
Skeletal and Dental Morphological Characteristics of the Maxillary in Patients with Impacted Canines Using Cone Beam Computed Tomography: A Retrospective Clinical Study


 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics Approval and Patient Consent
2.2. Sample Size Calculation and Participants
2.3. Study Design
2.4. Measurement Procedure
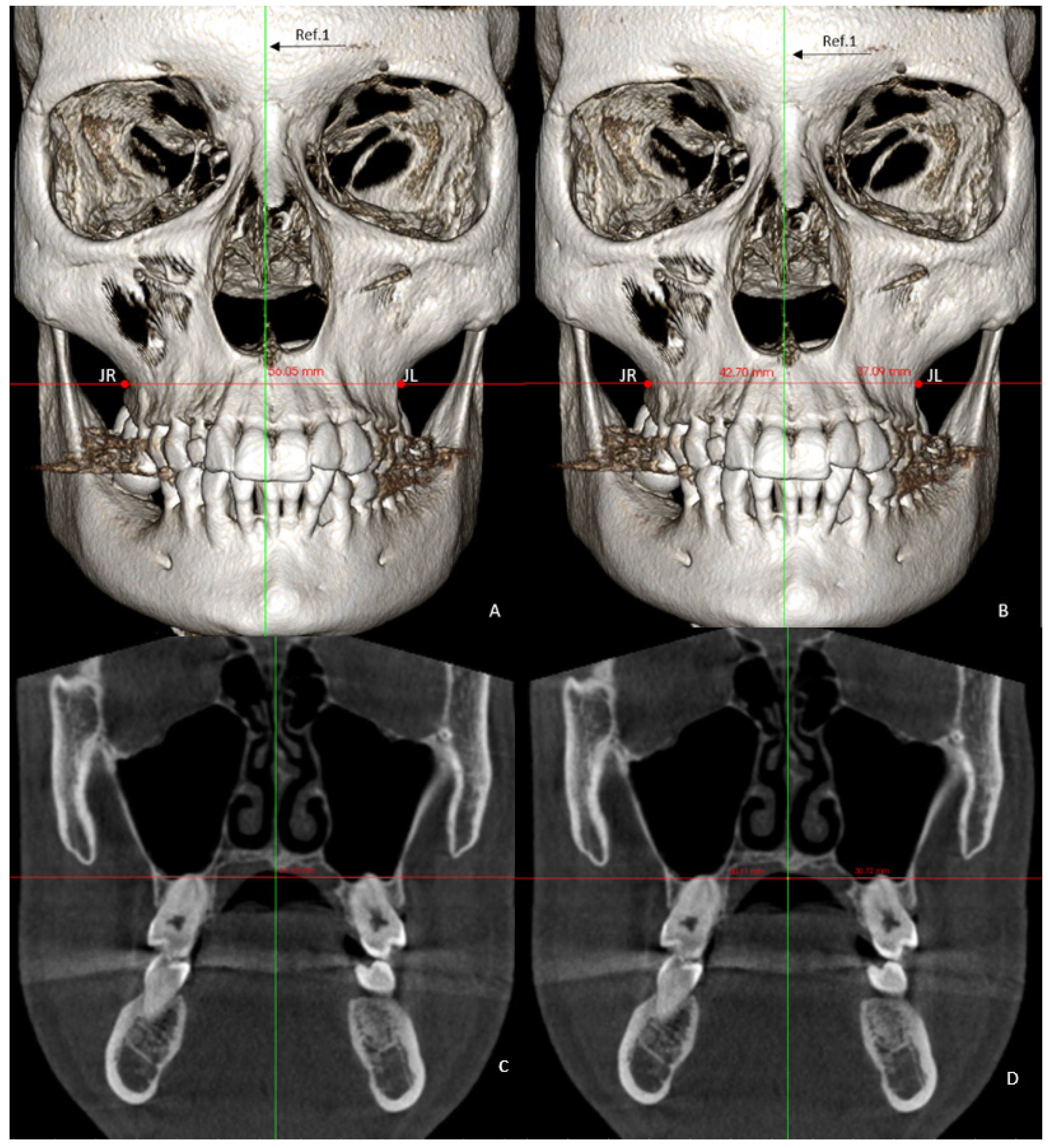
- Basal maxillary width (BMW) in the frontal plane, measured in the JL-JR Ricketts distance in the GC and GI (linear measurement between points on the jugal process at the intersection of the outline of the maxillary tuberosity and the zygomatic buttress) [26] and in the GI-R and GI-L, the JR and JL distance to the median palatal raphe (J-PR) (Figure 1).
