
A Novel Tool for a Challenging Disease: Stasis Leg Ulcers Assessed Using QFlow in Triggered Angiography Noncontrast Enhanced Magnetic Resonance Imaging

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. MRI Acquisition
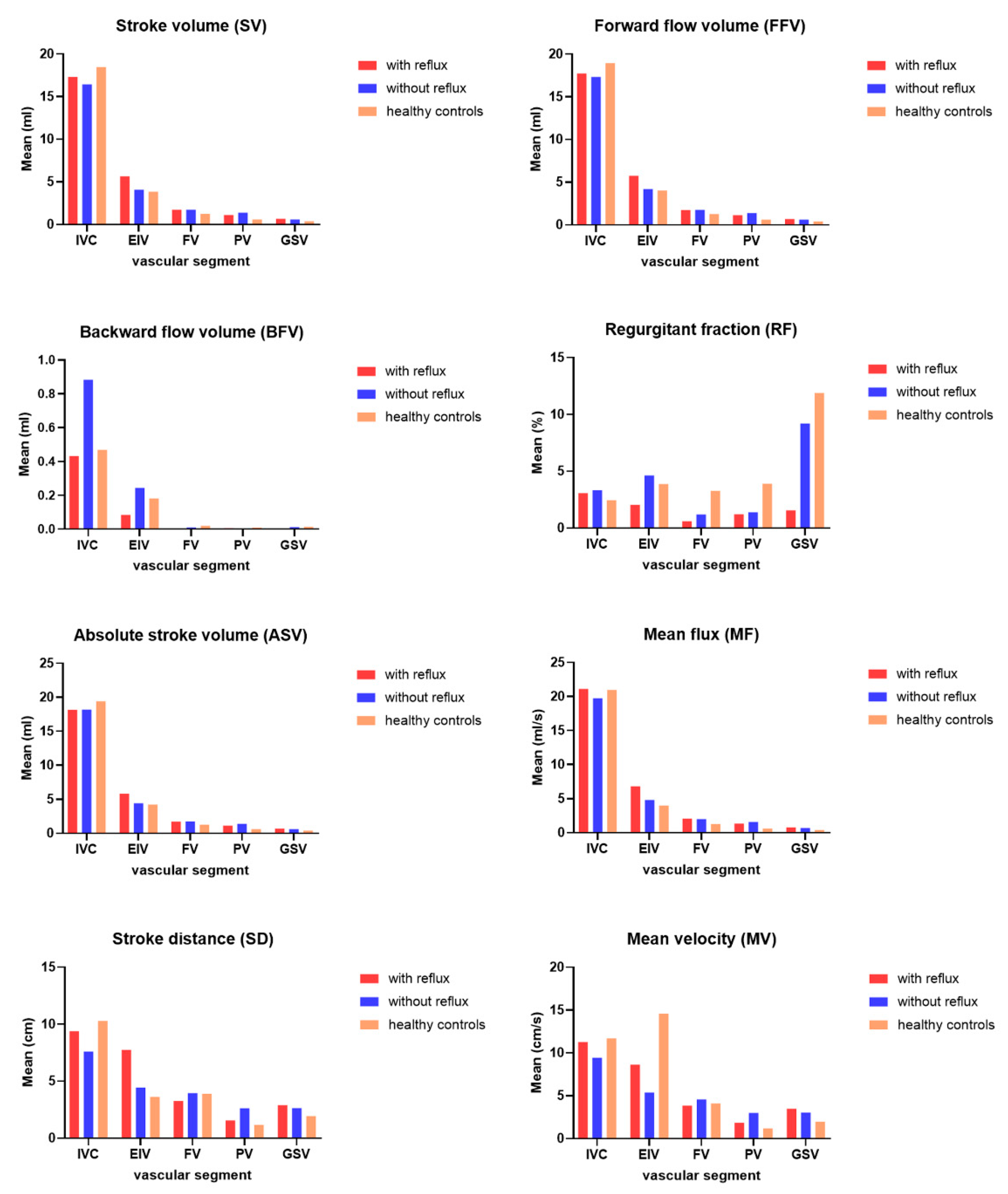
- Stroke volume (SV), mLThe net volume of blood that passes through the contour of ROI during one R–R interval.
- Forward flow volume (FFV), mLThe volume of blood that passes through the contour of ROI in the positive direction (toward head direction) during 1 R–R interval.
- Backward flow volume (BFV), mLThe volume of blood that passes through the contour of ROI in the negative direction (toward foot direction) during 1 R–R interval.
- Regurgitant fraction (RF), %The fraction of the backward flow to forwarding flow.
