Abstract
In Italy, during the COVID-19 waves two lockdowns were implemented to prevent virus diffusion in the general population. Data on antidepressant (AD) use in these periods are still scarce. This study aimed at exploring the impact of COVID-19 lockdowns on prevalence and incidence of antidepressant drug use in the general population. A population-based study using the healthcare administrative database of Tuscany was performed. We selected a dynamic cohort of subjects with at least one ADs dispensing from 1 January 2018 to 27 December 2020. The weekly prevalence and incidence of drug use were estimated across different segments: pre-lockdown (1 January 2018–8 March 2020), first lockdown (9 March 2020–15 June 2020), post-first lockdown (16 June 2020–15 November 2020) and second lockdown (16 November 2020–27 December 2020). An interrupted time-series analysis was used to assess the effect of lockdowns on the observed outcomes. Compared to the pre-lockdown we observed an abrupt reduction of ADs incidence (Incidence-Ratio: 0.82; 95% Confidence-Intervals: 0.74–0.91) and a slight weekly decrease of prevalence (Prevalence-Ratio: 0.997; 0.996–0.999). During the post-first lockdown AD use increased, with higher incidence- and similar prevalence values compared with those expected in the absence of the outbreak. This pandemic has impacted AD drug use in the general population with potential rebound effects during the period between waves. This calls for future studies aimed at exploring the mid–long term effects of this phenomenon.
1. Introduction
The COVID-19 pandemic caused by the SARS-CoV-2 virus has resulted in more than 228 million verified cases of virus infections and over 4.6 million COVID-19 related deaths globally [1]. Italy was one of the first countries in Europe to be hit by the new virus [2,3,4]. The emergency situation, characterized by an exponential growth of cases with high fatality rates, forced the Italian government to impose the first national lockdown from 9 March 2020 to 15 June 2020 to stop the virus spread in the general population [5]. In the following summer months, restrictions have been eased and people were allowed to work and travel. This resulted in a second large COVID-19 wave with a higher number of cases and consequent implementation of new lockdown restrictions from November 2020 to the end of December 2020 [5]. The measures adopted during the two lockdowns encompassed social distancing, smart-working, quarantine, people movement restriction, closure of non-essential activities, and limitation of the physical interactions.
The impact of stressful events on mental health has been already documented in the literature [6,7]. In particular, during the first COVID-19 wave an increased number of psychiatric diagnoses such as post-traumatic stress disorder (PTSD), depression, and anxiety were reported [7,8,9,10,11,12,13,14]. Previous studies already investigated the impact of lockdown on antidepressant drug (AD) use. In particular, some studies reported an increased use of these medications during the first wave [15,16] that in some case persist also during the subsequent period of 2020 [17,18,19,20]. On the contrary, other studies found an initial reduction of AD use during the peak of the first wave followed by an increased use in the subsequent periods [21]. Finally, some authors reported a non-significant change in psychotropic medication dispensing, including ADs, during the outbreak [22]. To the best of our knowledge, evidence on the impact of lockdowns on AD use in Italy is still scant and deserves careful evaluation.
This study, therefore, aimed at assessing whether the lockdown measures implemented in Italy during COVID-19 waves influenced prevalence and incidence of AD use in the general population.
2. Materials and Methods
2.1. Data Source and Ethical Approval
The method used in this study have been already described in other publications aimed at assessing the impact of lockdown on other drug classes in the Tuscan general population [23,24]. In this observational retrospective study, the healthcare administrative database (HAD) of Tuscany was used, covering approximately 3.6 million inhabitants. The HAD contains data on healthcare services accesses in the regional area, reimbursed by the Italian Healthcare System (NHS) to all regional citizens. The HADs consulted for this study included: (i) the archive of demographic and administrative data of individuals living in the catchment area who receive national healthcare service assistance; and (ii) the pharmacy claim registry that provides information (i.e., dispensing date, number of packages, substance name, anatomical therapeutic chemical code [ATC] and defined daily dose [DDD]) on all community prescription reimbursed by the NHS [25]. Approval for the study was obtained from the “Agenzia Regionale di Sanità della Toscana” Internal Governance Board.
2.2. Study Cohorts
All individuals with at least one dispensing of ADs (ATC: N06A*) between 1 January 2018 and 27 December 2020 were selected. The date of the first AD dispensing in the period was considered as the index date in the study. Subjects registered in the HAD less than 1 year before the index date were excluded from the cohort. Each patient was followed from the index date until 27 December 2020 or death/emigration, whichever came first.
2.3. Exposure Definition
During follow-up, patients were considered exposed to ADs when they claimed an AD dispensing of the same drug class (selective serotonin reuptake inhibitors—SSRIs, other antidepressants and tricyclic antidepressants). They were considered exposed until the end of duration of their last consecutive AD dispensing (treatment episode). We considered a dispensing as consecutive if it was claimed within the duration of the prior dispensing plus a 30-day grace period, which was added to account for irregular refill patterns and minor non-compliance. The duration of each dispensing was calculated by dividing the total quantity of active substance dispensed by the relevant defined daily dose (DDD) [26,27]. The number of treatment episodes was used to estimate the number of patients with incidental or prevalent AD use in each week of the study period. Patients switching therapy or using concomitantly more than one AD in the week, were counted as just one user.