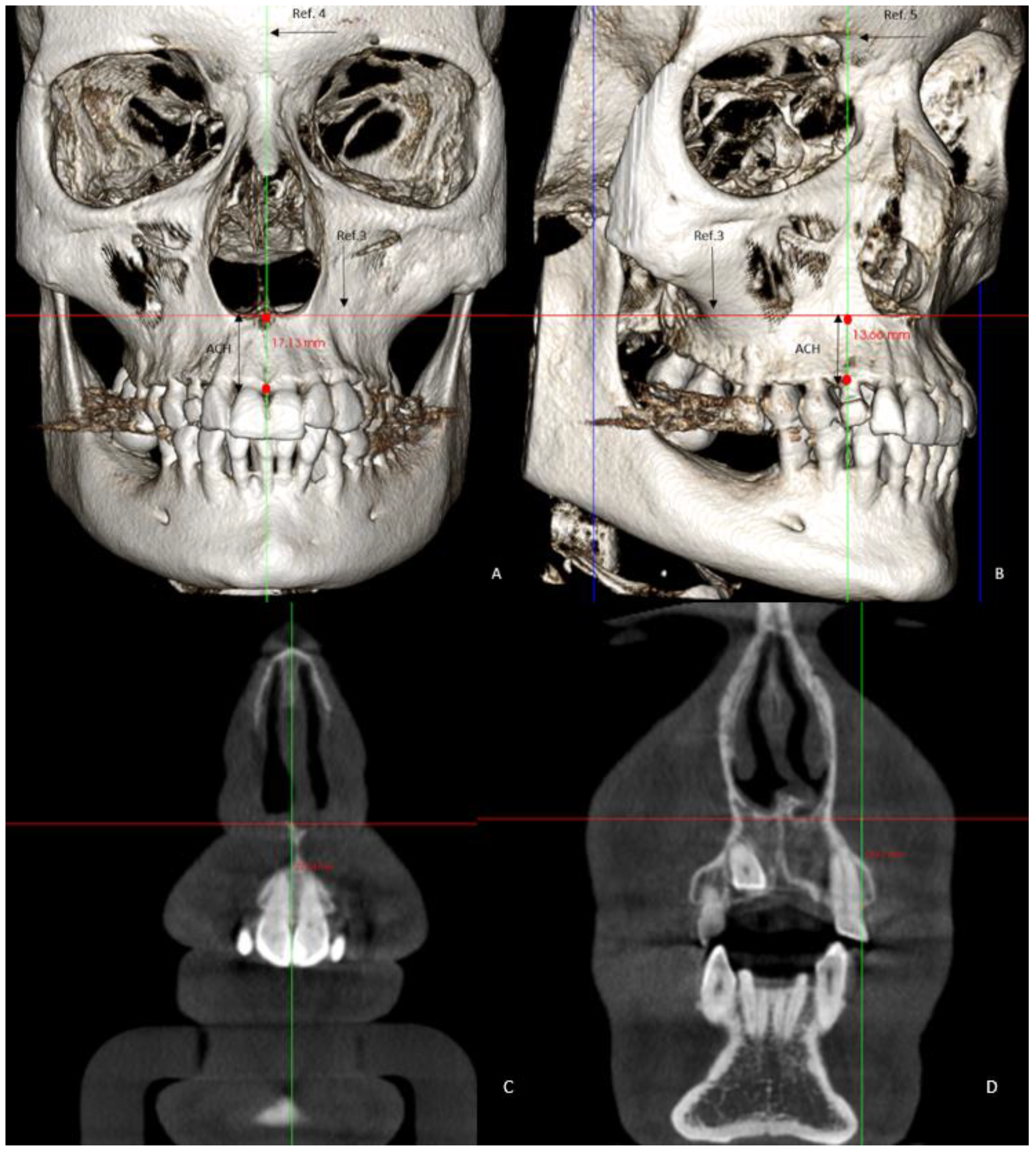
- Maxillary alveolar crest height (ACH) was measured from a tangent to the floor of the nasal fossa, to the lowest alveolar crest between both central incisors (Figure 2) in the GC and GI and, in the GI-R and GI-L, the alveolar crest height from a tangent to the floor of the nasal fossa, to the lowest alveolar crest of the canines, and in its absence, to the lowest alveolar crest of the place that would correspond to the impacted canine (ACH′) [8] (Figure 2).
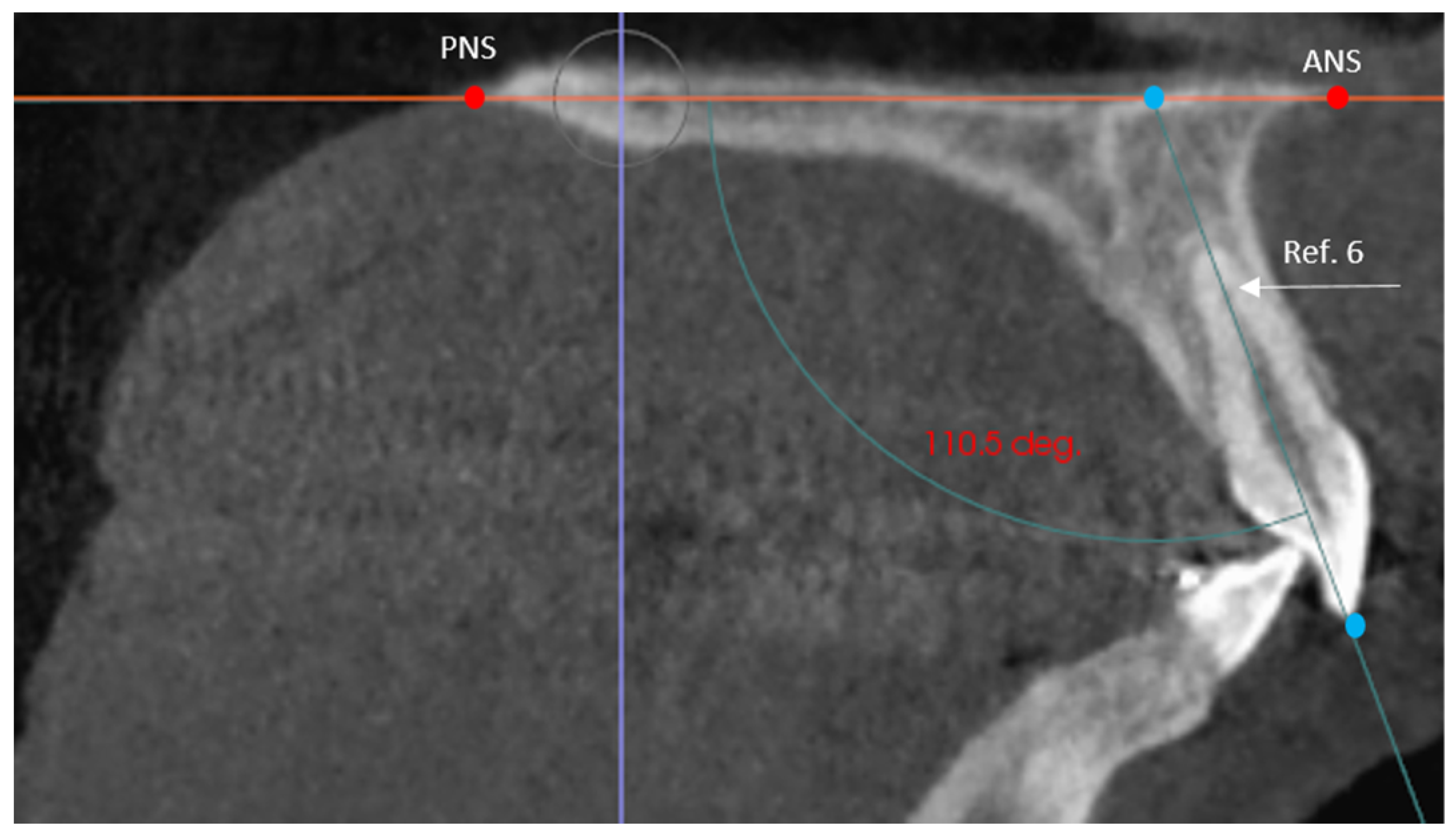
- The angle of the coronal inclination of the upper right and left central incisors with respect to the palatal plane (II) was measured in the sagittal plane (anterior nasal spine-posterior nasal spine) [33] where the angle obtained is that between the major axis of the upper incisor and the palatal plane in the GI and GC. In the GI-R and GI-L subgroups, the coronal inclination of the upper right and left central incisors was measured separately with respect to the palatal plane (II′) (Figure 3).
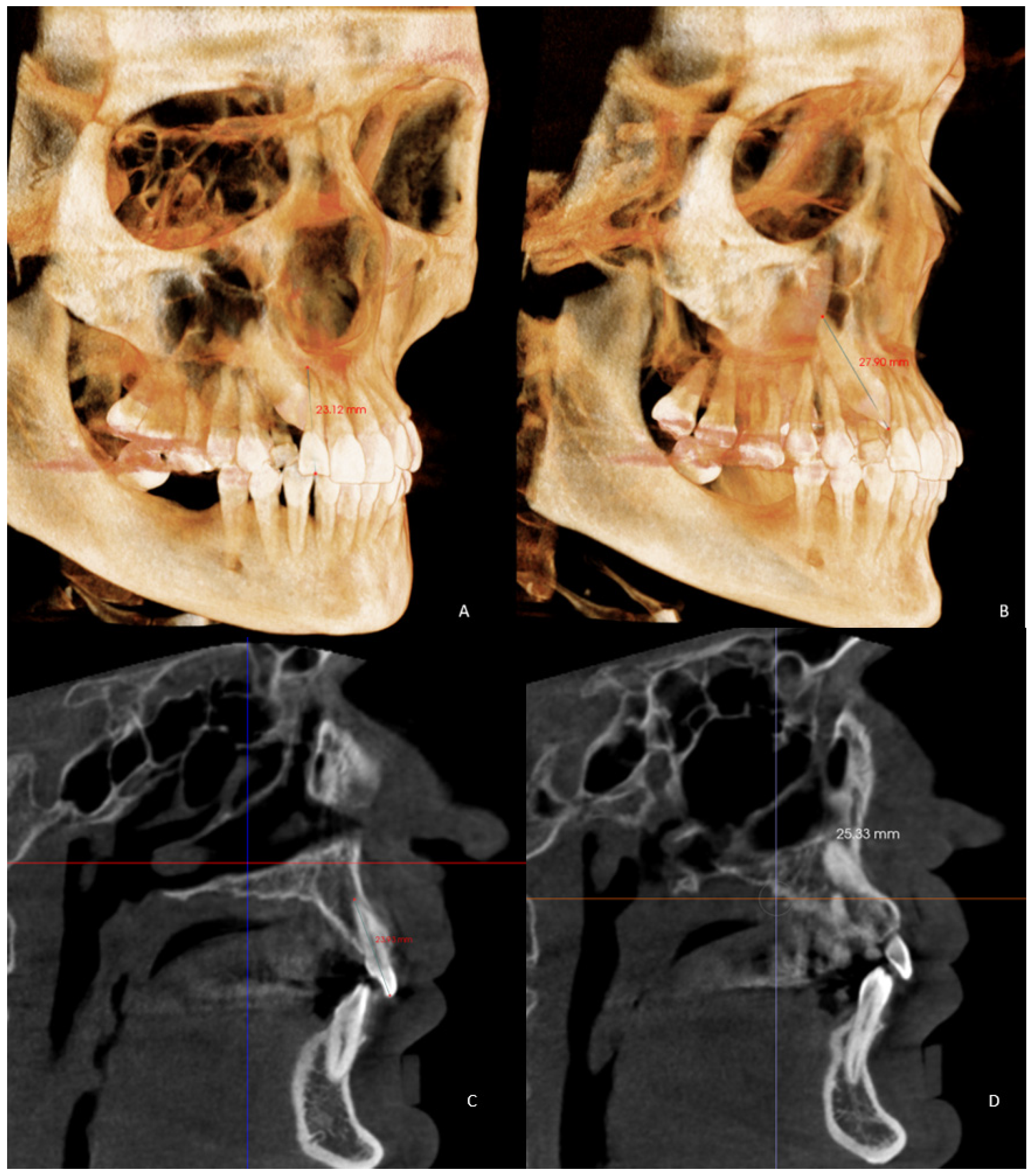
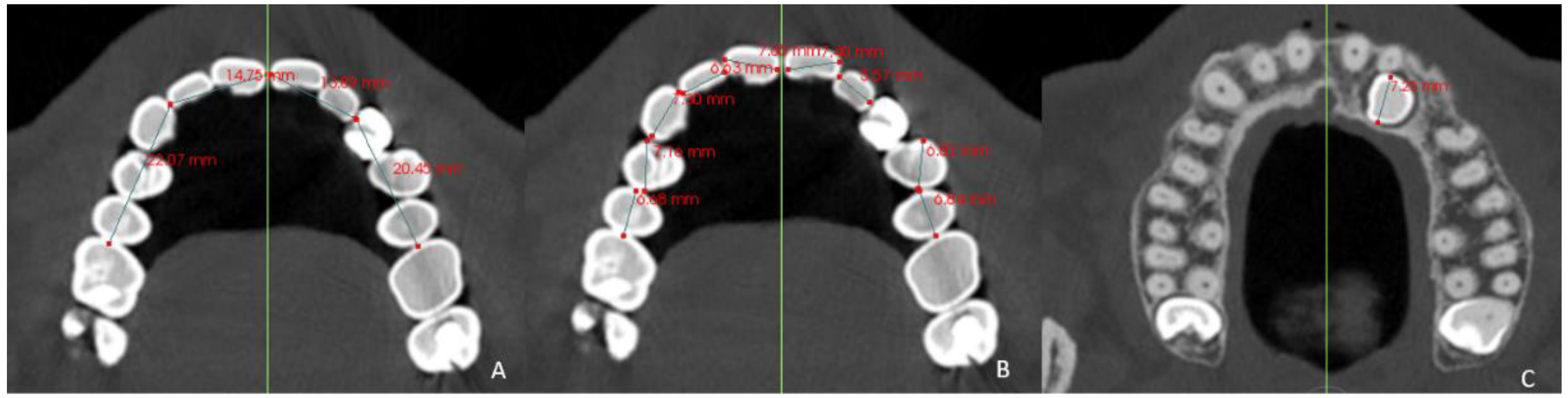
- Arch length (AL) from mesial of the first permanent molar on one side to mesial of the first permanent molar on the contralateral side [35] in the GI and GC. In the GI-R and GI-L, from mesial of the first permanent molar on one side to the dental midline and from the dental midline to the mesial side of the contralateral first permanent molar (AL′) was measured (Figure 5).
2.5. Statistical Analysis
3. Results
3.1. Intraclass Correlation Coefficient
3.2. Differences between the Impacted Group (GI) and Control Group (GC)
3.3. Differences between the GI-R and Control Side
3.4. Differences between the GI-L and the Control Side
3.5. Differences between the GI-L and GI-R with Control Side
3.6. Differences between Male and Female Sex
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tadinada, A.; Mahdian, M.; Vishwanath, M.; Allareddy, V.; Upadhyay, M.; Yadav, S. Evaluation of alveolar bone dimensions in unilateral palatally impacted canine: A cone-beam computed tomographic analyses. Eur. J. Orthod. 2015, 37, 596–602. [Google Scholar] [CrossRef] [PubMed]
- Schubert, M.; Proff, P.; Kirschneck, C. Improved eruption path quantification and treatment time prognosis in alignment of impacted maxillary canines using CBCT imaging. Eur. J. Orthod. 2018, 40, 597–607. [Google Scholar] [CrossRef]
- Dewel, B.F. The upper cuspid: Its development and impaction. Angle Orthod. 1949, 19, 79–90. [Google Scholar]
