
Temporomandibular Disorders as a Risk Factor for Suicidal Behavior: A Systematic Review

 ,
,  ,
,  ,
,  , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
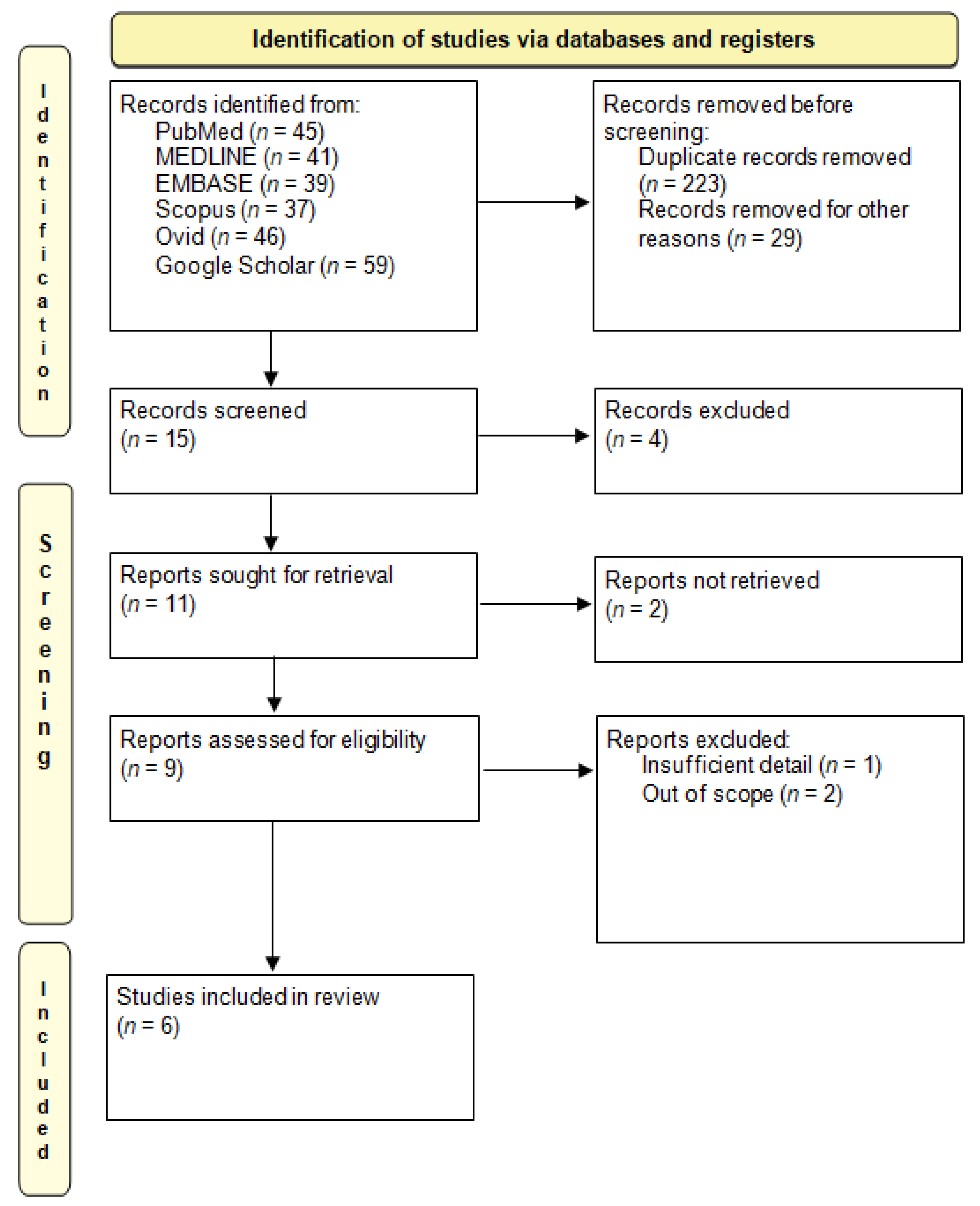
2.1. Search Strategy and Data Extraction
2.2. Protocol and Registration
2.3. Quality Assessment within and across Studies and Overall Quality Assessment
3. Results
3.1. Temporomandibular Disorders Assessment Tools
3.2. Suicidal Behavior Assessment
3.3. Summary of Findings on the Association of Temporomandibular Disorders and Suicidal Behavior
3.4. Methodological Quality Assessment within Studies and Overall Quality Assessment across Studies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferneini, E.M. Temporomandibular Joint Disorders (TMD). J. Oral Maxillofac. Surg. 2021, 79, 2171–2172. [Google Scholar] [CrossRef]
- Gauer, R.L.; Semidey, M.J. Diagnosis and treatment of temporomandibular disorders. Am. Fam. Physician 2015, 91, 378–386. [Google Scholar]
- Valesan, L.F.; Da-Cas, C.D.; Réus, J.C.; Denardin, A.C.S.; Garanhani, R.R.; Bonotto, D.; Januzzi, E.; de Souza, B.D.M. Prevalence of temporomandibular joint disorders: A systematic review and meta-analysis. Clin. Oral Investig. 2021, 25, 441–453. [Google Scholar] [CrossRef]
- Kafas, P.; Leeson, R. Assessment of pain in temporomandibular disorders: The bio-psychosocial complexity. Int. J. Oral Maxillofac. Surg. 2006, 35, 145–149. [Google Scholar] [CrossRef]
- Magalhães, B.G.; Freitas, J.L.M.; Barbosa, A.; Gueiros, M.; Gomes, S.G.F.; Rosenblatt, A.; Caldas Júnior, A.F. Temporomandibular disorder: Otologic implications and its relationship to sleep bruxism. Braz. J. Otorhinolaryngol. 2018, 84, 614–619. [Google Scholar] [CrossRef]
- Manfredini, D.; Segù, M.; Arveda, N.; Lombardo, L.; Siciliani, G.; Rossi, A.; Guarda-Nardini, L. Temporomandibular Joint Disorders in Patients With Different Facial Morphology. A Systematic Review of the Literature. J. Oral Maxillofac. Surg. 2016, 74, 29–46. [Google Scholar] [CrossRef] [PubMed]
- Crincoli, V.; Cannavale, M.; Cazzolla, A.P.; Dioguardi, M.; Piancino, M.G.; Di Comite, M. Temporomandibular Disorders and Oral Features in Idiopathic Inflammatory Myopathies (IIMs) Patients: An Observational Study. Int. J. Med. Sci. 2021, 18, 3158–3170. [Google Scholar] [CrossRef] [PubMed]
- Kmeid, E.; Nacouzi, M.; Hallit, S.; Rohayem, Z. Prevalence of temporomandibular joint disorder in the Lebanese population, and its association with depression, anxiety, and stress. Head Face Med. 2020, 16, 19. [Google Scholar] [CrossRef]
