
Contemporary Management of Severely Calcified Coronary Lesions

Abstract
1. Introduction
2. Definition and Characterization of Coronary Calcification
3. Modalities for Coronary Calcium Modification
3.1. Balloon Angioplasty
3.1.1. Non-Compliant Balloons
3.1.2. High-Pressure Balloons
3.1.3. Cutting Balloons
3.1.4. Scoring Balloons
3.2. Intravascular Lithotripsy
3.3. Coronary Atherectomy
3.3.1. Rotational Atherectomy
3.3.2. Orbital Atherectomy
3.3.3. Laser Atherectomy
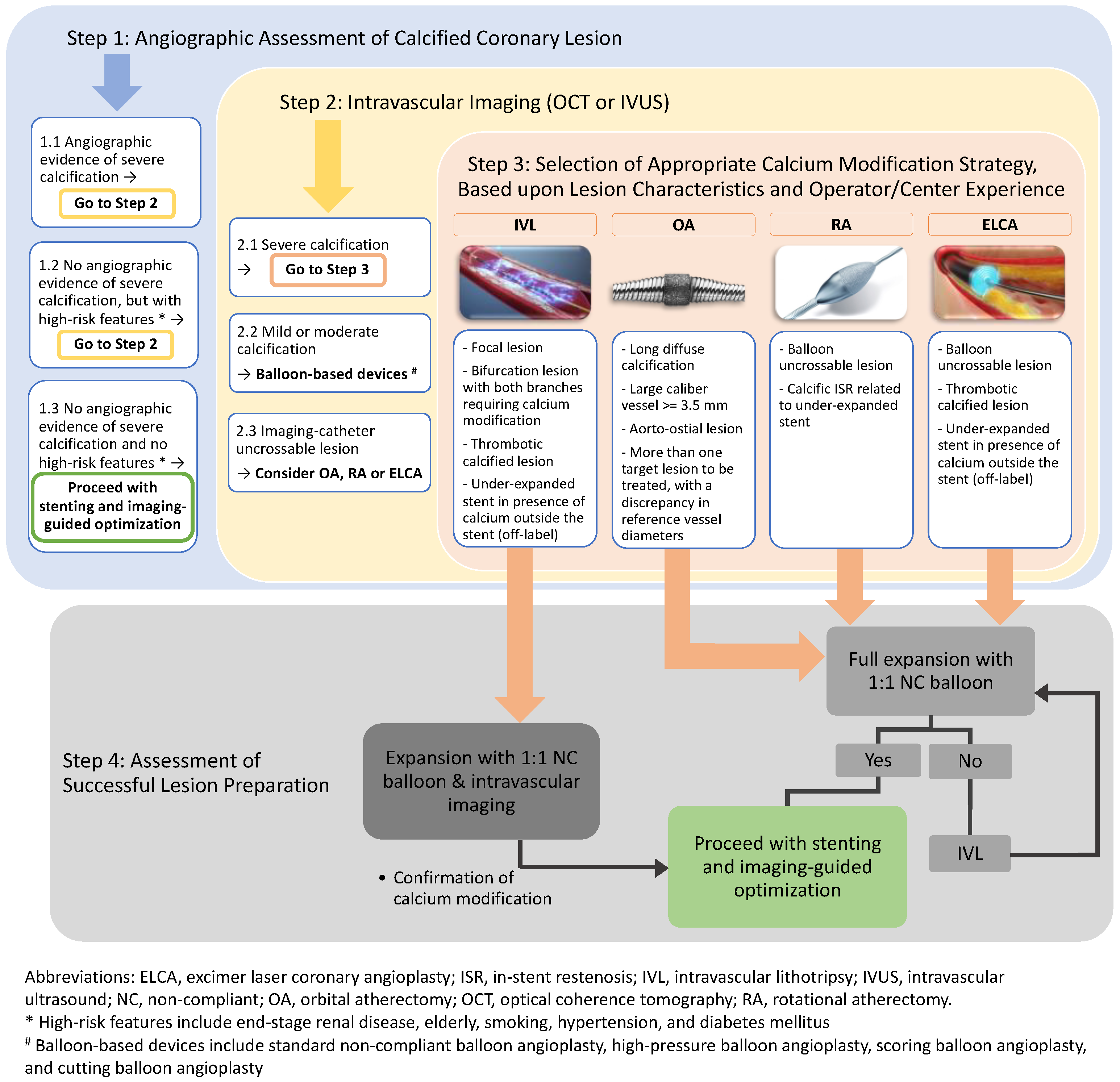
4. Management Algorithm for Calcified Coronary Lesions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bourantas, C.V.; Zhang, Y.J.; Garg, S.; Iqbal, J.; Valgimigli, M.; Windecker, S.; Mohr, F.W.; Silber, S.; Vries, T.; Onuma, Y.; et al. Prognostic implications of coronary calcification in patients with obstructive coronary artery disease treated by percutaneous coronary intervention: A patient-level pooled analysis of 7 contemporary stent trials. Heart 2014, 100, 1158–1164. [Google Scholar] [CrossRef] [PubMed]
- Copeland-Halperin, R.S.; Baber, U.; Aquino, M.; Rajamanickam, A.; Roy, S.; Hasan, C.; Barman, N.; Kovacic, J.C.; Moreno, P.; Krishnan, P.; et al. Prevalence, correlates, and impact of coronary calcification on adverse events following PCI with newer-generation DES: Findings from a large multiethnic registry. Catheter. Cardiovasc. Interv. 2018, 91, 859–866. [Google Scholar] [CrossRef] [PubMed]
- Huisman, J.; van der Heijden, L.C.; Kok, M.M.; Louwerenburg, J.H.; Danse, P.W.; Jessurun, G.A.; de Man, F.H.; Lowik, M.M.; Linssen, G.C.; IJzerman, M.J.; et al. Two-year outcome after treatment of severely calcified lesions with newer-generation drug-eluting stents in acute coronary syndromes: A patient-level pooled analysis from TWENTE and DUTCH PEERS. J. Cardiol. 2017, 69, 660–665. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.S.; Shah, N. The Impact and Pathophysiologic Consequences of Coronary Artery Calcium Deposition in Percutaneous Coronary Interventions. J. Invasive Cardiol. 2016, 28, 160–167. [Google Scholar]
- Madhavan, M.V.; Tarigopula, M.; Mintz, G.S.; Maehara, A.; Stone, G.W.; Genereux, P. Coronary artery calcification: Pathogenesis and prognostic implications. J. Am. Coll. Cardiol. 2014, 63, 1703–1714. [Google Scholar] [CrossRef]
- Tan, K.; Sulke, N.; Taub, N.; Sowton, E. Clinical and lesion morphologic determinants of coronary angioplasty success and complications: Current experience. J. Am. Coll. Cardiol. 1995, 25, 855–865. [Google Scholar] [CrossRef]
- Riley, R.F.; Henry, T.D.; Mahmud, E.; Kirtane, A.J.; Brilakis, E.S.; Goyal, A.; Grines, C.L.; Lombardi, W.L.; Maran, A.; Rab, T.; et al. SCAI position statement on optimal percutaneous coronary interventional therapy for complex coronary artery disease. Catheter. Cardiovasc. Interv. 2020, 96, 346–362. [Google Scholar] [CrossRef]
- Lawton, J.S.; Tamis-Holland, J.E.; Bangalore, S.; Bates, E.R.; Beckie, T.M.; Bischoff, J.M.; Bittl, J.A.; Cohen, M.G.; DiMaio, J.M.; Don, C.W.; et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e18–e114. [Google Scholar]
- Bulluck, H.; McEntegart, M. Contemporary tools and devices for coronary calcium modification. JRSM Cardiovasc. Dis. 2022, 11, 20480040221089760. [Google Scholar] [CrossRef]
- Mauri, L.; Bonan, R.; Weiner, B.H.; Legrand, V.; Bassand, J.P.; Popma, J.J.; Niemyski, P.; Prpic, R.; Ho, K.K.; Chauhan, M.S.; et al. Cutting balloon angioplasty for the prevention of restenosis: Results of the Cutting Balloon Global Randomized Trial. Am. J. Cardiol. 2002, 90, 1079–1083. [Google Scholar] [CrossRef]
- Albiero, R.; Silber, S.; Di Mario, C.; Cernigliaro, C.; Battaglia, S.; Reimers, B.; Frasheri, A.; Klauss, V.; Auge, J.M.; Rubartelli, P.; et al. Cutting balloon versus conventional balloon angioplasty for the treatment of in-stent restenosis: Results of the restenosis cutting balloon evaluation trial (RESCUT). J. Am. Coll. Cardiol. 2004, 43, 943–949. [Google Scholar] [CrossRef] [PubMed]
- Tang, Z.; Bai, J.; Su, S.P.; Wang, Y.; Liu, M.H.; Bai, Q.C.; Tian, J.W.; Xue, Q.; Gao, L.; An, C.X.; et al. Cutting-balloon angioplasty before drug-eluting stent implantation for the treatment of severely calcified coronary lesions. J. Geriatr. Cardiol. 2014, 11, 44–49. [Google Scholar] [PubMed]
