
Vulnerability of β-Thalassemia Heterozygotes to COVID-19: Results from a Cohort Study

 ,
,  , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Methods
2.1. Settings
2.2. Participants and Study Design
2.3. Ethical Considerations
2.4. Sample Estimation
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 8 January 2022).
- Ramírez-Soto, M.C.; Arroyo-Hernández, H.; Ortega-Cáceres, G. Sex differences in the incidence, mortality, and fatality of COVID-19 in Peru. PLoS ONE 2021, 16, e0253193. [Google Scholar] [CrossRef] [PubMed]
- Shakor, J.K.; Isa, R.A.; Babakir-Mina, M.; Ali, S.I.; Hama-Soor, T.A.; Abdulla, J.E. Health related factors contributing to COVID-19 fatality rates in various communities across the world. J. Infect. Dev. Ctries 2021, 15, 1263–1272. [Google Scholar] [CrossRef] [PubMed]
- Seong, G.M.; Baek, A.R.; Baek, M.S.; Kim, W.Y.; Kim, J.H.; Lee, B.Y.; Na, Y.S.; Lee, S.I. Comparison of Clinical Characteristics and Outcomes of Younger and Elderly Patients with Severe COVID-19 in Korea: A Retrospective Multicenter Study. J. Pers. Med. 2021, 11, 1258. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.D.; Ding, M.; Dong, X.; Zhang, J.J.; Kursat Azkur, A.; Azkur, D.; Gan, H.; Sun, Y.L.; Fu, W.; Li, W.; et al. Risk factors for severe and critically ill COVID-19 patients: A review. Allergy 2021, 76, 428–455. [Google Scholar] [CrossRef] [PubMed]
- Whetheral, D.J. The thalassemias. In Williams Hematology, 5th ed.; Beutler, E., Lichtman, M.A., Coller, B.S., Kipps, T.J., Eds.; McGraw-Hill: New York, NY, USA, 1995. [Google Scholar]
- Sotiriou, S.; Samara, A.A.; Vamvakopoulou, D.; Vamvakopoulos, K.-O.; Sidiropoulos, A.; Vamvakopoulos, N.; Janho, M.B.; Gourgoulianis, K.I.; Boutlas, S. Susceptibility of β-thalassemia heterozygotes to COVID-19. J. Clin. Med. 2021, 10, 3645. [Google Scholar] [CrossRef] [PubMed]
