
Association between General Anesthesia and Root Canal Treatment Outcomes in Patients with Mental Disability: A Retrospective Cohort Study

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sources of Data
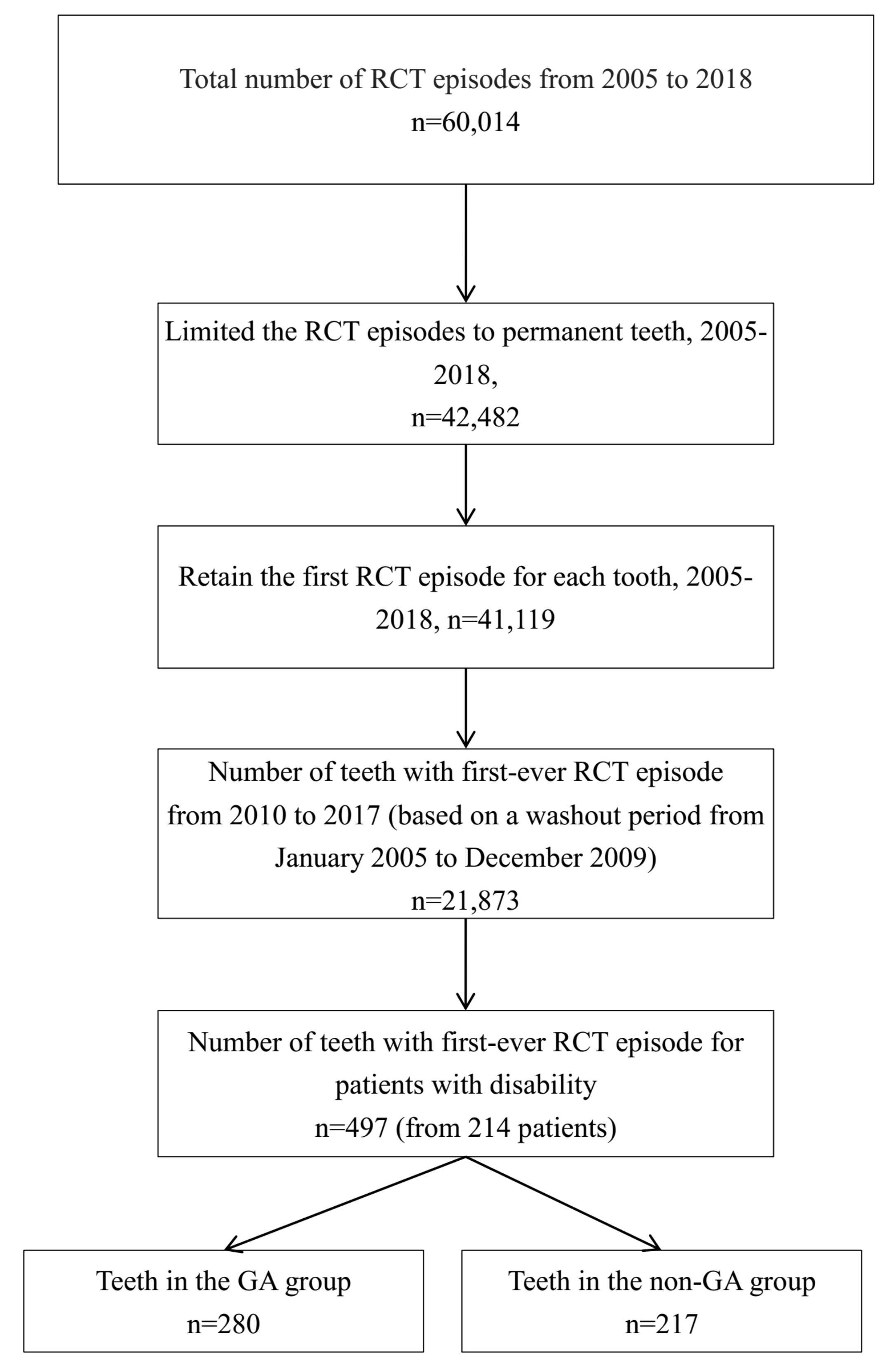
2.2. Study Sample
2.3. Exposure
2.4. Outcome Measure
2.5. Covariates
2.6. Statistical Analysis
3. Results
3.1. Participants
3.2. The Baseline Characteristics Comparison between the Two Groups