- Okura, H.; Hayase, M.; Shimodozono, S.; Kobayashi, T.; Sano, K.; Matsushita, T.; Kondo, T.; Kijima, M.; Nishikawa, H.; Kurogane, H.; et al. Mechanisms of acute lumen gain following cutting balloon angioplasty in calcified and noncalcified lesions: An intravascular ultrasound study. Catheter. Cardiovasc. Interv. 2002, 57, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Jujo, K.; Saito, K.; Ishida, I.; Kim, A.; Suzuki, Y.; Furuki, Y.; Ouchi, T.; Ishii, Y.; Sekiguchi, H.; Yamaguchi, J.; et al. Intimal disruption affects drug-eluting cobalt-chromium stent expansion: A randomized trial comparing scoring and conventional balloon predilation. Int. J. Cardiol. 2016, 221, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Sadamatsu, K.; Yoshida, K.; Yoshidomi, Y.; Koga, Y.; Amari, K.; Tokunou, T. Comparison of pre-dilation with a non-compliant balloon versus a dual wire scoring balloon for coronary stenting. World J. Cardiovasc. Dis. 2013, 3, 395–400. [Google Scholar] [CrossRef]
- Reifart, N.; Vandormael, M.; Krajcar, M.; Gohring, S.; Preusler, W.; Schwarz, F.; Storger, H.; Hofmann, M.; Klopper, J.; Muller, S.; et al. Randomized comparison of angioplasty of complex coronary lesions at a single center. Excimer Laser, Rotational Atherectomy, and Balloon Angioplasty Comparison (ERBAC) Study. Circulation 1997, 96, 91–98. [Google Scholar] [CrossRef]
- Dill, T.; Dietz, U.; Hamm, C.W.; Kuchler, R.; Rupprecht, H.J.; Haude, M.; Cyran, J.; Ozbek, C.; Kuck, K.H.; Berger, J.; et al. A randomized comparison of balloon angioplasty versus rotational atherectomy in complex coronary lesions (COBRA study). Eur. Heart J. 2000, 21, 1759–1766. [Google Scholar] [CrossRef]
- Mauri, L.; Reisman, M.; Buchbinder, M.; Popma, J.J.; Sharma, S.K.; Cutlip, D.E.; Ho, K.K.; Prpic, R.; Zimetbaum, P.J.; Kuntz, R.E.; et al. Comparison of rotational atherectomy with conventional balloon angioplasty in the prevention of restenosis of small coronary arteries: Results of the Dilatation vs Ablation Revascularization Trial Targeting Restenosis (DART). Am. Heart J. 2003, 145, 847–854. [Google Scholar] [CrossRef]
- Whitlow, P.L.; Bass, T.A.; Kipperman, R.M.; Sharaf, B.L.; Ho, K.K.; Cutlip, D.E.; Zhang, Y.; Kuntz, R.E.; Williams, D.O.; Lasorda, D.M.; et al. Results of the study to determine rotablator and transluminal angioplasty strategy (STRATAS). Am. J. Cardiol. 2001, 87, 699–705. [Google Scholar] [CrossRef]
- Safian, R.D.; Feldman, T.; Muller, D.W.; Mason, D.; Schreiber, T.; Haik, B.; Mooney, M.; O’Neill, W.W. Coronary angioplasty and Rotablator atherectomy trial (CARAT): Immediate and late results of a prospective multicenter randomized trial. Catheter. Cardiovasc. Interv. 2001, 53, 213–220. [Google Scholar] [CrossRef]
- Sharma, S.K.; Kini, A.; Mehran, R.; Lansky, A.; Kobayashi, Y.; Marmur, J.D. Randomized trial of Rotational Atherectomy Versus Balloon Angioplasty for Diffuse In-stent Restenosis (ROSTER). Am. Heart J. 2004, 147, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Vom Dahl, J.; Dietz, U.; Haager, P.K.; Silber, S.; Niccoli, L.; Buettner, H.J.; Schiele, F.; Thomas, M.; Commeau, P.; Ramsdale, D.R.; et al. Rotational atherectomy does not reduce recurrent in-stent restenosis: Results of the angioplasty versus rotational atherectomy for treatment of diffuse in-stent restenosis trial (ARTIST). Circulation 2002, 105, 583–588. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Wahab, M.; Richardt, G.; Joachim Büttner, H.; Toelg, R.; Geist, V.; Meinertz, T.; Schofer, J.; King, L.; Neumann, F.J.; Khattab, A.A. High-speed rotational atherectomy before paclitaxel-eluting stent implantation in complex calcified coronary lesions: The randomized ROTAXUS (Rotational Atherectomy Prior to Taxus Stent Treatment for Complex Native Coronary Artery Disease) trial. JACC Cardiovasc. Interv. 2013, 6, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Wahab, M.; Toelg, R.; Byrne, R.A.; Geist, V.; El-Mawardy, M.; Allali, A.; Rheude, T.; Robinson, D.R.; Abdelghani, M.; Sulimov, D.S.; et al. High-Speed Rotational Atherectomy Versus Modified Balloons Prior to Drug-Eluting Stent Implantation in Severely Calcified Coronary Lesions. Circ. Cardiovasc. Interv. 2018, 11, e007415. [Google Scholar] [CrossRef]
- Parikh, K.; Chandra, P.; Choksi, N.; Khanna, P.; Chambers, J. Safety and feasibility of orbital atherectomy for the treatment of calcified coronary lesions: The ORBIT I trial. Catheter. Cardiovasc. Interv. 2013, 81, 1134–1139. [Google Scholar] [CrossRef] [PubMed]
- Chambers, J.W.; Feldman, R.L.; Himmelstein, S.I.; Bhatheja, R.; Villa, A.E.; Strickman, N.E.; Shlofmitz, R.A.; Dulas, D.D.; Arab, D.; Khanna, P.K.; et al. Pivotal trial to evaluate the safety and efficacy of the orbital atherectomy system in treating de novo, severely calcified coronary lesions (ORBIT II). JACC Cardiovasc. Interv. 2014, 7, 510–518. [Google Scholar] [CrossRef]