2.4. Outcomes and Definitions
The outcomes of interest were weekly prevalence and incidence of AD use during the observation period. In particular, the weekly prevalence of AD use was calculated by dividing the weekly number of patients under AD treatment by the number of inhabitants living in the region at 1 January of each corresponding calendar year as reference population [28]. Similarly, the weekly incidence of AD use was estimated by including only patients who started an incident treatment episode at the numerator and the same reference population. For each treatment episode, we classified the patient as incident if he/she did not have an AD dispensed in the year prior the starting date of the treatment episode. During the study period, patients might have had more than one incident treatment episode.
2.5. Statistical Analysis
First, we estimated the weekly prevalence and incidence of ADs use in each segment of the study period: pre-lockdown period from 1 January 2018 to 8 March 2020 (114 weeks), the first lockdown from 9 March 2020 to 15 June 2020 (14 weeks), the post-First lockdown from 16 June 2020 to 15 November 2020 (22 weeks) and the initial period of second lockdown from 16 November 2020 to 27 December 2020 (6 weeks). Second, the impact of lockdown restrictions on the study outcomes was assessed by performing an interrupted time series (ITS) analysis with a quasi-Poisson generalized additive model [29,30,31]. The model included the weekly count of the observed outcome as response variable (Y) and the reference population as offset variable to transform the count outcome in incidence or prevalence. The fitted model was of the following form:
Log [E(Yi)] = β0 + f (weeki) + β1I (holidayi) + β2I (First lockdowni) + β3 (First lockdown weeki) + β4I (Post-First lockdowni) + β5 (Post-First lockdown weeki) + β6I (Second lockdowni) + β7 (Second lockdown weeki).
The model included a non-linear function of the week (f(weeki), spline function) and a dummy holiday indicator (0 = no, 1 = yes) to account for time trend and seasonality. Model coefficients were: β0, which represents the baseline level of outcome during the pre-lockdown period; β2, β4 and β6 which estimate the level change during first, post and second lockdown, respectively and β3, β5 and β7 which estimate the trends/slopes of the time series during the aforementioned periods [31,32]. Negative βi coefficients indicate reduction over the corresponding period. In the model, a level change means an abrupt effect of the intervention whereas a change in trend/slope represents a gradual change in the estimated outcome [31]. In this specific case, a level change indicated an immediate and sustained effect on drug use, whereas a trend/slope change imply that the use of the antidepressants changed gradually in the studied segment. Next, we also investigated a possible delayed effect of lockdown restrictions implementation or cancellation, using the delayed or “lagged” level and slope indicators for all segments.
Finally, we plotted graphs of the outcomes over time to illustrate trends. Statistical significance of the parameters and the goodness of fit of the model were used to choose the best model. Significance was defined as a p-value less than 0.05. The models were implemented separately for each outcome.
In this study both the data processing and data analysis were performed using the R studio software (version 4.0.2 Rstudio, PBC: Boston, MA, USA).
2.6. Patient and Public Involvement
The research was conceived and performed by public institutions. All authors are employed or collaborate with public institutions.
3. Results
3.1. Prevalence of Drug Use
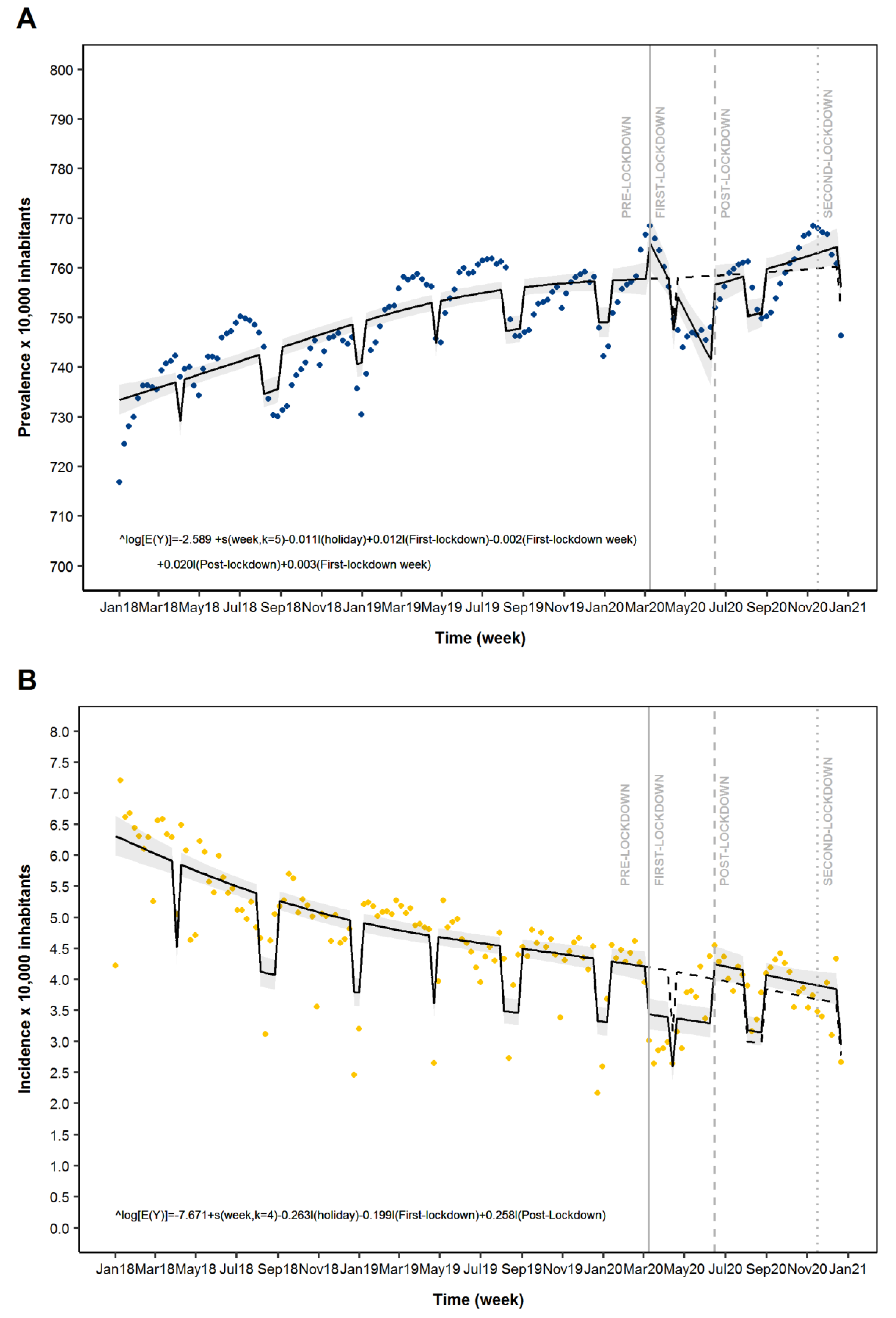
As reported in Table 1 and Figure 1A, a variation of the ADs prevalence was observed during the COVID-19 pandemic. In particular, the ITS analysis suggested a slight increase of weekly prevalence of ADs use in the first week of the first lockdown (Prevalence Ratio: 1.01; 95% CI: 1.00–1.02) followed by a weekly reduction (0.997; 0.996–0.999) for the entire first lockdown segment. During the post-First lockdown segment we observed a level change indicating a rapid increase of AD prevalence (1.02; 1.01–1.03) in the first week and slope change (1.002; 1.001–1.003) indicating a weekly increase of the prevalence for the rest of the period (Table 1 and Figure 1A). During the initial phase of second lockdown, no significant variation in AD prevalence was observed (Table 1 and Figure 1A).

