
Short- and Long-Term Outcomes of Left Main Coronary Artery Stenting in Patients Disqualified from Coronary Artery Bypass Graft Surgery


 , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
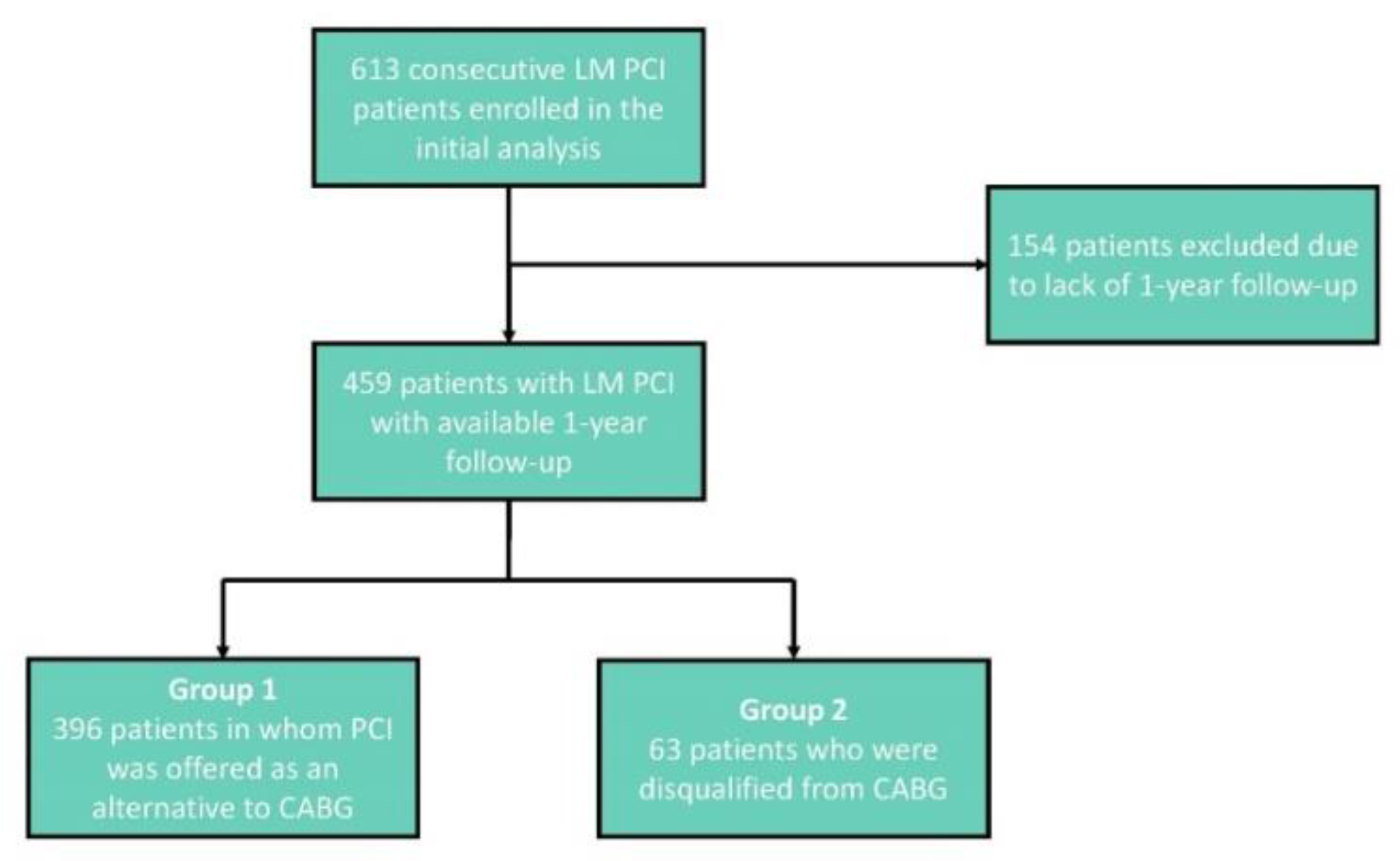
2.1. Study Population
2.2. Study Procedures
2.3. Study Endpoints
2.4. Statistical Analysis
3. Results
3.1. Study Population
3.2. CAD Characteristics
3.3. LM PCI Procedure
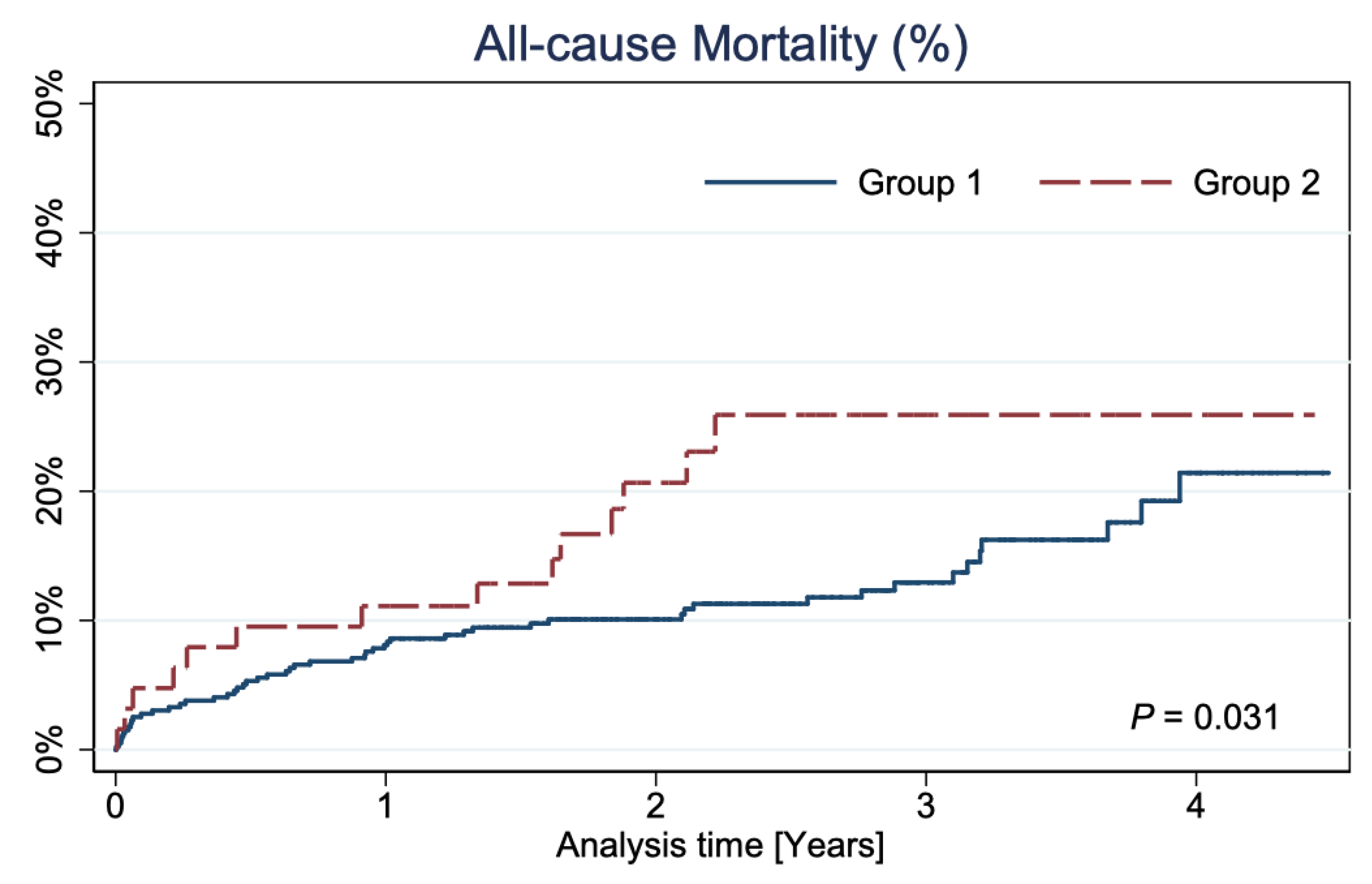
3.4. Clinical Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sianos, G.; Morel, M.-A.; Kappetein, A.P.; Morice, M.-C.; Colombo, A.; Dawkins, K.; Brand, M.V.D.; Van Dyck, N.; Russell, M.E.; Mohr, F.W.; et al. The SYNTAX Score: An angiographic tool grading the complexity of coronary artery disease. EuroIntervention 2005, 1, 219–227. [Google Scholar] [PubMed]
- El-Menyar, A.A.; Al Suwaidi, J.; Holmes, D.R. Left Main Coronary Artery Stenosis: State-of-the-Art. Curr. Probl. Cardiol. 2007, 32, 103–193. [Google Scholar] [CrossRef] [PubMed]
- Hitchcock, J.F.; Robles de Medina, E.O.; Jambroes, G. Angioplasty of the left main coronary artery for isolated left main coronary artery disease. J. Thorac. Cardiovasc. Surg. 1983, 85, 880–884. [Google Scholar] [CrossRef]
- Conley, M.J.; Ely, R.L.; Kisslo, J.; Lee, K.L.; McNeer, J.F.; Rosati, R.A. The prognostic spectrum of left main stenosis. Circulation 1978, 57, 947–952. [Google Scholar] [CrossRef] [Green Version]
- Herrick, J.B. Clinical features of sudden obstruction of the coronary arteries. J. Am. Med. Assoc. 1912, 23, 2015–2022. [Google Scholar] [CrossRef] [Green Version]
- Favaloro, R.G. Saphenous Vein Autograft Replacement of Severe Segmental Coronary Artery Occlusion: Operative Technique. Ann. Thorac. Surg. 1968, 5, 334–339. [Google Scholar] [CrossRef]
- Killip, T.; Passamani, E.; Davis, K. Coronary Artery Surgery study (CASS): A randomized trial of coronary artery bypass surgery. Surviv. Data Circ. 1983, 68, 939–950. [Google Scholar]
- Group ECSS. Long-term results of prospective randomized study or coronary artery bypass surgery in stable angina pectoris. Lancet 1982, 2, 1173–1180. [Google Scholar]
- Yusuf, S.; Zucker, D.; Passamani, E.; Peduzzi, P.; Takaro, T.; Fisher, L.; Kennedy, J.; Davis, K.; Killip, T.; Norris, R.; et al. Effect of coronary artery bypass graft surgery on survival: Overview of 10-year results from randomised trials by the Coronary Artery Bypass Graft Surgery Trialists Collaboration. Lancet 1994, 344, 563–570. [Google Scholar] [CrossRef]
