
Factors Influencing Personalized Management of Vestibular Schwannoma: A Systematic Review


 ,
,  ,
,  and
and 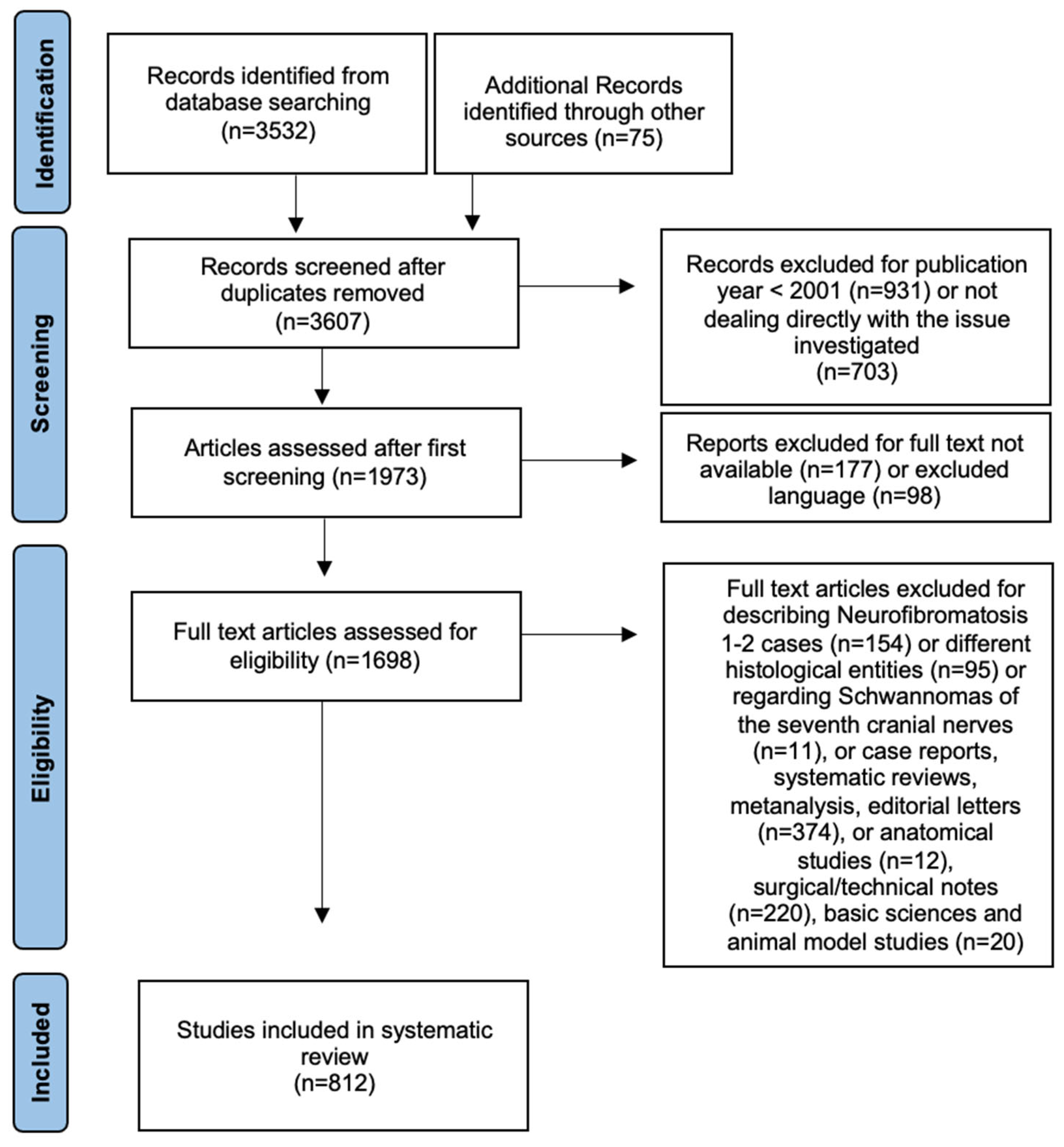{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
3. Results and Discussion
3.1. Incidental VS
3.2. Tumor Size
3.3. Tumor Regrowth after sRT
3.4. Planned Sub-Total Resection and Residual Tumor Management
3.5. Patient’s Age
3.6. Symptoms
3.6.1. Dizziness
3.6.2. Tinnitus
3.6.3. Hearing Function
- Age (usually less than 65–70 years old) [105]
- The preoperative hearing class, despite the size of the VS, correlates with postoperative hearing results [108].
- Degree of fundus filling: Tringali et al., using regression analysis, demonstrated that the degree of IAC involvement was the most correlated predictor of successful hearing preservation. When the fundus was completely involved, the possibility of preserving hearing dropped significantly, in absolute terms and also compared to all other degrees of IAC filling [109].
