
Applicability of Oculomotor Tests for Predicting Central Vestibular Disorder Using Principal Component Analysis

 ,
,  , , ,
, , ,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
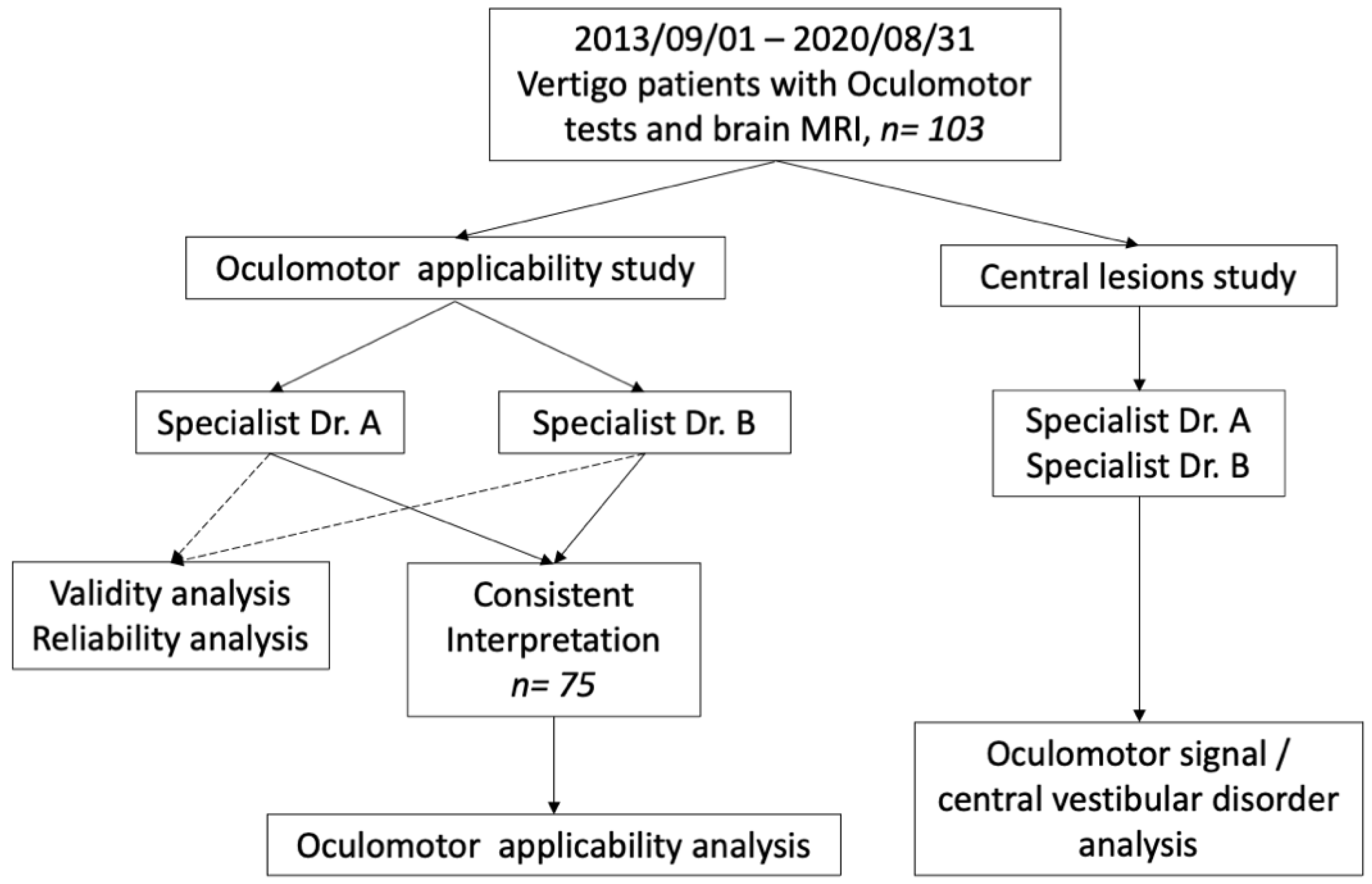
2.1. Study Design and Population
2.2. Oculomotor Tests
- Gaze-evoked nystagmus (horizontal or vertical axis): The patient was made to look front, left, right, up, and down at angles of 15° for 20 s at one side, and the nystagmus was recorded. The whole interpretation range for one dimension was 60 s. Pure torsional or vertical nystagmus, direction-changing nystagmus, and gaze-evoked nystagmus opposite to Alexander’s law were considered as central vestibular findings.