- Morice, M.-C.; Serruys, P.W.; Kappetein, A.P.; Feldman, T.E.; Ståhle, E.; Colombo, A.; Mack, M.J.; Holmes, D.R.; Torracca, L.; van Es, G.-A.; et al. Outcomes in patients with de novo left main disease treated with either percutaneous coronary intervention using paclitaxel-eluting stents or coronary artery bypass graft treatment in the Synergy Between Percutaneous Coronary Intervention with TAXUS and Cardiac Surgery (SYNTAX) trial. Circulation 2010, 121, 2645–2653. [Google Scholar]
- Park, S.-J.; Kim, Y.-H.; Park, D.-W.; Yun, S.-C.; Ahn, J.-M.; Song, H.G.; Lee, J.-Y.; Kim, W.-J.; Kang, S.-J.; Lee, S.-W.; et al. Randomized trial of stents versus bypass surgery for left main coronary artery disease. N. Engl. J. Med. 2011, 364, 1718–1727. [Google Scholar] [CrossRef] [PubMed]
- Rab, T.; Sheiban, I.; Louvard, Y.; Sawaya, F.J.; Zhang, J.J.; Chen, S.L. Current Interventions for the Left Main Bifurcation. JACC Cardiovasc. Interv. 2017, 10, 849–865. [Google Scholar] [CrossRef] [PubMed]
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2018, 40, 87–165. [Google Scholar] [CrossRef] [PubMed]
- Morice, M.-C.; Serruys, P.W.; Kappetein, A.P.; Feldman, T.E.; Ståhle, E.; Colombo, A.; Mack, M.J.; Holmes, D.R.; Choi, J.W.; Ruzyllo, W.; et al. Five-Year Outcomes in Patients With Left Main Disease Treated with Either Percutaneous Coronary Intervention or Coronary Artery Bypass Grafting in the Synergy Between Percutaneous Coronary Intervention with Taxus and Cardiac Surgery Trial. Circulation 2014, 129, 2388–2394. [Google Scholar] [CrossRef] [Green Version]
- Ahn, J.M.; Roh, J.H.; Kim, Y.H.; Park, D.W.; Yun, S.C.; Lee, P.H.; Chang, M.; Park, H.W.; Lee, S.W.; Lee, C.W.; et al. Randomized Trial of Stents Versus Bypass Surgery for Left Main Coronary Artery Disease: 5-Year Outcomes of the PRECOMBAT Study. J. Am. Coll. Cardiol. 2015, 65, 2198–2206. [Google Scholar] [CrossRef] [Green Version]
- Stone, G.W.; Sabik, J.F.; Serruys, P.W.; Simonton, C.A.; Généreux, P.; Puskas, J.; Kandzari, D.E.; Morice, M.-C.; Lembo, N.; Brown, W.M.; et al. Everolimus-eluting stents or bypass surgery for left main coronary artery disease. N. Engl. J. Med. 2016, 375, 2223–2235. [Google Scholar] [CrossRef]