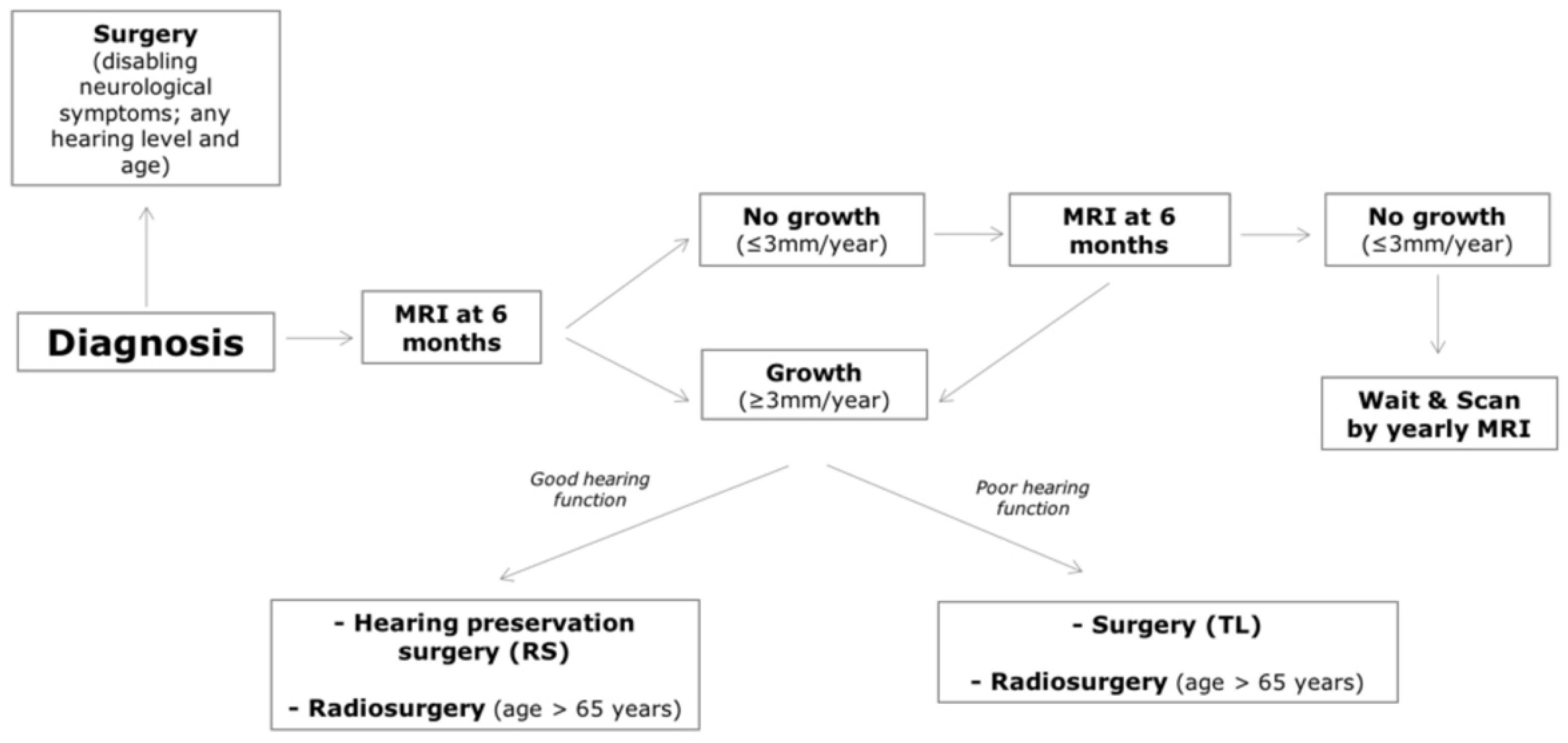
3.7. Multidisciplinary and Personalized Management of VS in Our Experience
4. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Carlson, M.L.; Link, M.J. Vestibular Schwannomas. N. Engl. J. Med. 2021, 384, 1335–1348. [Google Scholar] [CrossRef]
- Halliday, J.; Rutherford, S.A.; McCabe, M.G.; Evans, D.G. An Update on the Diagnosis and Treatment of Vestibular Schwannoma. Expert Rev. Neurother. 2018, 18, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Sergi, B.; Balducci, M.; Paludetti, G.; Olivi, A.; Picciotti, P.M.; de Corso, E.; Passali, G.C.; Fetoni, A.R.; Lucidi, D. Decision Making on Vestibular Schwannoma: Lessons from a Multidisciplinary Board. World Neurosurg. 2022, 157, e506–e513. [Google Scholar] [CrossRef] [PubMed]
- Carlson, M.L.; Habermann, E.B.; Wagie, A.E.; Driscoll, C.L.; van Gompel, J.J.; Jacob, J.T.; Link, M.J. The Changing Landscape of Vestibular Schwannoma Management in the United States—A Shift Toward Conservatism. Otolaryngol. Head Neck Surg. 2015, 153, 440–446. [Google Scholar] [CrossRef]
- Gal, T.J.; Shinn, J.; Huang, B. Current Epidemiology and Management Trends in Acoustic Neuroma. Otolaryngol. Head Neck Surg. 2010, 142, 677–681. [Google Scholar] [CrossRef]
- Babu, R.; Sharma, R.; Bagley, J.H.; Hatef, J.; Friedman, A.H.; Adamsons, C. Vestibular Schwannomas in the Modern Era: Epidemiology, Treatment Trends, and Disparities in Management. J. Neurosurg. 2013, 119, 121–130. [Google Scholar] [CrossRef]
- Lucidi, D.; Fabbris, C.; Cerullo, R.; di Gioia, S.; Calvaruso, F.; Monzani, D.; Alicandri-Ciufelli, M.; Marchioni, D.; Presutti, L. Quality of Life in Vestibular Schwannoma: A Comparison of Three Surgical Techniques. Eur. Arch. Otorhinolaryngol. 2022, 279, 1795–1803. [Google Scholar] [CrossRef]
- Gauden, A.; Weir, P.; Hawthorne, G.; Kaye, A. Systematic Review of Quality of Life in the Management of Vestibular Schwannoma. J. Clin. Neurosci. 2011, 18, 1573–1584. [Google Scholar] [CrossRef]
- Marinelli, J.P.; Grossardt, B.R.; Lohse, C.M.; Carlson, M.L. Prevalence of Sporadic Vestibular Schwannoma: Reconciling Temporal Bone, Radiologic, and Population-Based Studies. Otol. Neurotol. 2019, 40, 384. [Google Scholar] [CrossRef]
- Carlson, M.L.; Lees, K.A.; Patel, N.S.; Lohse, C.M.; Neff, B.A.; Link, M.J.; Driscoll, C.L. The Clinical Behavior of Asymptomatic Incidental Vestibular Schwannomas Is Similar to That of Symptomatic Tumors. Otol. Neurotol. 2016, 37, 1435–1441. [Google Scholar] [CrossRef]
- Tawfik, K.O.; Alexander, T.H.; Saliba, J.; Mastrodimos, B.; Cueva, R.A. The Effect of Tumor Size on Likelihood of Hearing Preservation After Retrosigmoid Vestibular Schwannoma Resection. Otol. Neurotol. 2020, 41, e1333–e1339. [Google Scholar] [CrossRef] [PubMed]
- Dang, L.; Tu, N.C.Y.; Chan, E.Y. Current Imaging Tools for Vestibular Schwannoma. Curr. Opin. Otolaryngol. Head Neck Surg. 2020, 28, 302–307. [Google Scholar] [CrossRef] [PubMed]
- Torres Maldonado, S.; Naples, J.G.; Fathy, R.; Eliades, S.J.; Lee, J.Y.K.; Brant, J.A.; Ruckenstein, M.J. Recent Trends in Vestibular Schwannoma Management: An 11-Year Analysis of the National Cancer Database. Otolaryngol. Head Neck Surg. 2019, 161, 137–143. [Google Scholar] [CrossRef]
- Goldbrunner, R.; Weller, M.; Regis, J.; Lund-Johansen, M.; Stavrinou, P.; Reuss, D.; Evans, D.G.; Lefranc, F.; Sallabanda, K.; Falini, A.; et al. EANO Guideline on the Diagnosis and Treatment of Vestibular Schwannoma. Neuro Oncol. 2020, 22, 31–45. [Google Scholar] [CrossRef]
- Fieux, M.; Pouzet, C.; Bonjour, M.; Zaouche, S.; Jouanneau, E.; Tringali, S. MRI Monitoring of Small and Medium-Sized Vestibular Schwannomas: Predictors of Growth. Acta Otolaryngol. 2020, 140, 361–365. [Google Scholar] [CrossRef] [PubMed]
- Kirchmann, M.; Karnov, K.; Hansen, S.; Dethloff, T.; Stangerup, S.E.; Caye-Thomasen, P. Ten-Year Follow-up on Tumor Growth and Hearing in Patients Observed With an Intracanalicular Vestibular Schwannoma. Neurosurgery 2017, 80, 49–56. [Google Scholar] [CrossRef] [PubMed]