- Saccades (horizontal or vertical axis): A sequence of spots displaced horizontally or vertically at roughly 4 s intervals were shown, and the patient was asked to follow the stimulus only with their eyes, keeping their head stable. The whole interpretation range for one dimension was 30 s, including 8–9 repetitive signals. Latency refers to the delay between the onset of target movement and initiation of eye movement; latency consistently >260 ms is considered abnormal. Precision refers to the amplitude of the eye movement relative to the target; hypometria of 10–20% is considered normal. Asymmetrical saccades indicate abnormality.
- Smooth pursuit (horizontal or vertical axis): Patients watched a bright spot that moved smoothly across a screen in the horizontal or vertical plane, at a frequency of 0.25 Hz. The whole interpretation range for one dimension was 30 s, including 7–8 repetitive signals. Pursuit may be saccadic/jerky if there is a lesion in the cerebellum, brainstem, or parietal lobe. “Symmetrically impaired” pursuit can be a nonspecific central finding, while “asymmetrically impaired” pursuit is suggestive of a unilateral hemispheric or asymmetrical posterior fossa lesion.
- Optokinetic nystagmus: The patient was asked to track a repetitive moving target across the screen at a frequency of 4 Hz. These were moved first toward the right and then toward the left. The whole interpretation range for optokinetic nystagmus was 15 s, and another 15 s for after nystagmus reading as well. Cerebral and cerebellar lesions lead to ipsilateral preponderance, and brainstem lesions to contralateral preponderance.
2.3. Brain MRI
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Strupp, M.; Brandt, T. Diagnosis and treatment of vertigo and dizziness. Dtsch. Ärzteblatt Int. 2008, 105, 173–180. [Google Scholar] [CrossRef] [PubMed]
- Venhovens, J.; Meulstee, J.; Verhagen, W.I. Acute vestibular syndrome: A critical review and diagnostic algorithm concerning the clinical differentiation of peripheral versus central aetiologies in the emergency department. J. Neurol. 2016, 263, 2151–2157. [Google Scholar] [CrossRef] [PubMed]
- Karatas, M. Central Vertigo and Dizziness: Epidemiology, Differential Diagnosis, and Common Causes. Neurologist 2008, 14, 355–364. [Google Scholar] [CrossRef] [PubMed]
- Cohn, B. Can bedside oculomotor (HINTS) testing differentiate central from peripheral causes of vertigo? Ann. Emerg. Med. 2014, 64, 265–268. [Google Scholar] [CrossRef]
- Kerber, K.A.; Brown, D.L.; Lisabeth, L.D.; Smith, M.A.; Morgenstern, L.B. Stroke among patients with dizziness, vertigo, and imbalance in the emergency department: A population-based study. Stroke 2006, 37, 2484–2487. [Google Scholar] [CrossRef]