- Dean, A.; Arner, T.; Sunki, G.; Friedman, R.; Lantinga, M.; Sangam, S.; Zubieta, J.C.; Sullivan, K.M.; Brendel, K.A.; Gao, Z.; et al. Epi Info. (TM), a Database and Statistics Program for Public Health Professionals, 7.2.3.1 ed.; CDC: Atlanta, GA, USA, 2011. [Google Scholar]
- Cho, K.H.; Kim, S.W.; Park, J.W.; Do, J.Y.; Kang, S.H. Effect of Sex on Clinical Outcomes in Patients with Coronavirus Disease: A Population-Based Study. J. Clin. Med. 2020, 10, 38. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, J.; Du, K.Y.; Peng, C. Incidence, clinical features, and outcomes of COVID-19 in Canada: Impact of sex and age. J. Ovarian Res. 2020, 13, 137. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Jiang, N.; Li, C.; Wang, J.; Yang, H.; Liu, L.; Tan, X.; Chen, Z.; Gong, Y.; Yin, X.; et al. Sex-Disaggregated Data on Clinical Characteristics and Outcomes of Hospitalized Patients With COVID-19: A Retrospective Study. Front. Cell. Infect. Microbiol. 2021, 11, 680422. [Google Scholar] [CrossRef] [PubMed]
- Peckham, H.; de Gruijter, N.M.; Raine, C.; Radziszewska, A.; Ciurtin, C.; Wedderburn, L.R.; Rosser, E.C.; Webb, K.; Deakin, C.T. Male sex identified by global COVID-19 meta-analysis as a risk factor for death and ITU admission. Nat. Commun. 2020, 11, 6317. [Google Scholar] [CrossRef] [PubMed]
- Seltzer, S. Linking ACE2 and angiotensin II to pulmonary immunovascular dysregulation in SARS-CoV-2 infection. Int. J. Infect. Dis. 2020, 101, 42–45. [Google Scholar] [CrossRef] [PubMed]
- Galanello, R.; Origa, R. Beta-thalassemia. Orphanet J. Rare Dis. 2010, 5, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karimi, M.; Haghpanah, S.; Zarei, T.; Azarkeivan, A.; Shirkavand, A.; Matin, S.; Tavakoli, M.A.; Zahedi, Z.; De Sanctis, V. Prevalence and severity of Coronavirus disease 2019 (COVID-19) in Transfusion Dependent and Non-Transfusion Dependent β-thalassemia patients and effects of associated comorbidities: An Iranian nationwide study. Acta Biomed. 2020, 91, e2020007. [Google Scholar] [CrossRef] [PubMed]