- Mäkikallio, T.; Holm, N.; Lindsay, M.; Spence, M.S.; Erglis, A.; Menown, I.B.A.; Trovik, T.; Eskola, M.; Romppanen, H.; Kellerth, T.; et al. Percutaneous coronary angioplasty versus coronary artery bypass grafting in treatment of unprotected left main stenosis (NOBLE): A prospective, randomised, open-label, non-inferiority trial. Lancet 2016, 388, 2743–2752. [Google Scholar] [CrossRef] [Green Version]
- Medina, A.; Suarez de Lezo, J.; Pan, M. A new classification of coronary bifurcation lesions. Rev. Esp. Cardiol. 2006, 59, 183. [Google Scholar] [CrossRef] [Green Version]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D.; Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction. Fourth Universal Definition of Myocardial Infarction (2018). J. Am. Coll. Cardiol. 2018, 72, 2231–2264. [Google Scholar] [CrossRef]
- Siersbæk-Nielsen, K.; Molholm Hansen, J.; Kampmann, J.; Kristensen, M. Rapid Evaluation of Creatinine Clearance. Lancet 1971, 297, 1133–1134. [Google Scholar] [CrossRef]
- Ben-Yehuda, O.; Chen, S.; Redfors, B.; McAndrew, T.; Crowley, A.; Kosmidou, I.; Kandzari, D.E.; Puskas, J.D.; Morice, M.-C.; Taggart, D.P.; et al. Impact of large periprocedural myocardial infarction on mortality after percutaneous coronary intervention and coronary artery bypass grafting for left main disease: An analysis from the EXCEL trial. Eur. Heart J. 2019, 40, 1930–1941. [Google Scholar] [CrossRef] [PubMed]
- Buszman, P.E.; Buszman, P.P.; Kiesz, R.S.; Bochenek, A.; Trela, B.; Konkolewska, M.; Wallace-Bradley, D.; Wilczyński, M.; Banasiewicz-Szkróbka, I.; Peszek-Przybyla, E.; et al. Early and Long-Term Results of Unprotected Left Main Coronary Artery Stenting. J. Am. Coll. Cardiol. 2009, 54, 1500–1511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, D.-W.; Kim, Y.-H.; Yun, S.-C.; Lee, J.-Y.; Kim, W.-J.; Kang, S.-J.; Lee, S.-W.; Lee, C.-W.; Kim, J.-J.; Choo, S.-J.; et al. Long-term outcomes after stenting versus coronary artery bypass grafting for unprotected left main coronary artery disease: 10-year results of bare-metal stents and 5-year results of drug-eluting stents from the ASAN-MAIN (ASAN Medical Center-Left MAIN Revascularization) Registry. J. Am. Coll. Cardiol. 2010, 56, 1366–1375. [Google Scholar] [PubMed] [Green Version]
- Chieffo, A.; Tanaka, A.; Giustino, G.; Briede, I.; Sawaya, F.J.; Daemen, J.; Kawamoto, H.; Meliga, E.; D’Ascenzo, F.; Cerrato, E.; et al. The DELTA 2 Registry. JACC Cardiovasc. Interv. 2017, 10, 2401–2410. [Google Scholar] [CrossRef] [PubMed]
