
MRI and Ultrasound Analysis of Corticosteroid Injection Combined with Extracorporeal Shockwave Therapy in Lateral Epicondylitis—A Prospective, Randomized, Double-Blinded, Placebo-Controlled Trial

 ,
,  , , ,
, , ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
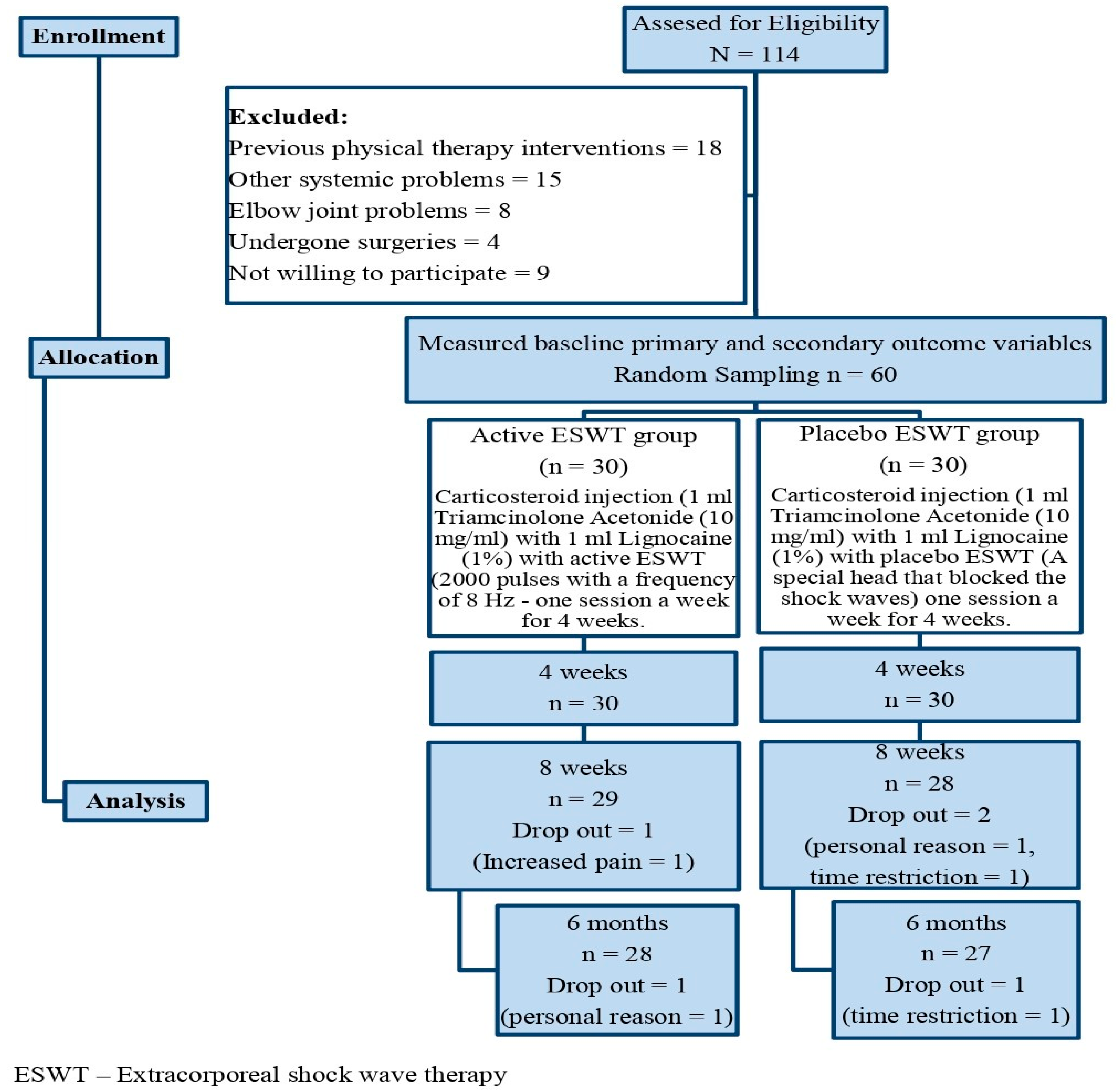
2.1. Trial Design
2.2. Participants
2.3. Interventions
2.3.1. Corticosteroid Injection
2.3.2. Physical Therapy
2.4. Outcome Measures
2.4.1. Pain Intensity
2.4.2. Magnetic Resonance Imaging (MRI)
2.4.3. Ultrasound (US) Imaging
2.4.4. Functional Disability
2.4.5. Handgrip Strength
2.4.6. Patient Perception
2.4.7. Kinesiophobia
2.4.8. Depression
2.4.9. Quality of Life
2.5. Sample Size
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shiri, R.; Viikari-Juntura, E.; Varonen, H.; Heliovaara, M. Prevalence and determinants of lateral and medial epicondylitis: A population study. Am. J. Epidemiol. 2006, 164, 1065–1074. [Google Scholar] [CrossRef] [PubMed]
- Vaquero-Picado, A.; Barco, R.; Antuña, S.A. Lateral epicondylitis of the elbow. EFORT Open Rev. 2016, 1, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Vukelic, B.; Abbey, R.; Knox, J.; Migdalski, A.; Guthmann, R. Which injections are effective for lateral epicondylitis? J. Fam. Pract. 2021, 70, 461–463. [Google Scholar] [CrossRef] [PubMed]
- Kemp, J.A.; Olson, M.A.; Tao, M.A.; Burcal, C.J. Platelet-Rich Plasma versus Corticosteroid Injection for the Treatment of Lateral Epicondylitis: A Systematic Review of Systematic Reviews. Int. J. Sport. Phys. Ther. 2021, 16, 597–605. [Google Scholar] [CrossRef] [PubMed]
- Bisset, L.; Beller, E.; Jull, G.; Brooks, P.; Darnell, R.; Vicenzino, B. Mobilisation with movement and exercise, corticosteroid injection, or wait and see for tennis elbow: Randomised trial. BMJ 2006, 333, 939. [Google Scholar] [CrossRef] [PubMed]
