
Oral and Periodontal Implications of Hepatitis Type B and D. Current State of Knowledge and Future Perspectives

 ,
,  ,
,  ,
,  , ,
, ,
Abstract
1. Introduction
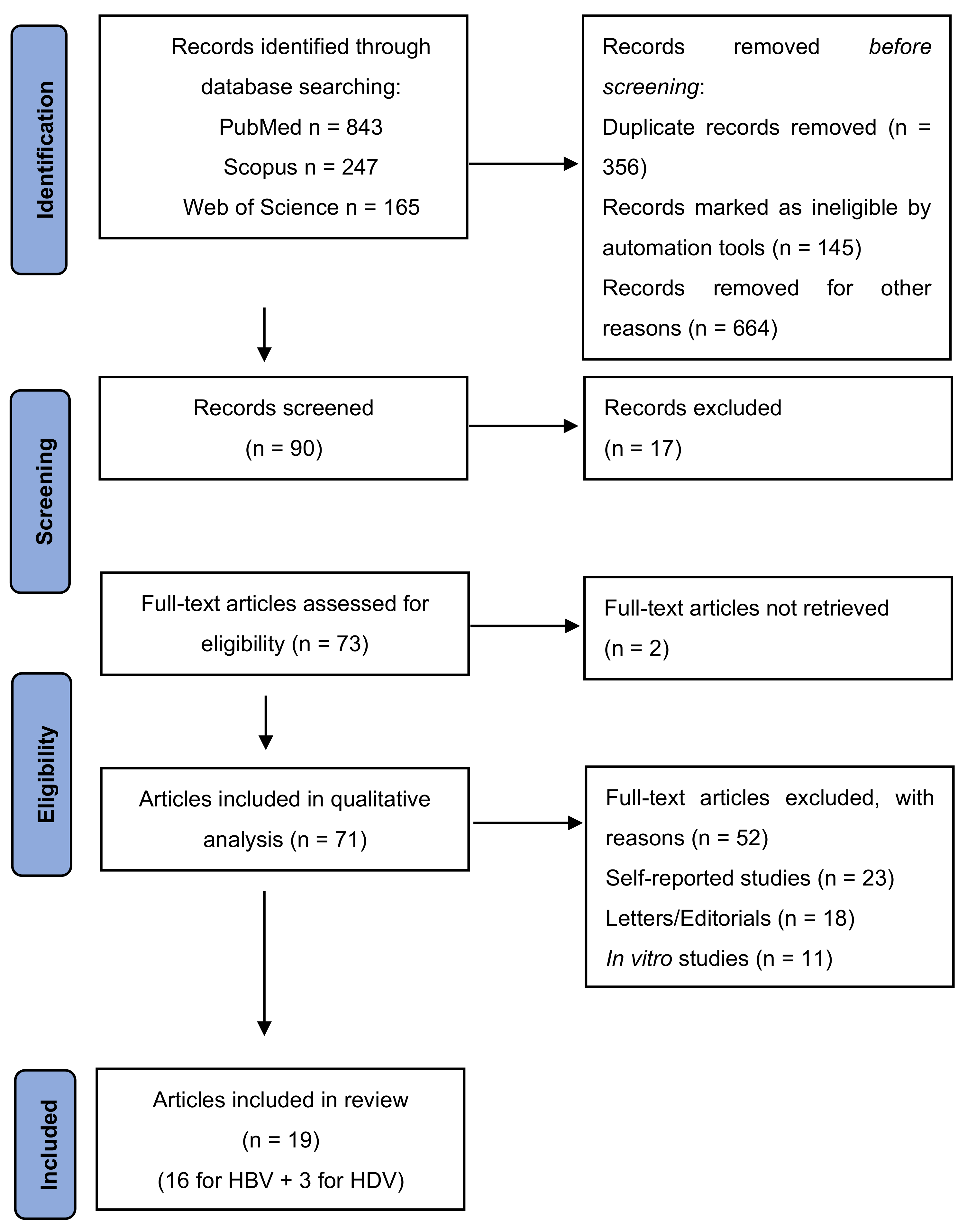
2. Materials and Methods
2.1. PICO Question
2.2. Search Strategy
2.3. Exclusion Criteria of the Studies
2.4. Information Extraction and Review Structuring
3. Results
3.1. HBV Infection and Oral Implications
3.2. HDV Infection and Oral Implications
4. Future Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nomura, Y.; Okada, A.; Hanada, N. Future Prospective of Oral Microbiome Research. Appl. Sci. 2022, 12, 55. [Google Scholar] [CrossRef]
- Schulz, S.; Stein, J.M.; Schumacher, A.; Kupietz, D.; Yekta-Michael, S.S.; Schittenhelm, F.; Conrads, G.; Schaller, H.-G.; Reichert, S. Nonsurgical Periodontal Treatment Options and Their Impact on Subgingival Microbiota. J. Clin. Med. 2022, 11, 1187. [Google Scholar] [CrossRef] [PubMed]
- Mombelli, A. Microbial colonization of the periodontal pocket and its significance for periodontal therapy. Periodontology 2000 2017, 76, 85–96. [Google Scholar] [CrossRef]
- Fiorillo, L.; Cervino, G.; Laino, L.; D’Amico, C.; Mauceri, R.; Tozum, T.F.; Gaeta, M.; Cicciù, M. Porphyromonas gingivalis, Periodontal and Systemic Implications: A Systematic Review. Dent. J. 2019, 7, 114. [Google Scholar] [CrossRef] [PubMed]
- Cecoro, G.; Annunziata, M.; Iuorio, M.T.; Nastri, L.; Guida, L. Periodontitis, Low-Grade Inflammation and Systemic Health: A Scoping Review. Medicina 2020, 56, 272. [Google Scholar] [CrossRef] [PubMed]
- Slots, J. Periodontitis: Facts, fallacies and the future. Periodontology 2000 2017, 75, 7–23. [Google Scholar] [CrossRef] [PubMed]
- Guarnieri, R.; Zanza, A.; D’Angelo, M.; Di Nardo, D.; Del Giudice, A.; Mazzoni, A.; Reda, R.; Testarelli, L. Correlation between Peri-Implant Marginal Bone Loss Progression and Peri-Implant Sulcular Fluid Levels of Metalloproteinase-8. J. Pers. Med. 2022, 12, 58. [Google Scholar] [CrossRef] [PubMed]
- Bosshardt, D. The periodontal pocket: Pathogenesis, histopathology and consequences. Periodontology 2000 2017, 76, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, Y.; Zhang, B.; Kato, S. Lymphatic networks in the periodontal tissue and dental pulp as revealed by histochemical study. Micros. Res. Tech. 2002, 56, 50–59. [Google Scholar] [CrossRef] [PubMed]
- Beck, J.; Papapanou, P.; Philips, K.; Offenbacher, S. Periodontal Medicine: 100 Years of Progress. J. Dent. Res. 2019, 98, 1053–1062. [Google Scholar] [CrossRef] [PubMed]