- Absolute stroke volume (ASV), mLThe absolute value of forwarding flow volume plus the absolute value of backward flow volume.
- Mean flux (MF), mL/sStroke amount × heartbeat/60 (1 R–R interval).
- Stroke distance (SD), cmThe net distance that blood proceeds in the vessel during 1 R–R interval.
- Mean velocity (MV), cm/sStroke distance × heartbeat/60 (1 R–R interval).
2.3. Statistical Analysis
3. Results
3.1. Comparison of Preoperative Duplex Scanning and TRANCE MRI
3.2. Comparison of TRANCE MRI Hemodynamic Parameters among the Reflux, Nonreflux, and Healthy Control Groups
4. Discussion
Study Limitations
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 3D | three-dimensional |
| ASV | absolute stroke volume |
| BFV | backward flow volume |
| CT | computed tomography |
| CTA | computed tomography angiography |
| DVT | deep venous thrombosis |
| EIV | external iliac vein |
| FFV | forward flow volume |
| FOV | field of view |
| FV | femoral vein |
| GSV | great saphenous vein |
| IR | inversion recovery |
| IRB | institutional review board |
| IVC | inferior vena cava |
| MF | mean flux |
| MRI | magnetic resonance imaging |
| MRV | magnetic resonance venography |
| MV | mean velocity |
| NSF | nephrogenic systemic fibrosis |
| PV | popliteal vein |
| RF | regurgitant fraction |
| SLU | stasis leg ulcer |
| SD | stroke distance |
| STIR | short tau inversion recovery |
| SV | stroke volume |
| TE | echo time |
| TOF | time-of-flight |
| TR | repetition time |
| TRANCE-MRI | triggered angiography non-contrast-enhanced MRI |
| TSE | turbo spin-echo |
References
- O’Donnell, T.F., Jr.; Passman, M.A.; Marston, W.A.; Ennis, W.J.; Dalsing, M.; Kistner, R.L.; Lurie, F.; Henke, P.K.; Gloviczki, M.L.; Eklof, B.G.; et al. Management of venous leg ulcers: Clinical practice guidelines of the Society for Vascular Surgery (R) and the American Venous Forum. J. Vasc. Surg. 2014, 60, 3S–59S. [Google Scholar] [CrossRef]
- Bonkemeyer Millan, S.; Gan, R.; Townsend, P.E. Venous Ulcers: Diagnosis and Treatment. Am. Fam. Physic. 2019, 100, 298–305. [Google Scholar]
- Star, A. Differentiating Lower Extremity Wounds: Arterial, Venous, Neurotrophic. Semin. Interv. Radiol. 2018, 35, 399–405. [Google Scholar] [CrossRef]
- Lim, C.S.; Baruah, M.; Bahia, S.S. Diagnosis and management of venous leg ulcers. BMJ 2018, 362, k3115. [Google Scholar] [CrossRef] [PubMed]
- Bradley, W.G., Jr.; Waluch, V. Blood flow: Magnetic resonance imaging. Radiology 1985, 154, 443–450. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.W.; Tseng, Y.H.; Lin, C.C.; Kao, C.C.; Wong, M.Y.; Lin, B.S.; Huang, Y.K. Novel Diagnostic Options without Contrast Media or Radiation: Triggered Angiography Non-Contrast-Enhanced Sequence Magnetic Resonance Imaging in Treating Different Leg Venous Diseases. Diagnostics 2020, 10, 355. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.K.; Tseng, Y.H.; Lin, C.H.; Tsai, Y.H.; Hsu, Y.C.; Wang, S.C.; Chen, C.W. Evaluation of venous pathology of the lower extremities with triggered angiography non-contrast-enhanced magnetic resonance imaging. BMC Med. Imaging 2019, 19, 96. [Google Scholar] [CrossRef]
- Tawfik, A.M.; Elsorogy, L.; Abdelghaffar, R.; Naby, A.A.; Elmenshawi, I. Phase-Contrast MRI CSF Flow Measurements for the Diagnosis of Normal-Pressure Hydrocephalus: Observer Agreement of Velocity Versus Volume Parameters. AJR Am. J. Roentgenol. 2017, 208, 838–843. [Google Scholar] [CrossRef]