- Dağsuyu, I.M.; Okşayan, R.; Kahraman, F.; Aydın, M.; Bayrakdar, I.; Uğurlu, M. The Relationship between Dental Follicle Width and Maxillary Impacted Canines’ Descriptive and Resorptive Features Using Cone-Beam Computed Tomography. BioMed Res. Int. 2017, 2017, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Wang, L.; Li, G.; Wu, T.-H.; Diachina, S.; Tejera, B.; Kwon, J.J.; Lin, F.-C.; Lee, Y.-T.; Xu, T.; et al. Machine Learning in Orthodontics: Introducing a 3d Auto-segmentation and Auto-landmark Finder of Cbct Images to Assess Maxillary Constriction in Unilateral Impacted Canine patients. Angle Orthod. 2020, 90, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Schindel, R.H.; Duffy, S.L. Maxillary Transverse Discrepancies and Potentially Impacted Maxillary Canines in Mixed-dentition Patients. Angle Orthod. 2007, 77, 430–435. [Google Scholar] [CrossRef]
- Coulter, J.; Richardson, A. Normal eruption of the maxillary canine quantified in three dimensions. Eur. J. Orthod. 1997, 19, 171–183. [Google Scholar] [CrossRef]
- Oleo-Aracena, M.F.D.; Arriola-Guillén, L.E.; Rodríguez-Cárdenas, Y.A.; Ruíz-Mora, G.A. Skeletal and dentoalveolar bilateral dimensions in unilateral palatally impacted canine using cone beam computed tomography. Prog. Orthod. 2017, 18, 7. [Google Scholar] [CrossRef]
- Kim, Y.; Hyun, H.K.; Jang, K.-T. Interrelationship between the position of impacted maxillary canines and the morphology of the maxilla. Am. J. Orthod. Dentofac. Orthop. 2012, 141, 556–562. [Google Scholar] [CrossRef]
- Naoumova, J.; Alfaro, G.E.; Peck, S. Space conditions, palatal vault height, and tooth size in patients with and without palatally displaced canines: A prospective cohort study. Angle Orthod. 2018, 88, 726–732. [Google Scholar] [CrossRef]
- Zeno, K.G.; Ghafari, J.G. Palatally impacted canines: A new 3-dimensional assessment of severity based on treatment objective. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 387–395. [Google Scholar] [CrossRef]
- Da Silva, A.C.; Capistrano, A.; De Almeida-Pedrin, R.R.; Cardoso, M.D.A.; Conti, A.C.D.C.F.; Filho, L.C.; Capelozza, L. Root length and alveolar bone level of impacted canines and adjacent teeth after orthodontic traction: A long-term evaluation. J. Appl. Oral Sci. 2017, 25, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Ngo, C.T.T.; Fishman, L.S.; Rossouw, P.E.; Wang, H.; Said, O. Correlation between panoramic radiography and cone-beam computed tomography in assessing maxillary impacted canines. Angle Orthod. 2018, 88, 384–389. [Google Scholar] [CrossRef]
- Vitria, E.E.; Tofani, I.; Bachtiar, E.W.; Kusdhany, L. Association of Maxillary Transverse Discrepancies and Impacted Maxillary Canines in Patients 10–25 Years Old. J. Int. Dent. Med. Res. 2016, 9, 322–328. [Google Scholar]
