
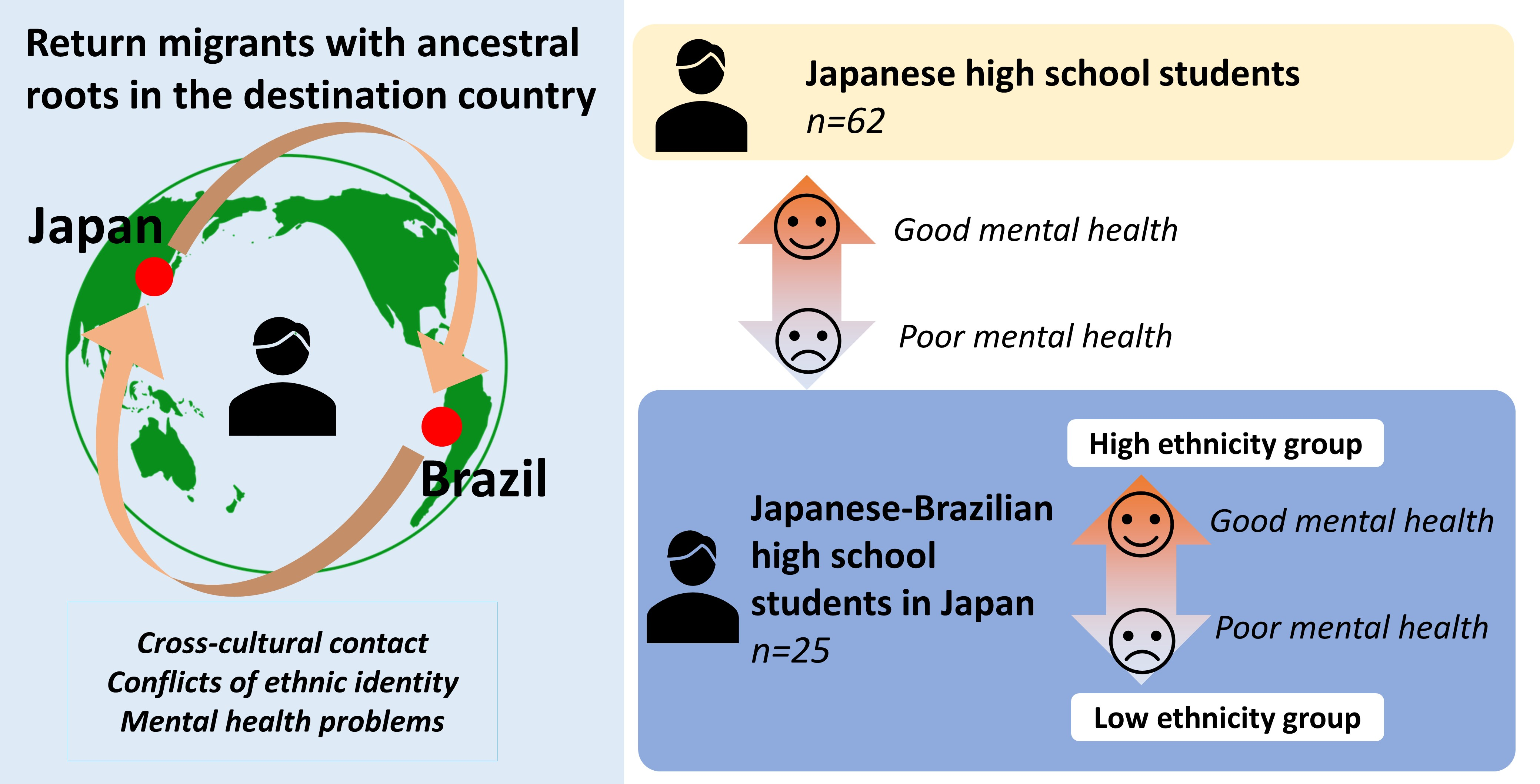
The Mental Health of Young Return Migrants with Ancestral Roots in Their Destination Country: A Cross-Sectional Study Focusing on the Ethnic Identities of Japanese–Brazilian High School Students Living in Japan

 ,
, 
Abstract
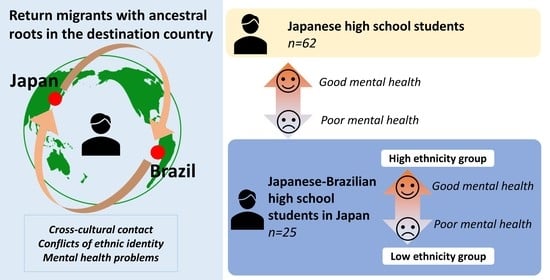
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Measures
2.3. Data Analysis