- Paldor, I.; Chen, A.S.; Kaye, A.H. Growth Rate of Vestibular Schwannoma. J. Clin. Neurosci. 2016, 32, 1–8. [Google Scholar] [CrossRef]
- Agrawal, Y.; Clark, J.H.; Limb, C.J.; Niparko, J.K.; Francis, H.W. Predictors of Vestibular Schwannoma Growth and Clinical Implications. Otol. Neurotol. 2010, 31, 807–812. [Google Scholar] [CrossRef]
- Hentschel, M.A.; Hannink, G.; Steens, S.C.A.; Mulder, J.J.S.; Rovers, M.M.; Kunst, H.P.M. Development of a Model to Predict Vestibular Schwannoma Growth: An Opportunity to Introduce New Wait and Scan Strategies. Clin. Otolaryngol. 2021, 46, 273–283. [Google Scholar] [CrossRef]
- Schmidt, R.F.; Boghani, Z.; Choudhry, O.J.; Eloy, J.A.; Jyung, R.W.; Liu, J.K. Incidental Vestibular Schwannomas: A Review of Prevalence, Growth Rate, and Management Challenges. Neurosurg. Focus 2012, 33, E4. [Google Scholar] [CrossRef]
- Kiyofuji, S.; Neff, B.A.; Carlson, M.L.; Driscoll, C.L.W.; Link, M.J. Large and Small Vestibular Schwannomas: Same, yet Different Tumors. Acta Neurochir. 2021, 163, 2199–2207. [Google Scholar] [CrossRef] [PubMed]
- Samii, M.; Gerganov, V.M.; Samii, A. Functional Outcome after Complete Surgical Removal of Giant Vestibular Schwannomas. J. Neurosurg. 2010, 112, 860–867. [Google Scholar] [CrossRef] [PubMed]
- Macielak, R.J.; Harris, M.S.; Kirsch, C.F.; Prevedello, L.M.; Adunka, O.F. Influence of Posterior Fossa Volume on Clinical Outcomes After Vestibular Schwannoma Resection. Otol. Neurotol. 2016, 37, 1155–1161. [Google Scholar] [CrossRef] [PubMed]
- Bozhkov, Y.; Shawarba, J.; Feulner, J.; Winter, F.; Rampp, S.; Hoppe, U.; Doerfler, A.; Iro, H.; Buchfelder, M.; Roessler, K. Prediction of Hearing Preservation in Vestibular Schwannoma Surgery According to Tumor Size and Anatomic Extension. Otolaryngol. Head Neck Surg. 2022, 166, 530–536. [Google Scholar] [CrossRef] [PubMed]
- Ismail, O.; Sobhy, O.; Assal, S.; Sanghera, P.; Begg, P.; Irving, R. Comparing Hearing Outcomes in Irradiated and Conservatively Managed Vestibular Schwannoma. Otol. Neurotol. 2022, 43, E374–E381. [Google Scholar] [CrossRef] [PubMed]
- Zanoletti, E.; Mazzoni, A. Hearing Preservation in Small Acoustic Neuroma: Observation or Active Therapy? Literature Review and Institutional Experience. Acta Neurochir. 2019, 161, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Myrseth, E.; Møller, P.; Pedersen, P.H.; Lund-Johansen, M. Vestibular Schwannoma: Surgery or Gamma Knife Radiosurgery? A Prospective, Nonrandomized Study. Neurosurgery 2009, 64, 654–661. [Google Scholar] [CrossRef]
- Pollock, B.E.; Driscoll, C.L.W.; Foote, R.L.; Link, M.J.; Gorman, D.A.; Bauch, C.D.; Mandrekar, J.N.; Krecke, K.N.; Johnson, C.H. Patient Outcomes after Vestibular Schwannoma Management: A Prospective Comparison of Microsurgical Resection and Stereotactic Radiosurgery. Neurosurgery 2006, 59, 77–83. [Google Scholar] [CrossRef]
- Huang, C.W.; Tu, H.T.; Chuang, C.Y.; Chang, C.S.; Chou, H.H.; Lee, M.T.; Huang, C.F. Gamma Knife Radiosurgery for Large Vestibular Schwannomas Greater than 3 Cm in Diameter. J. Neurosurg. 2018, 128, 1380–1387. [Google Scholar] [CrossRef]
- Slattery, W.H. Microsurgery After Radiosurgery or Radiotherapy for Vestibular Schwannomas. Otolaryngol. Clin. N. Am. 2009, 42, 707–715. [Google Scholar] [CrossRef]
- Nakamura, H.; Jokura, H.; Takahashi, K.; Boku, N.; Akabane, A.; Yoshimoto, T. Serial Follow-up MR Imaging after Gamma Knife Radiosurgery for Vestibular Schwannoma. AJNR Am. J. Neuroradiol. 2000, 21, 1540–1546. [Google Scholar] [PubMed]
- Yomo, S.; Arkha, Y.; Delsanti, C.; Roche, P.H.; Thomassin, J.M.; Régis, J. Repeat Gamma Knife Surgery for Regrowth of Vestibular Schwannomas. Neurosurgery 2009, 64, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Fu, V.X.; Verheul, J.B.; Beute, G.N.; Leenstra, S.; Kunst, H.P.M.; Mulder, J.J.S.; Hanssens, P.E.J. Retreatment of Vestibular Schwannoma with Gamma Knife Radiosurgery: Clinical Outcome, Tumor Control, and Review of Literature. J. Neurosurg. 2018, 129, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Roche, P.H.; Khalil, M.; Thomassin, J.M.; Delsanti, C.; Régis, J. Surgical Removal of Vestibular Schwannoma after Failed Gamma Knife Radiosurgery. Prog. Neurol. Surg. 2008, 21, 152–157. [Google Scholar] [CrossRef]