- Peck, S.; Peck, L.; Kataja, M. The palatally displaced canine as a dental anomaly of genetic origin. Angle Orthod. 1994, 64, 249–256. [Google Scholar]
- Warford, J.H.; Grandhi, R.K.; Tira, D.E. Prediction of maxillary canine impaction using sectors and angular measurement. Am. J. Orthod. Dentofac. Orthop. 2003, 124, 651–655. [Google Scholar] [CrossRef]
- Kim, Y.; Hyun, H.-K.; Jang, K.-T. Morphological relationship analysis of impacted maxillary canines and the adjacent teeth on 3-dimensional reconstructed CT images. Angle Orthod. 2017, 87, 590–597. [Google Scholar] [CrossRef] [PubMed]
- Langberg, B.J.; Peck, S. Tooth-size reduction associated with occurrence of palatal displacement of canines. Angle Orthod. 2000, 70, 126–128. [Google Scholar]
- Lüdicke, G.; Harzer, W.; Tausche, E. Incisor Inclination—Risk Factor for Palatally-impacted Canines. J. Orofac. Orthop. 2008, 69, 357–364. [Google Scholar] [CrossRef]
- Al-Nimri, K.; Gharaibeh, T. Space conditions and dental and occlusal features in patients with palatally impacted maxillary canines: An aetiological study. Eur. J. Orthod. 2005, 27, 461–465. [Google Scholar] [CrossRef] [PubMed]
- Mummolo, S.; Nota, A.; De Felice, M.E.; Marcattili, D.; Tecco, S.; Marzo, G. Periodontal status of buccally and palatally impacted maxillary canines after surgical-orthodontic treatment with open technique. J. Oral Sci. 2018, 60, 552–556. [Google Scholar] [CrossRef] [PubMed]
- Jacoby, H. The etiology of maxillary canine impactions. Am. J. Orthod. Dentofac. Orthop. 1983, 84, 125–132. [Google Scholar] [CrossRef]
- Kuftinec, M.M.; Shapira, Y. The impacted maxillary canine: I. Review of concepts. ASDC J. Dent. Child. 1995, 62, 317–324. [Google Scholar]
- Dağsuyu, I.M.; Kahraman, F.; Okşayan, R. Three-dimensional evaluation of angular, linear, and resorption features of maxillary impacted canines on cone-beam computed tomography. Oral Radiol. 2018, 34, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Arboleda-Ariza, N.; Schilling, J.; Arriola-Guillén, L.E.; Ruíz-Mora, G.A.; Rodríguez-Cárdenas, Y.A.; Castillo, A.A.-D. Maxillary transverse dimensions in subjects with and without impacted canines: A comparative cone-beam computed tomography study. Am. J. Orthod. Dentofac. Orthop. 2018, 154, 495–503. [Google Scholar] [CrossRef]
- Saiar, M.; Rebellato, J.; Sheats, R.D. Palatal displacement of canines and maxillary skeletal width. Am. J. Orthod. Dentofac. Orthop. 2006, 129, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Li, Y.; Ge, Z.; Zhao, H.; Miao, L.; Pan, Y. The dimension and morphology of alveolar bone at maxillary anterior teeth in periodontitis: A retrospective analysis—using CBCT. Int. J. Oral Sci. 2020, 12, 4. [Google Scholar] [CrossRef]