- Coombes, B.K.; Bisset, L.; Brooks, P.; Khan, A.; Vicenzino, B. Effect of corticosteroid injection, physiotherapy, or both on clinical outcomes in patients with unilateral lateral epicondylalgia: A randomized controlled trial. JAMA 2013, 309, 461–469. [Google Scholar] [CrossRef]
- Tonks, J.H.; Pai, S.K.; Murali, S.R. Steroid injection therapy is the best conservative treatment for lateral epicondylitis: A prospective randomised controlled trial. Int. J. Clin. Pract. 2007, 61, 240–246. [Google Scholar] [CrossRef]
- Olaussen, M.; Holmedal, O.; Lindbaek, M.; Brage, S.; Solvang, H. Treating lateral epicondylitis with corticosteroid injections or non-electrotherapeutical physiotherapy: A systematic review. BMJ Open 2013, 3, e003564. [Google Scholar] [CrossRef]
- Newcomer, K.L.; Laskowski, E.R.; Idank, D.M.; McLean, T.J.; Egan, K.S. Corticosteroid injection in early treatment of lateral epicondylitis. Clin. J. Sport Med. 2001, 11, 214–222. [Google Scholar] [CrossRef]
- Taheri, P.; Emadi, M.; Poorghasemian, J. Comparison the Effect of Extra Corporeal Shockwave Therapy with Low Dosage Versus High Dosage in Treatment of the Patients with Lateral Epicondylitis. Adv. Biomed. Res. 2017, 6, 61. [Google Scholar] [PubMed]
- Chung, B.; Wiley, J.P. Effectiveness of extracorporeal shock wave therapy in the treatment of previously untreated lateral epicondylitis: A randomized controlled trial. Am. J. Sports Med. 2004, 32, 1660–1667. [Google Scholar] [CrossRef] [PubMed]
- Helbig, K.; Herbert, C.; Schostok, T.; Brown, M.; Thiele, R. Correlations between the duration of pain and the success of shock wave therapy. Clin. Orthop. 2001, 387, 68–71. [Google Scholar] [CrossRef] [PubMed]
- Bachta, A.; Rowicki, K.; Kisiel, B.; Zabicka, M.; Kopec, S.E.; Plominski, J.; Tlustochowicz, W.; Maliborski, A. Ultrasonography versus magnetic resonance imaging in detecting and grading common extensor tendon tear in chronic lateral epicondylitis. PLoS ONE 2017, 12, e0181828. [Google Scholar] [CrossRef] [PubMed]