- Karimi, M.; Haghpanah, S.; Azarkeivan, A.; Zahedi, Z.; Zarei, T.; Akhavan Tavakoli, M.; Bazrafshan, A.; Shirkavand, A.; De Sanctis, V. Prevalence and mortality in β-thalassaemias due to outbreak of novel coronavirus disease (COVID-19): The nationwide Iranian experience. Br. J. Haematol. 2020, 190, e137–e140. [Google Scholar] [CrossRef] [PubMed]
- Ondei, L.D.S.; Estevão, I.D.F.; Rocha, M.I.P.; Percário, S.; Souza, D.R.S.; Pinhel, M.A.D.S.; Bonini-Domingos, C.R. Oxidative stress and antioxidant status in beta-thalassemia heterozygotes. Rev. Bras. Hematol. Hemoter. 2013, 35, 409–413. [Google Scholar] [CrossRef] [PubMed]
- Chung, M.K.; Zidar, D.A.; Bristow, M.R.; Cameron, S.J.; Chan, T.; Harding, C.V., III; Kwon, D.H.; Singh, T.; Tilton, J.C.; Tsai, E.J.; et al. COVID-19 and Cardiovascular Disease. Circ. Res. 2021, 128, 1214–1236. [Google Scholar] [CrossRef] [PubMed]
- Li, X.C.; Zhang, J.; Zhuo, J.L. The vasoprotective axes of the renin-angiotensin system: Physiological relevance and therapeutic implications in cardiovascular, hypertensive and kidney diseases. Pharmacol. Res. 2017, 125, 21–38. [Google Scholar] [CrossRef] [PubMed]
- Aleksova, A.; Gagno, G.; Sinagra, G.; Beltrami, A.; Janjusevic, M.; Ippolito, G.; Zumla, A.; Fluca, A.; Ferro, F. Effects of SARS-CoV-2 on Cardiovascular System: The Dual Role of Angiotensin-Converting Enzyme 2 (ACE2) as the Virus Receptor and Homeostasis Regulator-Review. Int. J. Mol. Sci. 2021, 22, 4526. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Outcome: Mortality | Univariate | Multivariate Binary Logistic Regression | |||||
|---|---|---|---|---|---|---|---|
| Yes (%) | Sig. | OR with 95% CI | RR with 95% CI | Sig. | aOR with 95% CI | ||
| Sex (M/F) | M: F: | 140 (31.3) 49 (15.7) | <0.001 (C) | 2.44 (1.69–3.51) | 1.99 (1.49–2.66) | <0.001 (C) | 2.59 (1.73–3.90) |