- Roche, P.H.; Robitail, S.; Delsanti, C.; Marouf, R.; Pellet, W.; Régis, J. Radiochirurgie Gamma Knife Après Microchirurgie Des Schwannomes Vestibulaires et Stratégie Combinée Radio-Microchirurgicale. Neurochirurgie 2004, 50, 394–400. [Google Scholar]
- Lee, D.J.; Westra, W.H.; Staecker, H.; Long, D.; Niparko, J.K. Clinical and Histopathologic Features of Recurrent Vestibular Schwannoma (Acoustic Neuroma) after Stereotactic Radiosurgery. Otol. Neurotol. 2003, 24, 650–660. [Google Scholar] [CrossRef]
- Bloch, D.C.; Oghalai, J.S.; Jackler, R.K.; Osofsky, M.; Pitts, L.H. The Fate of the Tumor Remnant after Less-than-Complete Acoustic Neuroma Resection. Otolaryngol. Head Neck Surg. 2004, 130, 104–112. [Google Scholar] [CrossRef]
- Freeman, S.R.M.; Ramsden, R.T.; Saeed, S.R.; Alzoubi, F.Q.; Simo, R.; Rutherford, S.A.; King, A.T. Revision Surgery for Residual or Recurrent Vestibular Schwannoma. Otol. Neurotol. 2007, 28, 1076–1082. [Google Scholar] [CrossRef]
- Kameyama, S.; Tanaka, R.; Honda, Y.; Hasegawa, A.; Yamazaki, H.; Kawaguchi, T. The Long-Term Growth Rate of Residual Acoustic Neurinomas. Acta Neurochir. 1994, 129, 127–130. [Google Scholar] [CrossRef]
- Kemink, J.L.; Langman, A.W.; Niparko, J.K.; Graham, M.D. Operative Management of Acoustic Neuromas: The Priority of Neurologic Function over Complete Resection. Otolaryngol. Head Neck Surg. 1991, 104, 96–99. [Google Scholar] [CrossRef]
- Park, C.K.; Jung, H.W.; Kim, J.E.; Son, Y.J.; Paek, S.H.; Kim, D.G. Therapeutic Strategy for Large Vestibular Schwannomas. J. Neurooncol. 2006, 77, 167–171. [Google Scholar] [CrossRef] [PubMed]
- Seol, H.J.; Kim, C.H.; Park, C.K.; Kim, C.H.; Kim, D.G.; Chung, Y.S.; Jung, H.W. Optimal Extent of Resection in Vestibular Schwannoma Surgery: Relationship to Recurrence and Facial Nerve Preservation. Neurol. Med. Chir. 2006, 46, 176–180. [Google Scholar] [CrossRef]
- Pruijn, I.M.J.; Kievit, W.; Hentschel, M.A.; Mulder, J.J.S.; Kunst, H.P.M. What Determines Quality of Life in Patients with Vestibular Schwannoma? Clin. Otolaryngol. 2021, 46, 412–420. [Google Scholar] [CrossRef]
- Santa Maria, C.; Santa Maria, P.L.; Bulsara, V.; Jayawardena, J.; Caldow, J.D.; Png, L.H.; Atlas, M.D. Long-Term Quality of Life in Patients with Vestibular Schwannoma Managed with Microsurgery. J. Laryngol. Otol. 2019, 133, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Marouf, R.; Noudel, R.; Roche, P.H. Facial Nerve Outcome after Microsurgical Resection of Vestibular Schwannoma. Prog. Neurol. Surg. 2008, 21, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Samii, M.; Gerganov, V.; Samii, A. Improved Preservation of Hearing and Facial Nerve Function in Vestibular Schwannoma Surgery via the Retrosigmoid Approach in a Series of 200 Patients. J. Neurosurg. 2006, 105, 527–535. [Google Scholar] [CrossRef]
- Brokinkel, B.; Sauerland, C.; Holling, M.; Ewelt, C.; Horstmann, G.; van Eck, A.T.C.J.; Stummer, W. Gamma Knife Radiosurgery Following Subtotal Resection of Vestibular Schwannoma. J. Clin. Neurosci. 2014, 21, 2077–2082. [Google Scholar] [CrossRef]
- Gurgel, R.K.; Theodosopoulos, P.V.; Jackler, R.K. Subtotal/near-Total Treatment of Vestibular Schwannomas. Curr. Opin. Otolaryngol. Head Neck Surg. 2012, 20, 380–384. [Google Scholar] [CrossRef]
- Jeltema, H.R.; Bakker, N.A.; Bijl, H.P.; Wagemakers, M.; Metzemaekers, J.D.M.; van Dijk, J.M.C. Near Total Extirpation of Vestibular Schwannoma with Salvage Radiosurgery. Laryngoscope 2015, 125, 1703–1707. [Google Scholar] [CrossRef]
- Chen, Z.; Prasad, S.C.; di Lella, F.; Medina, M.; Piccirillo, E.; Taibah, A.; Russo, A.; Yin, S.; Sanna, M. The Behavior of Residual Tumors and Facial Nerve Outcomes after Incomplete Excision of Vestibular Schwannomas. J. Neurosurg. 2014, 120, 1278–1287. [Google Scholar] [CrossRef]
- El-Kashlan, H.K.; Zeitoun, H.; Alexander Arts, H.; Hoff, J.T.; Telian, S.A. Recurrence of Acoustic Neuroma after Incomplete Resection. Am. J. Otol. 2000, 21, 389–392. [Google Scholar] [CrossRef]