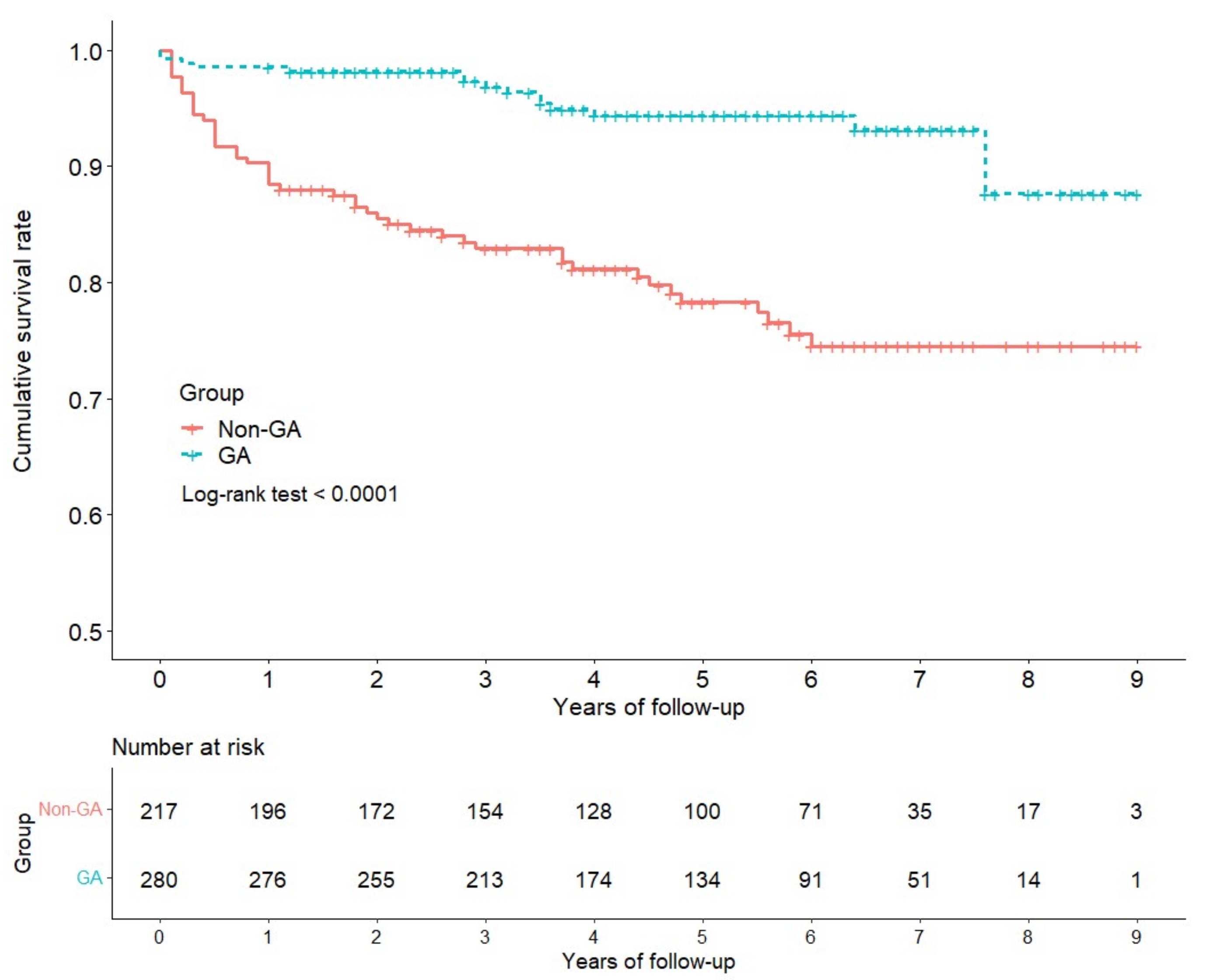
3.3. The Cumulative Survival Rate of Teeth between Two Groups
3.4. The Risk Factors Analysis for Cumulative Survival Rate of Teeth
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. World report on disability 2011, World Health Organization. 2011. Available online: https://www.who.int/disabilities/world_report/2011/report.pdf (accessed on 2 May 2021).
