 0.5954 |
| Tofacitinib 5 mg twd | 0.5845 |
| Filgotinib 200 mg qd | 0.5431 |
| Certolizumab pegol 200 mg eow | 0.3888 |
| Abatacept 125 mg s.c. weekly | 0.3846 |
| Adalimumab biosimilar 40 mg eow | 0.3675 |
| Adalimuamb originator 40 mg eow | 0.2491 |
| Monotherapy | |
| Tocilizumab 8 mg/kg e4w | 0.8511 |
| Sarilumab 200 mg eow | 0.7497 |
| Adalimumab originator 40 mg eow | 0.2324 |
| Adalimumab biosimilar 40 mg eow | 0.1668 |
| Efficacy (ACR50 Response) | |||||||
|---|---|---|---|---|---|---|---|
| Combination therapy | |||||||
| ADAor | |||||||
| 1.05 (0.73–1.50) | ADAbio | ||||||
| 1.06 (0.56–1.97) | 1.00 (0.49–2.06) | ABA | |||||
| 1.23 (0.67–2.25) | 1.17 (0.58–2.36) | 1.16 (0.49–2.78) | BAR | ||||
| 1.06 (0.58–1.95) | 1.01 (0.50–2.06) | 1.01 (0.42–2.42) | 0.86 (0.37–2.04) | CZP | |||
| 1.21 (0.79–1.95) | 1.14 (0.66–2.10) | 1.14 (0.54–2.54 | 0.98 (0.47–2.15) | 1.14 (0.55–2.50) | TOFA | ||
| 1.64 (0.89–2.99) | 1.55 (0.77–3.15) | 1.55 (0.65–3.70) | 1.33 (0.57–3.12) | 1.54 (0.65–3.63) | 1.36 (0.62–2.80) | UPA | |
| 1.18 (0.65–2.18) | 1.12 (0.56–2.28) | 1.12 (0.47–2.68) | 0.96 (0.41–2.27) | 1.12 (0.47–2.64) | 0.98 (0.45- 2.04) | 0.72 (0.31–1.70) | FIL |
| Monotherapy | |||||||
| ADAor | |||||||
| 0.96 (0.52–1.75) | ADAbio | ||||||
| 2.35 (0.80–6.80) | 2.45 (0.71–8.43) | TCZ | |||||
| 2.00 (0.68–5.79) | 2.08 (0.61–7.08) | 0.85 (0.18–3.89) | SARI | ||||
| SAFETY (withdrawals for any adverse event) | |||||||
| Combination therapy | |||||||
| ADAor | |||||||
| 0.88 (0.62–1.20) | ADAbio | ||||||
| 0.85 (0.45–1.43) | 1.02 (0.47–1.80) | ABA | |||||
| 1.22 (0.63–2.05) | 1.44 (0.66–2.61) | 1.70 (0.62–3.18) | BAR | ||||
| 1.12 (0.60–1.86) | 1.31 (0.64–2.40) | 1.49 (0.59–3.03) | 1.03 (0.42–2.17) | CZP | |||
| 0.90 (0.57–1.38) | 1.06 (0.60–1.79) | 1.22 (0.54–2.28) | 0.83 (0.37–1.62) | 0.90 (0.40–1.78) | TOFA | ||
| 1.23 (0.66–2.05) | 1.44 (0.70–2.64) | 1.65 (0.63–3.42) | 1.13 (0.44–2.38) | 1.23 (0.50–2.54) | 1.19 (0.38–1.59) | UPA | |
| 1.20 (0.64–2.01) | 1.42 (0.68–2.62) | 1.63 (0.63–3.20) | 1.11 (0.44–2.31) | 1.19 (0.49–2.38) | 1.40 (0.63–2.63) | 1.11 (0.43–2.29) | FIL |
| Monotherapy | |||||||
| ADAor | |||||||
| 0.91 (0.49–1.53) | ADAbio | ||||||
| 1.10 (0.32–2.64) | 1.42 (0.32–3.59) | TCZ | |||||
| 1.20 (0.39–2.71) | 1.51 (0.37–3.71) | 1.70 (0.26–4.74) | SARI | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cacciapaglia, F.; Venerito, V.; Stano, S.; Fornaro, M.; Lopalco, G.; Iannone, F. Comparison of Adalimumab to Other Targeted Therapies in Rheumatoid Arthritis: Results from Systematic Literature Review and Meta-Analysis. J. Pers. Med. 2022, 12, 353. https://doi.org/10.3390/jpm12030353
Cacciapaglia F, Venerito V, Stano S, Fornaro M, Lopalco G, Iannone F. Comparison of Adalimumab to Other Targeted Therapies in Rheumatoid Arthritis: Results from Systematic Literature Review and Meta-Analysis. Journal of Personalized Medicine. 2022; 12(3):353. https://doi.org/10.3390/jpm12030353
Chicago/Turabian StyleCacciapaglia, Fabio, Vincenzo Venerito, Stefano Stano, Marco Fornaro, Giuseppe Lopalco, and Florenzo Iannone. 2022. "Comparison of Adalimumab to Other Targeted Therapies in Rheumatoid Arthritis: Results from Systematic Literature Review and Meta-Analysis" Journal of Personalized Medicine 12, no. 3: 353. https://doi.org/10.3390/jpm12030353
APA StyleCacciapaglia, F., Venerito, V., Stano, S., Fornaro, M., Lopalco, G., & Iannone, F. (2022). Comparison of Adalimumab to Other Targeted Therapies in Rheumatoid Arthritis: Results from Systematic Literature Review and Meta-Analysis. Journal of Personalized Medicine, 12(3), 353. https://doi.org/10.3390/jpm12030353