- Choi, J.Y.; Lee, S.H.; Kim, J.S. Central vertigo. Curr. Opin. Neurol. 2018, 31, 81–89. [Google Scholar] [CrossRef]
- Chen, L.; Lee, W.; Chambers, B.R.; Dewey, H.M. Diagnostic accuracy of acute vestibular syndrome at the bedside in a stroke unit. J. Neurol. 2011, 258, 855–861. [Google Scholar] [CrossRef]
- Newman-Toker, D.E.; Curthoys, I.S.; Halmagyi, G.M. Diagnosing Stroke in Acute Vertigo: The HINTS Family of Eye Movement Tests and the Future of the “Eye ECG”. Semin. Neurol. 2015, 35, 506–521. [Google Scholar] [CrossRef]
- Kerber, K.A.; Meurer, W.J.; Brown, D.L.; Burke, J.F.; Hofer, T.P.; Tsodikov, A.; Hoeffner, E.G.; Fendrick, A.M.; Adelman, E.E.; Morgenstern, L.B. Stroke risk stratification in acute dizziness presentations: A prospective imaging-based study. Neurology 2015, 85, 1869–1878. [Google Scholar] [CrossRef] [Green Version]
- Colledge, N.; Lewis, S.; Mead, G.; Sellar, R.; Wardlaw, J.; Wilson, J. Magnetic resonance brain imaging in people with dizziness: A comparison with non-dizzy people. J. Neurol. Neurosurg. Psychiatry 2002, 72, 587–589. [Google Scholar] [CrossRef]
- Ahsan, S.F.; Syamal, M.N.; Yaremchuk, K.; Peterson, E.; Seidman, M. The costs and utility of imaging in evaluating dizzy patients in the emergency room. Laryngoscope 2013, 123, 2250–2253. [Google Scholar] [CrossRef] [PubMed]
- Bachi, T.H.; Vicky, S.K. Videonystagmography. Otorhinolaryngol. Clin. Ann. Int. J. 2012, 4, 17–24. [Google Scholar]
- Mackenzie, S.W.; Iriving, R.; Monksfield, P.; Dezso, A.; Dawe, N.; Lindley, K.; Reynolds, R.F. Comparing Ocular Responses to Caloric Irrigation and Electrical Vestibular Stimulation in Vestibular Schwannoma. Front. Neurol. 2019, 10, 1181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohamed, E.S. Predictors of central vestibular disorders from videonystagmography tests. Egypt. J. Otolaryngol. 2016, 32, 202–209. [Google Scholar] [CrossRef]
- Silvoniemi, P.; Laurikainen, E.; Johansson, R.; Karjalainen, S. Electronystagmographic findings in patients with acute cerebral vascular disease and vertigo. Acta Otolaryngol. Suppl. 2000, 543, 41–43. [Google Scholar] [CrossRef]
- Mekki, S. The role of videonystagmography (VNG) in assessment of dizzy patient. Egypt. J. Otolaryngol. 2014, 30, 69–72. [Google Scholar] [CrossRef]
- Strupp, M.; Hüfner, K.; Sandmann, R.; Zwergal, A.; Dieterich, M.; Jahn, K.; Brandt, T. Central oculomotor disturbances and nystagmus: A window into the brainstem and cerebellum. Dtsch. Ärzteblatt Int. 2011, 108, 197–204. [Google Scholar] [CrossRef]
- Lee, H.J.; Kim, E.S.; Kim, M.; Chu, H.; Ma, H.I.; Lee, J.S.; Koo, J.W.; Kim, H.J.; Hong, S.K. Isolated horizontal positional nystagmus from a posterior fossa lesion. Ann. Neurol. 2014, 76, 905–910. [Google Scholar] [CrossRef]