- Anders, P.L.; Davis, E. Oral health of patients with intellectual disabilities: A systematic review. Spéc. Care Dent. 2010, 30, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Rocha, L.L.; De Lima Saintrain, M.V.; Vieira-Meyer, A.P.G.F. Access to dental public services by disabled persons. BMC Oral Health 2015, 15, 35. [Google Scholar] [CrossRef] [Green Version]
- Lim, M.A.W.T.; Borromeo, G.L. The use of general anesthesia to facilitate dental treatment in adult patients with special needs. J. Dent. Anesthesia Pain Med. 2017, 17, 91–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, J.; Patton, L.; Kim, H.-Y. Impact of dental treatment under general anesthesia on the oral health-related quality of life of adolescents and adults with special needs. Eur. J. Oral Sci. 2014, 122, 363–371. [Google Scholar] [CrossRef]
- Hillebrecht, A.-L.; Hrasky, V.; Anten, C.; Wiegand, A. Changes in the oral health-related quality of life in adult patients with intellectual disabilities after dental treatment under general anesthesia. Clin. Oral Investig. 2019, 23, 3895–3903. [Google Scholar] [CrossRef] [PubMed]
- Jankauskiene, B.; Narbutaite, J. Changes in oral health-related quality of life among children following dental treatment under general anaesthesia. A Syst. Rev. Stomatol. 2010, 12, 60–64. [Google Scholar]
- Mallineni, S.K.; Yiu, C.K. Dental treatment under general anesthesia for special-needs patients: Analysis of the literature. J. Investig. Clin. Dent. 2015, 7, 325–331. [Google Scholar] [CrossRef]
- Nelson, T.; Xu, Z. Pediatric dental sedation: Challenges and opportunities. Clin. Cosmet. Investig. Dent. 2015, ume 7, 97–106. [Google Scholar] [CrossRef] [Green Version]
- Roberts, G.J.; Mokhtar, S.M.; Lucas, V.S.; Mason, C. Deaths associated with GA for dentistry 1948–2016: The evolution of a policy for general anaesthesia (GA) for dental treatment. Heliyon 2020, 6, e02671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cousson, P.-Y.; Nicolas, E.; Hennequin, M. A follow-up study of pulpotomies and root canal treatments performed under general anaesthesia. Clin. Oral Investig. 2014, 18, 1155–1163. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.; Kim, H.-Y. Prognostic factors of single-visit endodontic and restorative treatment under general anaesthesia for special needs patients. J. Oral Rehabil. 2016, 44, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Üstün, T.; Chatterji, S.; Bickenbach, J.; Kostanjsek, N.; Schneider, M. The International Classification of Functioning, Disability and Health: A new tool for understanding disability and health. Disabil. Rehabil. 2003, 25, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Aminoshariae, A.; Kulild, J.C.; Mickel, A.; Fouad, A.F. Association between Systemic Diseases and Endodontic Outcome: A Systematic Review. J. Endod. 2017, 43, 514–519. [Google Scholar] [CrossRef] [PubMed]