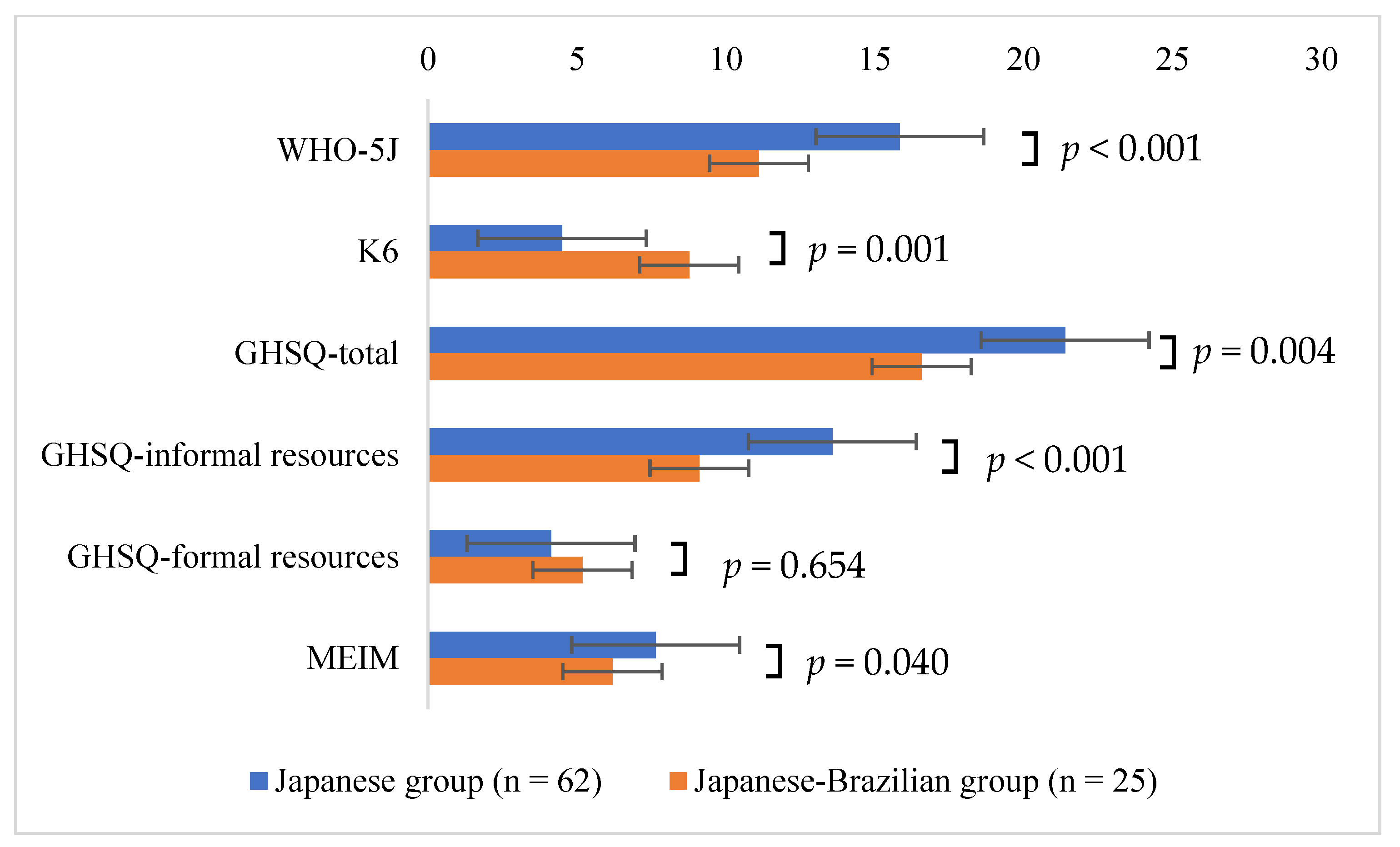
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Immigration Services Agency of Japan. Available online: https://www.moj.go.jp/isa/publications/press/13_00017.html (accessed on 3 August 2022).
- Immigration Services Agency of Japan. Available online: https://www.moj.go.jp/isa/policies/statistics/toukei_ichiran_touroku.html (accessed on 3 August 2022).