- Godefroy, W.P.; Hastan, D.; van der Mey, A.G.L. Translabyrinthine Surgery for Disabling Vertigo in Vestibular Schwannoma Patients. Clin. Otolaryngol. 2007, 32, 167–172. [Google Scholar] [CrossRef] [PubMed]
- Lownie, S.P.; Drake, C.G. Radical Intracapsular Removal of Acoustic Neurinomas. Long-Term Follow-up Review of 11 Patients. J. Neurosurg. 1991, 74, 422–425. [Google Scholar] [CrossRef] [PubMed]
- Ohta, S.; Yokoyama, T.; Nishizawa, S.; Uemura, K. Regrowth of the Residual Tumour after Acoustic Neurinoma Surgery. Br. J. Neurosurg. 1998, 12, 419–422. [Google Scholar] [CrossRef] [PubMed]
- Pollock, B.E.; Lunsford, L.D.; Flickinger, J.C.; Clyde, B.L.; Kondziolka, D. Vestibular Schwannoma Management. Part I. Failed Microsurgery and the Role of Delayed Stereotactic Radiosurgery. J. Neurosurg. 1998, 89, 944–948. [Google Scholar] [CrossRef] [PubMed]
- Ramina, R.; Neto, M.C.; Bordignon, K.C.; Mattei, T.; Clemente, R.; Pires Aguiar, P.H. Treatment of Large and Giant Residual and Recurrent Vestibular Schwannomas. Skull Base 2007, 17, 109–118. [Google Scholar] [CrossRef]
- Sanna, M.; Falcioni, M.; Taibah, A.; de Donato, G.; Russo, A.; Piccirillo, E. Treatment of Residual Vestibular Schwannoma. Otol. Neurotol. 2002, 23, 980–987. [Google Scholar] [CrossRef]
- Rosenberg, S.I. Natural History of Acoustic Neuromas. Laryngoscope 2000, 110, 497–508. [Google Scholar] [CrossRef]
- Syed, M.I.; Wolf, A.; Ilan, O.; Hughes, C.O.; Chung, J.; Tymianski, M.; Pothier, D.D.; Rutka, J.A. The Behaviour of Residual Tumour after the Intentional Incomplete Excision of a Vestibular Schwannoma: Is It Such a Bad Thing to Leave Some Behind? Clin. Otolaryngol. 2017, 42, 92–97. [Google Scholar] [CrossRef]
- Strickland, B.A.; Ravina, K.; Rennert, R.C.; Jackanich, A.; Aaron, K.; Bakhsheshian, J.; Russin, J.J.; Friedman, R.A.; Giannotta, S.L. Intentional Subtotal Resection of Vestibular Schwannoma: A Reexamination. J. Neurol. Surg. B Skull Base 2020, 81, 136–141. [Google Scholar] [CrossRef]
- Starnoni, D.; Daniel, R.T.; Tuleasca, C.; George, M.; Levivier, M.; Messerer, M. Systematic Review and Meta-Analysis of the Technique of Subtotal Resection and Stereotactic Radiosurgery for Large Vestibular Schwannomas: A “Nerve-Centered” Approach. Neurosurg. Focus 2018, 44, E4. [Google Scholar] [CrossRef] [PubMed]
- Iwai, Y.; Yamanaka, K.; Ishiguro, T. Surgery Combined with Radiosurgery of Large Acoustic Neuromas. Surg. Neurol. 2003, 59, 283–289. [Google Scholar] [CrossRef]
- Iwai, Y.; Ishibashi, K.; Watanabe, Y.; Uemura, G.; Yamanaka, K. Functional Preservation After Planned Partial Resection Followed by Gamma Knife Radiosurgery for Large Vestibular Schwannomas. World Neurosurg. 2015, 84, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Fuentes, S.; Arkha, Y.; Pech-Gourg, G.; Grisoli, F.; Dufour, H.; Régis, J. Management of Large Vestibular Schwannomas by Combined Surgical Resection and Gamma Knife Radiosurgery. Prog. Neurol. Surg. 2008, 21, 79–82. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.Y.; Kim, D.G.; Chung, H.T.; Park, S.H.; Paek, S.H.; Jung, H.W. Evaluation of Tumour Response after Gamma Knife Radiosurgery for Residual Vestibular Schwannomas Based on MRI Morphological Features. J. Neurol. Neurosurg. Psychiatry 2008, 79, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Van de Langenberg, R.; Hanssens, P.E.J.; van Overbeeke, J.J.; Verheul, J.B.; Nelemans, P.J.; de Bondt, B.J.; Stokroos, R.J. Management of Large Vestibular Schwannoma. Part I. Planned Subtotal Resection Followed by Gamma Knife Surgery: Radiological and Clinical Aspects. J. Neurosurg. 2011, 115, 875–884. [Google Scholar] [CrossRef] [PubMed]
- Pan, H.C.; Sheehan, J.; Sheu, M.L.; Chiu, W.T.; Yang, D.Y. Intracapsular Decompression or Radical Resection Followed by Gamma Knife Surgery for Patients Harboring a Large Vestibular Schwannoma. J. Neurosurg. 2012, 117, 69–77. [Google Scholar] [CrossRef]
- Daniel, R.T.; Tuleasca, C.; George, M.; Pralong, E.; Schiappacasse, L.; Zeverino, M.; Maire, R.; Levivier, M. Preserving Normal Facial Nerve Function and Improving Hearing Outcome in Large Vestibular Schwannomas with a Combined Approach: Planned Subtotal Resection Followed by Gamma Knife Radiosurgery. Acta Neurochir. 2017, 159, 1197–1211. [Google Scholar] [CrossRef]