- Stone, G.W.; de Marchena, E.; Dageforde, D.; Foschi, A.; Muhlestein, J.B.; McIvor, M.; Rizik, D.; Vanderlaan, R.; McDonnell, J. Prospective, randomized, multicenter comparison of laser-facilitated balloon angioplasty versus stand-alone balloon angioplasty in patients with obstructive coronary artery disease. The Laser Angioplasty Versus Angioplasty (LAVA) Trial Investigators. J. Am. Coll. Cardiol. 1997, 30, 1714–1721. [Google Scholar] [CrossRef]
- Appelman, Y.E.; Piek, J.J.; Strikwerda, S.; Tijssen, J.G.; de Feyter, P.J.; David, G.K.; Serruys, P.W.; Margolis, J.R.; Koelemay, M.J.; Montauban van Swijndregt, E.W.; et al. Randomised trial of excimer laser angioplasty versus balloon angioplasty for treatment of obstructive coronary artery disease. Lancet 1996, 347, 79–84. [Google Scholar] [CrossRef]
- Brinton, T.J.; Ali, Z.A.; Hill, J.M.; Meredith, I.T.; Maehara, A.; Illindala, U.; Lansky, A.; Gotberg, M.; Van Mieghem, N.M.; Whitbourn, R.; et al. Feasibility of Shockwave Coronary Intravascular Lithotripsy for the Treatment of Calcified Coronary Stenoses. Circulation 2019, 139, 834–836. [Google Scholar] [CrossRef]
- Ali, Z.A.; Nef, H.; Escaned, J.; Werner, N.; Banning, A.P.; Hill, J.M.; De Bruyne, B.; Montorfano, M.; Lefevre, T.; Stone, G.W.; et al. Safety and Effectiveness of Coronary Intravascular Lithotripsy for Treatment of Severely Calcified Coronary Stenoses: The Disrupt CAD II Study. Circ. Cardiovasc. Interv. 2019, 12, e008434. [Google Scholar] [CrossRef]
- Hill, J.M.; Kereiakes, D.J.; Shlofmitz, R.A.; Klein, A.J.; Riley, R.F.; Price, M.J.; Herrmann, H.C.; Bachinsky, W.; Waksman, R.; Stone, G.W.; et al. Intravascular Lithotripsy for Treatment of Severely Calcified Coronary Artery Disease. J. Am. Coll. Cardiol. 2020, 76, 2635–2646. [Google Scholar] [CrossRef] [PubMed]
- Saito, S.; Yamazaki, S.; Takahashi, A.; Namiki, A.; Kawasaki, T.; Otsuji, S.; Nakamura, S.; Shibata, Y.; Disrupt CAD IV Investigators. Intravascular Lithotripsy for Vessel Preparation in Severely Calcified Coronary Arteries Prior to Stent Placement- Primary Outcomes From the Japanese Disrupt CAD IV Study. Circ. J. 2021, 85, 826–833. [Google Scholar] [CrossRef] [PubMed]
- Maehara, A.; Matsumura, M.; Ali, Z.A.; Mintz, G.S.; Stone, G.W. IVUS-Guided Versus OCT-Guided Coronary Stent Implantation: A Critical Appraisal. JACC Cardiovasc. Imaging 2017, 10, 1487–1503. [Google Scholar] [CrossRef] [PubMed]
- Fujino, A.; Mintz, G.S.; Matsumura, M.; Lee, T.; Kim, S.Y.; Hoshino, M.; Usui, E.; Yonetsu, T.; Haag, E.S.; Shlofmitz, R.A.; et al. A new optical coherence tomography-based calcium scoring system to predict stent underexpansion. EuroIntervention 2018, 13, e2182–e2189. [Google Scholar] [CrossRef]
- Zhang, M.; Matsumura, M.; Usui, E.; Noguchi, M.; Fujimura, T.; Fall, K.N.; Zhang, Z.; Nazif, T.M.; Parikh, S.A.; Rabbani, L.E.; et al. Intravascular Ultrasound-Derived Calcium Score to Predict Stent Expansion in Severely Calcified Lesions. Circ. Cardiovasc. Interv. 2021, 14, e010296. [Google Scholar] [CrossRef]
- Shah, M.; Najam, O.; Bhindi, R.; de Silva, K. Calcium Modification Techniques in Complex Percutaneous Coronary Intervention. Circ. Cardiovasc. Interv. 2021, 14, e009870. [Google Scholar] [CrossRef]
- Hoffmann, R.; Mintz, G.S.; Popma, J.J.; Satler, L.F.; Kent, K.M.; Pichard, A.D.; Leon, M.B. Treatment of calcified coronary lesions with Palmaz-Schatz stents. An intravascular ultrasound study. Eur. Heart J. 1998, 19, 1224–1231. [Google Scholar] [CrossRef]
- Felekos, I.; Karamasis, G.V.; Pavlidis, A.N. When everything else fails: High-pressure balloon for undilatable lesions. Cardiovasc. Revasc. Med. 2018, 193 Pt A, 306–313. [Google Scholar] [CrossRef]
- Raja, Y.; Routledge, H.C.; Doshi, S.N. A noncompliant, high pressure balloon to manage undilatable coronary lesions. Catheter. Cardiovasc. Interv. 2010, 75, 1067–1073. [Google Scholar] [CrossRef]
- Diaz, J.F.; Gomez-Menchero, A.; Cardenal, R.; Sanchez-Gonzalez, C.; Sanghvi, A. Extremely high-pressure dilation with a new noncompliant balloon. Tex. Heart Inst. J. 2012, 39, 635–638. [Google Scholar]
- Secco, G.G.; Ghione, M.; Mattesini, A.; Dall’Ara, G.; Ghilencea, L.; Kilickesmez, K.; De Luca, G.; Fattori, R.; Parisi, R.; Marino, P.N.; et al. Very high-pressure dilatation for undilatable coronary lesions: Indications and results with a new dedicated balloon. EuroIntervention 2016, 12, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Secco, G.G.; Buettner, A.; Parisi, R.; Pistis, G.; Vercellino, M.; Audo, A.; Kambis, M.; Garbo, R.; Porto, I.; Tarantini, G.; et al. Clinical Experience with Very High-Pressure Dilatation for Resistant Coronary Lesions. Cardiovasc. Revasc. Med. 2019, 20, 1083–1087. [Google Scholar] [CrossRef]