- Williams, R.; Offenbacher, S. Periodontal medicine: The emergence of a new branch of periodontology. Periodontology 2000 2000, 23, 9–12. [Google Scholar] [CrossRef]
- Battancs, E.; Gheorghita, D.; Nyiraty, S.; Lengyel, C.; Eördegh, G.; Baráth, Z.; Várkonyi, T.; Antal, M. Periodontal Disease in Diabetes Mellitus: A Case–Control Study in Smokers and Non-Smokers. Diabetes Ther. 2020, 11, 2715–2728. [Google Scholar] [CrossRef] [PubMed]
- Antal, M.; Battancs, E.; Bocskai, M.; Braunitzer, G.; Kovács, L. An observation on the severity of periodontal disease in past cigarette smokers suffering from rheumatoid arthritis- evidence for a long-term effect of cigarette smoke exposure? BMC Oral Health 2018, 18, 82. [Google Scholar] [CrossRef] [PubMed]
- Antal, M.; Braunitzer, G.; Mattheos, N.; Gyulai, R.; Nagy, K. Smoking as a Permissive Factor of Periodontal Disease in Psoriasis. PLoS ONE 2014, 9, e92333. [Google Scholar] [CrossRef] [PubMed]
- Caton, J.; Armitage, G.; Berglundh, T.; Chapple, I.; Jepsen, S.; Kornman, K.; Mealey, B.; Papapanou, P.; Sanz, M.; Tonetti, M. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Periodontol. 2018, 89, S1–S8. [Google Scholar] [CrossRef] [PubMed]
- Tu, T.; Block, J.M.; Wang, S.; Cohen, C.; Douglas, M.W. The Lived Experience of Chronic Hepatitis B: A Broader View of Its Impacts and Why We Need a Cure. Viruses 2020, 12, 515. [Google Scholar] [CrossRef] [PubMed]
- Chang, M. Hepatitis B virus infection. Semin. Fetal Neonatal Med. 2007, 12, 160–167. [Google Scholar] [CrossRef]
- Guvenir, M.; Arikan, A. Hepatitis B Virus: From Diagnosis to Treatment. Pol. J. Microbiol. 2020, 69, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Herrscher, C.; Roingeard, P.; Blanchard, E. Hepatitis B Virus Entry into Cells. Cells 2020, 9, 1486. [Google Scholar] [CrossRef]
- Nicolini, L.A.; Orsi, A.; Tatarelli, P.; Viscoli, C.; Icardi, G.; Sticchi, L. A Global View to HBV Chronic Infection: Evolving Strategies for Diagnosis, Treatment and Prevention in Immunocompetent Individuals. Int. J. Environ. Res. Public Health 2019, 16, 3307. [Google Scholar] [CrossRef] [PubMed]
- Noverati, N.; Bashir-Hamidu, R.; Halegoua-DeMarzio, D.; Hann, H.-W. Hepatitis B Virus-Associated Hepatocellular Carcinoma and Chronic Stress. Int. J. Mol. Sci. 2022, 23, 3917. [Google Scholar] [CrossRef]
- Rizzo, G.E.M.; Cabibbo, G.; Craxì, A. Hepatitis B Virus-Associated Hepatocellular Carcinoma. Viruses 2022, 14, 986. [Google Scholar] [CrossRef]
- Rizzetto, M.; Stroffolini, T. Forty-Five Years after the Discovery of the Hepatitis D Virus: Where Do We Stand? Viruses 2021, 13, 555. [Google Scholar] [CrossRef]