- von Spiczak, J.; Crelier, G.; Giese, D.; Kozerke, S.; Maintz, D.; Bunck, A.C. Quantitative Analysis of Vortical Blood Flow in the Thoracic Aorta Using 4D Phase Contrast MRI. PLoS ONE 2015, 10, e0139025. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.W.; Tseng, Y.H.; Lin, C.C.; Kao, C.C.; Wong, M.Y.; Ting, H.; Huang, Y.K. Aortic dissection assessment by 4D phase-contrast MRI with hemodynamic parameters: The impact of stent type. Quant. Imaging Med. Surg. 2021, 11, 490–501. [Google Scholar] [CrossRef]
- Tseng, Y.H.; Chen, C.W.; Wong, M.Y.; Yang, T.Y.; Lin, B.S.; Ting, H.; Huang, Y.K. Discriminating Reflux from Non-Reflux Diseases of Superficial Veins in Legs by Novel Non-Contrast MR with QFlow Technique. J. Pers. Med. 2021, 11, 242. [Google Scholar] [CrossRef]
- O’Donnell, T.F., Jr.; Passman, M.A. Clinical practice guidelines of the Society for Vascular Surgery (SVS) and the American Venous Forum (AVF)--Management of venous leg ulcers. Introduction. J. Vasc. Surg. 2014, 60, 1S–2S. [Google Scholar] [CrossRef] [PubMed]
- Kelechi, T.J.; Brunette, G.; Bonham, P.A.; Crestodina, L.; Droste, L.R.; Ratliff, C.R.; Varnado, M.F. 2019 Guideline for Management of Wounds in Patients With Lower-Extremity Venous Disease (LEVD): An Executive Summary. J. Wound Ostomy Cont. Nurs. 2020, 47, 97–110. [Google Scholar] [CrossRef]
- Lurie, F.; Passman, M. What is new in the 2020 update of the CEAP classification? Int. Angiol. 2020, 39, 443–444. [Google Scholar] [CrossRef]
- Khilnani, N.M.; Davies, A.H. CEAP: A review of the 2020 revision. Phlebology 2020, 35, 745–748. [Google Scholar] [CrossRef]
- Lurie, F.; Passman, M.; Meisner, M.; Dalsing, M.; Masuda, E.; Welch, H.; Bush, R.L.; Blebea, J.; Carpentier, P.H.; De Maeseneer, M.; et al. The 2020 update of the CEAP classification system and reporting standards. J. Vasc. Surg. Venous Lymphat. Disord. 2020, 8, 342–352. [Google Scholar] [CrossRef] [PubMed]
- Mutlak, O.; Aslam, M.; Standfield, N.J. Chronic venous insufficiency: A new concept to understand pathophysiology at the microvascular level—A pilot study. Perfusion 2019, 34, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Bjarnsholt, T.; Kirketerp-Moller, K.; Jensen, P.O.; Madsen, K.G.; Phipps, R.; Krogfelt, K.; Hoiby, N.; Givskov, M. Why chronic wounds will not heal: A novel hypothesis. Wound Repair Regen. 2008, 16, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Morilla-Herrera, J.C.; Morales-Asencio, J.M.; Gomez-Gonzalez, A.J.; Diez-De Los Rios, A.; Lupianez-Perez, I.; Acosta-Andrade, C.; Aranda-Gallardo, M.; Moya-Suarez, A.B.; Kaknani-Uttumchandani, S.; Garcia-Mayor, S. Effectiveness of a hydrophobic dressing for microorganisms’ colonization of vascular ulcers: Protocol for a randomized controlled trial (CUCO-UV Study). J. Adv. Nurs. 2020. [CrossRef]
- Lo, Z.J.; Lim, X.; Eng, D.; Car, J.; Hong, Q.; Yong, E.; Zhang, L.; Chandrasekar, S.; Tan, G.W.L.; Chan, Y.M.; et al. Clinical and economic burden of wound care in the tropics: A 5-year institutional population health review. Int. Wound J. 2020, 17, 790–803. [Google Scholar] [CrossRef]
- Rice, J.B.; Desai, U.; Cummings, A.K.; Birnbaum, H.G.; Skornicki, M.; Parsons, N. Burden of venous leg ulcers in the United States. J. Med. Econ. 2014, 17, 347–356. [Google Scholar] [CrossRef]
- Gaitini, D. Current approaches and controversial issues in the diagnosis of deep vein thrombosis via duplex Doppler ultrasound. J. Clin. Ultrasound 2006, 34, 289–297. [Google Scholar] [CrossRef]
- Reid, J.H. Multislice CT pulmonary angiography and CT venography. Br. J. Radiol. 2004, 77, S39–S45. [Google Scholar] [CrossRef] [PubMed]