- Jeon, J.Y.; Lee, M.H.; Jeon, I.H.; Chung, H.W.; Lee, S.H.; Shin, M.J. Lateral epicondylitis: Associations of MR imaging and clinical assessments with treatment options in patients receiving conservative and arthroscopic managements. Eur. Radiol. 2018, 28, 972–981. [Google Scholar] [CrossRef]
- Coombes, B.K.; Bisset, L.; Connelly, L.B.; Brooks, P.; Vicenzino, B. Optimising corticosteroid injection for lateral epicondylalgia with the addition of physiotherapy: A protocol for a randomised control trial with placebo comparison. BMC Musculoskelet. Disord. 2009, 10, 76. [Google Scholar] [CrossRef]
- Maffulli, G.; Hemmings, S.; Maffulli, N. Assessment of the Effectiveness of Extracorporeal Shock Wave Therapy (ESWT) For Soft Tissue Injuries (ASSERT): An Online Database Protocol. Transl. Med. UniSa 2014, 10, 46–51. [Google Scholar]
- Raman, J.; MacDermid, J.C.; Grewal, R. Effectiveness of different methods of resistance exercises in lateral epicondylosis—A systematic review. J. Hand Ther. 2012, 25, 5–26. [Google Scholar] [CrossRef]
- Emshoff, R.; Bertram, S.; Emshoff, I. Clinically important difference thresholds of the visual analog scale: A conceptual model for identifying meaningful intra individual changes for pain intensity. Pain 2011, 152, 2277–2282. [Google Scholar] [CrossRef]
- Marks, M.; Rickenbacher, D.; Audigé, L.; Glanzmann, M.C. Patient-Rated Tennis Elbow Evaluation (PRTEE). Z. Orthop. Unfall. 2021, 159, 391–396. [Google Scholar] [CrossRef]
- Fischer, D.; Stewart, A.L.; Bloch, D.A.; Lorig, K.; Laurent, D.; Holman, H. Capturing the patient’s view of change as a clinical outcome measure. JAMA 1999, 282, 1157–1162. [Google Scholar] [CrossRef]