- Serrano-Gimenez, M.; Sánchez-Torres, A.; Escoda, C.G. Prognostic factors on periapical surgery: A systematic review. Medicina Oral Patología Oral y Cirugia Bucal 2015, 20, e715–e722. [Google Scholar] [CrossRef] [PubMed]
- Mordohai, N.; Reshad, M.; Jivraj, S.; Chee, W. Factors that affect individual tooth prognosis and choices in contemporary treatment planning. Br. Dent. J. 2007, 202, 63–72. [Google Scholar] [CrossRef] [Green Version]
- Türp, J.C. Alt KW Designating teeth: The advantages of the FDI’s two-digit system. Quintessence Int. 1995, 26, 501–504. [Google Scholar]
- Austin, P.C. A Tutorial on Multilevel Survival Analysis: Methods, Models and Applications. Int. Stat. Rev. 2017, 85, 185–203. [Google Scholar] [CrossRef]
- Fine, J.P.; Ray, M. A Proportional Hazards Model for the Subdistribution of a Competing Risk. J. Am. Stat. Assoc. 1999, 94, 496–509. [Google Scholar] [CrossRef]
- Lee, C.B.; Chang, Y.-H.; Wen, P.-C.; Li, C.-Y. Association of Failed Root Canal Treatment with Dentist and Institutional Volumes: A Population-based Cohort Study in Taiwan. J. Endod. 2017, 43, 1628–1634. [Google Scholar] [CrossRef]
- Donabedian, A. An Introduction to Quality Assurance in Health Care; Oxford University Press: Oxford, UK, 2002. [Google Scholar]
- Gulabivala, K.; Patel, B.; Evans, G.; Ng, Y.-L. Effects of mechanical and chemical procedures on root canal surfaces. Endod. Top. 2005, 10, 103–122. [Google Scholar] [CrossRef]
- Tabassum, S.; Khan, F.R. Failure of endodontic treatment: The usual suspects. Eur. J. Dent. 2016, 10, 144–147. [Google Scholar] [CrossRef]
- Siqueira, J.F., Jr. Aetiology of root canal treatment failure: Why well-treated teeth can fail. Int. Endod. J. 2001, 34, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chicka, M.C.; Dembo, J.B.; Mathu-Muju, K.R.; Nash, D.A.; Bush, H.M. Adverse events during pediatric dental anesthesia and sedation: A review of closed malpractice insurance claims. Pediatric Dent. 2012, 34, 231–238. [Google Scholar]
- Song, S.; Han, M.; Kim, J. Safety of chloral hydrate sedation in dental practice for children: An overview. J. Dent. Anesthesia Pain Med. 2020, 20, 107–118. [Google Scholar] [CrossRef] [PubMed]
- Huang, A.; Tanbonliong, T. Oral Sedation Postdischarge Adverse Events in Pediatric Dental Patients. Anesthesia Prog. 2015, 62, 91–99. [Google Scholar] [CrossRef] [Green Version]
- Nordt, S.P.; Rangan, C.; Hardmaslani, M.; Clark, R.F.; Wendler, C.; Valente, M. Pediatric Chloral Hydrate Poisonings and Death Following Outpatient Procedural Sedation. J. Med Toxicol. 2014, 10, 219–222. [Google Scholar] [CrossRef] [Green Version]
- Britto, L.R.; Katz, J.; Guelmann, M.; Heft, M. Periradicular radiographic assessment in diabetic and control individuals. Oral Surgery, Oral Med. Oral Pathol. Oral Radiol. Endodontology 2003, 96, 449–452. [Google Scholar] [CrossRef]