- Oz, A.Z.; Oz, A.A.; Palomo, J.M.; El, H. Maxillary sinus volume in patients with impacted canines. Angle Orthod. 2016, 87, 25–32. [Google Scholar] [CrossRef]
- Brooks, S.L. CBCT dosimetry: Orthodontic considerations. Semin Orthod. 2009, 15, 14–18. [Google Scholar] [CrossRef]
- Bjerklin, K.; Ericson, S. How a computerized tomography examination changed the treatment plans of 80 children with retained and ectopically positioned maxillary canines. Angle Orthod. 2006, 76, 43–51. [Google Scholar]
- Baccetti, T. A controlled study of associated dental anomalies. Angle Orthod. 1998, 68, 267–274. [Google Scholar] [PubMed]
- Mercuri, E.; Cassetta, M.; Cavallini, C.; Vicari, D.; Leonardi, R.; Barbato, E. Dental anomalies and clinical features in patients with maxillary canine impaction. Angle Orthod. 2013, 83, 22–28. [Google Scholar] [CrossRef]
- Nahás-Scocate, A.C.R.; Brandão, A.D.S.; Patel, M.P.; Lipiec-Ximenez, M.E.; Chilvarquer, I.; Valle-Corotti, K.M.D. Bone tissue amount related to upper incisors inclination. Angle Orthod. 2014, 84, 279–285. [Google Scholar] [CrossRef]
- Flores-Mir, C.; Rosenblatt, M.R.; Major, P.W.; Carey, J.P.; Heo, G. Measurement accuracy and reliability of tooth length on conventional and CBCT reconstructed panoramic radiographs. Dent. Press J. Orthod. 2014, 19, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Correia, G.D.C.; Habib, F.A.L.; Vogel, C.J. Tooth-size discrepancy: A comparison between manual and digital methods. Dent. Press J. Orthod. 2014, 19, 107–113. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Langberg, B.J.; Peck, S. Adequacy of maxillary dental arch width in patients with palatally displaced canines. Am. J. Orthod. Dentofac. Orthop. 2000, 118, 220–223. [Google Scholar] [CrossRef]
- Eslami, E.; Barkhordar, H.; Abramovitch, K.; Kim, J.; Masoud, M.I. Cone-beam computed tomography vs conventional radiography in visualization of maxillary impacted-canine localization: A systematic review of comparative studies. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 248–258. [Google Scholar] [CrossRef]
- Grisar, K.; Piccart, F.; Al-Rimawi, A.S.; Basso, I.; Politis, C.; Jacobs, R. Three-dimensional position of impacted maxillary canines: Prevalence, associated pathology and introduction to a new classification system. Clin. Exp. Dent. Res. 2019, 5, 19–25. [Google Scholar] [CrossRef]
- Björk, A.; Skieller, V. Growth of the Maxilla in Three Dimensions as Revealed Radiographically by the Implant Method. Br. J. Orthod. 1977, 4, 53–64. [Google Scholar] [CrossRef] [PubMed]
- Gandini, L.G.; Buschang, P.H. Maxillary and mandibular width changes studied using metallic implants. Am. J. Orthod. Dentofac. Orthop. 2000, 117, 75–80. [Google Scholar] [CrossRef]