- Kortlever, J.T.P.; Karyampudi, P.; Ottenhoff, J.S.E.; Ring, D.; Vagner, G.A.; Reichel, L.M. Using the Tampa Scale for Kinesiophobia Short Form in Patients with Upper Extremity Specific Limitations. Hand 2021, 16, 847–853. [Google Scholar] [CrossRef]
- Cassiani-Miranda, C.A.; Scoppetta, O.; Cabanzo-Arenas, D.F. Validity of the Hospital Anxiety and Depression Scale (HADS) in primary care patients in Colombia. Gen. Hosp. Psychiatry 2021, 74, 102–109. [Google Scholar] [CrossRef]
- Feng, Y.S.; Kohlmann, T.; Janssen, M.F.; Buchholz, I. Psychometric properties of the EQ-5D-5L: A systematic review of the literature. Qual. Life Res. 2021, 30, 647–673. [Google Scholar] [CrossRef] [PubMed]
- Olaussen, M.; Holmedal, Ø.; Mdala, I.; Brage, S.; Lindbæk, M. Corticosteroid or placebo injection combined with deep transverse friction massage, Mills manipulation, stretching and eccentric exercise for acute lateral epicondylitis: A randomised, controlled trial. BMC Musculoskelet. Disord. 2015, 16, 122. [Google Scholar] [CrossRef]
- Smidt, N.; Assendelft, W.J.; van der Windt, D.A.; Hay, E.M.; Buchbinder, R.; Bouter, L.M. Corticosteroid injections for lateral epicondylitis: A systematic review. Pain 2002, 96, 23–40. [Google Scholar] [CrossRef]
- Wolf, J.M.; Ozer, K.; Scott, F.; Gordon, M.J.; Williams, A.E. Comparison of autologous blood, corticosteroid, and saline injection in the treatment of lateral epicondylitis: A prospective, randomized, controlled multicenter study. J. Hand Surg. Am. 2011, 36, 1269–1272. [Google Scholar] [CrossRef]
- Marwaha, V.; Pawah, A.K.J.; Kumar, K.V.S.H. Combined steroid and lignocaine injection in resistant cases of tennis elbow: A prospective, interventional study from India. J. Family Med. Prim. Care 2017, 6, 498–501. [Google Scholar] [PubMed]