- Wang, C.-H.; Chueh, L.-H.; Chen, S.-C.; Feng, Y.-C.; Hsiao, C.K.; Chiang, C.-P. Impact of Diabetes Mellitus, Hypertension, and Coronary Artery Disease on Tooth Extraction after Nonsurgical Endodontic Treatment. J. Endod. 2011, 37, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Mindiola, M.J.; Mickel, A.K.; Sami, C.; Jones, J.J.; Lalumandier, J.A.; Nelson, S.S. Endodontic Treatment in an American Indian Population: A 10-Year Retrospective Study. J. Endod. 2006, 32, 828–832. [Google Scholar] [CrossRef]
- Klaassen, M.A.; Veerkamp, J.S.J.; Hoogstraten, J. Young children’s Oral Health-Related Quality of Life and dental fear after treatment under general anaesthesia: A randomized controlled trial. Eur. J. Oral Sci. 2009, 117, 273–278. [Google Scholar] [CrossRef]
- Travassos, C.; Martins, M. Uma revisão sobre os conceitos de acesso e utilização de serviços de saúde. Cadernos de Saúde Pública 2004, 20, S190–S198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laukkanen, E.; Vehkalahti, M.M.; Kotiranta, A.K. Impact of systemic diseases and tooth-based factors on outcome of root canal treatment. Int. Endod. J. 2019, 52, 1417–1426. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Characteristics | GA (n = 280) | Non-GA (n = 217) | p-Value |
|---|---|---|---|
| Patients number | 108 | 106 | |
| Age | 25.3 ± 13.7 | 31.5 ± 16.5 | <0.001 ** |
| Gender (male) | 158 (56.4) | 117(53.9) | 0.577 |
| Comorbidity | |||
| Periodontitis | 110 (39.3) | 133(61.3) | <0.001 ** |
| Hypertension | 0 (0.0) | 6(2.8) | 0.005 ** |
| Dyslipidemia | 3 (1.1) | 11(5.1) | 0.008 ** |
| Diabetes mellitus | 3 (1.1) | 11(5.1) | 0.008 ** |
| Ischemia heart disease | 0 (<0.1) | 1(0.5) | 0.256 |
| Disability type | <0.001 ** | ||
| Mental retard | 210 (75.0) | 152 (70.0) | |
| Dementia | 2 (0.7) | 18 (8.3) | |
| Autism | 45 (16.1) | 21 (9.7) | |
| Chronic mental illness | 23 (8.2) | 26 (12.0) | |
| Severity of disability | 0.030 * | ||
| Mild | 16 (5.7) | 24 (11.1) | |
| Moderate | 86 (30.7) | 77 (35.5) | |
| Severe | 108 (38.6) | 79 (36.4) | |
| Extremely severe | 70 (25.0) | 37 (17.1) | |
| Teeth position | 0.367 | ||
| Incisor and canine | 101 (36.1) | 82 (37.8) | |
| Premolar | 75 (26.8) | 67 (30.9) | |
| Molar | 104 (37.1) | 68 (31.3) | |
| Maxillary teeth (upper) | 153 (54.6) | 114 (52.5) | 0.640 |
| Endpoints | |||
| Endodontic re-treatment | 7 (2.5) | 24 (11.1) | <0.001 ** |
| Extraction | 9 (3.2) | 24 (11.1) | <0.001 ** |
| Failure of RCT | 15 (5.4) | 47 (21.7) | <0.001 ** |
| Follow-Up (Years) | Definition of Failure | |||||
|---|---|---|---|---|---|---|
| Endodontic Re-Treatment | Extraction | Failure of RCT | ||||
| GA | Non-GA | GA | Non-GA | GA | Non-GA | |
| % | % | % | % | % | % | |
| 1 | 99.64 | 92.63 | 98.93 | 95.85 | 98.57 | 88.48 |
| 2 | 99.64 | 91.18 | 98.57 | 93.85 | 98.21 | 85.54 |
| 3 | 98.76 | 89.57 | 98.11 | 92.83 | 96.88 | 82.93 |
| 4 | 97.21 | 89.57 | 97.15 | 91.08 | 94.38 | 81.19 |
| 5 | 97.21 | 88.08 | 97.15 | 89.70 | 94.38 | 78.30 |
| 6 | 97.21 | 88.08 | 96.30 | 85.99 | 94.38 | 74.51 |
| 7 | 95.98 | 88.08 | 96.30 | 85.99 | 93.16 | 74.51 |
| 8 | 95.98 | 88.08 | 91.23 | 85.99 | 87.68 | 74.51 |