- Fabris, E.; Caiazzo, G.; Kilic, I.D.; Serdoz, R.; Secco, G.G.; Sinagra, G.; Lee, R.; Foin, N.; Di Mario, C. Is high pressure postdilation safe in bioresorbable vascular scaffolds? Optical coherence tomography observations after noncompliant balloons inflated at more than 24 atmospheres. Catheter. Cardiovasc. Interv. 2016, 87, 839–846. [Google Scholar] [CrossRef] [PubMed]
- Ishihara, T.; Iida, O.; Takahara, M.; Tsujimura, T.; Okuno, S.; Kurata, N.; Asai, M.; Okamoto, S.; Nanto, K.; Mano, T. Improved crossability with novel cutting balloon versus scoring balloon in the treatment of calcified lesion. Cardiovasc. Interv. Ther. 2021, 36, 198–207. [Google Scholar] [CrossRef] [PubMed]
- Karvouni, E.; Stankovic, G.; Albiero, R.; Takagi, T.; Corvaja, N.; Vaghetti, M.; Di Mario, C.; Colombo, A. Cutting balloon angioplasty for treatment of calcified coronary lesions. Catheter. Cardiovasc. Interv. 2001, 54, 473–481. [Google Scholar] [CrossRef]
- Ozaki, Y.; Yamaguchi, T.; Suzuki, T.; Nakamura, M.; Kitayama, M.; Nishikawa, H.; Inoue, T.; Hara, K.; Usuba, F.; Sakurada, M.; et al. Impact of cutting balloon angioplasty (CBA) prior to bare metal stenting on restenosis. Circ. J. 2007, 71, 1–8. [Google Scholar] [CrossRef]
- Tian, W.; Mahmoudi, M.; Lhermusier, T.; Kiramijyan, S.; Ota, H.; Chen, F.; Torguson, R.; Suddath, W.O.; Satler, L.F.; Pichard, A.D.; et al. Comparison of Rotational Atherectomy, Plain Old Balloon Angioplasty, and Cutting-Balloon Angioplasty Prior to Drug-Eluting Stent Implantation for the Treatment of Heavily Calcified Coronary Lesions. J. Invasive Cardiol. 2015, 27, 387–391. [Google Scholar]
- Takano, M.; Yamamoto, M.; Murakami, D.; Takano, H.; Asai, K.; Yasutake, M.; Seino, Y.; Mizuno, K. Optical coherence tomography after new scoring balloon angioplasty for in-stent restenosis and de novo coronary lesions. Int. J. Cardiol. 2010, 141, e51–e53. [Google Scholar] [CrossRef]
- Fonseca, A.; Costa Jde, R., Jr.; Abizaid, A.; Feres, F.; Abizaid, A.S.; Costa, R.; Staico, R.; Mattos, L.A.; Sousa, A.G.; Grube, E.; et al. Intravascular ultrasound assessment of the novel AngioSculpt scoring balloon catheter for the treatment of complex coronary lesions. J. Invasive Cardiol. 2008, 20, 21–27. [Google Scholar]
- Ashida, K.; Hayase, T.; Shinmura, T. Efficacy of lacrosse NSE using the “leopard-crawl” technique on severely calcified lesions. J. Invasive Cardiol. 2013, 25, 555–564. [Google Scholar]
- Otsuka, Y.; Koyama, T.; Imoto, Y.; Katsuki, Y.; Kawahara, M.; Nakamura, K.; Kodama, S.; Noguchi, H.; Iwasaki, K. Prolonged Inflation Technique Using a Scoring Balloon for Severe Calcified Lesion. Int. Heart J. 2017, 58, 982–987. [Google Scholar] [CrossRef] [PubMed]
- Kawase, Y.; Saito, N.; Watanabe, S.; Bao, B.; Yamamoto, E.; Watanabe, H.; Higami, H.; Matsuo, H.; Ueno, K.; Kimura, T. Utility of a scoring balloon for a severely calcified lesion: Bench test and finite element analysis. Cardiovasc. Interv. Ther. 2014, 29, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Sugawara, Y.; Ueda, T.; Soeda, T.; Watanabe, M.; Okura, H.; Saito, Y. Plaque modification of severely calcified coronary lesions by scoring balloon angioplasty using Lacrosse non-slip element: Insights from an optical coherence tomography evaluation. Cardiovasc. Interv. Ther. 2019, 34, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Karimi Galougahi, K.; Patel, S.; Shlofmitz, R.A.; Maehara, A.; Kereiakes, D.J.; Hill, J.M.; Stone, G.W.; Ali, Z.A. Calcific Plaque Modification by Acoustic Shock Waves: Intravascular Lithotripsy in Coronary Interventions. Circ. Cardiovasc. Interv. 2021, 14, e009354. [Google Scholar] [CrossRef]
- Ali, Z.A.; Brinton, T.J.; Hill, J.M.; Maehara, A.; Matsumura, M.; Karimi Galougahi, K.; Illindala, U.; Gotberg, M.; Whitbourn, R.; Van Mieghem, N.; et al. Optical Coherence Tomography Characterization of Coronary Lithoplasty for Treatment of Calcified Lesions: First Description. JACC Cardiovasc. Imaging 2017, 10, 897–906. [Google Scholar] [CrossRef]
- Kereiakes, D.J.; Di Mario, C.; Riley, R.F.; Fajadet, J.; Shlofmitz, R.A.; Saito, S.; Ali, Z.A.; Klein, A.J.; Price, M.J.; Hill, J.M.; et al. Intravascular Lithotripsy for Treatment of Calcified Coronary Lesions: Patient-Level Pooled Analysis of the Disrupt CAD Studies. JACC Cardiovasc. Interv. 2021, 14, 1337–1348. [Google Scholar] [CrossRef]
- Tomey, M.I.; Kini, A.S.; Sharma, S.K. Current status of rotational atherectomy. JACC Cardiovasc. Interv. 2014, 7, 345–353. [Google Scholar] [CrossRef]
- Kini, A.S.; Vengrenyuk, Y.; Pena, J.; Motoyama, S.; Feig, J.E.; Meelu, O.A.; Rajamanickam, A.; Bhat, A.M.; Panwar, S.; Baber, U.; et al. Optical coherence tomography assessment of the mechanistic effects of rotational and orbital atherectomy in severely calcified coronary lesions. Catheter. Cardiovasc. Interv. 2015, 86, 1024–1032. [Google Scholar] [CrossRef]