- Wise, G.E.; He, H.; Gutierrez, D.L.; Ring, S.; Yao, S. Requirement of alveolar bone formation for eruption of rat molars. Eur. J. Oral Sci. 2011, 119, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Basdra, E.K.; Kiokpasoglou, M.; Stellzig, A. The Class II Division 2 craniofacial type is associated with numerous congenital tooth anomalies. Eur. J. Orthod. 2000, 22, 529–535. [Google Scholar] [CrossRef]
- Chávez-Alvarez, C.; Arriola-Guillén, L.E.; Rodríguez-Cárdenas, Y.A.; Ruíz-Mora, G.A.; Fiori-Chincaro, G.; Silveira, H.L.D.-D.; Castillo, A.A.-D. Changes in maxillary incisor inclination and position after traction of unilateral vs bilateral maxillary impacted canines in nonextraction treatment: A cone-beam computed tomography study. Am. J. Orthod. Dentofac. Orthop. 2019, 156, 767–778. [Google Scholar] [CrossRef]
- Karacin, G.; Şenişik, N.E.; Yildirim, D. Comparison of Lateral Tooth Volume and Morphology between Buccally and Palatally Localised Unilateral Impacted Maxillary Canine Cases on Cone-Beam Computed Tomography. J. Craniofacial Surg. 2021, 32, 752–756. [Google Scholar] [CrossRef] [PubMed]
- Hettiarachchi, P.V.K.S.; Olive, R.J.; Monsour, P. Morphology of palatally impacted canines: A case-controlled cone-beam volumetric tomography study. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 357–362. [Google Scholar] [CrossRef]
- Becker, A.; Smith, P.; Behar, R. The incidence of anomalous maxillary lateral incisors in relation to palatally-displaced cuspids. Angle Orthod. 1981, 51, 24–29. [Google Scholar]
- Capitaneanu, C.; Willems, G.; Jacobs, R.; Fieuws, S.; Thevissen, P. Sex estimation based on tooth measurements using panoramic radiographs. Int. J. Legal Med. 2017, 131, 813–821. [Google Scholar] [CrossRef]
- Seeman, E. Clinical review 137: Sexual dimorphism in skeletal size, density, and strength. J. Clin. Endocrinol. Metab. 2001, 86, 4576–4584. [Google Scholar] [CrossRef]
- Schneider, S.; Gandhi, V.; Upadhyay, M.; Allareddy, V.; Tadinada, A.; Yadav, S. Sex, growth pattern, and growth status-related variability in maxillary and mandibular buccal cortical thickness and density. Korean J. Orthod. 2020, 50, 108–119. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Group (GI) | Subgroup Left Side Impaction (GI-L) | Subgroup Right Side Impaction (GI-R) | Control Group (GC) | |||
|---|---|---|---|---|---|---|
| Total Sample | 50 | 21 | 29 | 50 | ||
| Age | Mean | 32.8 | 30.33 | 34.55 | 26.8 | |
| SD | 9.16 | 9.35 | 9.08 | 5.78 | ||
| Sex | Men | n | 21 | 12 | 9 | 23 |
| % | 46 | 57.14 | 31.03 | 43 | ||
| Women | n | 29 | 9 | 20 | 27 | |