- Kubot, A.; Grzegorzewski, A.; Synder, M.; Szymczak, W.; Kozłowski, P. Radial Extracorporeal Shockwave Therapy and Ultrasound Therapy in the Treatment of Tennis Elbow Syndrome. Ortop. Traumatol. Rehabil. 2017, 19, 415–426. [Google Scholar] [CrossRef] [PubMed]
- Gunduz, R.; Malas, F.U.; Borman, P.; Kocaoglu, S.; Ozcakar, L. Physical therapy, corticosteroid injection, and extracorporeal shock waves treatment in lateral epicondylitis: Clinical and ultrasonographical comparison. Clin. Rheumatol. 2012, 31, 807–812. [Google Scholar] [CrossRef]
- Krol, P.; Franek, A.; Durmała, J.; Blaszczak, E.; Ficek, K.; Krol, B.; Detko, E.; Wnuk, B.; Bialek, L.; Taradaj, J. Focused and Radial Shock Wave Therapy in the Treatment of Tennis Elbow: A Pilot Randomised Controlled Study. J. Hum. Kinet. 2015, 14, 127–135. [Google Scholar] [CrossRef]
- Cha, Y.K.; Kim, S.J.; Park, N.H.; Kim, J.Y.; Kim, J.H.; Park, J.Y. Magnetic resonance imaging of patients with lateral epicondylitis: Relationship between pain and severity of imaging features in elbow joints. Acta Orthop Traumatol Turc. 2019, 53, 366–371. [Google Scholar] [CrossRef] [PubMed]
- Alizadehkhaiyat, O.; Fisher, A.C.; Kemp, G.J.; Vishwanathan, K.; Frostick, S.P. Assessment of functional recovery in tennis elbow. J. Electromyogr. Kinesiol. 2009, 19, 631–638. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Sr. No | Variable | Active ESWT (n = 30) | Placebo ESWT (n = 30) | p-Value |
|---|---|---|---|---|
| 1 | Age (y) | 47.12 ± 3.2 | 46.56 ± 4.1 | n.s. |
| 2 | Height (m) | 1.68 ± 0.16 | 1.67 ± 0.18 | n.s. |
| 3 | Weight (kg) | 68.8 ± 4.3 | 69.2 ± 4.8 | n.s. |
| 4 | Side involved (%) | |||
| Right side | 24 (80%) | 23 (77%) | n.s. | |
| Left side | 5 (17%) | 6 (20%) | n.s. | |
| Bilateral | 1 (4%) | 1 (4%) | n.s. | |
| 5 | Dominance side affected (%) | |||
| Dominance = Right | 21/28 (75%) | 21/27 (78%) | n.s. | |
| Dominance = Left | 1/2 (50%) | 1/3 (34%) | n.s. | |
| 6 | Previous episodes of LE, N (%) | 4/30 (13%) | 4/30 (13%) | n.s. |