- Lu, T.-M.; Lee, W.-L.; Hsu, P.-F.; Lin, T.-C.; Sung, S.-H.; Wang, K.-L.; Huang, S.-S.; Chan, W.-L.; Shih, C.-C.; Lin, S.-J.; et al. Long-term results of stenting versus coronary artery bypass surgery for left main coronary artery disease—A single-center experience. J. Chin. Med. Assoc. 2016, 79, 356–362. [Google Scholar] [CrossRef] [Green Version]
- Park, D.-W.; Seung, K.B.; Kim, Y.-H.; Lee, J.-Y.; Kim, W.-J.; Kang, S.-J.; Lee, S.-W.; Lee, C.W.; Park, S.-W.; Yun, S.-C.; et al. Long-Term Safety and Efficacy of Stenting Versus Coronary Artery Bypass Grafting for Unprotected Left Main Coronary Artery Disease. J. Am. Coll. Cardiol. 2010, 56, 117–124. [Google Scholar] [CrossRef] [Green Version]
- Lee, P.H.; Ahn, J.M.; Chang, M.; Baek, S.; Yoon, S.H.; Kang, S.J.; Lee, S.W.; Kim, Y.H.; Lee, C.W.; Park, S.W.; et al. Left Main Coronary Artery Disease. J. Am. Coll. Cardiol. 2016, 68, 1233–1246. [Google Scholar] [CrossRef]
- Fajadet, J.; Capodanno, D.; Stone, G.W. Management of left main disease: An update. Eur. Heart J. 2019, 40, 1454–1466. [Google Scholar] [CrossRef] [Green Version]
- Burzotta, F.; Lassen, J.F.; Banning, A.; Lefèvre, T.; Hildick-Smith, D.; Chieffo, A.; Darremont, O.; Pan, M.; Chatzizisis, Y.S.; Albiero, R.; et al. Percutaneous coronary intervention in left main coronary artery disease: The 13th consensus document from the European Bifurcation Club. EuroIntervention 2018, 14, 112–120. [Google Scholar] [CrossRef]
- Kang, D.-Y.; Ahn, J.-M.; Yun, S.-C.; Park, H.; Cho, S.-C.; Kim, T.O.; Park, S.; Lee, P.H.; Lee, S.-W.; Park, S.-W.; et al. Long-Term Clinical Impact of Intravascular Ultrasound Guidance in Stenting for Left Main Coronary Artery Disease. Circ. Cardiovasc. Interv. 2021, 14, e011011. [Google Scholar] [CrossRef]
- Kim, W.-J.; Kim, Y.-H.; Park, D.-W.; Yun, S.-C.; Lee, J.-Y.; Kang, S.-J.; Lee, S.-W.; Lee, C.W.; Park, S.-W.; Park, S.-J. Comparison of single-versus two-stent techniques in treatment of unprotected left main coronary bifurcation disease. Catheter. Cardiovasc. Interv. 2011, 77, 775–782. [Google Scholar] [CrossRef]
- Choi, K.H.; Bin Song, Y.; Lee, J.M.; Park, T.K.; Yang, J.H.; Hahn, J.-Y.; Choi, J.-H.; Choi, S.-H.; Kim, H.-S.; Chun, W.J.; et al. Prognostic effects of treatment strategies for left main versus non-left main bifurcation percutaneous coronary intervention with current-generation drug-eluting stent. Circ. Cardiovasc. Interv. 2020, 13, e008543. [Google Scholar] [CrossRef]