- Rizzetto, M. Hepatitis D Virus: Introduction and Epidemiology. Cold Spring Harb. Perspect. Med. 2015, 5, a021576. [Google Scholar] [CrossRef]
- Brillanti, S. Management of Delta Hepatitis 45 Years after the Discovery of HDV. J. Clin. Med. 2022, 11, 1587. [Google Scholar] [CrossRef]
- Taylor, J.M. Infection by Hepatitis Delta Virus. Viruses 2020, 12, 648. [Google Scholar] [CrossRef]
- Miao, Z.; Zhang, S.; Ou, X.; Li, S.; Ma, Z.; Wang, W.; Peppelenbosch, M.; Liu, J.; Pan, Q. Estimating the Global Prevalence, Disease Progression, and Clinical Outcome of Hepatitis Delta Virus Infection. J. Infect. Dis. 2019, 221, 1677–1687. [Google Scholar] [CrossRef]
- Gheorghe, D.N.; Camen, A.; Popescu, D.M.; Sincar, C.; Pitru, A.; Ionele, C.M.; Nicolae, F.M.; Danilescu, C.M.; Roman, A.; Florescu, C. Periodontitis, Metabolic and Gastrointestinal Tract Diseases: Current Perspectives on Possible Pathogenic Connections. J. Pers. Med. 2022, 12, 341. [Google Scholar] [CrossRef]
- Surlin, P.; Gheorghe, D.N.; Foia, L.; Surdu, A.; Toma, V.; Solomon, S.M.; Rogoveanu, I. Periodontal Implications of Hepatitis C Infection. In Hepatitis C—From Infection to Cure; IntechOpen: London, UK, 2018. [Google Scholar] [CrossRef]
- Pollock, J.; Andors, L.; Gulumoglu, A.; Ells, P. Direct measurement of hepatitis B viral antibody and antigen markers in gingival crevicular fluid. Oral Surg. Oral Med. Oral Pathol. 1984, 57, 499–503. [Google Scholar] [CrossRef]
- Ben-Aryeh, H.; Ur, I.; Ben-Porath, E. The relationship between antigenaemia and excretion of hepatitis B surface antigen in human whole saliva and in gingival crevicular fluid. Arch. Oral Biol. 1985, 30, 97–99. [Google Scholar] [CrossRef]
- Lamster, I.; Ahlo, J. Analysis of Gingival Crevicular Fluid as Applied to the Diagnosis of Oral and Systemic Diseases. Ann. N. Y. Acad. Sci. 2007, 1098, 216–229. [Google Scholar] [CrossRef]
- Hurlen, B.; Jacobsen, N.; Hurlen, P. Hepatitis B serum markers and oral health in a group of Norwegian male prisoners. Acta Odontol. Scand. 1984, 42, 53–58. [Google Scholar] [CrossRef]
- Kamimura, H.; Watanabe, J.; Sugano, T.; Kohisa, J.; Abe, H.; Kamimura, K.; Tsuchiya, A.; Takamura, M.; Okoshi, S.; Tanabe, Y.; et al. Relationship between detection of hepatitis B virus in saliva and periodontal disease in hepatitis B virus carriers in Japan. J. Infect. Chemother. 2021, 27, 492–496. [Google Scholar] [CrossRef]
- Farghaly, A.G.; Mansour, G.A.; Mahdy, N.H.; Yousri, A. Hepatitis B and C virus infections among patients with gingivitis and adult periodontitis: Seroprevalence and public health importance. J. Egypt. Public Health Assoc. 1998, 73, 707–735. [Google Scholar] [PubMed]