Table 1.
Time series analysis of antidepressants drug use across different time segments: Pre-Lockdown, First Lockdown, Post-First Lockdown and Second Lockdown.
Figure 1.
Time series analysis of antidepressant drugs (ADs) use across different periods: Pre-Lockdown, First-Lockdown, Post-First Lockdown and Second-Lockdown. Legend: Panel (A): Prevalence of AD use; Panel (B): Incidence of AD use. Blue dots: estimated prevalence of AD drug use; Orange dots: estimated incidence of AD drug use; solid line: predicted model based on estimated outcome; Grey zone: 95% CI of the predicted model; Dashed line: expected scenario in the absence of LMI.
3.2. Incidence of Drug Use
In the study period, a variation in the trend of AD incidence was observed in the Tuscan general population across the different segments (Figure 1B). As shown in Table 2, individuals were mainly female and aged 40 years and older. Among the study ADs drug classes, the most used was the selective serotonin reuptake inhibitors (SSRIs), whereas the less used were tricyclic ADs (Figure A1). As reported in Figure 1B, a level change, indicating an abrupt reduction of the AD incidence was observed during the first week of the first lockdown segment (Incidence Ratio: 0.82; 95% CI: 0.74–0.91). At post-First lockdown a level change, which indicates a rapid increase of AD incidence (1.30; 1.16–1.45) in the first week, was shown. During the initial phase of second lockdown, no significant variation was observed (Figure 1B and Table 1).
Table 2.
Demographic characteristics of incident AD users across different time segments: Pre-Lockdown, First Lockdown, Post-First Lockdown and Second Lockdown.
4. Discussion
The findings of this observational descriptive study showed that an abrupt reduction of AD incidence and a gradual reduction of AD prevalence occurred in the general population during the first lockdown. This initial reduction was followed by new increase of both prevalence and incidence during the subsequent periods (post-first lockdown and second lockdown). In particular, the AD prevalence reverted to values similar to those registered in the pre-lockdown period following the secular trend. On the contrary, after the first-lockdown the AD incidence reached higher values compared with expected values in case of no lockdown measures implementation.
Our data on AD use during the first lockdown appeared to be consistent with those reported in previous studies from Italy and other European countries that analysed mental health services access during the first lockdown [33,34,35,36]. The first COVID-19 outbreak has disrupted these services in most countries, especially during the first weeks of lockdown implementation. This might have caused an abrupt reduction of new diagnosis of psychiatric diseases with consequent reduction of new treatment cycle initiation. In parallel, the slight increase of the AD prevalence observed around the first week of the first lockdown and its subsequent reduction during the following weeks might result by combination of two phenomena. In fact, it is possible to speculate that during the early phase of virus spread (end of February) stress, worries and fear may have been the precursor of clinical exacerbation of existing anxiety/depression symptoms with consequent re-initiation of AD treatment in patients who had previously used ADs. On the contrary, during the subsequent weeks of lockdown patients might have been more reluctant to seek treatment, following the pattern of behaviour already described in other medical fields [34]. It is also possible that during the COVID-19 outbreak physicians were less prone to prescribe ADs to these patients by preferring other alternatives such as benzodiazepines. This hypothesis is supported by findings from Balestri and colleagues that documented an increased use of benzodiazepines in the psychiatric setting during the first lockdown [37].