- Yamamoto, M.H.; Maehara, A.; Karimi Galougahi, K.; Mintz, G.S.; Parviz, Y.; Kim, S.S.; Koyama, K.; Amemiya, K.; Kim, S.Y.; Ishida, M.; et al. Mechanisms of Orbital Versus Rotational Atherectomy Plaque Modification in Severely Calcified Lesions Assessed by Optical Coherence Tomography. JACC Cardiovasc. Interv. 2017, 10, 2584–2586. [Google Scholar] [CrossRef]
- Ali, Z.A.; McEntegart, M.; Hill, J.M.; Spratt, J.C. Intravascular lithotripsy for treatment of stent underexpansion secondary to severe coronary calcification. Eur. Heart J. 2020, 41, 485–486. [Google Scholar] [CrossRef]
- Salazar, C.; Escaned, J.; Tirado, G.; Gonzalo, N. Intravascular lithotripsy for recurrent restenosis caused by severe calcific neoatherosclerosis. EuroIntervention 2020, 16, e351–e352. [Google Scholar] [CrossRef] [PubMed]
- Tovar Forero, M.N.; Wilschut, J.; van Mieghem, N.M.; Daemen, J. Coronary lithoplasty: A novel treatment for stent underexpansion. Eur. Heart J. 2019, 40, 221. [Google Scholar] [CrossRef] [PubMed]
- Alfonso, F.; Bastante, T.; Antuna, P.; de la Cuerda, F.; Cuesta, J.; Garcia-Guimaraes, M.; Rivero, F. Coronary Lithoplasty for the Treatment of Undilatable Calcified De Novo and In-Stent Restenosis Lesions. JACC Cardiovasc. Interv. 2019, 12, 497–499. [Google Scholar] [CrossRef] [PubMed]
- Seif, S.; Kumar, A.; Arya, S.; Karthikeyan, V.J. Intravascular lithotripsy to treat an underexpanded coronary stent during index procedure: A case report study. Avicenna J. Med. 2021, 11, 54–57. [Google Scholar] [CrossRef]
- Ielasi, A.; Loffi, M.; de Blasio, G.; Tespili, M. “Rota-Tripsy”: A Successful Combined Approach for the Treatment of a Long and Heavily Calcified Coronary Lesion. Cardiovasc. Revasc. Med. 2020, 21, 152–154. [Google Scholar] [CrossRef]
- Wilson, S.J.; Spratt, J.C.; Hill, J.; Spence, M.S.; Cosgrove, C.; Jones, J.; Strange, J.W.; Halperin, H.; Walsh, S.J.; Hanratty, C.G. Incidence of “shocktopics” and asynchronous cardiac pacing in patients undergoing coronary intravascular lithotripsy. EuroIntervention 2020, 15, 1429–1435. [Google Scholar] [CrossRef]
- Ali, Z.A.; Hill, J.; Saito, S.; Gonzalo, N.; Mario, C.D.; Riley, R.; Honton, B.; Maehara, A.; Matsumura, M.; Kereiakes, D.; et al. TCT-163 Optical Coherence Tomography Characterization of Eccentric Versus Concentric Calcium Treated With Shockwave Intravascular Lithotripsy: Patient-Level Pooled Analysis of the Disrupt CAD OCT Substudies. J. Am. Coll. Cardiol. 2021, 78 (Suppl. S), B67–B68. [Google Scholar] [CrossRef]
- Farb, A.; Roberts, D.K.; Pichard, A.D.; Kent, K.M.; Virmani, R. Coronary artery morphologic features after coronary rotational atherectomy: Insights into mechanisms of lumen enlargement and embolization. Am. Heart J. 1995, 129, 1058–1067. [Google Scholar] [CrossRef]
- Cockburn, J.; Hildick-Smith, D.; Cotton, J.; Doshi, S.; Hanratty, C.; Ludman, P.; Robinson, D.; Redwood, S.; de Belder, M.; de Belder, A. Contemporary clinical outcomes of patients treated with or without rotational coronary atherectomy—An analysis of the UK central cardiac audit database. Int. J. Cardiol. 2014, 170, 381–387. [Google Scholar] [CrossRef]
- Van Gaal, W.J.; Banning, A.P. Percutaneous coronary intervention and the no-reflow phenomenon. Expert Rev. Cardiovasc. Ther. 2007, 5, 715–731. [Google Scholar] [CrossRef]
- Barbato, E.; Carrie, D.; Dardas, P.; Fajadet, J.; Gaul, G.; Haude, M.; Khashaba, A.; Koch, K.; Meyer-Gessner, M.; Palazuelos, J.; et al. European expert consensus on rotational atherectomy. EuroIntervention 2015, 11, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Beohar, N.; Kaltenbach, L.A.; Wojdyla, D.; Pineda, A.M.; Rao, S.V.; Stone, G.W.; Leon, M.B.; Sanghvi, K.A.; Moses, J.W.; Kirtane, A.J. Trends in Usage and Clinical Outcomes of Coronary Atherectomy: A Report From the National Cardiovascular Data Registry CathPCI Registry. Circ. Cardiovasc. Interv. 2020, 13, e008239. [Google Scholar] [CrossRef] [PubMed]
- Isogai, T.; Yasunaga, H.; Matsui, H.; Tanaka, H.; Fushimi, K. Relationship between hospital volume and major cardiac complications of rotational atherectomy: A nationwide retrospective cohort study in Japan. J. Cardiol. 2016, 67, 442–448. [Google Scholar] [CrossRef] [PubMed]
- Genereux, P.; Lee, A.C.; Kim, C.Y.; Lee, M.; Shlofmitz, R.; Moses, J.W.; Stone, G.W.; Chambers, J.W. Orbital Atherectomy for Treating De Novo Severely Calcified Coronary Narrowing (1-Year Results from the Pivotal ORBIT II Trial). Am. J. Cardiol. 2015, 115, 1685–1690. [Google Scholar] [CrossRef]
- Lee, M.S.; Gordin, J.S.; Stone, G.W.; Sharma, S.K.; Saito, S.; Mahmud, E.; Chambers, J.; Genereux, P.; Shlofmitz, R. Orbital and rotational atherectomy during percutaneous coronary intervention for coronary artery calcification. Catheter. Cardiovasc. Interv. 2018, 92, 61–67. [Google Scholar] [CrossRef]