- Mankekar, G.; Jeha, G.; Erbele, I.; Klumpp, M.; Sevy, A.; Mehta, R.; Son, L.; Arriaga, M.A. Do central vestibular findings predict abnormal findings on magnetic resonance imaging? J. Laryngol. Otol. 2019, 133, 554–559. [Google Scholar] [CrossRef]
- Patino, C.M.; Ferreira, J.C. Understanding diagnostic tests. Part 2. J. Bras. Pneumol. 2017, 43, 408. [Google Scholar] [CrossRef] [Green Version]
- Piker, E.G.; Jacobson, G.P. Self-report symptoms differ between younger and older dizzy patients. Otol. Neurotol. 2014, 35, 873–879. [Google Scholar] [CrossRef] [PubMed]
- Jahn, K. The Aging Vestibular System: Dizziness and Imbalance in the Elderly. Vestib. Disord. 2019, 82, 143–149. [Google Scholar] [CrossRef]
- Jahn, K.; Kressig, R.W.; Bridenbaugh, S.A.; Brandt, T.; Schniepp, R. Dizziness and Unstable Gait in Old Age: Etiology, Diagnosis and Treatment. Dtsch. Ärzteblatt Int. 2015, 112, 387–393. [Google Scholar] [CrossRef] [Green Version]
- Leigh, R.J.; Zee, J.; David, S. The Neurology of Eye Movements, 5th ed.; Oxford University Press: New York, NY, USA, 2015. [Google Scholar]
- Assir, M.Z.K.; Das, J.M. How to Localize Neurologic Lesions by Physical Examination; StatPearls: Treasure Island, FL, USA, 2021. [Google Scholar]
- Ringnér, M. What is principal component analysis? Nat. Biotechnol. 2008, 26, 303–304. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variables | All Patients n = 103 | Central n = 24 | Nonspecific n = 79 | p-Value |
|---|---|---|---|---|
| Median age at diagnosis, | 0.794 | |||
| years (IQR) | 60 (49–69) | 61 (48–69) | 60 (49–69) | |
| Gender | * 0.014 | |||
| Female | 65 (63.1%) | 10 (41.7%) | 55 (69.6%) | |
| Male | 38 (36.9%) | 14 (58.3%) | 24 (30.4%) | |
| Body mass index (n = 99) | 0.339 | |||
| Median (IQR) | 24.0 (21.7–25.7) | 24.7 (22.5–26.6) | 23.8 (21.7–25.7) | |
| Asymmetric hearing loss (n = 85) | 0.379 | |||
| No | 71 (83.5%) | 11 (91.7%) | 60 (82.2%) | |
| Yes (>30 dB loss) | 14 (16.5%) | 1 (8.3%) | 13 (17.8%) | |
| Neurologic symptoms | * <0.001 | |||
| No | 78 (75.7%) | 8 (33.3%) | 70 (88.6%) | |
| Yes | 25 (24.3%) | 16 (66.7%) | 9 (11.4%) | |
| Central lesions (MRI) | N/A | N/A | ||
| No | 79 (76.7%) | |||
| Yes | 24 (23.3%) | |||
| Lesion sites (MRI) | N/A | N/A | ||
| Cortical and subcortical | 10 (38.5%) | |||
| Brain stem | 10 (38.5%) | |||
| Cerebellar | 5 (19.2%) | |||
| Skull base | 1 (3.8%) | |||
| Lesion types (MRI) | N/A | N/A | ||
| Cerebrovascular accident | 13 (54.2%) | |||
| Tumor | 9 (37.5%) | |||
| Inflammation | 2 (8.3%) | |||
| Comorbidities | ||||
| Diabetes mellitus | 0.556 | |||