During the post-first lockdown period, an increased use of ADs was registered. In particular, our results showed that the AD prevalence returned to pre-lockdown levels, whereas the number of new AD treatments were higher during this period compared with expected values in case of no lockdown measures implementation. In this regard, it should be noted that during the last phase of the first-lockdown and subsequent periods, several digital solutions were implemented to guarantee medical assistance to psychiatry patients [38]. This might have represented a crucial event for medical/therapeutic assistance to patients who experienced anxiety/depression symptoms onset during the last part of the first lockdown and those who had symptoms exacerbation with consequent mental health problems [39,40]. Additionally, data on incidence of drug use might also suggest a potential rebound/mid-long term effect of lockdown. In fact, it is possible to speculate that the emergency situation might have contribute to development of mental problems in individuals without pre-existing mental health problems who were resilient during the early phase of lockdown [37,41]. In this regard, stressors such as fear of contagion, long quarantine, isolation and movement restriction, lack of information, financial loss, inadequate supplies and stigma, and loss of relatives due to COVID-19 might have contributed to the deterioration in psychological outcomes with consequent onset of anxiety, depression and related symptoms [42,43,44].
The mid/long term consequences of the under-diagnosis and under-treatment of anxiety and depression during the first lockdown are still under-investigation. Previous studies suggested that an increase in psychiatric disorders and suicidal ideations and attempts might appear several months after stressful events even if a temporary reduction might be observed during the emergency situation [45,46,47,48,49]. This highlights the need of continuous monitoring of patients with psychiatry problems under exceptional circumstances like future COVID-19 waves. From clinical point of view, our findings suggest the necessity to encourage new tools such as telemedicine in order to guarantee medical assistance to psychiatric patients. This could be crucial to reduce the risk of adverse events due to non-optimal drug treatment. Additionally, telemedicine could increase also the effect of non-pharmacological management of these patients contributing to the aforementioned events improvements.
Future research should be performed to investigate whether new users of ADs during the pandemic outbreak had different demographic and clinical characteristics compared with those who started an AD treatment in the pre-lockdown period. In addition, new studies are warranted to investigate the potential consequence associated with the observed variations in AD use in the study population.
Strengths and Limitations
An important strength of this study is that data related to an unselected population from one of the largest Italian regions, which accounts for over over 3.5 million of inhabitants. This study has some limitations. First, in Italy both ADs and anxiolytic drugs (i.e., benzodiazepines) are indicated for the treatment of the mental health symptoms after traumatic events. However, in Italy only ADs are fully reimbursed by the NHS and thus captured in the HAD, while the cost of anxiolytics is totally charged to patients. As a consequence, data about benzodiazepines use is generally not available in the Italian HAD. Moreover, the study did not include information about drug indications because in Italy this information is not available in the HAD. Additionally, for the second lockdown we included only six data points, which is slightly lower than the minimum number of points (eight) required to have robust estimates, therefore the results on the second lockdown should be considered with caution. Finally, as per study design we were not able to ensure a causal correlation between COVID-19 waves and studied outcomes, although the observed changes in the ADs use occurred around the studied events.
5. Conclusions
In conclusion, we found a change in AD use during pandemic lockdowns in the general population. There was a reduction of both prevalence and incidence of AD use during the first lockdown that reversed during the post-first lockdown reaching higher value compared with the expected results observed in the counterfactual scenario. The potential under-treatment occurred during the pandemic waves might be associated with increased risk of negative events (i.e., suicidal attempts) occurrence in the general population. These findings might be used to implement strategies to ensure access to adequate mental healthcare services for vulnerable population during extreme circumstances such as lockdown periods.
Author Contributions
Conceptualization, I.C.A., C.F., L.G.M., R.G. and G.M.; Methodology: I.C.A., C.F., S.M.-R., R.G. and G.M.; data curation: C.F., E.C., O.P., R.G.; formal analysis: C.F., E.C., O.P., R.G.; writing original draft preparation: I.C.A., C.F. and G.M.; writing—review and editing: all authors. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This is an observational, non-interventional database study, reutilising administrative data for the purpose of addressing a research question. The Agenzia regionale di Sanità della Toscana has general legal and ethical frameworks that allow conducting research by making secondary use of administrative data, upon approval of an internal governance board. Permission to contribute to this study was granted by the governance boards of the Agenzia regionale di Sanità della Toscana.
Informed Consent Statement
Not applicable. The Agenzia regionale di Sanità della Toscana has general legal and ethical frameworks that allow conducting research by making secondary use of administrative data, upon approval of an internal governance board.
Data Availability Statement
Not applicable.
Conflicts of Interest
I.C.A., C.F., S.C., P.F., P.C. and G.M. have no disclosure to declare. L.G.M. reported receiving grants from Bayer, Daiiki-Sankyo, and Boehringer Ingelheim outside the submitted work and speaker fees from Pfizer and Bayer. O.P. and R.G. are employed by ARS, a public health agency that conducts or participates in pharmacoepidemiology studies compliant with the ENCePP Code of Conduct. The budget of ARS is partially sustained by such studies. S.M.-R. is part of DRUGS-SAFER centre of pharmacoemidemiology, which is granted by the Agence Nationale de Sécurité du Médicament et des Produits de Santé (French Medicine Agency). The centre is conducting drug utilization studies on the impact of COVID-19, in which SMR is not involved.