| 7 | Duration of pain (m) | 4.1 ± 2.5 | 3.2 ± 2.9 | n.s. |
| 8 | Education level | |||
| School level | 2/30 (7%) | 2/30 (7%) | n.s. | |
| Bachelor | 18/30 (60%) | 16/30 (53%) | n.s. | |
| Master | 7/30 (23%) | 10/30 (33%) | n.s. | |
| PhD | 3/30 (10%) | 2/30 (7%) | n.s. | |
| 9 | Employment | |||
| Manual work | 19/30 (63%) | 21/30 (78%) | n.s. | |
| Non-manual work | 7/30 (23%) | 6/30 (20%) | n.s. | |
| Not working | 4/30 (13%) | 3/30 (10%) | n.s. | |
| 10 | Percentage of tear | |||
| Low grade (less than 20%) | 6/30 (20%) | 5/30 (17%) | n.s. | |
| Intermediate grade (20–80%) | 22/30 (73%) | 23/30 (77%) | n.s. | |
| High grade (more than 80%) | 2/30 (7%) | 2/30 (7%) | n.s. |
| Sr. No | Variable | Duration | Active | Placebo | p-Value |
|---|---|---|---|---|---|
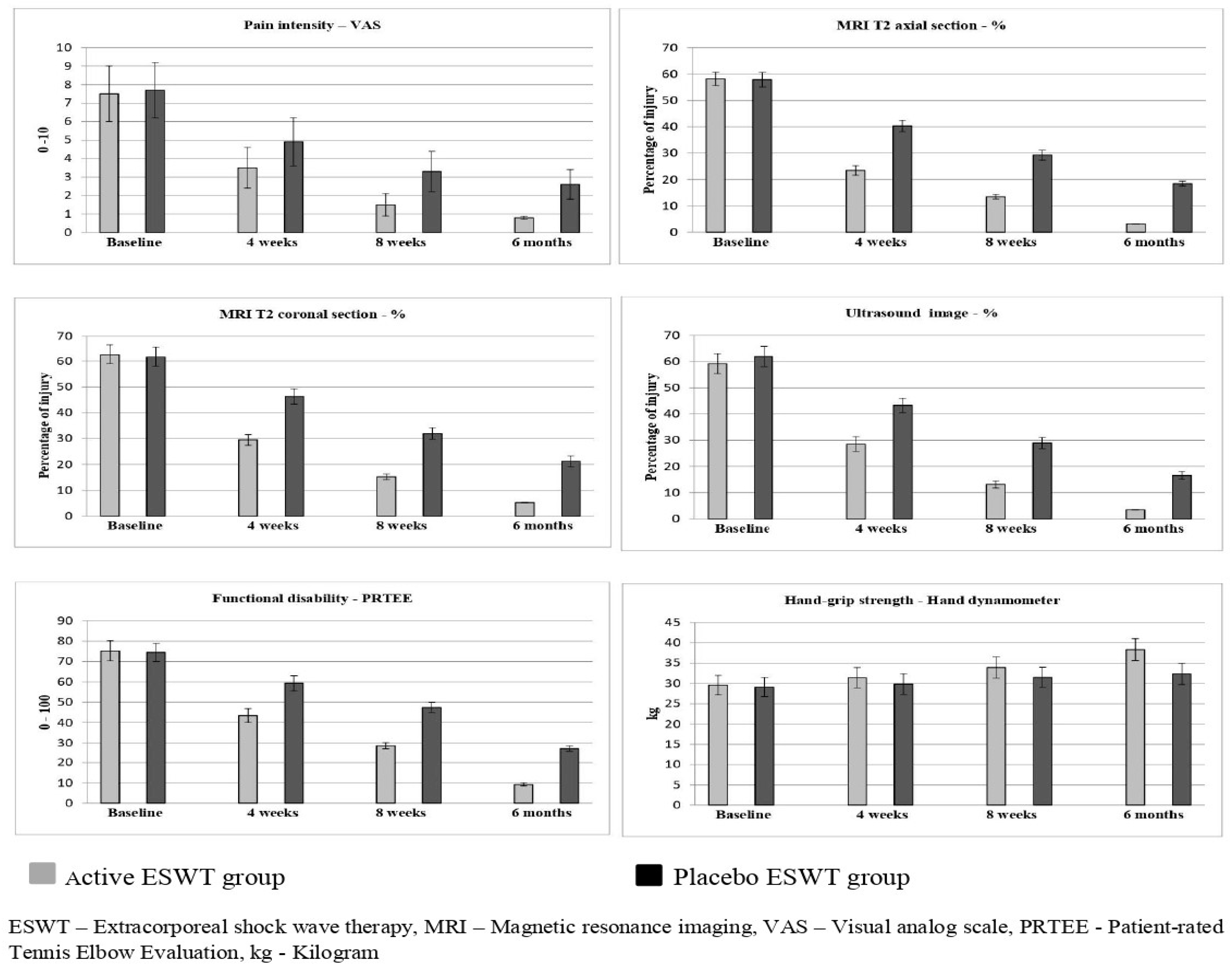
| 1 | Pain intensity—VAS (0–10 cm) | Baseline | 7.5 ± 1.5 | 7.7 ± 1.5 | 0.607 |
| 4 weeks | 3.5 ± 1.1 | 4.9 ± 1.3 | 0.001 * | ||
| 8 weeks | 1.5 ± 0.6 | 3.3 ± 1.1 | 0.001 * | ||
| 6 months | 0.8 ± 0.09 | 2.6 ± 0.8 | 0.001 * | ||
| p-value | 0.001 * | 0.001 * | |||
| 2 | MRI T2 axial section—% (Percentage of injury) | Baseline | 58.2 ± 2.5 | 57.9 ± 2.7 | 0.656 |
| 4 weeks | 23.5 ± 1.8 | 40.3 ± 2.1 | 0.001 * | ||
| 8 weeks | 13.5 ± 0.8 | 29.3 ± 1.9 | 0.001 * | ||
| 6 months | 3.2 ± 0.1 | 18.5 ± 0.9 | 0.001 * | ||
| p-value | 0.001 * | 0.001 * | |||
| 3 | MRI T2 coronal section—%(Percentage of injury) | Baseline | 62.8 ± 3.8 | 61.9 ± 3.9 | 0.369 |
| 4 weeks | 29.5 ± 2.1 | 46.3 ± 2.9 | 0.001 * | ||
| 8 weeks | 15.2 ± 1.1 | 32.0 ± 2.3 | 0.001 * | ||
| 6 months | 5.2 ± 0.1 | 21.2 ± 2.1 | 0.001 * | ||
| p-value | 0.001 * | 0.001 * | |||
| 4 | Ultrasound image—%(Percentage of injury) | Baseline | 59.2 ± 4.2 | 61.1 ± 4.1 | 0.081 |
| 4 weeks | 28.5 ± 2.8 | 43.3 ± 2.7 | 0.001 * | ||
| 8 weeks | 13.2 ± 1.4 | 28.9 ± 2.1 | 0.001 * | ||