| % | 54 | 42.86 | 68.96 | 58 |
| Single Measures | Intraclass Correlation |
|---|---|
| Skeletal Variables | |
| BMW | 0.717 |
| ACH | 0.874 |
| Dentoalveolar Variables | |
| II | 0.957 |
| RCL | 0.874 |
| RLIL | 0.791 |
| LLIL | 0.574 |
| LCL | 0.870 |
| AL | 0.935 |
| TS | 0.670 |
| ATD | 0.743 |
| Variables | GI n = 50 | GC n = 50 | p Value |
|---|---|---|---|
| Skeletal variables | |||
| BMW (mean ± SD) (mm) | 58.39 ± 3.50 | 59.77 ± 4.14 | 0.075 |
| ACH (mean ± SD) (mm) | 18.52 ± 3.47 | 20.80 ± 2.74 | >0.001 ** |
| Dentoalveolar variables | |||
| II (mean ± SD) (degree) | 101.76 ± 8.31 | 106.58 ± 6.61 | 0.002 ** |
| RCL (mean ± SD) (mm) | 25.08 ± 2.54 | 26.29 ± 2.37 | 0.016 * |
| RLIL (mean ± SD) (mm) | 21.24 ± 2.02 | 22.14 ± 2.07 | 0.031 * |
| LLIL (mean ± SD) (mm) | 21.14 ± 2.08 | 22.33 ± 1.89 | 0.003 ** |
| LCL (mean ± SD) (mm) | 25.08 ± 2.50 | 26.12 ± 256 | 0.043 * |
| AL (mean ± SD) (mm) | 69.37 ± 3.83 | 71.05 ± 3.25 | 0.021 * |
| TS (mean ± SD) (mm) | 69.80 ± 4.24 | 70.43 ± 3.79 | 0.433 |
| ATD (mean ± SD) (mm) | −0.42 ± 4.11 | 0.61 ± 2.90 | 0.147 |
| Variables | GI-R n = 29 | Control Side n = 29 | p-Value |
|---|---|---|---|
| Skeletal variables | |||
| J-PR (mean ± SD) (mm) | 40.18 ± 4.08 | 38.88 ± 3.36 | 0.126 |
| ACH′ (mean ± SD) (mm) | 14.87 ± 2.98 | 15.40 ± 3.06 | 0.005 ** |
| Dentoalveolar variables | |||
| II′ (mean ± SD) (degree) | 99.70 ± 8.08 | 101.67 ± 8.48 | 0.036 * |
| CL (mean ± SD) (mm) | 25.20 ± 2.27 | 24.97 ± 2.65 | 0.523 |
| LIL (mean ± SD) (mm) | 21.01 ± 2.23 | 21.24 ± 1.97 | 0.369 |
| AL′ (mean ± SD) (mm) | 33.72 ± 1.95 | 35.09 ± 1.64 | <0.001 ** |
| TS′ (mean ± SD) (mm) | 34.69 ± 1.71 | 34.21 ± 1.90 | 0.037 * |
| ATD′ (mean ± SD) (mm) | −0.96 ± 1.63 | 0.88 ± 2.28 | <0.001 ** |
| Variables | GI-L n = 21 | Control Side n = 21 | p-Value |
|---|---|---|---|
| Skeletal variables | |||
| J-PR (mean ± SD) (mm) | 40.46 ± 3.28 | 41.63 ± 4.09 | 0.211 |
| ACH′ (mean ± SD) (mm) | 15.53 ± 3.00 | 16.99 ± 3.43 | >0.001 ** |
| Dentoalveolar variables | |||
| II′ (mean ± SD) (degree) | 102.76 ± 8.75 | 103.73 ± 9.03 | 0.125 |
| CL (mean ± SD) (mm) | 25.24 ± 2.34 | 24.92 ± 2.93 | 0.380 |
| LIL (mean ± SD) (mm) | 20.99 ± 2.27 | 21.56 ± 1.70 | 0.055 * |
| AL′ (mean ± SD) (mm) | 34.14 ± 2.65 | 35.80 ± 2.22 | >0.001 ** |
| TS′ (mean ± SD) (mm) | 35.40 ± 2.58 | 35.63 ± 2.62 | 0.496 |
| ATD′ (mean ± SD) (mm) | −1.26 ± 3.08 | 0.16 ± 2.40 | 0.003 ** |
| Variables | Imp. n = 50 | Control Side. Non-Imp. n = 50 | p-Value |
|---|---|---|---|
| Skeletal variables | |||
| J-PR (mean ± SD) (mm) | 40.30 ± 3.73 | 40.03 ± 3.89 | 0.674 |
| ACH′ (mean ± SD) (mm) | 15.15 ± 2.98 | 16.07 ± 3.28 | >0.001 ** |
| Dentoalveolar variables | |||