- Radwan, H.; Eisenberg, M.B.; Sandberg Knisely, J.P.; Ghaly, M.M.; Schulder, M. Outcomes in Patients with Vestibular Schwannoma after Subtotal Resection and Adjuvant Radiosurgery. Stereotact. Funct. Neurosurg. 2016, 94, 216–224. [Google Scholar] [CrossRef]
- Borsetto, D.; Gair, J.; Kenyon, O.; Das, T.; Donnelly, N.; Axon, P.; MacFarlane, R.; Mannion, R.; Scoffings, D.; Bance, M.; et al. When Should We Stop Scanning Older Patients with Vestibular Schwannomas? J. Neurol. Surg. B Skull Base 2019, 80, 333–337. [Google Scholar] [CrossRef]
- Ostler, B.; Killeen, D.E.; Reisch, J.; Barnett, S.; Kutz, J.W.; Isaacson, B.; Hunter, J.B. Patient Demographics Influencing Vestibular Schwannoma Size and Initial Management Plans. World Neurosurg. 2020, 136, e440–e446. [Google Scholar] [CrossRef] [PubMed]
- Krengli, M.; Zanoletti, E.; Deantonio, L. Radiation Therapy in Acoustic Neuroma. In Radiation Oncology; Wenz, F., Ed.; Springer: Cham, Switzerland, 2018; pp. 1–16. [Google Scholar] [CrossRef]
- Zanoletti, E.; Mazzoni, A.; Martini, A.; Abbritti, R.V.; Albertini, R.; Alexandre, E.; Baro, V.; Bartolini, S.; Bernardeschi, D.; Bivona, R.; et al. Surgery of the Lateral Skull Base: A 50-Year Endeavour. Acta Otorhinolaryngol. Ital. 2019, 39, S1–S146. [Google Scholar] [CrossRef] [PubMed]
- Gulya, A.J.; Minor, L.; Poe, D. Glasscock-Shambaugh Surgery of the Ear; PMPH-USA: Shelton, CT, USA, 2010; p. 801. [Google Scholar]
- Nasrollahi, T.S.; Shahrestani, S.; Borrelli, M.; Raskin, J.; Hopp, M.L.; Wu, A.W.; Miller, M.E.; Wong, Y.T. Analysis of Readmissions Data among Frail and Non-Frail Patients Presenting for Acoustic Neuroma. J. Clin. Neurosci. 2022, 99, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Luryi, A.L.; Babu, S.; Bojrab, D.I.; Kveton, J.F.; Schutt, C.A. Surgical Outcomes After Conservative Resection of Vestibular Schwannoma in the Elderly. Otol. Neurotol. 2021, 42, e1358–e1361. [Google Scholar] [CrossRef]
- Helal, A.; Graffeo, C.S.; Perry, A.; van Abel, K.M.; Carlson, M.L.; Neff, B.A.; Driscoll, C.L.W.; Link, M.J. Differential Impact of Advanced Age on Clinical Outcomes After Vestibular Schwannoma Resection in the Very Elderly: Cohort Study. Oper. Neurosurg. 2021, 21, 104–110. [Google Scholar] [CrossRef]
- Andersen, J.F.; Nilsen, K.S.; Vassbotn, F.S.; Møller, P.; Myrseth, E.; Lund-Johansen, M.; Goplen, F.K. Predictors of Vertigo in Patients with Untreated Vestibular Schwannoma. Otol. Neurotol. 2015, 36, 647–652. [Google Scholar] [CrossRef]
- Kentala, E.; Pyykkö, I. Clinical Picture of Vestibular Schwannoma. Auris Nasus Larynx 2001, 28, 15–22. [Google Scholar] [CrossRef]
- Myrseth, E.; Møller, P.; Wentzel-Larsen, T.; Goplen, F.; Lund-Johansen, M. Untreated Vestibular Schwannoma: Vertigo Is a Powerful Predictor for Health-Related Quality of Life. Neurosurgery 2006, 59, 67–76. [Google Scholar] [CrossRef]
- Kanzaki, J.; Tos, M.; Sanna, M.; Moffat, D.A. New and Modified Reporting Systems from the Consensus Meeting on Systems for Reporting Results in Vestibular Schwannoma. Otol. Neurotol. 2003, 24, 642–648. [Google Scholar] [CrossRef]
- Humphriss, R.L.; Baguley, D.M.; Axon, P.R.; Moffat, D.A. Preoperative Audiovestibular Handicap in Patients with Vestibular Schwannoma. Skull Base 2006, 16, 193–200. [Google Scholar] [CrossRef]
- Breivik, C.N.; Varughese, J.K.; Wentzel-Larsen, T.; Vassbotn, F.; Lund-Johansen, M. Conservative Management of Vestibular Schwannoma--a Prospective Cohort Study: Treatment, Symptoms, and Quality of Life. Neurosurgery 2012, 70, 1072–1080. [Google Scholar] [CrossRef] [PubMed]
- Nilsen, K.S.; Lund-Johansen, M.; Nordahl, S.H.G.; Finnkirk, M.; Goplen, F.K. Long-Term Effects of Conservative Management of Vestibular Schwannoma on Dizziness, Balance, and Caloric Function. Otolaryngol. Head Neck Surg. 2019, 161, 846–851. [Google Scholar] [CrossRef]
- Kim, G.; Hullar, T.E.; Seo, J.H. Comparison of Balance Outcomes According to Treatment Modality of Vestibular Schwannoma. Laryngoscope 2020, 130, 178–189. [Google Scholar] [CrossRef]