- Zhang, J.-J.; Ye, F.; Xu, K.; Kan, J.; Tao, L.; Santoso, T.; Munawar, M.; Tresukosol, D.; Li, L.; Sheiban, I.; et al. Multicentre, randomized comparison of two-stent and provisional stenting techniques in patients with complex coronary bifurcation lesions: The DEFINITION II trial. Eur. Heart J. 2020, 41, 2523–2536. [Google Scholar] [CrossRef]
- Chen, S.L.; Xu, B.; Han, Y.L.; Sheiban, I.; Zhang, J.J.; Ye, F.; Kwan, T.W.; Paiboon, C.; Zhou, Y.J.; Lv, S.Z.; et al. Comparison of double kissing crush versus Culotte stenting for unprotected distal left main bifurcation lesions: Results from a multicenter, randomized, prospective DKCRUSH-III study. J. Am. Coll. Cardiol. 2013, 61, 1482–1488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hildick-Smith, D.; Egred, M.; Banning, A.; Brunel, P.; Ferenc, M.; Hovasse, T.; Wlodarczak, A.; Pan, M.; Schmitz, T.; Silvestri, M.; et al. The European bifurcation club Left Main Coronary Stent study: A randomized comparison of stepwise provisional vs. systematic dual stenting strategies (EBC MAIN). Eur. Heart J. 2021, 42, 3829–3839. [Google Scholar] [CrossRef] [PubMed]
- Suh, J.; Park, D.W.; Lee, J.Y.; Jung, I.H.; Lee, S.W.; Kim, Y.H.; Lee, C.W.; Cheong, S.S.; Kim, J.J.; Park, S.W.; et al. The Relationship and Threshold of Stent Length With Regard to Risk of Stent Thrombosis after Drug-Eluting Stent Implantation. JACC Cardiovasc. Interv. 2010, 3, 383–389. [Google Scholar] [CrossRef] [Green Version]
- Kandzari, D.E.; Gershlick, A.H.; Serruys, P.W.; Leon, M.B.; Morice, M.-C.; Simonton, C.A.; Lembo, N.J.; Banning, A.P.; Merkely, B.; van Boven, A.J.; et al. Outcomes Among Patients Undergoing Distal Left Main Percutaneous Coronary Intervention. Circ. Cardiovasc. Interv. 2018, 11, e007007. [Google Scholar] [CrossRef] [Green Version]
- Ferenc, M.; Banholzer, N.; Hochholzer, W.; Mashayekhi, K.; Comberg, T.; Rothe, J.; Valina, C.M.; Toma, A.; Löffelhardt, N.; Gick, M.; et al. Long-term results after PCI of unprotected distal left main coronary artery stenosis: The Bifurcations Bad Krozingen (BBK)-Left Main Registry. Clin. Res. Cardiol. 2019, 108, 175–184. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Disqualification Factors | |||
|---|---|---|---|
| Cardiac Factors | Number of Patients | Extra-Cardiac Factors | Number of Patients |
| Enlargement of LV (LVEDD > 70 mm) | 6 | Severe obesity (BMI > 35 kg/m2) | 19 |