Appendix A
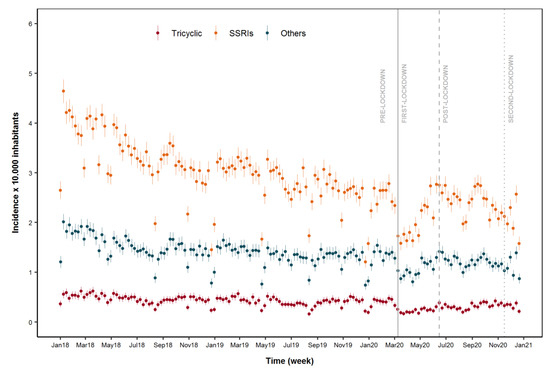
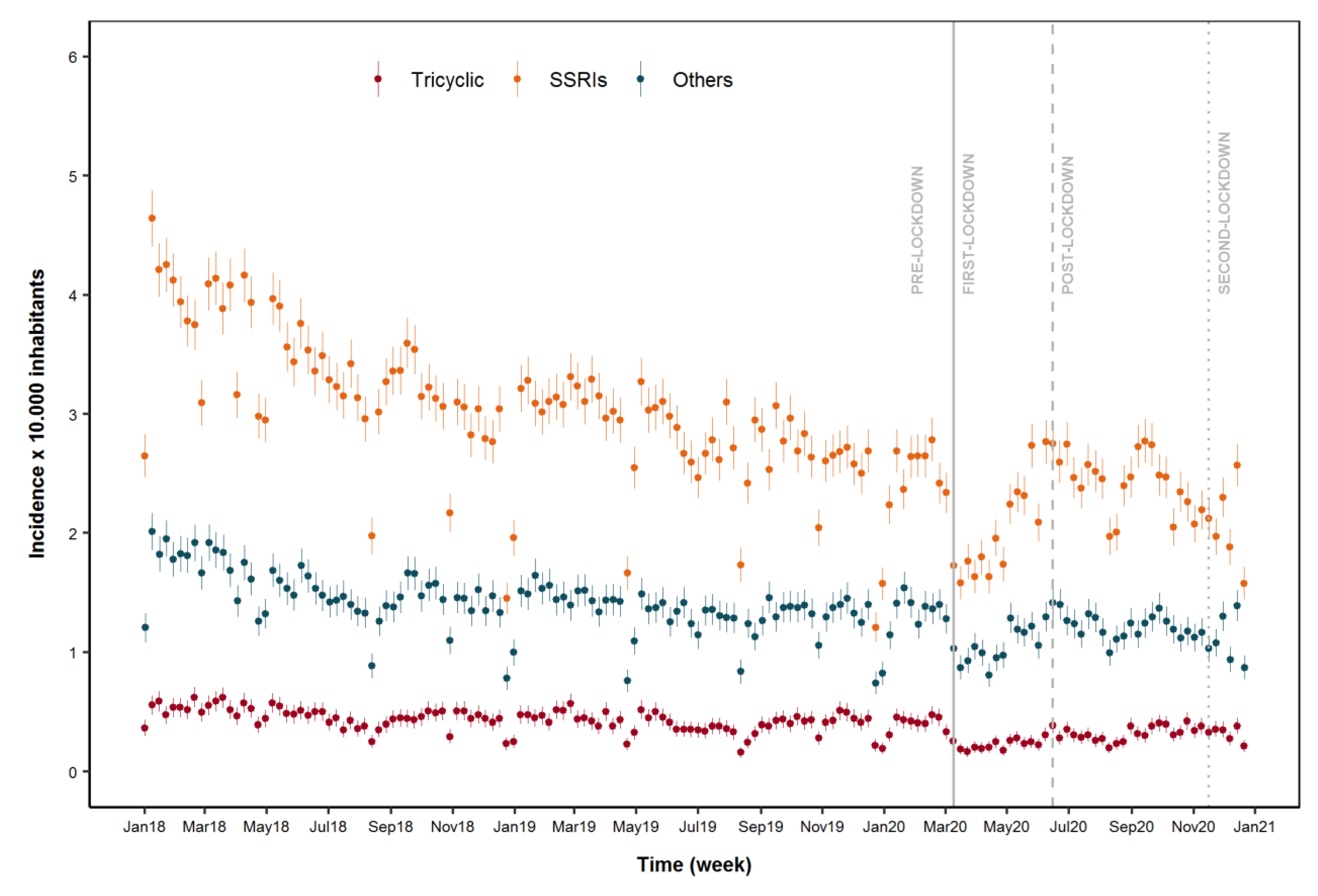
Figure A1.
Incidence of different antidepressant drugs (ADs) classes use in the general population in the study period. Legend: Orange dots: estimated incidence of Selective Serotonin Reuptake inhibitors (SSRIs); blue dots: estimated incidence of Others antidepressants and red dots: estimated incidence of tricyclic antidepressants.
Figure A1.
Incidence of different antidepressant drugs (ADs) classes use in the general population in the study period. Legend: Orange dots: estimated incidence of Selective Serotonin Reuptake inhibitors (SSRIs); blue dots: estimated incidence of Others antidepressants and red dots: estimated incidence of tricyclic antidepressants.