| 6 months | 3.5 ± 0.1 | 16.6 ± 1.5 | 0.001 * | ||
| p-value | 0.001 * | 0.001 * | |||
| 5 | Functional disability PRTEE (0–100) | Baseline | 75.2 ± 4.9 | 74.5 ± 4.5 | 0.566 |
| 4 weeks | 43.5 ± 3.4 | 59.3 ± 3.7 | 0.001 * | ||
| 8 weeks | 28.7 ± 1.5 | 47.4 ± 2.5 | 0.001 * | ||
| 6 months | 9.2 ± 0.7 | 27.3 ± 1.4 | 0.001 * | ||
| p-value | 0.001 * | 0.001 * | |||
| 6 | Handgrip strengthHand dynamometer (kg) | Baseline | 29.6± 2.4 | 29.1± 2.4 | 0.423 |
| 4 weeks | 31.4± 2.5 | 29.8± 2.5 | 0.016 * | ||
| 8 weeks | 33.9± 2.6 | 31.5± 2.5 | 0.001 * | ||
| 6 months | 38.3± 2.7 | 32.3± 2.6 | 0.001 * | ||
| p-value | 0.001 * | 0.001 * |
| Sr. No | Variable | Duration | Active | Placebo | p-Value |
|---|---|---|---|---|---|
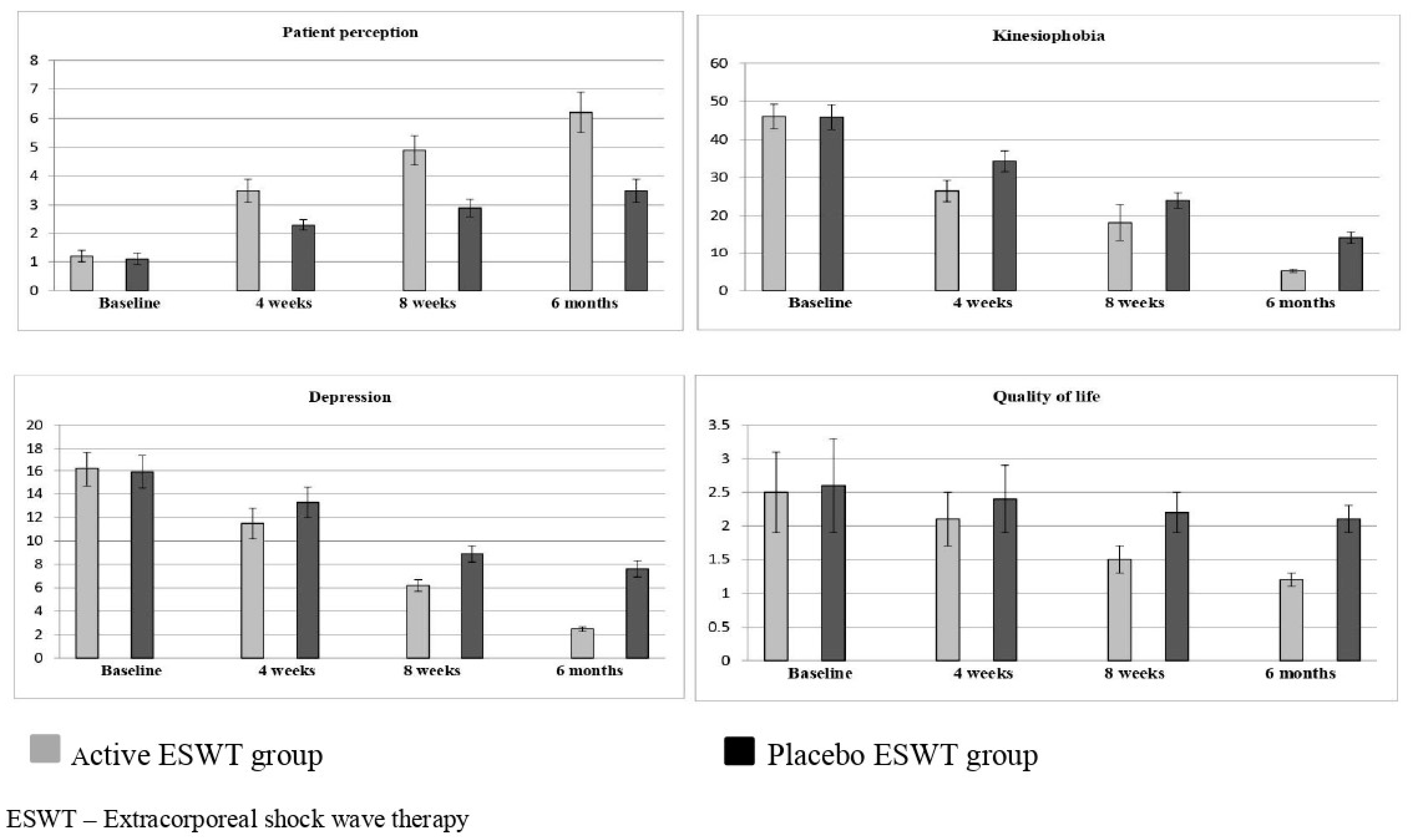
| 1 | Patient perception (GPI questionnaire) | Baseline | 1.2 ± 0.2 | 1.1 ± 0.2 | 0.057 |
| 4 weeks | 3.5 ± 0.4 | 2.3 ± 0.2 | 0.001 * | ||
| 8 weeks | 4.9 ± 0.5 | 2.9 ± 0.3 | 0.001 * | ||
| 6 months | 6.2 ± 0.7 | 3.5 ± 0.4 | 0.001 * | ||
| p-value | 0.001 * | 0.001 * | |||
| 2 | Kinesiophobia (TSK-AV) | Baseline | 46.1 ± 3.2 | 45.9 ± 3.3 | 0.812 |
| 4 weeks | 26.5 ± 2.8 | 34.3 ± 2.7 | 0.001 * | ||
| 8 weeks | 18.2 ± 4.7 | 24.0 ± 2.0 | 0.001 * | ||
| 6 months | 5.2 ± 0.5 | 14.2 ± 1.5 | 0.001 * | ||
| p-value | 0.001 * | 0.001 * | |||
| 3 | Depression (HADS) | Baseline | 16.2 ± 1.5 | 15.9 ± 1.4 | 0.426 |
| 4 weeks | 11.5 ± 1.3 | 13.3 ± 1.3 | 0.001 * | ||
| 8 weeks | 6.2 ± 0.5 | 8.9 ± 0.7 | 0.001 * | ||
| 6 months | 2.5 ± 0.2 | 7.6 ± 0.7 | 0.001 * | ||
| p-value | 0.001 * | 0.001 * | |||
| 4 | Quality of life (EuroQol EQ-5D) | Baseline | 2.5 ± 0.6 | 2.6 ± 0.7 | 0.554 |
| 4 weeks | 2.1 ± 0.4 | 2.4 ± 0.5 | 0.001 * | ||
| 8 weeks | 1.5 ± 0.2 | 2.2 ± 0.3 | 0.001 * | ||
| 6 months | 1.2 ± 0.1 | 2.1 ± 0.2 | 0.001 * | ||