- Ojha, S.; Clamp, P.J. A Systematic Review of Interventions for Balance Dysfunction in Patients With Vestibular Schwannoma. Otol. Neurotol. 2020, 41, e295–e303. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Jia, H.; Li, G.; Huang, M.; Zhu, W.; Wang, Z.; Li, Y.; Wu, H. Intratympanic Gentamicin for Small Vestibular Schwannomas With Intractable Vertigo. Otol. Neurotol. 2018, 39, E699–E703. [Google Scholar] [CrossRef] [PubMed]
- Magnusson, M.; Kahlon, B.; Karlberg, M.; Lindberg, S.; Siesjö, P. Preoperative Vestibular Ablation with Gentamicin and Vestibular “prehab” Enhance Postoperative Recovery after Surgery for Pontine Angle Tumours--First Report. Acta Otolaryngol. 2007, 127, 1236–1240. [Google Scholar] [CrossRef]
- Peris-Celda, M.; Graffeo, C.S.; Perry, A.; Kerezoudis, P.; Tombers, N.M.; Carlson, M.L.; Link, M.J. Main Symptom That Led to Medical Evaluation and Diagnosis of Vestibular Schwannoma and Patient-Reported Tumor Size: Cross-Sectional Study in 1304 Patients. J. Neurol. Surg. B Skull Base 2019, 80, 316–322. [Google Scholar] [CrossRef]
- Naros, G.; Sandritter, J.; Liebsch, M.; Ofori, A.; Rizk, A.R.; del Moro, G.; Ebner, F.; Tatagiba, M. Predictors of Preoperative Tinnitus in Unilateral Sporadic Vestibular Schwannoma. Front. Neurol. 2017, 8, 378. [Google Scholar] [CrossRef]
- Cao, W.; Hou, Z.; Wang, F.; Jiang, Q.; Shen, W.; Yang, S. Larger Tumor Size and Female Gender Suggest Better Tinnitus Prognosis after Surgical Treatment in Vestibular Schwannoma Patients with Tinnitus. Acta Otolaryngol. 2020, 140, 373–377. [Google Scholar] [CrossRef]
- Kojima, T.; Oishi, N.; Nishiyama, T.; Ogawa, K. Severity of Tinnitus Distress Negatively Impacts Quality of Life in Patients with Vestibular Schwannoma and Mimics Primary Tinnitus. Front. Neurol. 2019, 10, 389. [Google Scholar] [CrossRef]
- Van Gompel, J.J.; Patel, J.; Danner, C.; Zhang, A.N.; Youssef, A.A.S.; van Loveren, H.R.; Agazzi, S. Acoustic Neuroma Observation Associated with an Increase in Symptomatic Tinnitus: Results of the 2007-2008 Acoustic Neuroma Association Survey. J. Neurosurg. 2013, 119, 864–868. [Google Scholar] [CrossRef] [PubMed]
- Gosselin, É.; Maniakas, A.; Saliba, I. Meta-Analysis on the Clinical Outcomes in Patients with Intralabyrinthine Schwannomas: Conservative Management VS Microsurgery. Eur. Arch. Otorhinolaryngol. 2016, 273, 1357–1367. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.J.; Feng, Y.M.; Wang, H.; Wu, Y.Q.; Shi, H.B.; Chen, Z.N.; Yin, S.K. Changes in Tinnitus after Vestibular Schwannoma Surgery. Sci. Rep. 2019, 9, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Chovanec, M.; Zvěřina, E.; Profant, O.; Balogová, Z.; Kluh, J.; Syka, J.; Lisý, J.; Merunka, I.; Skřivan, J.; Betka, J. Does Attempt at Hearing Preservation Microsurgery of Vestibular Schwannoma Affect Postoperative Tinnitus? BioMed Res. Int. 2015, 2015, 783169. [Google Scholar] [CrossRef] [PubMed]
- Kohno, M.; Shinogami, M.; Yoneyama, H.; Nagata, O.; Sora, S.; Sato, H. Prognosis of Tinnitus after Acoustic Neuroma Surgery--Surgical Management of Postoperative Tinnitus. World Neurosurg. 2014, 81, 357–367. [Google Scholar] [CrossRef]
- Zhang, C.; Wang, F.; Cao, W.; Ma, X.; Chen, J.; Shen, W.; Yang, S. Identification of Factors Associated with Tinnitus Outcomes Following the Microsurgical Treatment of Vestibular Schwannoma Patients. Acta Otolaryngol. 2021, 141, 334–339. [Google Scholar] [CrossRef]
- Kitamura, M.; Oishi, N.; Suzuki, N.; Kojima, T.; Nishiyama, T.; Noguchi, M.; Hosoya, M.; Ogawa, K. Management of Tinnitus in Patients with Vestibular Schwannoma Who Underwent Surgical Resection. Eur. Arch. Otorhinolaryngol. 2021, 278, 4243–4249. [Google Scholar] [CrossRef]
- Bell, J.R.; Anderson-Kim, S.J.; Low, C.; Leonetti, J.P. The Persistence of Tinnitus after Acoustic Neuroma Surgery. Otolaryngol. Head Neck Surg. 2016, 155, 317–323. [Google Scholar] [CrossRef]
- Stangerup, S.E.; Caye-Thomasen, P. Epidemiology and Natural History of Vestibular Schwannomas. Otolaryngol. Clin. N. Am. 2012, 45, 257–268. [Google Scholar] [CrossRef]