- Sójka, A.; Stelcer, B.; Roy, M.; Mojs, E.; Pryliński, M. Is there a relationship between psychological factors and TMD? Brain Behav. 2019, 9, e01360. [Google Scholar] [CrossRef] [PubMed]
- Al-Dajani, N.; Horwitz, A.G.; Czyz, E.K. Does coping reduce suicidal urges in everyday life? Evidence from a daily diary study of adolescent inpatients. Depress. Anxiety 2022, 39, 496–503. [Google Scholar] [CrossRef]
- Noyman-Veksler, G.; Lerman, S.F.; Joiner, T.E.; Brill, S.; Rudich, Z.; Shalev, H.; Shahar, G. Role of Pain-Based Catastrophizing in Pain, Disability, Distress, and Suicidal Ideation. Psychiatry 2017, 80, 155–170. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.Y.; Shin, J.S.; Lee, J.; Lee, Y.J.; Kim, M.R.; Ahn, Y.J.; Park, K.B.; Hwang, D.S.; Ha, I.H. Gender Difference in Associations between Chronic Temporomandibular Disorders and General Quality of Life in Koreans: A Cross-Sectional Study. PLoS ONE 2015, 10, e0145002. [Google Scholar] [CrossRef]
- Beghi, M.; Butera, E.; Cerri, C.G.; Cornaggia, C.M.; Febbo, F.; Mollica, A.; Berardino, G.; Piscitelli, D.; Resta, E.; Logroscino, G.; et al. Suicidal behaviour in older age: A systematic review of risk factors associated to suicide attempts and completed suicides. Neurosci. Biobehav. Rev. 2021, 127, 193–211. [Google Scholar] [CrossRef]
- Prasad, S.R.; Kumar, N.R.; Shruthi, H.R.; Kalavathi, S.D. Temporomandibular pain. J. Oral Maxillofac. Pathol. 2016, 20, 272–275. [Google Scholar] [CrossRef]
- Reissmann, D.R.; John, M.T.; Schierz, O.; Wassell, R.W. Functional and psychosocial impact related to specific temporomandibular disorder diagnoses. J. Dent. 2007, 35, 643–650. [Google Scholar] [CrossRef]
- Park, S.; Heo, H.A.; Yun, K.I.; Pyo, S.W. High prevalence of stress and suicidal ideation in women with temporomandibular disorder: A population-based cross-sectional survey. Cranio 2022, 40, 174–180. [Google Scholar] [CrossRef]
- Lin, S.L.; Wu, S.L.; Huang, H.T.; Lung, F.W.; Chi, T.C.; Yang, J.W. Can a 10-Minute Questionnaire Identify Significant Psychological Issues in Patients With Temporomandibular Joint Disease? J. Oral Maxillofac. Surg. 2017, 75, 1856–1865. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- National Institutes of Health (NIH). Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies; NIH Library: Bethesda, MD, USA, 2022. Available online: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools (accessed on 16 August 2022).
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J.; GRADE Working Group. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef]