| 9 | 95.98 | 88.08 | 91.23 | 85.99 | 87.68 | 74.51 |
| p for Log-rank test | 0.0001 | 0.0012 | <0.0001 | |||
| Variables | NFRCT | CHR (95%CI) | p Value | AHR (95%CI) | p Value |
|---|---|---|---|---|---|
| General anesthesia | |||||
| No | 47 | Reference group | Reference group | ||
| Yes | 15 | 0.24 (0.13–0.44) | <0.001** | 0.24 (0.12–0.49) | <0.001 ** |
| Age | 1.00 (0.98–1–02) | 0.982 | 0.97 (0.93–1.00) | 0.071 | |
| Periodontitis | |||||
| No | 27 | Reference group | Reference group | ||
| Yes | 35 | 1.48 (0.84–2.62) | 0.177 | 1.31 (0.71–2.41) | 0.381 |
| Hypertension | |||||
| No | 61 | Reference group | Reference group | ||
| Yes | 1 | 1.38 (0.15–12.69) | 0.776 | 0.82 (0.06–10.90) | 0.885 |
| Dyslipidemia | |||||
| No | 57 | Reference group | Reference group | ||
| Yes | 5 | 3.28 (1.64–6.54) | 0.001** | 1.89 (0.59–6.10) | 0.287 |
| Diabetes mellitus | |||||
| No | 58 | Reference group | Reference group | ||
| Yes | 4 | 2.46 (0.97–6.27) | 0.059 | 0.80 (0.22–2.88) | 0.734 |
| Disability type | |||||
| Mental retard | 49 | Reference group | Reference group | ||
| Dementia | 4 | 1.92 (0.74–4.98) | 0.178 | 4.15 (0.73–23.61) | 0.108 |
| Autism | 4 | 0.45 (0.17–1.21) | 0.114 | 0.39 (0.14–1.08) | 0.071 |
| Chronic mental illness | 5 | 0.69 (0.22–2.20) | 0.535 | 0.82 (0.27–2.49) | 0.720 |
| Severity | |||||
| Mild | 6 | Reference group | Reference group | ||
| Moderate | 22 | 0.91 (0.32–2.61) | 0.865 | 0.99 (0.32–3.11) | 0.992 |
| Severe | 26 | 0.94 (0.33–2.68) | 0.910 | 1.06 (0.35–3.22) | 0.918 |
| Extreme severe | 8 | 0.53 (0.17–1.63) | 0.266 | 0.65 (0.19–2.23) | 0.489 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, G.-Y.; Wu, Z.-F.; Lin, Y.-T.; Cheng, K.-I.; Huang, Y.-T.; Huang, S.-T.; Hargono, A.; Li, C.-Y. Association between General Anesthesia and Root Canal Treatment Outcomes in Patients with Mental Disability: A Retrospective Cohort Study. J. Pers. Med. 2022, 12, 213. https://doi.org/10.3390/jpm12020213
Chen G-Y, Wu Z-F, Lin Y-T, Cheng K-I, Huang Y-T, Huang S-T, Hargono A, Li C-Y. Association between General Anesthesia and Root Canal Treatment Outcomes in Patients with Mental Disability: A Retrospective Cohort Study. Journal of Personalized Medicine. 2022; 12(2):213. https://doi.org/10.3390/jpm12020213
Chicago/Turabian StyleChen, Guan-Yu, Zhi-Fu Wu, Yi-Ting Lin, Kuang-I Cheng, Yu-Ting Huang, Shun-Te Huang, Arief Hargono, and Chung-Yi Li. 2022. "Association between General Anesthesia and Root Canal Treatment Outcomes in Patients with Mental Disability: A Retrospective Cohort Study" Journal of Personalized Medicine 12, no. 2: 213. https://doi.org/10.3390/jpm12020213
APA StyleChen, G.-Y., Wu, Z.-F., Lin, Y.-T., Cheng, K.-I., Huang, Y.-T., Huang, S.-T., Hargono, A., & Li, C.-Y. (2022). Association between General Anesthesia and Root Canal Treatment Outcomes in Patients with Mental Disability: A Retrospective Cohort Study. Journal of Personalized Medicine, 12(2), 213. https://doi.org/10.3390/jpm12020213