| Age (median, IQR) | Dead: 73 (16) Alive: 62 (23) | <0.001 (M–W) | - | - | <0.001 (C) | 1.049 (1.031–1.066) | |
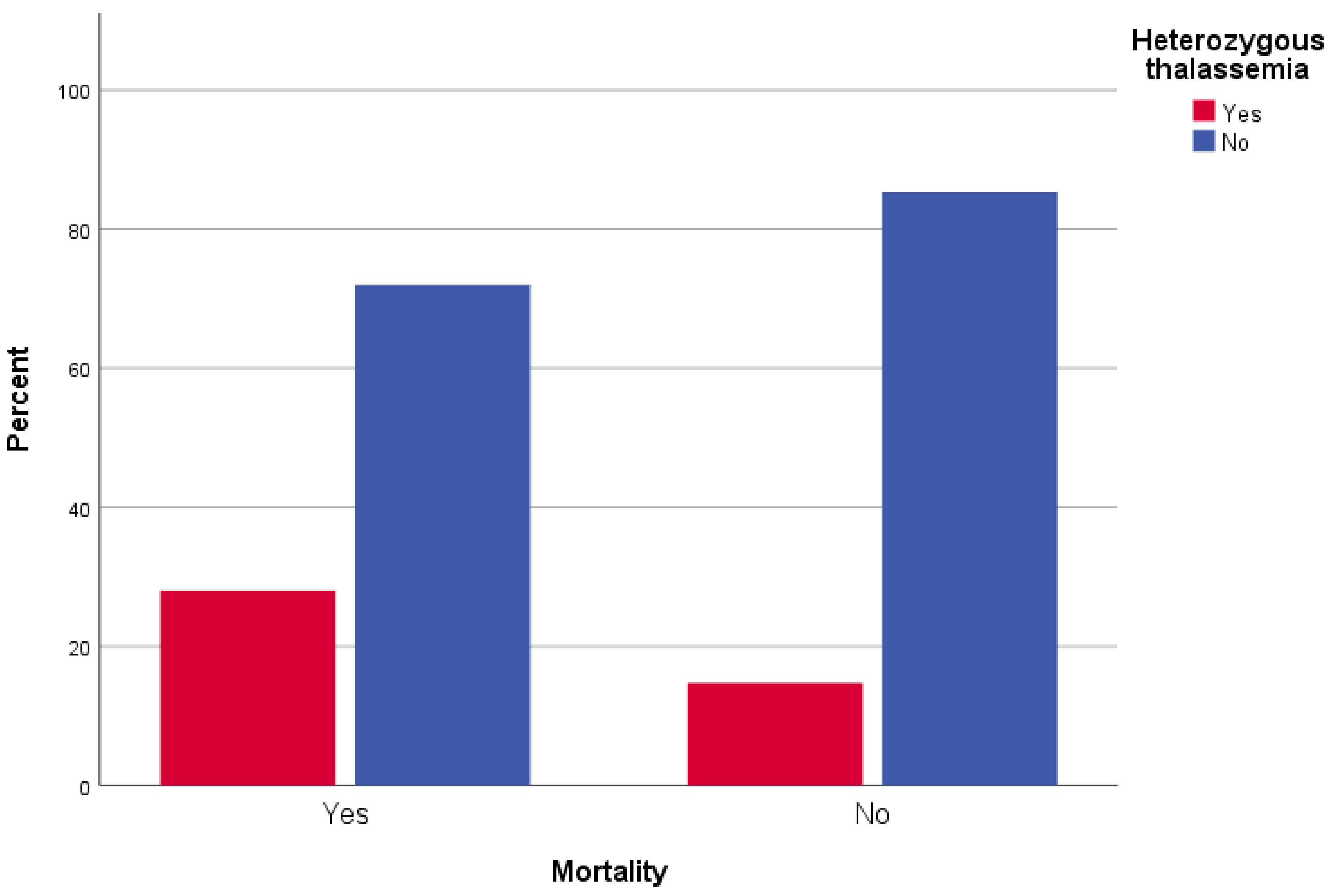
| β-Thalassemia heterozygosity | Yes: No: | 53 (38.7) 136 (21.8) | <0.001 (C) | 2.26 (1.53–3.35) | 1.77 (1.37–2.29) | 0.001 | 2.41 (1.55–3.74) |
| Chronic respiratory disease | Yes: No: | 41 (43.6) 148 (22.2) | <0.001 (C) | 2.71 (1.73–4.23) | 1.96 (1.50–2.57) | 0.018 | 1.84 (1.11–3.05) |
| Atrial fibrillation | Yes: No: | 84 (37.0) 103 (19.4) | <0.001 (C) | 2.44 (1.73–3.45) | 1.91 (1.50–2.43) | 0.058 | 1.50 (0.99– 2.28) |
| Hypertension | Yes: No: | 138 (32.9) 51 (15.0) | <0.001 (C) | 2.77 (1.93–3.98) | 2.19 (1.64–2.92) | 0.243 | 1.31 (0.83–2.04) |
| Coronary disease | Yes: No: | 53 (37.3) 136 (22.0) | <0.001 (C) | 2.11 (1.43–3.12) | 1.70 (1.31–2.20) | 0.617 | 0.89 (0.55–1.42) |
| Diabetes mellitus type II | Yes: No: | 48 (30.8) 141 (23.3) | 0.056 (C) | 1.46 (0.99–2.15) | 1.32 (1.00–1.74) | 0.439 | 0.84 (0.54–1.30) |
| Neoplasia | Yes: No: | 27 (31.8) 162 (24.1) | 0.122 (C) | 1.47 (0.90–2.40) | 1.32 (0.94–1.85) | 0.653 | 0.88 (0.52–1.51) |
| Outcome: Severity | Univariate | Multivariate Ordinal Logistic Regression | ||||
|---|---|---|---|---|---|---|
| Asymptomatic-Mild (%) | Moderate (%) | Severe-Critical (%) | Sig. | Sig. | aOR with 95% CI | |
| Sex (Male) | 94 (49.5) | 210 (56.3) | 144 (73.1) | <0.001 (C) | <0.001 | 1.98 (1.47–2.66) |
| Age (median, IQR) | 52 (32) | 65 (18) | 72 (16) | <0.001 (Κ–W) | <0.001 | 1.052 (1.040–1.064) |
| Atrial Fibrillation | 51 (26.8) | 93 (24.9) | 83 (42.6) | <0.001 (C) | 0.373 | 0.85 (0.60–1.21) |
| Chronic respiratory disease | 15 (7.9) | 38 (10.2) | 41 (20.8) | <0.001 (C) | 0.098 | 1.45 (0.93–2.26) |
| Coronary disease | 20 (10.5) | 69 (18.5) | 53 (26.9) | <0.001 (C) | 0.634 | 1.10 (0.73–1.67) |
| Diabetes mellitus Type II | 29 (15.3) | 79 (21.2) | 48 (24.4) | 0.078 (C) | 0.331 | 0.83 (0.58–1.20) |