| LVEF < 30% | 4 | Renal failure (GFR < 30 mL/min) | 13 |
| Diffusely diseased peripheral segments (no useful for CABG) | 3 | Multilevel peripheral atherosclerosis | 10 |
| Valve diseases—not eligible for surgery | 2 | Frailty syndrome | 9 |
| Advanced COPD (GOLD ≥ 3) | 8 | ||
| Mental disorders | 7 | ||
| Others * | 23 | ||
| Variable | Total n = 459 | Group 1 n = 396 | Group 2 n = 63 | p-Value (Group 1 vs. Group 2) |
|---|---|---|---|---|
| Age (y) | 68.4 ± 9.4 | 68 ± 9.1 | 70.9 ± 10.9 | 0.024 |
| Gender (female) | 112 (24.4%) | 90 (22.7%) | 22 (34.9%) | 0.036 |
| BMI (kg/m2) | 28.1 ± 4.6 | 28.1 ± 4.4 | 28.2 ± 5.8 | 0.353 |
| Hypertension | 375 (81.7%) | 326 (82.3%) | 49 (77.8%) | 0.386 |
| Hyperlipidemia | 230 (50.1%) | 203 (51.2%) | 27 (42.9%) | 0.215 |
| CKD | 159 (34.6%) | 125 (31.6%) | 34 (54%) | <0.001 |
| DM | 164 (35.7%) | 136 (34.3%) | 28 (44.4%) | 0.120 |
| Stroke/TIA | 34 (7.4%) | 29 (7.3%) | 5 (7.9%) | 0.863 |
| COPD | 37 (8.1%) | 29 (7.3%) | 8 (12.7%) | 0.145 |
| PVD | 66 (14.4%) | 56 (14.1%) | 10 (15.9%) | 0.716 |
| AF | 59 (12.9%) | 48 (12.1%) | 11 (17.5%) | 0.240 |
| Smoking (current) | 168 (36.6%) | 140 (35.4%) | 28 (44.4%) | 0.164 |
| Prior MI | 227 (49.5%) | 199 (50.3%) | 28 (44.4%) | 0.382 |
| Stable CAD | 272 (59.2%) | 243 (61.4%) | 29 (46%) | 0.021 |
| Unstable CAD | 125 (27.2%) | 108 (27.3%) | 17 (27%) | 0.962 |
| NSTEMI | 45 (9.8%) | 31 (7.8%) | 14 (22.2%) | <0.001 |
| STEMI | 13 (2.8%) | 10 (2.5%) | 3 (4.8%) | 0.558 |
| Prior PCI LAD | 104 (22.7%) | 91 (23%) | 13 (20.6%) | 0.672 |
| Prior PCI LCX | 65 (14.2%) | 59 (14.9%) | 6 (9.5%) | 0.253 |
| Prior PCI RCA | 132 (28.8%) | 118 (29.8%) | 14 (22.2%) | 0.217 |
| Prior CABG | 92 (20%) | 88 (22.2%) | 4 (6.3%) | 0.003 |
| LVEDD (mm) | 51.6 ± 7.7 | 51.5 ± 7.6 | 52.4 ± 8.2 | 0.523 |
| LVEF (%) | 50.6 ± 11.2 | 51.4 ± 11 | 46 ± 11.4 | <0.001 |
| EuroScore II | 2.32 ± 2.13 | 2.15 ± 2.16 | 2.72 ± 2.01 | 0.007 |
| Syntax Score | 24.0 ± 9.9 | 23.2 ± 9.7 | 29.1 ± 9.5 | <0.001 |
| 0–22 (low) | 230 (50.1%) | 214 (54%) | 16 (25.4%) | <0.001 |
| 23–32 (intermediate) | 145 (31.6%) | 120 (30.3%) | 25 (39.7%) | 0.137 |
| ≥33 (high) | 84 (18.3%) | 62 (15.7%) | 22 (34.9%) | <0.001 |
| Variable | Total n = 459 | Group 1 n = 396 | Group 2 n = 63 | p-Value (Group 1 vs. Group 2 ) |
|---|---|---|---|---|
| LM distal | 375 (81.7%) | 319 (80.1%) | 56 (88.9%) | 0.087 |
| LM bifurcation | 292 (63.6%) | 249 (62.9%) | 43 (68.3%) | 0.410 |