- Berry, J.W. Immigration, Acculturation, and Adaptation. Appl. Psychol. 1997, 46, 5–34. [Google Scholar] [CrossRef]
- Voglino, G.; Gualano, M.R.; Lo Moro, G.; Forghieri, P.; Caprioli, M.; Elhadidy, H.; Bert, F.; Siliquini, R. Mental health and discrimination among migrants from Africa: An Italian cross-sectional study. J. Community Psychol. 2022, 50, 601–619. [Google Scholar] [CrossRef] [PubMed]
- Morgan, C.; Knowles, G.; Hutchinson, G. Migration, ethnicity and psychoses: Evidence, models and future directions. World Psychiatry 2019, 3, 247–258. [Google Scholar] [CrossRef]
- Miller, R.; Tomita, Y.; Ong, K.I.C.; Shibanuma, A.; Jimba, M. Mental well-being of international migrants to Japan: A systematic review. BMJ Open 2019, 9, e029988. [Google Scholar] [CrossRef] [PubMed]
- Aldridge, R.W.; Nellums, L.B.; Bartlett, S.; Barr, A.L.; Patel, P.; Burns, R.; Hargreaves, S.; Miranda, J.J.; Tollman, S.; Friedland, J.S.; et al. Global patterns of mortality in international migrants: A systematic review and meta-analysis. Lancet 2018, 392, 2553–2566. [Google Scholar] [CrossRef]
- Troya, M.I.; Spittal, M.J.; Pendrous, R.; Crowley, G.; Gorton, H.C.; Russell, K.; Byrne, S.; Musgrove, R.; Hannah-Swain, S.; Kapur, N.; et al. Suicide rates amongst individuals from ethnic minority backgrounds: A systematic review and meta-analysis. EClinicalMedicine 2022, 47, 101399. [Google Scholar] [CrossRef]
- Zhang, K.; Xu, C.; Zhang, Y.; Wang, R.; Yu, X.; Hu, T.; Chen, Y.; Wang, Z.; Cao, B.; Chen, H.; et al. The Mental Health and Syndemic Effect on Suicidal Ideation among Migrant Workers in China: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 11363. [Google Scholar] [CrossRef]
- Fellmeth, G.; Rose-Clarke, K.; Zhao, C.; Busert, L.K.; Zheng, Y.; Massazza, A.; Sonmez, H.; Eder, B.; Blewitt, A.; Lertgrai, W.; et al. Health impacts of parental migration on left-behind children and adolescents: A systematic review and meta-analysis. Lancet 2018, 392, 2567–2582. [Google Scholar] [CrossRef]
- Derr, A.S. Mental Health Service Use Among Immigrants in the United States: A Systematic Review. Psychiatr. Serv. 2016, 67, 265–274. [Google Scholar] [CrossRef]
- Zhu, J.; Ye, Z.; Fang, Q.; Huang, L.; Zheng, X. Surveillance of Parenting Outcomes, Mental Health and Social Support for Primiparous Women among the Rural-to-Urban Floating Population. Healthcare 2021, 9, 1516. [Google Scholar] [CrossRef]
- Takubo, Y.; Nemoto, T.; Iwai, M.; Kashima, M.; Yamaguchi, E.; Maruyama, A.; Miura, S.; Saito, H.; Tsujino, N.; Mizuno, M. Demographic and clinical characteristics of foreign nationals accessing psychiatric services in Japan: A multicentre study in a metropolitan area. BMC Psychiatry 2020, 20, 569. [Google Scholar] [CrossRef] [PubMed]
- Uchino, T.; Kotsuji, Y.; Kitano, T.; Shiozawa, T.; Iida, S.; Aoki, A.; Iwai, M.; Shirahata, M.; Seki, A.; Mizuno, M.; et al. An integrated youth mental health service in a densely populated metropolitan area in Japan: Clinical case management bridges the gap between mental health and illness services. Early Interv. Psychiatry 2022, 16, 568–575. [Google Scholar] [CrossRef] [PubMed]
- Ojio, Y.; Mori, R.; Matsumoto, K.; Nemoto, T.; Sumiyoshi, T.; Fujita, H.; Morimoto, T.; Nishizono-Maher, A.; Fuji, C.; Mizuno, M. Innovative approach to adolescent mental health in Japan: School-based education about mental health literacy. Early Interv. Psychiatry 2021, 15, 174–182. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Angermeyer, M.; Anthony, J.C.; DEGraaf, R.; Demyttenaere, K.; Gasquet, I.; DEGirolamo, G.; Gluzman, S.; Gureje, O.; Haro, J.M.; et al. Lifetime prevalence and age-of-onset distributions of mental disorders in the World Health Organization’s World Mental Health Survey Initiative. World Psychiatry 2007, 3, 168–176. [Google Scholar]