- Han, D.H. The association between temporomandibular disorders and suicide ideation in a representative sample of the South Korean population. J. Oral Facial Pain Headache 2014, 28, 338–345. [Google Scholar] [CrossRef]
- Bertoli, E.; de Leeuw, R. Prevalence of Suicidal Ideation, Depression, and Anxiety in Chronic Temporomandibular Disorder Patients. J. Oral Facial Pain Headache 2016, 30, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Yeung, E.; Abou-Foul, A.; Matcham, F.; Poate, T.; Fan, K. Integration of mental health screening in the management of patients with temporomandibular disorders. Br. J. Oral Maxillofac. Surg. 2017, 55, 594–599. [Google Scholar] [CrossRef] [PubMed]
- Heo, H.A.; Park, S.; Pyo, S.W. Association of temporomandibular disorder and high frequency of suicide ideation in Korean adolescents: A cross-sectional survey. Acta Odontol. Scand. 2018, 76, 374–379. [Google Scholar] [CrossRef] [PubMed]
- Chin, Y.R.; Choi, K. Suicide Attempts and Associated Factors in Male and Female Korean Adolescents A Population-Based Cross-Sectional Survey. Community Ment. Health J. 2015, 51, 862–866. [Google Scholar] [CrossRef] [PubMed]
- de Heer, E.W.; Ten Have, M.; van Marwijk, H.W.J.; Dekker, J.; de Graaf, R.; Beekman, A.T.F.; van der Feltz-Cornelis, C.M. Pain as a risk factor for suicidal ideation. A population-based longitudinal cohort study. Gen. Hosp. Psychiatry 2020, 63, 54–61. [Google Scholar] [CrossRef]
- Fenton, B.T.; Goulet, J.L.; Bair, M.J.; Cowley, T.; Kerns, R.D. Relationships Between Temporomandibular Disorders, MSDConditions, and Mental Health Comorbidities: Findings from the Veterans Musculoskeletal Disorders Cohort. Pain Med. 2018, 19, S61–S68. [Google Scholar] [CrossRef]
- Ohrbach, R.; Fillingim, R.B.; Mulkey, F.; Gonzalez, Y.; Gordon, S.; Gremillion, H.; Lim, P.F.; Ribeiro-Dasilva, M.; Greenspan, J.D.; Knott, C.; et al. Clinical findings and pain symptoms as potential risk factors for chronic TMD: Descriptive data and empirically identified domains from the OPPERA case-control study. J. Pain 2011, 12 (Suppl. 11), T27–T45. [Google Scholar] [CrossRef]
- Zorina-Lichtenwalter, K.; Meloto, C.B.; Khoury, S.; Diatchenko, L. Genetic predictors of human chronic pain conditions. Neuroscience 2016, 338, 36–62. [Google Scholar] [CrossRef]
- Ibi, M. Inflammation and Temporomandibular Joint Derangement. Biol. Pharm. Bull. 2019, 42, 538–542. [Google Scholar] [CrossRef]
- Beurel, E.; Toups, M.; Nemeroff, C.B. The Bidirectional Relationship of Depression and Inflammation: Double Trouble. Neuron 2020, 107, 234–256. [Google Scholar] [CrossRef]