| No | 83 (80.6%) | 18 (75.0%) | 65 (82.3%) | |
| Yes | 20 (19.4%) | 6 (25.0%) | 14 (17.7%) | |
| Hypertension | 0.323 | |||
| No | 52 (50.5%) | 10 (41.7%) | 42 (53.2%) | |
| Yes | 51 (49.5%) | 14 (58.3%) | 37 (46.8%) | |
| Hyperlipidemia | 0.253 | |||
| No | 66 (64.1%) | 13 (54.2%) | 53 (67.1%) | |
| Yes | 37 (35.9%) | 11 (45.8%) | 26 (32.9%) | |
| History of CVA | 0.622 | |||
| No | 97 (94.2%) | 22 (91.7%) | 75 (94.9%) | |
| Yes | 6 (5.8%) | 2 (8.3%) | 4 (5.1%) | |
| Cardiovascular disease | 0.588 | |||
| No | 98 (95.2%) | 24 (100.0%) | 74 (93.7%) | |
| Yes | 5 (4.8%) | 0 (0.0%) | 5 (6.3%) | |
| Accumulated comorbidities | 0.709 | |||
| 0 | 28 (27.2%) | 5 (20.8%) | 23 (29.1%) | |
| 1–2 | 64 (62.1%) | 16 (66.7%) | 48 (60.8%) | |
| ≥3 | 11 (10.7%) | 3 (12.5%) | 8 (10.1%) |
| Raters | Sensitivity | Specificity | PPV | NPV | Test–Retest Reliability Kappa (95% CI) | Inter-Rater Reliability Kappa (95% CI) |
|---|---|---|---|---|---|---|
| Dr. A | 54.2% | 67.1% | 33.3% | 82.8% | 0.669 (0.521–0.817) | 0.480 (0.329–0.630) |
| Dr. B | 66.7% | 43.0% | 26.2% | 81.0% | 0.571 (0.413–0.729) |
| Variables | Consistent n = 44 | Inconsistent n = 31 | p-Value |
|---|---|---|---|
| Median age at diagnosis, | * <0.001 | ||
| years (IQR) | 55 (41.5–63.5) | 69 (52–76) | |
| Gender | 0.968 | ||
| Female | 30 (68.2%) | 21 (67.7%) | |
| Male | 14 (31.8%) | 10 (32.3%) | |
| Body mass index | 0.378 | ||
| Median (IQR) | 23.2 (20.6–25.5) | 24.0 (21.8–25.9) | |
| Asymmetric hearing loss | 0.804 | ||
| No | 33 (86.8%) | 24 (88.9%) | |
| Yes (>30 dB loss) | 5 (13.2%) | 3 (11.1%) | |
| Neurologic symptoms | 0.640 | ||
| No | 36 (81.4%) | 24 (77.4%) | |
| Yes | 8 (18.6%) | 7 (22.6%) | |
| Central lesions (MRI) | 0.478 | ||
| No | 34 (77.3%) | 26 (83.9%) | |
| Yes | 10 (22.7%) | 5 (16.1%) | |
| Lesion sites (MRI) | 0.327 | ||
| Cortical and subcortical | 3 (27.3%) | 1 (20.0%) | |
| Brain stem | 6 (54.6%) | 1 (20.0%) | |
| Cerebellar | 2 (18.1%) | 3 (60.0%) | |
| Lesion types (MRI) | 0.213 | ||
| Cerebrovascular accident | 7 (70.0%) | 2 (40.0%) | |
| Tumors | 3 (30.0%) | 1 (20.0%) | |
| Inflammation | 0 (0.0%) | 2 (40.0%) | |
| Comorbidities | |||
| Diabetes mellitus | 0.468 | ||
| No | 37 (84.1%) | 24 (77.4%) | |
| Yes | 7 (15.9%) | 7 (22.6%) | |
| Hypertension | 0.204 | ||
| No | 25 (56.8%) | 13 (41.9%) | |
| Yes | 19 (43.2%) | 18 (58.1%) | |
| Hyperlipidemia | 0.240 | ||
| No | 30 (68.2%) | 17 (54.8%) | |
| Yes | 14 (31.8%) | 14 (45.2%) | |
| History of CVA | 0.067 | ||
| No | 43 (97.7%) | 27 (87.1%) | |
| Yes | 1 (2.3%) | 4 (12.9%) | |
| Cardiovascular disease | 0.160 | ||
| No | 43 (97.7%) | 28 (90.3%) | |
| Yes | 1 (2.3%) | 3 (9.7%) | |
| Accumulated comorbidities | * 0.017 | ||