| LM trifurcation | 52 (11.3%) | 43 (10.9%) | 9 (14.3%) | 0.425 |
| LM calcification | 70 (15.3%) | 54 (13.6%) | 16 (25.4%) | 0.016 |
| LAD disease (not ostial) | 240 (52.3%) | 202 (51%) | 38 (60.3%) | 0.167 |
| LCx disease (not ostial) | 159 (34.6%) | 130 (32.8%) | 29 (46%) | 0.041 |
| Protected LM | 63 (13.7%) | 62 (15.7%) | 1 (1.6%) | 0.003 |
| RCA recessive (a) | 29 (6.3%) | 23 (5.8%) | 6 (9.5%) | 0.260 |
| RCA with critical stenosis (b) | 70 (15.3%) | 54 (13.6%) | 16 (25.4%) | 0.016 |
| RCA total occlusion (c) | 82 (17.9%) | 68 (17.2%) | 14 (22.2%) | 0.331 |
| Lack of RCA support to LM-CAD (a + b + c) | 156 (34%) | 124 (31.3%) | 32 (50.8%) | 0.002 |
| Extent of diseased vessels | ||||
| LM only | 126 (27.5%) | 118 (29.8%) | 8 (12.7%) | 0.005 |
| LM plus 1-vessel disease | 164 (35.7%) | 144 (36.4%) | 20 (31.7%) | 0.477 |
| LM plus 2-vessel disease | 116 (25.3%) | 90 (22.7%) | 26 (41.3%) | 0.002 |
| LM plus 3-vessel disease | 53 (11.5%) | 44 (11.1%) | 9 (14.3%) | 0.464 |
| Bifurcation Medina | ||||
| 1.0.0 | 94 (20.5%) | 83 (21%) | 11 (17.5%) | 0.522 |
| 1.0.1 | 37 (8.1%) | 32 (8.1%) | 5 (7.9%) | 0.968 |
| 1.1.0 | 91 (19.8%) | 80 (20.2%) | 11 (17.5%) | 0.612 |
| 1.1.1 | 70 (15.3%) | 54 (13.6%) | 16 (25.4%) | 0.016 |
| Variable | Total n = 459 | Group 1 n = 396 | Group 2 n = 63 | p-Value (Group 1 vs. Group 2) |
|---|---|---|---|---|
| PCI success | 456 (99.3%) | 393 (99.2%) | 63 (100%) | 0.882 |
| Number of stents | 1.67 ± 0.81 | 1.63 ± 0.79 | 1.9 ± 0.9 | 0.012 |
| Total length of implanted stents (mm) | 38.0 ± 21.5 | 37.1 ± 21.2 | 43.7 ± 22.3 | 0.009 |
| Fluoroscopy time (min) | 17.47 ± 9.25 | 17.16 ± 9.17 | 19.42 ± 9.57 | 0.060 |
| Radiation dose (mGy) | 1442 ± 877 | 1427 ± 879 | 1531 ± 871 | 0.370 |
| Contrast volume (mL) | 247.4 ± 94.2 | 248.1 ± 96.9 | 242.9 ± 76.3 | 0.804 |
| Arterial Access site | ||||
| Radial | 270 (58.8%) | 235 (59.3%) | 35 (55.6%) | 0.570 |
| Femoral | 189 (41.2%) | 161 (40.7%) | 28 (44.4%) | |
| Stenting LM only | 57 (12.4%) | 50 (12.6%) | 7 (11.1%) | 0.735 |
| Stenting LM bifurcation | ||||
| One-stent technique | 317 (69.1%) | 282 (71.2%) | 35 (55.5%) | 0.013 |
| Two-stents technique | 85 (18.5%) | 64 (16.2%) | 21 (33.3%) | 0.001 |
| Two-stents techniques | Total n = 85 | n = 64 | n = 21 | |
| Crush | 30 (35.3%) | 18 (28.1%) | 12 (57.1%) | 0.016 |
| DK-Crush | 11 (12.9%) | 9 (14.1%) | 2 (9.5%) | 0.879 |