- Shlofmitz, E.; Shlofmitz, R.; Lee, M.S. Orbital Atherectomy: A Comprehensive Review. Interv. Cardiol. Clin. 2019, 8, 161–171. [Google Scholar]
- Sulimov, D.S.; Abdel-Wahab, M.; Toelg, R.; Kassner, G.; Geist, V.; Richardt, G. Stuck rotablator: The nightmare of rotational atherectomy. EuroIntervention 2013, 9, 251–258. [Google Scholar] [CrossRef]
- Bhatt, P.; Parikh, P.; Patel, A.; Chag, M.; Chandarana, A.; Parikh, R.; Parikh, K. Long-term safety and performance of the orbital atherectomy system for treating calcified coronary artery lesions: 5-Year follow-up in the ORBIT I trial. Cardiovasc. Revasc. Med. 2015, 16, 213–216. [Google Scholar] [CrossRef]
- Lee, M.; Genereux, P.; Shlofmitz, R.; Phillipson, D.; Anose, B.M.; Martinsen, B.J.; Himmelstein, S.I.; Chambers, J.W. Orbital atherectomy for treating de novo, severely calcified coronary lesions: 3-year results of the pivotal ORBIT II trial. Cardiovasc. Revasc. Med. 2017, 18, 261–264. [Google Scholar] [CrossRef]
- Meraj, P.M.; Shlofmitz, E.; Kaplan, B.; Jauhar, R.; Doshi, R. Clinical outcomes of atherectomy prior to percutaneous coronary intervention: A comparison of outcomes following rotational versus orbital atherectomy (COAP-PCI study). J. Interv. Cardiol. 2018, 31, 478–485. [Google Scholar] [CrossRef]
- Genereux, P.; Kirtane, A.J.; Kandzari, D.E.; Armstrong, E.J.; Krucoff, M.W.; Redfors, B.; Ben-Yehuda, O.; Lerew, D.R.; Ali, Z.A.; Maehara, A.; et al. Randomized evaluation of vessel preparation with orbital atherectomy prior to drug-eluting stent implantation in severely calcified coronary artery lesions: Design and rationale of the ECLIPSE trial. Am. Heart J. 2022, 249, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Koster, R.; Kahler, J.; Brockhoff, C.; Munzel, T.; Meinertz, T. Laser coronary angioplasty: History, present and future. Am. J. Cardiovasc. Drugs 2002, 2, 197–207. [Google Scholar] [CrossRef] [PubMed]
- Mintz, G.S.; Kovach, J.A.; Javier, S.P.; Pichard, A.D.; Kent, K.M.; Popma, J.J.; Salter, L.F.; Leon, M.B. Mechanisms of lumen enlargement after excimer laser coronary angioplasty. An intravascular ultrasound study. Circulation 1995, 92, 3408–3414. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, J.P.; Hobson, A.R.; McKenzie, D.; Shah, N.; Sinha, M.K.; Wells, T.A.; Levy, T.M.; Swallow, R.A.; Talwar, S.; O’Kane, P.D. Beyond the balloon: Excimer coronary laser atherectomy used alone or in combination with rotational atherectomy in the treatment of chronic total occlusions, non-crossable and non-expansible coronary lesions. EuroIntervention 2013, 9, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Mangieri, A.; Jabbour, R.J.; Tanaka, A.; Aurelio, A.; Colombo, A.; Latib, A. Excimer laser facilitated coronary angioplasty of a heavy calcified lesion treated with bioresorbable scaffolds. J. Cardiovasc. Med. 2016, 17 (Suppl. 2), e149–e150. [Google Scholar] [CrossRef]
- Mohandes, M.; Rojas, S.; Torres, M.; Moreno, C.; Fernandez, F.; Guarinos, J.; Bardaji, A. Percutaneous coronary intervention of chronically occluded saphenous vein grafts using excimer laser atherectomy as an adjuvant therapy. Cardiovasc. Revasc. Med. 2017, 18, 2–6. [Google Scholar] [CrossRef]
- Azzalini, L.; Ly, H.Q. Laser atherectomy for balloon failure in chronic total occlusion. When the going gets tough. Int. Heart J. 2014, 55, 546–549. [Google Scholar] [CrossRef][Green Version]
- Niccoli, G.; Di Vito, L.; Montone, R.A.; Porto, I.; Crea, F. Excimer laser for a highly stenotic saphenous vein graft: Evidence of debulking by optical coherence tomography. EuroIntervention 2014, 9, 1484. [Google Scholar] [CrossRef]
- Mohandes, M.; Rojas, S.; Moreno, C.; Fernandez, F.; Fuertes, M.; Guarinos, J. Excimer Laser in Percutaneous Coronary Intervention of Device Uncrossable Chronic Total and Functional Occlusions. Cardiovasc. Revasc. Med. 2020, 21, 657–660. [Google Scholar] [CrossRef]
- Lee, T.; Shlofmitz, R.A.; Song, L.; Tsiamtsiouris, T.; Pappas, T.; Madrid, A.; Jeremias, A.; Haag, E.S.; Ali, Z.A.; Moses, J.W.; et al. The effectiveness of excimer laser angioplasty to treat coronary in-stent restenosis with peri-stent calcium as assessed by optical coherence tomography. EuroIntervention 2019, 15, e279–e288. [Google Scholar] [CrossRef]