| 0 | 15 (34.1%) | 3 (9.7%) | |
| 1–2 | 27 (61.3%) | 23 (74.2%) | |
| ≥3 | 2 (4.6%) | 5 (16.1%) |
| Variables | Univariate OR (95% CI) | p-Value | Multivariate OR (95% CI) | p-Value |
|---|---|---|---|---|
| Age | ||||
| <60 years old (n = 34) | 1 | 1 | ||
| ≥60 years old (n = 41) | 4.15 (1.52–11.34) | * 0.006 | 3.09 (1.04–9.14) | * 0.042 |
| Gender | ||||
| Female | 1 | 1 | ||
| Male | 1.02 (0.38–2.73) | 0.968 | 0.91 (0.30–2.83) | 0.877 |
| Body mass index (n = 74) | 1.05 (0.94–1.17) | 0.407 | ||
| Asymmetric hearing loss | ||||
| No (n = 57) | 1 | |||
| Yes (>30 dB loss) (n = 8) | 0.83 (0.18–3.79) | 0.805 | ||
| Neurologic symptoms | ||||
| No | 1 | 1 | ||
| Yes | 1.31 (0.42–4.10) | 0.640 | 0.99 (0.28–3.56) | 0.991 |
| Central lesions (MRI) | ||||
| No | 1 | |||
| Yes | 0.65 (0.20–2.15) | 0.484 | ||
| Comorbidities | ||||
| Diabetes mellitus | ||||
| No | 1 | |||
| Yes | 1.54 (0.48–4.95) | 0.467 | ||
| Hypertension | ||||
| No | 1 | |||
| Yes | 1.82 (0.72–4.72) | 0.206 | ||
| Hyperlipidemia | ||||
| No | 1 | |||
| Yes | 1.77 (0.68–4.56) | 0.241 | ||
| History of CVA | ||||
| No | 1 | |||
| Yes | 6.37 (0.68–60.05) | 0.106 | ||
| Cardiovascular disease | ||||
| No | 1 | |||
| Yes | 4.61 (0.46–46.54) | 0.195 | ||
| Accumulated Comorbidities | ||||
| 0 | 1 | 1 | ||
| 1–2 | 4.26 (1.10–16.57) | * 0.037 | 2.89 (0.65–12.92) | 0.164 |
| ≥3 | 12.50 (1.60–97.64) | * 0.016 | 8.31 (0.96–71.71) | 0.054 |
| Oculomotor Signals | Univariate OR (95% CI) | p-Value | Factor Score |
|---|---|---|---|
| Saccade | |||
| Horizontal | |||
| No | 1 | ||
| Yes | 1.85 (0.71–4.83) | 0.206 | |
| Vertical | |||
| No | 1 | ||
| Yes | 3.58 (1.29–9.98) | * 0.015 | 0.4981 |
| Pursuit | |||
| Horizontal | |||
| No | 1 | ||
| Yes | 3.39 (1.26–9.09) | * 0.016 | 0.5120 |
| Vertical | |||
| No | 1 | ||
| Yes | 2.25 (0.84–6.03) | 0.106 | |
| Gaze | |||
| Horizontal | |||
| No | 1 | ||
| Yes | 3.06 (1.19–7.85) | * 0.020 | 0.5228 |
| Vertical | |||
| No | 1 | ||
| Yes | 4.72 (1.72–12.99) | * 0.003 | 0.4653 |
| OPK | |||
| No | 1 | ||
| Yes | 1.22 (0.44–3.36) | 0.707 | |
| OKAN | |||
| No | 1 | ||
| Yes | 2.32 (0.83–6.48) | 0.108 |
| Variables | Univariate OR (95% CI) | p-Value | Multivariate OR (95% CI) | p-Value |
|---|---|---|---|---|
| Age | ||||
| <60 years-old (n = 48) | 1 | 1 | ||
| ≥60 years-old (n = 55) | 1.30 (0.52–3.27) | 0.581 | 0.73 (0.20–2.68) | 0.632 |
| Gender | ||||
| Female | 1 | 1 | ||
| Male | 3.21 (1.25–8.23) | * 0.015 | 2.85 (0.82–9.90) | 0.100 |
| Body mass index (n = 99) | ||||
| Median (IQR) | 1.03 (0.93–1.15) | 0.528 | ||
| Asymmetric hearing loss (n = 85) | ||||
| No | 1 | |||
| Yes (>30 dB loss) | 0.42 (0.05–3.54) | 0.425 | ||
| Neurologic symptoms | ||||