| Cullote | 1 (1.1%) | 0 (0%) | 1 (4.8%) | 0.247 |
| T-stenting | 19 (22.4%) | 15 23.4%) | 4 (19%) | 0.905 |
| Provisional stenting | 24 (28.2%) | 22 (34.3%) | 2 (9.5%) | 0.028 |
| Variable | Total n = 459 | Group 1 n = 396 | Group 2 n = 63 | p-Value (Group 1 vs. Group 2) |
|---|---|---|---|---|
| Significant troponin elevation (5×) after PCI | 222 (48.4%) | 185 (46.7%) | 36 (57.1%) | 0.136 |
| Myocardial Infarction | 21 (4.6%) | 16 (4%) | 5 (7.9%) | 0.294 |
| In-hospital Death | 2 (0.4%) | 2 (0.5%) | 0 (0%) | 0.642 |
| Stroke | 1 (0.2%) | 0 (0%) | 1 (1.6%) | 0.137 |
| Tamponade | 2 (0.4%) | 2 (0.5%) | 0 (0%) | 0.642 |
| Pulmonary oedema | 1 (0.2%) | 0 (0%) | 1 (1.6%) | 0.137 |
| Dissection of aorta | 1 (0.2%) | 1 (0.3%) | 0 (0%) | 0.291 |
| Perforation of femoral artery | 1 (0.2%) | 1 (0.3%) | 0 (0%) | 0.291 |
| Contrast induced nephropathy | 17 (3.7%) | 12 (3%) | 5 (7.9%) | 0.120 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skorupski, W.J.; Kałużna-Oleksy, M.; Lesiak, M.; Araszkiewicz, A.; Skorupski, W.; Grajek, S.; Mitkowski, P.; Pyda, M.; Grygier, M. Short- and Long-Term Outcomes of Left Main Coronary Artery Stenting in Patients Disqualified from Coronary Artery Bypass Graft Surgery. J. Pers. Med. 2022, 12, 348. https://doi.org/10.3390/jpm12030348
Skorupski WJ, Kałużna-Oleksy M, Lesiak M, Araszkiewicz A, Skorupski W, Grajek S, Mitkowski P, Pyda M, Grygier M. Short- and Long-Term Outcomes of Left Main Coronary Artery Stenting in Patients Disqualified from Coronary Artery Bypass Graft Surgery. Journal of Personalized Medicine. 2022; 12(3):348. https://doi.org/10.3390/jpm12030348
Chicago/Turabian StyleSkorupski, Wojciech Jan, Marta Kałużna-Oleksy, Maciej Lesiak, Aleksander Araszkiewicz, Włodzimierz Skorupski, Stefan Grajek, Przemysław Mitkowski, Małgorzata Pyda, and Marek Grygier. 2022. "Short- and Long-Term Outcomes of Left Main Coronary Artery Stenting in Patients Disqualified from Coronary Artery Bypass Graft Surgery" Journal of Personalized Medicine 12, no. 3: 348. https://doi.org/10.3390/jpm12030348
APA StyleSkorupski, W. J., Kałużna-Oleksy, M., Lesiak, M., Araszkiewicz, A., Skorupski, W., Grajek, S., Mitkowski, P., Pyda, M., & Grygier, M. (2022). Short- and Long-Term Outcomes of Left Main Coronary Artery Stenting in Patients Disqualified from Coronary Artery Bypass Graft Surgery. Journal of Personalized Medicine, 12(3), 348. https://doi.org/10.3390/jpm12030348