- Solmi, M.; Radua, J.; Olivola, M.; Croce, E.; Soardo, L.; Salazar de Pablo, G.; Il Shin, J.; Kirkbride, J.B.; Jones, P.; Kim, J.H.; et al. Age at onset of mental disorders worldwide: Large-scale meta-analysis of 192 epidemiological studies. Mol. Psychiatry 2022, 1, 281–295. [Google Scholar] [CrossRef] [PubMed]
- Hou, W.K.; Liu, H.; Liang, L.; Ho, J.; Kim, H.; Seong, E.; Bonanno, G.A.; Hobfoll, S.E.; Hall, B.J. Everyday life experiences and mental health among conflict-affected forced migrants: A meta-analysis. J. Affect. Disord. 2020, 264, 50–68. [Google Scholar] [CrossRef]
- Lugo-Candelas, C.; Polanco-Roman, L.; Duarte, C.S. Intergenerational Effects of Racism: Can Psychiatry and Psychology Make a Difference for Future Generations? JAMA Psychiatry 2021, 78, 1065–1066. [Google Scholar] [CrossRef]
- Bhugra, D.; Becker, M.A. Migration, cultural bereavement and cultural identity. World Psychiatry 2005, 4, 18–24. [Google Scholar]
- Noda, F. Migration and Mental Disorder. J. Jpn. Soc. Soc. Psychiatry 1995, 4, 53–57. (In Japanese) [Google Scholar]
- Fortuna, L.R.; Álvarez, K.; Ramos Ortiz, Z.; Wang, Y.; Mozo Alegría, X.; Cook, B.L.; Alegría, M. Mental health, migration stressors and suicidal ideation among Latino immigrants in Spain and the United States. Eur. Psychiatry 2016, 36, 15–22. [Google Scholar] [CrossRef]
- Udry, J.R.; Li, R.M.; Hendrickson-Smith, J. Health and behavior risks of adolescents with mixed-race identity. Am. J. Public Health 2003, 93, 1865–1870. [Google Scholar] [CrossRef] [PubMed]
- Uematsu, A. The Role of Ethnic Identity in a Cross-Cultural Environment: The Relationship between Group Identity and Ego Identity. Jpn. J. Personal. 2010, 19, 25–37. (In Japanese) [Google Scholar] [CrossRef][Green Version]
- Kessler, R.C.; Andrews, G.; Colpe, L.J.; Hiripi, E.; Mroczek, D.K.; Normand, S.L.; Walters, E.E.; Zaslavsky, A.M. Short screening scales to monitor population prevalences and trends in non-specific psychological distress. Psychol. Med. 2002, 32, 959–976. [Google Scholar] [CrossRef]
- Psychiatric Research Unit, Mental Health Centre North Zealand. WHO-Five Well-being Index (who-5). Available online: https://www.who.int/ (accessed on 3 August 2022).
- Wilson, C.; Deane, F.; Ciarrochi, J.; Rickwood, D. Measuring help-seeking intentions: Properties of the General Help-Seeking Questionnaire. Can. J. Couns. 2005, 39, 15–28. [Google Scholar]
- Phinney, J.S. The multigroup ethnic identity measure: A new scale for use with adolescents and adults from diverse groups. J. Adolesc. Res. 1992, 7, 156–176. [Google Scholar] [CrossRef]
- Abe, Y. Recent Trends in Foreign Mental Disorders. Jpn. J. Clin. Psychiatry 1999, 28, 483–490. (In Japanese) [Google Scholar]
- Otsuka, K.; Miyasaka, L.; Tsuji, K.; Honda, G.; Yamaga, K.; Kato, S.; Nakamura, Y.; Abe, Y. Cultural adaptation and mental health among Brazilians of Japanese descent living in Japan. Jpn. Bull Soc. Psychiat 2001, 10, 149–158. [Google Scholar]
- Mental Health and Early Intervention in the Community-Based Integrated Care System (MEICIS). Available online: https://meicis.jp/en/home-en/ (accessed on 10 August 2022).