- Tamura, K.; Nakahara, H. MR Venography for the Assessment of Deep Vein Thrombosis in Lower Extremities with Varicose Veins. Ann. Vasc. Dis. 2014, 7, 399–403. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ruehm, S.G.; Wiesner, W.; Debatin, J.F. Pelvic and lower extremity veins: Contrast-enhanced three-dimensional MR venography with a dedicated vascular coil-initial experience. Radiology 2000, 215, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Renard, D.; Le Bars, E.; Arquizan, C.; Gaillard, N.; de Champfleur, N.M.; Mourand, I. Time-of-flight MR angiography in cerebral venous sinus thrombosis. Acta Neurol. Belg. 2017, 117, 837–840. [Google Scholar] [CrossRef] [PubMed]
- Yucel, E.K.; Kaufman, J.A.; Geller, S.C.; Waltman, A.C. Atherosclerotic occlusive disease of the lower extremity: Prospective evaluation with two-dimensional time-of-flight MR angiography. Radiology 1993, 187, 637–641. [Google Scholar] [CrossRef]
- Suttmeyer, B.; Teichgraber, U.; Thomas, A.; Rathke, H.; Albrecht, L.; Jonczyk, M.; Verba, M.; Guttler, F.; Schnackenburg, B.; Hamm, B.; et al. Non-invasive ECG-triggered 2D TOF MR angiography of the pelvic and leg arteries in an open 1.0-tesla high-field MRI system in comparison to conventional DSA. Biomed. Tech. Biomed. Eng. 2014, 59, 29–37. [Google Scholar] [CrossRef]
- Harigai, M.; Okada, T.; Umeoka, S.; Nagayama, S.; Tanaka, E.; Fujimoto, K.; Kido, A.; Takeda, K.; Togashi, K.; Sakai, Y. Non-contrast-enhanced MR venography of the upper limb: A comparative study of acquisitions with fresh blood imaging vs. time-of-flight methods. Clin. Imaging 2012, 36, 496–501. [Google Scholar] [CrossRef]
- Steffens, J.C.; Link, J.; Schwarzenberg, H.; Mueller-Huelsbeck, S.; Brinkmann, G.; Heller, M. Lower extremity occlusive disease: Diagnostic imaging with a combination of cardiac-gated 2D phase-contrast and cardiac-gated 2D time-of-flight MRA. J. Comput. Assist. Tomogr. 1999, 23, 7–12. [Google Scholar] [CrossRef]
- Gurel, K.; Gurel, S.; Karavas, E.; Buharalioglu, Y.; Daglar, B. Direct contrast-enhanced MR venography in the diagnosis of May-Thurner syndrome. Eur. J. Radiol. 2011, 80, 533–536. [Google Scholar] [CrossRef]
- Ruehm, S.G.; Zimny, K.; Debatin, J.F. Direct contrast-enhanced 3D MR venography. Eur. Radiol. 2001, 11, 102–112. [Google Scholar] [CrossRef] [PubMed]
- Alfano, G.; Fontana, F.; Ferrari, A.; Solazzo, A.; Perrone, R.; Giaroni, F.; Torricelli, P.; Cappelli, G. Incidence of nephrogenic systemic fibrosis after administration of gadoteric acid in patients on renal replacement treatment. Magn. Reson. Imaging 2020, 70, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Schieda, N.; Maralani, P.J.; Hurrell, C.; Tsampalieros, A.K.; Hiremath, S. Updated Clinical Practice Guideline on Use of Gadolinium-Based Contrast Agents in Kidney Disease Issued by the Canadian Association of Radiologists. Can. Assoc. Radiol. J. 2019, 70, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Ross, M.R.; Pelc, N.J.; Enzmann, D.R. Qualitative phase contrast MRA in the normal and abnormal circle of Willis. AJNR Am. J. Neuroradiol. 1993, 14, 19–25. [Google Scholar]
- Forner Giner, J.; Sanz-Requena, R.; Florez, N.; Alberich-Bayarri, A.; Garcia-Marti, G.; Ponz, A.; Marti-Bonmati, L. Quantitative phase-contrast MRI study of cerebrospinal fluid flow: A method for identifying patients with normal-pressure hydrocephalus. Neurologia 2014, 29, 68–75. [Google Scholar] [CrossRef]
- Gutzeit, A.; Sutter, R.; Froehlich, J.M.; Roos, J.E.; Sautter, T.; Schoch, E.; Giger, B.; Wyss, M.; Graf, N.; von Weymarn, C.; et al. ECG-triggered non-contrast-enhanced MR angiography (TRANCE) versus digital subtraction angiography (DSA) in patients with peripheral arterial occlusive disease of the lower extremities. Eur. Radiol. 2011, 21, 1979–1987. [Google Scholar] [CrossRef] [PubMed]