| II′ (mean ± SD) (degree) | 100.99 ± 8.42 | 102.54 ± 8.69 | 0.010 ** |
| CL (mean ± SD) (mm) | 25.22 ± 2.28 | 24.95 ± 2.74 | 0.294 |
| LIL (mean ± SD) (mm) | 21.01 ± 2.22 | 21.37 ± 1.85 | 0.051 * |
| AL′ (mean ± SD) (mm) | 33.90 ± 2.26 | 35.39 ± 1.91 | >0.001 ** |
| TS′ (mean ± SD) (mm) | 34.99 ± 2.12 | 34.81 ± 2.31 | 0.347 |
| ATD′ (mean ± SD) (mm) | −1.08 ± 2.62 | 0.58 ± 2.00 | >0.001 ** |
| Variables | Male n = 21 | Female n = 29 | p-Value |
|---|---|---|---|
| Skeletal variables | |||
| J-PR (mean ± SD) (mm) | 41.37 ± 3.29 | 39.52 ± 3.89 | 0.084 |
| ACH′ (mean ± SD) (mm) | 19.10 ± 3.73 | 19.39 ± 3.23 | 0.769 |
| Dentoalveolar variables | |||
| II′ (mean ± SD) (degree) | 101.98 ± 8.65 | 100.27 ± 8.34 | 0.485 |
| CL (mean ± SD) (mm) | 25.56 ± 2.35 | 24.97 ± 2.22 | 0.368 |
| LIL (mean ± SD) (mm) | 21.58 ± 1.52 | 20.49 ± 2.56 | 0.124 |
| AL′ (mean ± SD) (mm) | 34.88 ± 2.23 | 33.19 ± 2.03 | 0.007 ** |
| TS′ (mean ± SD) (mm) | 35.59 ± 1.88 | 34.55 ± 2.21 | 0.089 |
| ATD′ (mean ± SD) (mm) | −0.70 ± 2.41 | −1.36 ± 2.77 | 0.387 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montes-Díaz, M.E.; Martínez-González, A.; Arriazu-Navarro, R.; Alvarado-Lorenzo, A.; Gallardo-López, N.E.; Ortega-Aranegui, R. Skeletal and Dental Morphological Characteristics of the Maxillary in Patients with Impacted Canines Using Cone Beam Computed Tomography: A Retrospective Clinical Study. J. Pers. Med. 2022, 12, 96. https://doi.org/10.3390/jpm12010096
Montes-Díaz ME, Martínez-González A, Arriazu-Navarro R, Alvarado-Lorenzo A, Gallardo-López NE, Ortega-Aranegui R. Skeletal and Dental Morphological Characteristics of the Maxillary in Patients with Impacted Canines Using Cone Beam Computed Tomography: A Retrospective Clinical Study. Journal of Personalized Medicine. 2022; 12(1):96. https://doi.org/10.3390/jpm12010096
Chicago/Turabian StyleMontes-Díaz, María Elena, Alicia Martínez-González, Riánsares Arriazu-Navarro, Alfonso Alvarado-Lorenzo, Nuria Esther Gallardo-López, and Ricardo Ortega-Aranegui. 2022. "Skeletal and Dental Morphological Characteristics of the Maxillary in Patients with Impacted Canines Using Cone Beam Computed Tomography: A Retrospective Clinical Study" Journal of Personalized Medicine 12, no. 1: 96. https://doi.org/10.3390/jpm12010096
APA StyleMontes-Díaz, M. E., Martínez-González, A., Arriazu-Navarro, R., Alvarado-Lorenzo, A., Gallardo-López, N. E., & Ortega-Aranegui, R. (2022). Skeletal and Dental Morphological Characteristics of the Maxillary in Patients with Impacted Canines Using Cone Beam Computed Tomography: A Retrospective Clinical Study. Journal of Personalized Medicine, 12(1), 96. https://doi.org/10.3390/jpm12010096