| No | 1 | 1 | ||
| Yes | 15.56 (5.20–46.56) | * <0.001 | 13.45 (4.00–45.12) | * <0.001 |
| Comorbidities | ||||
| Diabetes mellitus | ||||
| No | 1 | |||
| Yes | 1.55 (0.52–4.60) | 0.432 | ||
| Hypertension | ||||
| No | 1 | |||
| Yes | 1.59 (0.63-4.00) | 0.326 | ||
| Hyperlipidemia | ||||
| No | 1 | |||
| Yes | 1.73 (0.68-4.37) | 0.251 | ||
| History of CVA | ||||
| No | 1 | |||
| Yes | 1.71 (0.29-9.94) | 0.553 | ||
| Accumulated comorbidities | ||||
| 0 | 1 | 1 | ||
| 1–2 | 1.53 (0.50–4.70) | 0.455 | 0.56 (0.11–2.79) | 0.481 |
| ≥3 | 1.73 (0.33–8.91) | 0.515 | 0.47 (0.05–4.44) | 0.506 |
| Oculomotor index | ||||
| <50% | 1 | 1 | ||
| >50% | 4.65 (1.66–12.99) | * 0.003 | 4.59 (1.28–16.44) | * 0.019 |
| Raters | Sensitivity | Specificity | PPV |
|---|---|---|---|
| Dr. A | |||
| <60 years old | 60.0% | 84.2% | 50.0% |
| ≥60 years old | 50.0% | 51.2% | 25.9% |
| Dr. B | |||
| <60 years old | 60.0% | 57.9% | 27.3% |
| ≥60 years old | 71.4% | 29.3% | 25.6% |
| Dr. A | |||
| Comorbidities: 0 | 40.0% | 100.0% | 100.0% |
| Comorbidities: 1, 2 | 62.5% | 56.3% | 32.3% |
| Comorbidities: ≥3 | 33.3% | 37.5% | 16.7% |
| Dr. B | |||
| Comorbidities: 0 | 0.0% | 65.2% | 0.0% |
| Comorbidities: 1, 2 | 87.5% | 35.4% | 31.1% |
| Comorbidities: ≥3 | 66.7% | 25.0% | 25.0% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, C.-N.; Luo, S.-D.; Chen, S.-F.; Huang, C.-W.; Chiang, P.-L.; Hwang, C.-F.; Yang, C.-H.; Ho, C.-H.; Cheng, W.-D.; Lin, C.-Y.; et al. Applicability of Oculomotor Tests for Predicting Central Vestibular Disorder Using Principal Component Analysis. J. Pers. Med. 2022, 12, 203. https://doi.org/10.3390/jpm12020203
Wu C-N, Luo S-D, Chen S-F, Huang C-W, Chiang P-L, Hwang C-F, Yang C-H, Ho C-H, Cheng W-D, Lin C-Y, et al. Applicability of Oculomotor Tests for Predicting Central Vestibular Disorder Using Principal Component Analysis. Journal of Personalized Medicine. 2022; 12(2):203. https://doi.org/10.3390/jpm12020203
Chicago/Turabian StyleWu, Ching-Nung, Sheng-Dean Luo, Shu-Fang Chen, Chi-Wei Huang, Pi-Ling Chiang, Chung-Feng Hwang, Chao-Hui Yang, Chun-Hsien Ho, Wei-De Cheng, Chung-Ying Lin, and et al. 2022. "Applicability of Oculomotor Tests for Predicting Central Vestibular Disorder Using Principal Component Analysis" Journal of Personalized Medicine 12, no. 2: 203. https://doi.org/10.3390/jpm12020203
APA StyleWu, C.-N., Luo, S.-D., Chen, S.-F., Huang, C.-W., Chiang, P.-L., Hwang, C.-F., Yang, C.-H., Ho, C.-H., Cheng, W.-D., Lin, C.-Y., & Li, Y.-L. (2022). Applicability of Oculomotor Tests for Predicting Central Vestibular Disorder Using Principal Component Analysis. Journal of Personalized Medicine, 12(2), 203. https://doi.org/10.3390/jpm12020203