- Sharifian, A.; Ashtari, S.; Hatami, B.; Mohebbi, S.R.; Naderi, N. Risk factors of transmission and natural history of chronic hepatitis B infection in Iranian patients. Gastroenterol. Hepatol. Bed Bench 2019, 12 (Suppl. 1), S149–S155. [Google Scholar]
- Yang, B.; Petrick, J.; Abnet, C.; Graubard, B.; Murphy, G.; Weinstein, S.; Männistö, S.; Albanes, D.; McGlynn, K. Tooth loss and liver cancer incidence in a Finnish cohort. Cancer Causes Control 2017, 28, 899–904. [Google Scholar] [CrossRef]
- Nagao, Y.; Kawahigashi, Y.; Sata, M. Association of Periodontal Diseases and Liver Fibrosis in Patients with HCV and/or HBV infection. Hepat. Mon. 2014, 14, e23264. [Google Scholar] [CrossRef]
- Anand, A.; Pardal, P.; Sachdev, V. Dental caries and periodontal disorders in chronic liver disease. Med. J. Armed Forces India 2001, 57, 26–30. [Google Scholar] [CrossRef]
- Han, D.; Lee, S.; Lee, J.; Kim, Y.; Kim, J. Association between viral hepatitis B infection and halitosis. Acta Odontol. Scand. 2013, 72, 274–282. [Google Scholar] [CrossRef]
- Seshima, F.; Nishina, M.; Namba, T.; Saito, A. Periodontal Regenerative Therapy in Patient with Chronic Periodontitis and Type 2 Diabetes Mellitus: A Case Report. Bull. Tokyo Dent. Coll. 2016, 57, 97–104. [Google Scholar] [CrossRef]
- Ting, M.; Whitaker, E.; Albandar, J. Systematic review of the in vitro effects of statins on oral and perioral microorganisms. Eur. J. Oral. Sci. 2015, 124, 4–10. [Google Scholar] [CrossRef] [PubMed]
- Hong, C.; Scobey, M.; Napenas, J.; Brennan, M.; Lockhart, P. Dental postoperative bleeding complications in patients with suspected and documented liver disease. Oral Dis. 2012, 18, 661–666. [Google Scholar] [CrossRef] [PubMed]
- Azatyan, V.; Yessayan, L.; Shmavonyan, M.; Melik-Andreasyan, G.; Perikhanyan, A.; Porkshenyan, K. Evaluation of IL-2, IL-10, IL-4 and γ-interferon levels in the oral fluids of patients with hepatitis C, B and HIV. J. Infect. Dev. Ctries. 2019, 13, 069S–074S. [Google Scholar] [CrossRef] [PubMed]
- Gharavi, M.; Esmaeili, M. Evaluation of HBs-Ag and anti-HBc levels in serum and saliva of patients with hepatitis B. Med. J. Islam. Repub. Iran 2020, 34, 101. [Google Scholar] [CrossRef]
- Cottone, J. Delta hepatitis: Another concern for dentistry. J. Am. Dent. Assoc. 1986, 112, 47–49. [Google Scholar] [CrossRef]