- Lozupone, M.; Donghia, R.; Sardone, R.; Mollica, A.; Berardino, G.; Lampignano, L.; Griseta, C.; Zupo, R.; Castellana, F.; Bortone, I.; et al. Apolipoprotein E genotype, inflammatory biomarkers, and non-psychiatric multimorbidity contribute to the suicidal ideation phenotype in older age. The Salus in Apulia Study. J. Affect Disord. 2022, 319, 202–212. [Google Scholar] [CrossRef] [PubMed]
- Suicide—WHO|World Health Organization. Available online: https://www.who.int/news-room/fact-sheets/detail/suicide (accessed on 20 September 2022).




{kind=link}
{kind=link}
{kind=link}
| Authors, Year (Reference) | TMDs Assessment Tool(s) | Outcome(s)’ Assessment | Design | n | Age | Setting(s) | Country | Quality Assessment | Main Findings |
|---|---|---|---|---|---|---|---|---|---|
| Han, 2014 [21] | World Health Organization (WHO) criteria | “In the last 12 months, did you think about committing suicide” | Cross-sectional | 16658 (42.3% M, 57.7% F) | >19 years old | Community | Asia (South Korea) | Moderate | Pain conditions, including TMD pain, may aggravate suicidal ideation among those with a cancer history |
| Kim et al., 2015 [12] | Self-reported (experience of TM pain persisting 3 months or longer during the year) | EuroQol-5 Dimension | Cross-sectional | 17198 (42.4% M, 57.6% F) | >19 years old | Community | Asia (South Korea) | Moderate | Chronic diseases and psychological factors are important in chronic TMD, and there may be physiological and pathological gender differences in TMD |
| Bertoli and de Leuwee, 2016 [22] | Research Diagnostic Criteria for TMD (RDC/TMD) | 3 items of the Symptom Checklist 90 (SCL-90R)
| Cross-sectional | 1241 (11.7% M, 88.3% F) | >18 years old; mean age 35.76 ± 12.6 | Community | North America (USA) | High | Elevated levels of suicidal ideation, depression and anxiety were reported in a chronic TMD population, especially in those with chronic muscle pain, compared to the general population |
| Yeung et al., 2017 [23] | Diagnostic Criteria for TMD (DC/TMD) | Item 9 of the Patient Health Questionnaire-9 (PHQ-9) | Cross-sectional | 162 (20% M, 80% F) | Median age 35 years old (27–47) | Community | Europe (United Kingdom) | High | Early identification of mental health problems and concurrent management may be most beneficial in subjects with TMD symptoms for up to two years |
| Heo et al., 2018 [24] | Interviews and oral examination | “Have you ever sincerely thought about committing suicide in the past year?” | Cross-sectional | 1337 (53.6% M; 46.4% F) | 12–18 years old | Community | Asia (South Korea) | Low | The results provide evidence that the depressed mood and suicidal ideation were associated with TMD in male adolescents |