- Nemoto, T. Changes of treatments for schizophrenia: Community-based-psychiatry and early intervention. Jpn. J. Clin. Psychiatry 2020, 49, 195–202. (In Japanese) [Google Scholar]
- Otsuka, K.; Kato, S.; Tsuji, K. Ethnic Identity in manic depressive patients- Case studies in Japanese Brazilians in Japan. Jpn. J. Psychopathol. 2000, 21, 70–71. [Google Scholar]
- Eyou, M.L.; Adair, V.; Dixon, R. Cultural identity and psychological adjustment of adolescent Chinese immigrants in New Zealand. J. Adolesc. 2000, 23, 531–543. [Google Scholar] [CrossRef]
- Hong, J. Effects of Ethnic Identity on the Relationship Between Mental Health and Perceived Discrimination Among Ethnic Return Migrants: The Case of Korean Chinese Return-Migrated to South Korea. J. Immigr. Minor. Health 2019, 21, 522–532. [Google Scholar] [CrossRef] [PubMed]
- Inagaki, H.; Ito, K.; Sakuma, N.; Sugiyama, M.; Okamura, T.; Awata, S. Reliability and validity of the simplified Japanese version of the WHO-Five Well-being Index (S-WHO-5-J). Jpn. J. Public Health 2013, 60, 294–301. [Google Scholar]
- Furukawa, T.A.; Kawakami, N.; Saitoh, M.; Ono, Y.; Nakane, Y.; Nakamura, Y.; Tachimori, H.; Iwata, N.; Uda, H.; Nakane, H.; et al. The performance of the Japanese version of the K6 and K10 in the World Mental Health Survey Japan. Int. J. Methods Psychiatr. Res. 2008, 17, 152–158. [Google Scholar] [CrossRef] [PubMed]
- Supratiknya, A. Ethnic Identity: A Study of Construct Equivalence. J. Psikol. 2019, 46, 196. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Japanese (n = 62) | Japanese Brazilian (n = 25) | p-Value | ||
|---|---|---|---|---|
| Age | Mean (SD) | 16.6 (1.1) | 16.2 (1.2) | 0.108 |
| Gender | M/F; n (%) | 35 (56.5)/27 (43.5) | 9 (36.0)/16 (64.0) | 0.123 |
| Owning a car | Yes/No (%) | 62 (100)/0 (0) | 25 (100)/0 (0) | - |
| Nationality | ||||
| Japan | n (%) | 62 (100.0) | - | |
| Brazil | n (%) | - | 23 (92.0) | |
| Japan and Brazil | n (%) | - | 2 (8.0) | |
| Sense of belonging | Japanese/ Brazilian; n (%) | 62 (100)/0 | 3 (12.0)/22 (88.0) | <0.001 |
| High Ethnicity Group n = 12 | Low Ethnicity Group n = 13 | |||
|---|---|---|---|---|
| Mean (SD) | Mean (SD) | p-Value | Cohen’s d * | |
| WHO-5J total score | 13.25 (3.36) | 9.31 (5.11) | 0.034 | 0.91 |
| K6 total score | 6.42 (4.12) | 10.38 (5.38) | 0.051 | 0.83 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fukui, E.; Uchino, T.; Onozaka, M.; Kawashimo, T.; Iwai, M.; Takubo, Y.; Maruyama, A.; Miura, S.; Sekizaki, R.; Mizuno, M.; et al. The Mental Health of Young Return Migrants with Ancestral Roots in Their Destination Country: A Cross-Sectional Study Focusing on the Ethnic Identities of Japanese–Brazilian High School Students Living in Japan. J. Pers. Med. 2022, 12, 1858. https://doi.org/10.3390/jpm12111858
Fukui E, Uchino T, Onozaka M, Kawashimo T, Iwai M, Takubo Y, Maruyama A, Miura S, Sekizaki R, Mizuno M, et al. The Mental Health of Young Return Migrants with Ancestral Roots in Their Destination Country: A Cross-Sectional Study Focusing on the Ethnic Identities of Japanese–Brazilian High School Students Living in Japan. Journal of Personalized Medicine. 2022; 12(11):1858. https://doi.org/10.3390/jpm12111858
Chicago/Turabian StyleFukui, Eriko, Takashi Uchino, Masunari Onozaka, Takashi Kawashimo, Momoko Iwai, Youji Takubo, Akiko Maruyama, Sachio Miura, Ryo Sekizaki, Masafumi Mizuno, and et al. 2022. "The Mental Health of Young Return Migrants with Ancestral Roots in Their Destination Country: A Cross-Sectional Study Focusing on the Ethnic Identities of Japanese–Brazilian High School Students Living in Japan" Journal of Personalized Medicine 12, no. 11: 1858. https://doi.org/10.3390/jpm12111858
APA StyleFukui, E., Uchino, T., Onozaka, M., Kawashimo, T., Iwai, M., Takubo, Y., Maruyama, A., Miura, S., Sekizaki, R., Mizuno, M., Katagiri, N., Tsujino, N., & Nemoto, T. (2022). The Mental Health of Young Return Migrants with Ancestral Roots in Their Destination Country: A Cross-Sectional Study Focusing on the Ethnic Identities of Japanese–Brazilian High School Students Living in Japan. Journal of Personalized Medicine, 12(11), 1858. https://doi.org/10.3390/jpm12111858