- Latib, A.; Takagi, K.; Chizzola, G.; Tobis, J.; Ambrosini, V.; Niccoli, G.; Sardella, G.; DiSalvo, M.E.; Armigliato, P.; Valgimigli, M.; et al. Excimer Laser LEsion modification to expand non-dilatable stents: The ELLEMENT registry. Cardiovasc. Revasc. Med. 2014, 15, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Karacsonyi, J.; Armstrong, E.J.; Truong, H.T.D.; Tsuda, R.; Kokkinidis, D.G.; Martinez-Parachini, J.R.; Alame, A.J.; Danek, B.A.; Karatasakis, A.; Roesle, M.; et al. Contemporary Use of Laser During Percutaneous Coronary Interventions: Insights from the Laser Veterans Affairs (LAVA) Multicenter Registry. J. Invasive Cardiol. 2018, 30, 195–201. [Google Scholar] [CrossRef]
- Mintz, G.S. Intravascular imaging of coronary calcification and its clinical implications. JACC Cardiovasc. Imaging 2015, 8, 461–471. [Google Scholar] [CrossRef] [PubMed]
- Kinnaird, T.; Gallagher, S.; Sharp, A.; Protty, M.; Salim, T.; Ludman, P.; Copt, S.; Curzen, N.; Mamas, M.A. Operator volumes and in-hospital outcomes: An analysis of 7,740 rotational atherectomy procedures from the BCIS national database. JACC Cardiovasc. Interv. 2021, 14, 1423–1430. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | Study Arms | Relevant Endpoint(s) | Outcomes/Results * | Conclusions |
|---|---|---|---|---|
| Cutting Balloon Angioplasty | ||||
| GRT [10] | CBA vs. PTCA | Binary restenosis after 6 months | CBA: 31.4% PTCA: 30.4% p = NS | No reduction in restenosis with CBA after 6 months. |
| REDUCE (unpublished) | CBA vs. PTCA | Binary restenosis after 6 months | CBA: 32.7% PTCA: 25.5% p = NS | No reduction in restenosis with CBA after 6 months. |
| RESCUT [11] | CBA vs. PTCA for ISR | Binary restenosis after 7 months | CBA: 29.8% PTCA: 31.4% p = NS | No reduction in recurrent ISR with CBA after 7 months. |
| CBA before DES [12] | CBA before DES vs. BA | Minimum stent CSA (mm2), Acute lumen gain (mm2) | CBA:6.26 ± 0.4, 3.74 ± 0.38 BA:5.03 ± 0.33, 2.44 ± 0.29 p = 0.031, 0.015 | CBA achieved larger lumen CSA and larger lumen gain compared to BA. |
| Mechanisms of Acute Lumen Gain Following Cutting Balloon Angioplasty in Calcified and Noncalcified Lesions [13] | CBA vs. BA in calcified and non-calcified group | ΔEEM CSA (mm2), ΔP + M CSA (mm2), Δlumen CSA (mm2) | Calcified lesions: CBA: 1.4 ± 1.7, −2.3 ± 1.9, 3.7 ± 1.5 BA: 1.2 ± 1.2, −1.8 ± 1.9, 3.0 ± 1.5 p = NS, NS, 0.05 Non-calcified lesions: CBA: 1.0 ± 1.8, −2.9 ± 2.1, 3.9 ± 1.9 BA: 1.6 ± 1.8, −2.0 ± 1.9, 3.6 ± 1.6 p = NS(0.11), 0.03, NS | In calcified lesions, CBA achieves a larger lumen gain vs. BA. In noncalcified lesions, there is larger plaque reduction with CBA but no difference in lumen gain vs. BA. |
| Scoring Balloon Angioplasty | ||||
| Intimal disruption and cobalt-chromium DES [14] | SBA vs. BA | Stent expansion, lumen eccentricity, intimal disruption frequency, extent | SBA: 68%, 0.94, 68%, 122° BA: 62.1%, 0.80, 0.8, 65° p = 0.017, 0.18, 0.035, 0.035 | SBA achieved increased stent expansion with similar lumen eccentricity when compared with BA. SBA had more frequent and extensive intimal disruption when compared with BA. |
| Predilatation with SBA vs. NC [15] | SBA vs. NC | Stent expansion (mm), in-stent late loss after 1 year (mm) | SBA: 70.7 ± 11.2, 0.71 ± 0.63 NC: 69.1 ± 11.1, 0.23 ± 0.52 p = NS, 0.03 | SBA achieved decreased in-stent late loss when compared to NC after 1 year. There was no difference in stent expansion between SBA and NC groups. |
| Rotational Atherectomy | ||||
| ERBAC [16] | RA vs. ELCA vs. PTCA | Procedural success ∑, TVR after 6 months | RA: 89%, 42.4% ELCA: 77%, 46% PTCA: 80%, 31.9% p = 0.0019, 0.013 | RA achieved superior procedural success when compared with ELCA and PTCA, but both RA and ELCA had unfavorable late outcomes when compared with PTCA. |
| COBRA [17] | RA vs. PTCA | Binary restenosis after 6 months | RA: 49% PTCA: 51% p = 0.35 | RA did not reduce restenosis after 6 months when compared with PTCA. |
| DART [18] | RA vs. PTCA in small vessels (2–3 mm) | TVF after 12 months | RA: 30.5% PTCA: 31.2% p = 0.98 | RA did not reduce TVF after 12 months when compared with PTCA. |
| STRATAS [19] | Aggressive RA (B/A 0.7–0.9) with PTCA (<1 bar) vs. routine RA (B/A < 0.7) with PTCA (4 bar) | Binary restenosis after 6 months | Aggressive: 58% Routine: 52% p = NS | Aggressive RA debulking did not reduce restenosis after 6 months when compared with routine RA debulking. |
| CARAT [20] | Aggressive RA (B/A > 0.7) vs. Routine RA (B/A = 0.7) | MACE after 6 months | Aggressive: 36.3% Routine: 32.7% p = NS | Aggressive RA debulking did not reduce MACE after 6 months compared with routine RA debulking. |
| ROOSTER [21] | RA (B/A = 0.7) vs. PTCA for diffuse ISR with IVUS guidance | TLR after 9 months | RA: 32% PTCA: 45% p = 0.04 | RA achieved less TLR after 9 months compared with PTCA in diffuse ISR. |
| ARTIST [22] | RA (B/A = 0.7) vs. PTCA for diffuse ISR with IVUS guidance in a subset | MACE after 6 months | RA: 80% PTCA: 91% p = 0.0052 | PTCA achieved a lower MACE when compared to RA in diffuse ISR. |