- Weller, M.; Gardener, M.; Bogus, Z.; Smith, M.; Astorri, E.; Michael, D.; Michael, D.; Zheng, C.; Burbelo, P.; Lai, Z.; et al. Hepatitis Delta Virus Detected in Salivary Glands of Sjögren’s Syndrome Patients and Recapitulates a Sjögren’s Syndrome-Like Phenotype in Vivo. Pathog. Immun. 2016, 1, 12. [Google Scholar] [CrossRef]
- Isaeva, O.; Ilchenko, L.; Kichatova, V.; Potemkin, I.; Amon, E.; Saryglar, A.; Al-Sharabi, S.; Kyuregyan, K.; Mikhailov, M. Detection of markers of hepatitis b and d virus infection in biological media and dried blood spots. Klin. Lab. Diagn. 2020, 65, 95–99. [Google Scholar] [CrossRef]
- Mahboobi, N.; Porter, S.; Karayiannis, P.; Alavian, S. Oral fluid and hepatitis A, B and C: A literature review. J. Oral Pathol. Med. 2011, 41, 505–516. [Google Scholar] [CrossRef]
- Lim, G.; Janu, U.; Chiou, L.-L.; Gandhi, K.K.; Palomo, L.; John, V. Periodontal Health and Systemic Conditions. Dent. J. 2020, 8, 130. [Google Scholar] [CrossRef]
- Gheorghe, L.; Csiki, I.; Iacob, S.; Gheorghe, C.; Trifan, A.; Grigorescu, M.; Motoc, A.; Suceveanu, A.; Curescu, M.; Caruntu, F.; et al. Hepatitis Delta Virus Infection in Romania: Prevalence and Risk Factors. J. Gastrointest. Liver Dis. 2015, 24, 413–421. [Google Scholar] [CrossRef]


{kind=link}
| Reference | Hepatitis Virus Type | Findings |
|---|---|---|
| Polloch et al., 1984 [30] | HBV | HBsAg detection in gingival crevicular samples of infected patients |
| Hurlem et al., 1984 [33] | HBV | HBV infected patients may pose a higher risk of viral transmission in the dental office, via saliva and gingival bleeding |
| Ben-Aryeh et al., 1985 [31] | HBV | HBsAg detection in 90% of gingival crevicular fluid and saliva samples of infected patients |
| Cottone et al., 1986 [46] | HDV | HDV infection is a significant risk in the dental office, recommended HBV vaccination for members of the dental team |
| Farghaly et al., 1998 [35] | HBV | Patients with periodontitis showed a higher percentage of hepatitis exposure and a higher detectability of salivary HBsAg |
| Anand et al., 2001 [39] | HBV/HCV | Periodontal status of patients with nonalcoholic cirrhosis did not differ significantly from that of controls with no liver disease |
| Azatyan et al., 2001 [44] | HBV | Elevated expression of pro-inflammatory interleukins in saliva samples of HBV infected patients |
| Lamster et al., 2007 [32] | HBV/HCV | Gingival crevicular fluid could be an important source for traces of hepatitis viruses’ presence in saliva |
| Hong et al., 2012 [43] | HBV | No episodes of postoperative bleeding in periodontal management of HBV infected patients, independent of INR values |
| Hun Han et al., 2013 [40] | HBV | Direct link between volatile sulphur halitosis, periodontitis, and HBV infection |