| p-value | 0.001 * | 0.001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nambi, G.; Alghadier, M.; Ebrahim, E.E.; Verma, A.; Aldhafian, O.R.; Mohamed, S.H.P.; Alshewaier, S.A.; Sirajudeen, M.S.; Muthusamy, H.; Unnikrishnan, R. MRI and Ultrasound Analysis of Corticosteroid Injection Combined with Extracorporeal Shockwave Therapy in Lateral Epicondylitis—A Prospective, Randomized, Double-Blinded, Placebo-Controlled Trial. J. Pers. Med. 2022, 12, 1892. https://doi.org/10.3390/jpm12111892
Nambi G, Alghadier M, Ebrahim EE, Verma A, Aldhafian OR, Mohamed SHP, Alshewaier SA, Sirajudeen MS, Muthusamy H, Unnikrishnan R. MRI and Ultrasound Analysis of Corticosteroid Injection Combined with Extracorporeal Shockwave Therapy in Lateral Epicondylitis—A Prospective, Randomized, Double-Blinded, Placebo-Controlled Trial. Journal of Personalized Medicine. 2022; 12(11):1892. https://doi.org/10.3390/jpm12111892
Chicago/Turabian StyleNambi, Gopal, Mshari Alghadier, Elturabi Elsayed Ebrahim, Anju Verma, Osama R. Aldhafian, Shahul Hameed Pakkir Mohamed, Shady Abdullah Alshewaier, Mohamed Sherif Sirajudeen, Hariraja Muthusamy, and Radhakrishnan Unnikrishnan. 2022. "MRI and Ultrasound Analysis of Corticosteroid Injection Combined with Extracorporeal Shockwave Therapy in Lateral Epicondylitis—A Prospective, Randomized, Double-Blinded, Placebo-Controlled Trial" Journal of Personalized Medicine 12, no. 11: 1892. https://doi.org/10.3390/jpm12111892
APA StyleNambi, G., Alghadier, M., Ebrahim, E. E., Verma, A., Aldhafian, O. R., Mohamed, S. H. P., Alshewaier, S. A., Sirajudeen, M. S., Muthusamy, H., & Unnikrishnan, R. (2022). MRI and Ultrasound Analysis of Corticosteroid Injection Combined with Extracorporeal Shockwave Therapy in Lateral Epicondylitis—A Prospective, Randomized, Double-Blinded, Placebo-Controlled Trial. Journal of Personalized Medicine, 12(11), 1892. https://doi.org/10.3390/jpm12111892