References
- World Health Organization (WHO). WH Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 10 October 2021).
- Helmy, Y.A.; Fawzy, M.; Elaswad, A.; Sobieh, A.; Kenney, S.P.; Shehata, A.A. The COVID-19 Pandemic: A Comprehensive Review of Taxonomy, Genetics, Epidemiology, Diagnosis, Treatment, and Control. J. Clin. Med. 2020, 9, 1225. [Google Scholar] [CrossRef] [PubMed]
- Sharma, R.; Agarwal, M.; Gupta, M.; Somendra, S.; Saxena, S.K. Clinical characteristics and differential clinical diagnosis of novel coronavirus disease 2019 (COVID-19). Coronavirus Dis. 2020; 9, 55–70. [Google Scholar] [CrossRef]
- Conti, S.; Ferrara, P.; Mazzaglia, G.; D’Orso, M.I.; Ciampichini, R.; Fornari, C.; Madotto, F.; Magoni, M.; Sampietro, G.; Silenzi, A.; et al. Magnitude and time-course of excess mortality during COVID-19 outbreak: Population-based empirical evidence from highly impacted provinces in northern Italy. ERJ Open Res. 2020, 6, 00458–2020. [Google Scholar] [CrossRef] [PubMed]
- Official Gazette of the Italian Republic. DPCM 22 marzo 2020. Ulteriori Disposizioni Attuative del Decreto-Legge 23 Febbraio 2020, n. 6, Recante Misure Urgenti in Materia di Contenimento e Gestione Dell’emergenza Epidemiologica da COVID-19, Applicabili Sull’intero Territorio Nazionale. n. 76 del 22 Marzo 2020. 2020. Available online: http://www.governo.it/it/articolo/coronavirus-firmato-il-dpcm-22-marzo-2020/14363 (accessed on 20 December 2020).
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- COVID-19 Mental Disorders Collaborators. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet 2021, 398, 1700–1712. [Google Scholar] [CrossRef]
- Jacob, L.; Smith, L.; Koyanagi, A.; Oh, H.; Tanislav, C.; Shin, J.I.; Konrad, M.; Kostev, K. Impact of the coronavirus 2019 (COVID-19) pandemic on anxiety diagnosis in general practices in Germany. J. Psychiatr. Res. 2020, 143, 528–533. [Google Scholar] [CrossRef] [PubMed]
- Bäuerle, A.; Teufel, M.; Musche, V.; Weismüller, B.; Kohler, H.; Hetkamp, M.; Dörrie, N.; Schweda, A.; Skoda, E.-M. Increased generalized anxiety, depression and distress during the COVID-19 pandemic: A cross-sectional study in Germany. J. Public Health 2020, 42, 672–678. [Google Scholar] [CrossRef] [PubMed]
- Kamal, N.M.; Othman, N. Depression, Anxiety, and Stress in the time of COVID-19 Pandemic in Kurdistan Region, Iraq. Kurd. J. Appl. Res. 2020, 37–44. [Google Scholar] [CrossRef]
- Mazza, C.; Ricci, E.; Biondi, S.; Colasanti, M.; Ferracuti, S.; Napoli, C.; Roma, P. A Nationwide Survey of Psychological Distress among Italian People during the COVID-19 Pandemic: Immediate Psychological Responses and Associated Factors. Int. J. Environ. Res. Public Health 2020, 17, 3165. [Google Scholar] [CrossRef]
- Moghanibashi-Mansourieh, A. Assessing the anxiety level of Iranian general population during COVID-19 outbreak. Asian J. Psychiatry 2020, 51, 102076. [Google Scholar] [CrossRef]
- Odriozola-González, P.; Planchuelo-Gómez, A.; Irurtia, M.J.; de Luis-García, R. Psychological effects of the COVID-19 outbreak and lockdown among students and workers of a Spanish university. Psychiatry Res. 2020, 290, 113108. [Google Scholar] [CrossRef]
- Stanton, R.; To, Q.G.; Khalesi, S.; Williams, S.L.; Alley, S.J.; Thwaite, T.L.; Fenning, A.S.; Vandelanotte, C. Depression, Anxiety and stress during COVID-19: Associations with changes in physical activity, sleep, tobacco and alcohol use in australian adults. Int. J. Environ. Res. Public Health 2020, 17, 4065. [Google Scholar] [CrossRef] [PubMed]
- Jones, C.M.; Guy, G.P.; Board, A. Comparing actual and forecasted numbers of unique patients dispensed select medications for opioid use disorder, opioid overdose reversal, and mental health, during the COVID-19 pandemic, United States, January 2019 to May 2020. Drug Alcohol Depend. 2021, 219, 108486. [Google Scholar] [CrossRef] [PubMed]
- Uthayakumar, S.; Tadrous, M.; Vigod, S.N.; Kitchen, S.A.; Gomes, T. The effects of COVID-19 on the dispensing rates of antidepressants and benzodiazepines in Canada. Depress. Anxiety 2021. [Google Scholar] [CrossRef] [PubMed]