| Neoplasia | 20 (10.5) | 35 (9.4) | 30 (15.2) | 0.108 (C) | 0.173 | 0.73 (0.47–1.15) |
| Hypertension | 69 (36.3) | 204 (54.7) | 147 (74.6) | <0.001 (C) | 0.104 | 1.34 (0.94–1.91) |
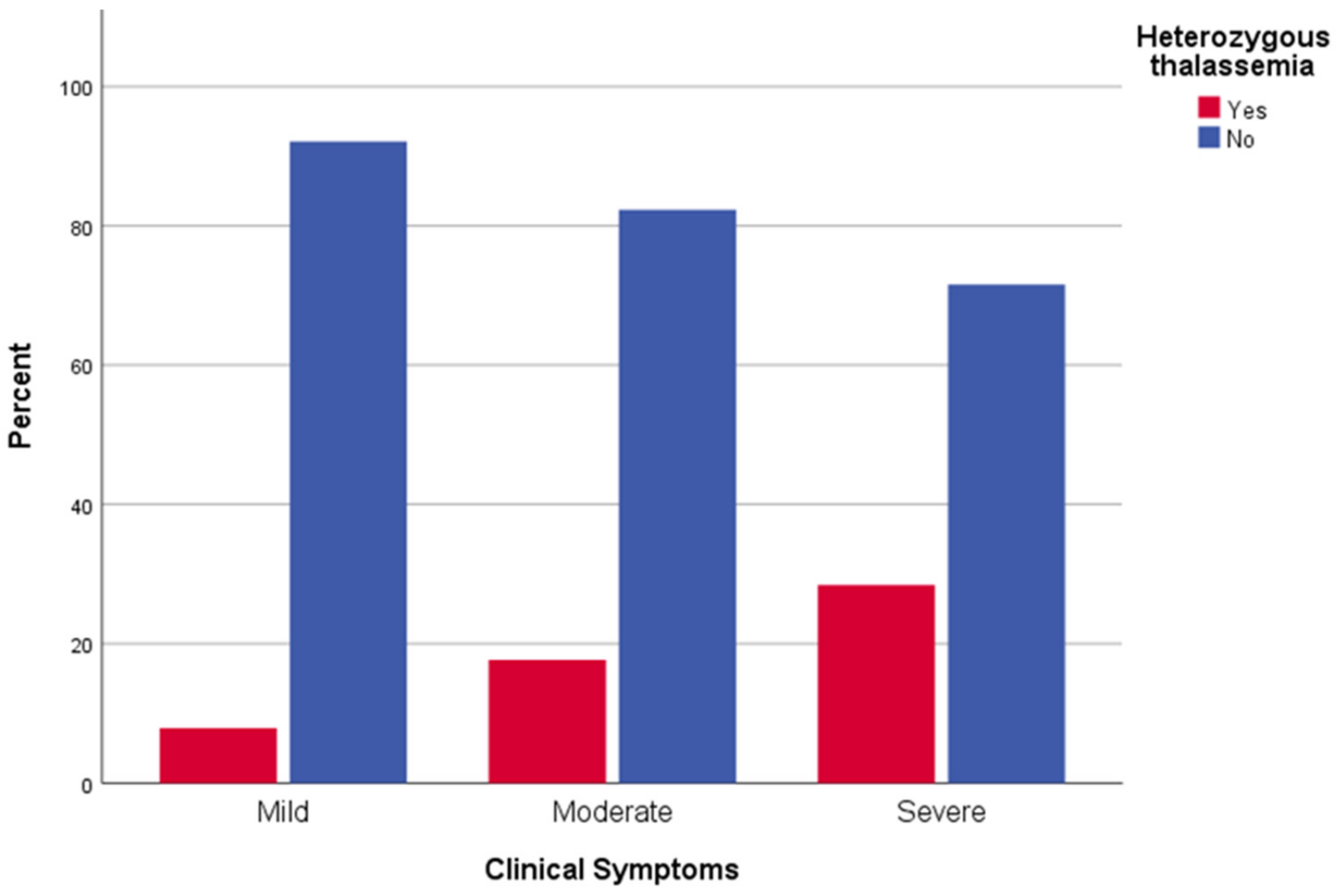
| β-Thalassemia heterozygosity | 15 (7.9) | 66 (17.7) | 56 (28.4) | <0.001 (C) | <0.001 | 2.59 (1.78–3.77) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sotiriou, S.; Samara, A.A.; Lachanas, K.E.; Vamvakopoulou, D.; Vamvakopoulos, K.-O.; Vamvakopoulos, N.; Janho, M.B.; Perivoliotis, K.; Donoudis, C.; Daponte, A.; et al. Vulnerability of β-Thalassemia Heterozygotes to COVID-19: Results from a Cohort Study. J. Pers. Med. 2022, 12, 352. https://doi.org/10.3390/jpm12030352
Sotiriou S, Samara AA, Lachanas KE, Vamvakopoulou D, Vamvakopoulos K-O, Vamvakopoulos N, Janho MB, Perivoliotis K, Donoudis C, Daponte A, et al. Vulnerability of β-Thalassemia Heterozygotes to COVID-19: Results from a Cohort Study. Journal of Personalized Medicine. 2022; 12(3):352. https://doi.org/10.3390/jpm12030352
Chicago/Turabian StyleSotiriou, Sotirios, Athina A. Samara, Konstantinos E. Lachanas, Dimitra Vamvakopoulou, Konstantinos-Odysseas Vamvakopoulos, Nikolaos Vamvakopoulos, Michel B. Janho, Konstantinos Perivoliotis, Christos Donoudis, Alexandros Daponte, and et al. 2022. "Vulnerability of β-Thalassemia Heterozygotes to COVID-19: Results from a Cohort Study" Journal of Personalized Medicine 12, no. 3: 352. https://doi.org/10.3390/jpm12030352
APA StyleSotiriou, S., Samara, A. A., Lachanas, K. E., Vamvakopoulou, D., Vamvakopoulos, K.-O., Vamvakopoulos, N., Janho, M. B., Perivoliotis, K., Donoudis, C., Daponte, A., Gourgoulianis, K. I., & Boutlas, S. (2022). Vulnerability of β-Thalassemia Heterozygotes to COVID-19: Results from a Cohort Study. Journal of Personalized Medicine, 12(3), 352. https://doi.org/10.3390/jpm12030352