| ROTAXUS [23] | RA with DES vs. DES | Late lumen loss (mm) after 9 months | RA with DES: 0.31 ± 0.52 DES: 0.44 ± 0.58 p = 0.04 | RA before DES achieved increased late lumen loss when compared to DES alone. |
| Prepare-CALC [24] | RA vs. modified CSA | Successful stent delivery and expansion, late lumen loss (mm) after 9 months | RA: 98%, 0.22 ± 0.41 CSA: 81%, 0.16 ± 0.40 p = 0.001, 0.21 | RA achieved greater success at stent delivery and expansion than CSA and had similar late lumen loss rates after 9 months. |
| Orbital Atherectomy | ||||
| ORBIT I [25] | OA single arm | Device success ∫ Procedural success ∬ TLR, MACE after 6 months | Device success: 98% Procedural success: 94% TLR, MACE (6 months): 2%, 8% | OA successfully facilitated stent delivery with a low cumulative TLR and MACE after 6 months. |
| ORBIT II [26] | OA single arm | Safety endpoint Ω (95% CI) Efficacy endpoint Ψ (95% CI) | Safety endpoint: 89.6% (86.7–92.5%) Efficacy endpoint: 88.9% (85.5–91.6%) | OA significantly exceeded the primary safety and efficacy endpoints of 83% and 82% respectively. OA also improved in-hospital and 30-day outcomes compared to historic controls with severe CAC. |
| Laser Atherectomy | ||||
| LAVA [27] | ELCA vs. PTCA in native vessels or SVG | MACE after 6 months | ELCA: 28.9% PTCA: 23.5% p = 0.55 | ELCA did not reduce MACE after 6 months compared with PTCA in native vessels or SVG. |
| AMRO [28] | ELCA vs. PTCA in native vessels | MACE after 6 months | ELCA: 33.3% PTCA: 29.9% p = 0.55 | ELCA did not reduce MACE after 6 months compared with PTCA in native vessels. |
| Intravascular Lithotripsy | ||||
| DISRUPT CAD I [29] | Coronary IVL single arm | Safety endpoint Ω Effectiveness endpoint Ψ | Safety endpoint: 95% Effectiveness endpoint: 98.5% | Coronary IVL safely and effectively aided stent placement with minimal perioperative complications. |
| DISRUPT CAD II [30] | Coronary IVL single arm | Safety endpoint Ω Effectiveness endpoint Ψ Calcium fractures measured by OCT Mean stent expansion | Safety endpoint: 100% Effectiveness endpoint: 94.2% Calcium fractures: 67.4% Mean stent expansion: 101.7% | Coronary IVL safely and effectively aided stent placement with minimal perioperative complications. OCT demonstrated that calcium fractures were an underlying mechanism for IVL. Coronary IVL allowed for excellent stent expansion. |
| DISRUPT CAD III [31] | Coronary IVL single arm | Safety endpoint Ω (lower-bound of 95% CI) Effectiveness endpoint Ψ (lower-bound of 95% CI) | Safety endpoint: 92.2% (89.9%, p = 0.0001) Effectiveness endpoint: 92.4% (90.2%, p = 0.0001) | Coronary IVL safely and successfully assisted with stent delivery. The lower bounds of the 95% CI for the safety and effectiveness endpoints exceeded the performance goal of 84.4% and 83.4%, respectively. |
| DISRUPT CAD IV [32] | Coronary IVL single arm | Safety endpoint Ω: CAD IV cohort vs. propensity matched historical IVL control group Effectiveness endpoint Ψ: CAD IV cohort vs. propensity matched historical IVL control group | Safety endpoint: 93.8% vs. 91.2%, p = 0.008 Effectiveness endpoint: 93.8% vs. 91.6%, p = 0.007 | Coronary IVL safely and effectively aided stent placement with minimal perioperative complications. The results from coronary IVL in the Japanese CAD IV cohort were non-inferior to those from a study of patients treated with IVL in the USA and Europe. |
| Severity | OCT-Based Calcium Score
| IVUS-Based Calcium Score
|
|---|---|---|
| Mild to moderate | 0–3 | 0–1 |
| Severe | ≥4 | ≥2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Angsubhakorn, N.; Kang, N.; Fearon, C.; Techorueangwiwat, C.; Swamy, P.; Brilakis, E.S.; Bharadwaj, A.S. Contemporary Management of Severely Calcified Coronary Lesions. J. Pers. Med. 2022, 12, 1638. https://doi.org/10.3390/jpm12101638
Angsubhakorn N, Kang N, Fearon C, Techorueangwiwat C, Swamy P, Brilakis ES, Bharadwaj AS. Contemporary Management of Severely Calcified Coronary Lesions. Journal of Personalized Medicine. 2022; 12(10):1638. https://doi.org/10.3390/jpm12101638
Chicago/Turabian StyleAngsubhakorn, Natthapon, Nicolas Kang, Colleen Fearon, Chol Techorueangwiwat, Pooja Swamy, Emmanouil S. Brilakis, and Aditya S. Bharadwaj. 2022. "Contemporary Management of Severely Calcified Coronary Lesions" Journal of Personalized Medicine 12, no. 10: 1638. https://doi.org/10.3390/jpm12101638
APA StyleAngsubhakorn, N., Kang, N., Fearon, C., Techorueangwiwat, C., Swamy, P., Brilakis, E. S., & Bharadwaj, A. S. (2022). Contemporary Management of Severely Calcified Coronary Lesions. Journal of Personalized Medicine, 12(10), 1638. https://doi.org/10.3390/jpm12101638