- Armitage, R. Antidepressants, primary care, and adult mental health services in England during COVID-19. Lancet Psychiatry 2021, 8, e3. [Google Scholar] [CrossRef]
- Milani, S.A.; Raji, M.A.; Chen, L.; Kuo, Y.-F. Trends in the Use of Benzodiazepines, Z-Hypnotics, and Serotonergic Drugs among US Women and Men Before and During the COVID-19 Pandemic. JAMA Netw. Open 2021, 4, e2131012. [Google Scholar] [CrossRef]
- Stall, N.M.; Zipursky, J.S.; Rangrej, J.; Jones, A.; Costa, A.P.; Hillmer, M.P.; Brown, K. Assessment of Psychotropic Drug Prescribing Among Nursing Home Residents in Ontario, Canada, During the COVID-19 Pandemic. JAMA Intern. Med. 2021, 181, 861. [Google Scholar] [CrossRef]
- De Oliveira Costa, J.; Gillies, M.B.; Schaffer, A.L.; Peiris, D.; Zoega, H.; Pearson, S. Changes in antidepressant use in Australia: A nationwide analysis prior to and during the COVID-19 pandemic. MedRxiv 2021. [Google Scholar] [CrossRef]
- Carr, M.J.; Steeg, S.; Webb, R.T.; Kapur, N.; Chew-Graham, A.C.; Abel, K.M.; Hope, H.; Pierce, M.; Ashcroft, D.M. Effects of the COVID-19 pandemic on primary care-recorded mental illness and self-harm episodes in the UK: A population-based cohort study. Lancet Public Health 2021, 6, e124–e135. [Google Scholar] [CrossRef]
- Wolfschlag, M.; Grudet, C.; Håkansson, A. Impact of the COVID-19 Pandemic on the General Mental Health in Sweden: No Observed Changes in the Dispensed Amount of Common Psychotropic Medications in the Region of Scania. Front. Psychiatry 2021, 12, 731297. [Google Scholar] [CrossRef]
- Antonazzo, I.C.; Fornari, C.; Paoletti, O.; Bartolini, C.; Conti, S.; Cortesi, P.A.; Mantovani, L.G.; Gini, R.; Mazzaglia, G. COVID-19 Outbreak Impact on Anticoagulants Utilization: An Interrupted Time-Series Analysis Using Health Care Administrative Databases. Thromb. Haemost. 2021, 121, 1115–1118. [Google Scholar] [CrossRef]
- Antonazzo, I.C.; Fornari, C.; Maumus-Robert, S.; Cei, E.; Paoletti, O.; Conti, S.; Cortesi, P.A.; Mantovani, L.G.; Gini, R.; Mazzaglia, G. Impact of COVID-19 Lockdown, during the Two Waves, on Drug Use and Emergency Department Access in People with Epilepsy: An Interrupted Time-Series Analysis. Int. J. Environ. Res. Public Health 2021, 24, 13253. [Google Scholar] [CrossRef] [PubMed]
- Trifirò, G.; Gini, R.; Barone-Adesi, F.; Beghi, E.; Cantarutti, A.; Capuano, A.; Carnovale, C.; Clavenna, A.; Dellagiovanna, M.; Ferrajolo, C.; et al. The Role of European Healthcare Databases for Post-Marketing Drug Effectiveness, Safety and Value Evaluation: Where Does Italy Stand? Drug Saf. 2019, 42, 347–363. [Google Scholar] [CrossRef] [PubMed]
- Merlo, J.; Wessling, A.; Melander, A. Comparison of dose standard units for drug utilisation studies. Eur. J. Clin. Pharmacol. 1996, 50, 27–30. [Google Scholar] [CrossRef]
- Pazzagli, L.; Brandt, L.; Linder, M.; Myers, D.; Mavros, P.; Andersen, M.; Bahmanyar, S. Methods for constructing treatment episodes and impact on exposure-outcome associations. Eur. J. Clin. Pharmacol. 2019, 76, 267–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Italian Office of National Statistics—Istituto Nazionale di Statistica (ISTAT). Available online: https://www.istat.it/ (accessed on 6 June 2021).
- Penfold, R.B.; Zhang, F. Use of Interrupted Time Series Analysis in Evaluating Health Care Quality Improvements. Acad. Pediatr. 2013, 13 (Suppl. S6), S38–S44. [Google Scholar] [CrossRef] [PubMed]
- Kontopantelis, E.; Doran, T.; Springate, D.A.; Buchan, I.; Reeves, D. Regression based quasi-experimental approach when randomisation is not an option: Interrupted time series analysis. BMJ 2015, 350, h2750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, A.K.; Soumerai, S.B.; Zhang, F.; Ross-Degnan, D. Segmented regression analysis of interrupted time series studies in medication use research. J. Clin. Pharm. Ther. 2002, 27, 299–309. [Google Scholar] [CrossRef]
- Derrick, T.R.; Thomas, J.M. Time Series Analysis: The Cross-Correlation Function. Kinesiology Publications 2004 at Iowa State University Digital Repository. Available online: https://lib.dr.iastate.edu/kin_pubs/46 (accessed on 10 December 2021).