- Coughlin, A.R.; Willman, T.J.; Gubbels, S.P. Systematic Review of Hearing Preservation After Radiotherapy for Vestibular Schwannoma. Otol. Neurotol. 2018, 39, 273–283. [Google Scholar] [CrossRef]
- Khandalavala, K.R.; Saba, E.S.; Kocharyan, A.; Daher, G.S.; Lohse, C.M.; Marinelli, J.P.; Carlson, M.L. Hearing Preservation in Observed Sporadic Vestibular Schwannoma. Otol. Neurotol. 2022, 43, 604–610. [Google Scholar] [CrossRef] [PubMed]
- Huo, Z.; Chen, J.; Wang, Z.; Zhang, Z.; Wu, H. Prognostic Factors of Long-Term Hearing Preservation in Small and Medium-Sized Vestibular Schwannomas After Microsurgery. Otol. Neurotol. 2019, 40, 957–964. [Google Scholar] [CrossRef] [PubMed]
- Saliba, J.; Friedman, R.A.; Cueva, R.A. Hearing Preservation in Vestibular Schwannoma Surgery. J. Neurol. Surg. B 2019, 80, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Kutz, J.W., Jr.; Scoresby, T.; Isaacson, B.; Mickey, B.E.; Madden, C.J.; Barnett, S.L.; Coimbra, C.; Hynan, L.S.; Roland, P.S. Hearing Preservation Using the Middle Fossa Approach for the Treatment of Vestibular Schwannoma. Neurosurgery 2012, 70, 334–341. [Google Scholar] [CrossRef]
- Nguyen, Q.T.; Wu, A.P.; Mastrodimos, B.J.; Cueva, R.A. Impact of Fundal Extension on Hearing after Surgery for Vestibular Schwannomas. Otol. Neurotol. 2012, 33, 455–458. [Google Scholar] [CrossRef]
- Wanibuchi, M.; Fukushima, T.; McElveen, J.T.; Friedman, A.H. Hearing Preservation in Surgery for Large Vestibular Schwannomas. J. Neurosurg. 2009, 111, 845–854. [Google Scholar] [CrossRef]
- Tringali, S.; Ferber-Viart, C.; Fuchsmann, C.; Buiret, G.; Zaouche, S.; Dubreuil, C. Hearing Preservation in Retrosigmoid Approach of Small Vestibular Schwannomas: Prognostic Value of the Degree of Internal Auditory Canal Filling. Otol. Neurotol. 2010, 31, 1469–1472. [Google Scholar] [CrossRef]
- Matsushima, K.; Kohno, M.; Nakajima, N. Hearing Preservation in Vestibular Schwannoma Surgery via Retrosigmoid Transmeatal Approach. Acta Neurochir. 2019, 161, 2265–2269. [Google Scholar] [CrossRef]
- Woolf, D.K.; Williams, M.; Goh, C.L.; Henderson, D.R.; Menashy, R.V.; Simpson, N.; Mastroianni, B.; Collis, C.H. Fractionated Stereotactic Radiotherapy for Acoustic Neuromas: Long-Term Outcomes. Clin. Oncol. 2013, 25, 734–738. [Google Scholar] [CrossRef]
- Combs, S.E.; Engelhard, C.; Kopp, C.; Wiedenmann, N.; Schramm, O.; Prokic, V.; Debus, J.; Molls, M.; Grosu, A.L. Long-Term Outcome after Highly Advanced Single-Dose or Fractionated Radiotherapy in Patients with Vestibular Schwannomas—Pooled Results from 3 Large German Centers. Radiother. Oncol. 2015, 114, 378–383. [Google Scholar] [CrossRef]
- Persson, O.; Bartek, J.; Shalom, N.B.; Wangerid, T.; Jakola, A.S.; Förander, P. Stereotactic Radiosurgery VS Fractionated Radiotherapy for Tumor Control in Vestibular Schwannoma Patients: A Systematic Review. Acta Neurochir. 2017, 159, 1013–1021. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sergi, B.; Settimi, S.; Federici, G.; Galloni, C.; Cantaffa, C.; De Corso, E.; Lucidi, D. Factors Influencing Personalized Management of Vestibular Schwannoma: A Systematic Review. J. Pers. Med. 2022, 12, 1616. https://doi.org/10.3390/jpm12101616
Sergi B, Settimi S, Federici G, Galloni C, Cantaffa C, De Corso E, Lucidi D. Factors Influencing Personalized Management of Vestibular Schwannoma: A Systematic Review. Journal of Personalized Medicine. 2022; 12(10):1616. https://doi.org/10.3390/jpm12101616
Chicago/Turabian StyleSergi, Bruno, Stefano Settimi, Gaia Federici, Costanza Galloni, Carla Cantaffa, Eugenio De Corso, and Daniela Lucidi. 2022. "Factors Influencing Personalized Management of Vestibular Schwannoma: A Systematic Review" Journal of Personalized Medicine 12, no. 10: 1616. https://doi.org/10.3390/jpm12101616
APA StyleSergi, B., Settimi, S., Federici, G., Galloni, C., Cantaffa, C., De Corso, E., & Lucidi, D. (2022). Factors Influencing Personalized Management of Vestibular Schwannoma: A Systematic Review. Journal of Personalized Medicine, 12(10), 1616. https://doi.org/10.3390/jpm12101616