| Park et al., 2022 [16] | World Health Organization (WHO) criteria | “Have you ever sincerely thought about committing suicide in the past year?” | Cross-sectional | 8049 (42.2% M, 57.8% F) | 19–59 years old | Community | Asia (South Korea) | Moderate | This study found that suicidal ideation is closely associated with TMD in women |
| Outcome | Number of Participants (Studies) Design | Study-Specific Results and Measurements | Certainty of Evidence (GRADE) |
|---|---|---|---|
| Suicidal behavior | 44,645 patients (six studies) [12,16,21,22,23,24] All cross-sectional | Total TMD vs. suicidal ideation: PR: 1.26, 95% CI: 1.15–1.37 (p < 0.001); Severe TMD vs. suicidal ideation: PR: 1.35, 95% CI: 1.19–1.54 (p < 0.001) [21] Chronic TMD vs. thoughts of suicide: ß = -0.028 (p < 0.0001) [12] Pain severity vs. SCL-90-R (item 15): ρ = 0.099 (p < 0.001); Pain severity vs. SCL-90-R (item 54): ρ = 0.137 (p < 0.001); Pain severity vs. SCL-90-R (item 59): ρ = 0.109 (p < 0.001) [22] TMD vs. Patient Health Questionnaire-9 (PHQ–9) = 3.6 (p = 0.033) [23] TMD (males) vs. suicidal ideation: OR: 2.56, 95% CI: 1.014–6.484 (p < 0.05) [24] TMD (women) vs. suicidal ideation: OR: 1.54, 95% CI: 1.157–2.051 (p < 0.05) [16] | ⊕⊕ Low a |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dibello, V.; Panza, F.; Mori, G.; Ballini, A.; Di Cosola, M.; Lozupone, M.; Dibello, A.; Santarcangelo, F.; Vertucci, V.; Dioguardi, M.; et al. Temporomandibular Disorders as a Risk Factor for Suicidal Behavior: A Systematic Review. J. Pers. Med. 2022, 12, 1782. https://doi.org/10.3390/jpm12111782
Dibello V, Panza F, Mori G, Ballini A, Di Cosola M, Lozupone M, Dibello A, Santarcangelo F, Vertucci V, Dioguardi M, et al. Temporomandibular Disorders as a Risk Factor for Suicidal Behavior: A Systematic Review. Journal of Personalized Medicine. 2022; 12(11):1782. https://doi.org/10.3390/jpm12111782
Chicago/Turabian StyleDibello, Vittorio, Francesco Panza, Giorgio Mori, Andrea Ballini, Michele Di Cosola, Madia Lozupone, Antonio Dibello, Filippo Santarcangelo, Vincenzo Vertucci, Mario Dioguardi, and et al. 2022. "Temporomandibular Disorders as a Risk Factor for Suicidal Behavior: A Systematic Review" Journal of Personalized Medicine 12, no. 11: 1782. https://doi.org/10.3390/jpm12111782
APA StyleDibello, V., Panza, F., Mori, G., Ballini, A., Di Cosola, M., Lozupone, M., Dibello, A., Santarcangelo, F., Vertucci, V., Dioguardi, M., & Cantore, S. (2022). Temporomandibular Disorders as a Risk Factor for Suicidal Behavior: A Systematic Review. Journal of Personalized Medicine, 12(11), 1782. https://doi.org/10.3390/jpm12111782