- Rømer, T.B.; Christensen, R.H.B.; Blomberg, S.N.; Folke, F.; Christensen, H.C.; Benros, M.E. Psychiatric Admissions, Referrals, and Suicidal Behavior Before and During the COVID-19 Pandemic in Denmark: A Time-Trend Study. Acta Psychiatr. Scand. 2021, 144, 553–562. [Google Scholar] [CrossRef]
- Abbas, M.J.; Kronenberg, G.; McBride, M.; Chari, D.; Alam, F.; Mukaetova-Ladinska, E.; Al-Uzri, M.; Brugha, T. The Early Impact of the COVID-19 Pandemic on Acute Care Mental Health Services. Psychiatr. Serv. 2021, 72, 242–246. [Google Scholar] [CrossRef]
- Clerici, M.; Durbano, F.; Spinogatti, F.; Vita, A.; De Girolamo, G.; Micciolo, R. Psychiatric hospitalization rates in Italy before and during COVID-19: Did they change? An analysis of register data. Ir. J. Psychol. Med. 2020, 37, 283–290. [Google Scholar] [CrossRef]
- Hansen, J.P.; van Sas, T.Q.B.; Fløjstrup, M.; Brabrand, M.; Hvolby, A. The effect of the March 2020 COVID-19 lockdown on national psychiatric contacts in Denmark: An interrupted time series analysis. Brain Behav. 2021, 11, e2264. [Google Scholar] [CrossRef] [PubMed]
- Balestrieri, M.; Rucci, P.; Amendola, D.; Bonizzoni, M.; Cerveri, G.; Colli, C.; Dragogna, F.; Ducci, G.; Elmo, M.G.; Ghio, L.; et al. Emergency Psychiatric Consultations During and After the COVID-19 Lockdown in Italy. A Multicentre Study. Front. Psychiatry 2021, 12, 697058. [Google Scholar] [CrossRef] [PubMed]
- Golinelli, D.; Boetto, E.; Carullo, G.; Nuzzolese, A.G.; Landini, M.P.; Fantini, M.P. Adoption of Digital Technologies in Health Care During the COVID-19 Pandemic: Systematic Review of Early Scientific Literature. J. Med. Internet Res. 2020, 22, e22280. [Google Scholar] [CrossRef] [PubMed]
- Lima, C.K.T.; Carvalho, P.M.D.M.; Lima, I.D.A.A.S.; Nunes, J.V.A.D.O.; Saraiva, J.S.; de Souza, R.I.; da Silva, C.G.L.; Neto, M.L.R. The emotional impact of Coronavirus 2019-nCoV (new Coronavirus disease). Psychiatry Res. 2020, 287, 112915. [Google Scholar] [CrossRef]
- Yao, H.; Chen, J.-H.; Xu, Y.-F. Patients with mental health disorders in the COVID-19 epidemic. Lancet Psychiatry 2020, 7, e21. [Google Scholar] [CrossRef]
- Pacchiarotti, I.; Anmella, G.; Fico, G.; Verdolini, N.; Vieta, E. A psychiatrist’s perspective from a COVID-19 epicentre: A personal account. BJPsych Open 2020, 6, e108. [Google Scholar] [CrossRef]
- Sim, K.; Chua, H.C.; Vieta, E.; Fernandez, G. The anatomy of panic buying related to the current COVID-19 pandemic. Psychiatry Res. 2020, 288, 113015. [Google Scholar] [CrossRef]
- Fullana, M.A.; Hidalgo-Mazzei, D.; Vieta, E.; Radua, J. Coping behaviors associated with decreased anxiety and depressive symptoms during the COVID-19 pandemic and lockdown. J. Affect. Disord. 2020, 275, 80–81. [Google Scholar] [CrossRef]
- Kozloff, N.; Mulsant, B.H.; Stergiopoulos, V.; Voineskos, A.N. The COVID-19 Global Pandemic: Implications for People with Schizophrenia and Related Disorders. Schizophr. Bull. 2020, 46, 752–757. [Google Scholar] [CrossRef]
- Claassen, C.A.; Carmody, T.; Stewart, S.M.; Bossarte, R.M.; Larkin, G.L.; Woodward, W.A.; Trivedi, M.H. Effect of 11 September 2001 terrorist attacks in the USA on suicide in areas surrounding the crash sites. Br. J. Psychiatry 2010, 196, 359–364. [Google Scholar] [CrossRef] [Green Version]
- Osman, M.; Parnell, A.C. Effect of the First World War on suicide rates in Ireland: An investigation of the 1864–1921 suicide trends. BJPsych Open 2015, 1, 164–165. [Google Scholar] [CrossRef] [Green Version]
- Batty, G.; Kivimäki, M.; Bell, S.; Gale, C.R.; Shipley, M.; Whitley, E.; Gunnell, D. Psychosocial characteristics as potential predictors of suicide in adults: An overview of the evidence with new results from prospective cohort studies. Transl. Psychiatry 2018, 8, 22. [Google Scholar] [CrossRef] [Green Version]
- Cobo, A.; Porras-Segovia, A.; Pérez-Rodríguez, M.M.; Artés-Rodríguez, A.; Barrigón, M.L.; Courtet, P.; Baca-García, E. Patients at high risk of suicide before and during a COVID-19 lockdown: Ecological momentary assessment study. BJPsych Open 2021, 7, e82. [Google Scholar] [CrossRef]
- Boldrini, T.; Girardi, P.; Clerici, M.; Conca, A.; Creati, C.; Di Cicilia, G.; Ducci, G.; Durbano, F.; Maci, C.; Maone, A.; et al. Consequences of the COVID-19 pandemic on admissions to general hospital psychiatric wards in Italy: Reduced psychiatric hospitalizations and increased suicidality. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 110, 110304. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).