| Nagao et al., 2014 [38] | HBV/HCV | Periodontitis might be correlated with viral liver disease |
| Ting et al., 2015 [42] | HBV | Use of statins as an adjunctive periodontal therapy in patients with HBV infection |
| Seshima et al., 2016 [41] | HBV | Effective and stable results of regenerative periodontal therapy in patients with HBV infection |
| Weller et al., 2016 [47] | HDV | Identification of independent HDV in 50% of salivary gland samples from HDV infected patients with primary Sjogren syndrome |
| Yang et al., 2017 [37] | HBV | Increased number of absent teeth is associated with increased risk of primary liver cancer |
| Sharifian et al., 2019 [36] | HBV | Risk factors for HBV infection: positive periodontal and family history |
| Gharavi et al., 2020 [45] | HBV | HBV can be detected in saliva samples of infected patients by means of ELISA method |
| Isaeva et al., 2020 [48] | HDV | No detection of HDV antibodies in saliva samples from patients with HBV and HDV infection |
| Kamimura et al., 2021 [34] | HBV | Strong correlation between occult blood traces in saliva and HBV presence in saliva samples |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gheorghe, D.N.; Bennardo, F.; Popescu, D.M.; Nicolae, F.M.; Ionele, C.M.; Boldeanu, M.V.; Camen, A.; Rogoveanu, I.; Surlin, P. Oral and Periodontal Implications of Hepatitis Type B and D. Current State of Knowledge and Future Perspectives. J. Pers. Med. 2022, 12, 1580. https://doi.org/10.3390/jpm12101580
Gheorghe DN, Bennardo F, Popescu DM, Nicolae FM, Ionele CM, Boldeanu MV, Camen A, Rogoveanu I, Surlin P. Oral and Periodontal Implications of Hepatitis Type B and D. Current State of Knowledge and Future Perspectives. Journal of Personalized Medicine. 2022; 12(10):1580. https://doi.org/10.3390/jpm12101580
Chicago/Turabian StyleGheorghe, Dorin Nicolae, Francesco Bennardo, Dora Maria Popescu, Flavia Mirela Nicolae, Claudiu Marinel Ionele, Mihail Virgil Boldeanu, Adrian Camen, Ion Rogoveanu, and Petra Surlin. 2022. "Oral and Periodontal Implications of Hepatitis Type B and D. Current State of Knowledge and Future Perspectives" Journal of Personalized Medicine 12, no. 10: 1580. https://doi.org/10.3390/jpm12101580
APA StyleGheorghe, D. N., Bennardo, F., Popescu, D. M., Nicolae, F. M., Ionele, C. M., Boldeanu, M. V., Camen, A., Rogoveanu, I., & Surlin, P. (2022). Oral and Periodontal Implications of Hepatitis Type B and D. Current State of Knowledge and Future Perspectives. Journal of Personalized Medicine, 12(10), 1580. https://doi.org/10.3390/jpm12101580