- Suttmeyer, B.; Teichgraber, U.; Rathke, H.; Albrecht, L.; Guttler, F.; Schnackenburg, B.; Hamm, B.; de Bucourt, M. Initial experience with imaging of the lower extremity arteries in an open 1.0 Tesla MRI system using the triggered angiography non-contrast-enhanced sequence (TRANCE) compared to digital subtraction angiography (DSA). Biomed. Eng. Biomed. Tech. 2016, 61, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Radlbauer, R.; Salomonowitz, E.; van der Riet, W.; Stadlbauer, A. Triggered non-contrast enhanced MR angiography of peripheral arteries: Optimization of systolic and diastolic time delays for electrocardiographic triggering. Eur. J. Radiol. 2011, 80, 331–335. [Google Scholar] [CrossRef]
- Ohno, N.; Miyati, T.; Noda, T.; Alperin, N.; Hamaguchi, T.; Ohno, M.; Matsushita, T.; Mase, M.; Gabata, T.; Kobayashi, S. Fast Phase-Contrast Cine MRI for Assessing Intracranial Hemodynamics and Cerebrospinal Fluid Dynamics. Diagnostics 2020, 10, 241. [Google Scholar] [CrossRef]
- Chen, C.W.; Ting, H.; Chen, P.Y.; Weng, J.C.; Hsu, Y.C.; Wang, S.C.; Tseng, Y.H.; Huang, Y.K. Usefulness of triggered non-contrast-enhanced magnetic resonance angiography in assessing lower extremity venous disease. Medicine 2021, 100, e25809. [Google Scholar] [CrossRef]
- Lin, B.S.; Chen, C.W.; Zhou, S.K.; Tseng, Y.H.; Wang, S.C.; Huang, Y.K. Evaluation of static ulcer on lower extremities using wireless wearable near-infrared spectroscopy device: Effect of deep venous thrombosis on TRiggered Angiography Non-Contrast-Enhanced sequence magnetic resonance imaging. Phlebology 2020, 35, 814–823. [Google Scholar] [CrossRef] [PubMed]
- Kao, C.-C.; Chen, C.-W.; Tseng, Y.-H.; Tsai, Y.-H.; Wang, S.-C.; Huang, Y.-K. Non-contrast-enhanced magnetic resonance imaging: Objective figures in differentiation between acute and chronic deep venous thrombosis in the lower extremities. Phlebology 2020, 35, 777–783. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.W.; Tseng, Y.H.; Wong, M.Y.; Wu, C.M.; Lin, B.S.; Huang, Y.K. Stasis Leg Ulcers: Venous System Revises by Triggered Angiography Non-Contrast-Enhanced Sequence Magnetic Resonance Imaging. Diagnostics 2020, 10, 707. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.-L.; Huang, Y.-K.; Hsu, L.-S.; Chen, P.-Y.; Chen, C.-W. The use of non-contrast-enhanced MRI to evaluate serial changes in endoleaks after aortic stenting: A case report. BMC Med. Imaging 2019, 19, 1–4. [Google Scholar] [CrossRef]
- Hsu, Y.C.; Huang, Y.K.; Hsu, L.S.; Chen, P.Y.; Chen, C.W. Using non-contrast-enhanced magnetic resonance venography for the evaluation of May-Thurner syndrome in patients with renal insufficiency: A case report. Medicine 2019, 98, e18427. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total | SLU with Superficial Venous Reflux | SLU without Superficial Venous Reflux | Healthy Volunteer | p-Value | |
|---|---|---|---|---|---|
| Patient Number | 33 | 15 | 18 | 14 | |
| Gender | 0.262 | ||||
| Male | 18 | 8 | 10 | 4 | |
| Female | 15 | 7 | 8 | 10 | |
| Age | 64.5 ± 11.4 | 59.5 ± 11.6 | 68.6 ± 9.7 | 51.4 ± 2.4 | <0.01 * |
| Substance | |||||
| Smoking | 9 | 3 | 6 | 0.324 | |
| Alcohol | 6 | 1 | 5 | 0.133 | |
| Betel nut | 6 | 3 | 3 | 0.577 | |
| Comorbidities | |||||
| Hypertension | 11 | 2 | 9 | 0.03 * | |
| Diabetes | 9 | 5 | 4 | 0.373 | |
| Stroke | 1 | 1 | 0 | 0.455 | |
| Coronary disease | 0 | 0 | 0 | NA | |
| DVT history | 1 | 9 | 1 | 0.545 | |
| Cancer | 3 | 0 | 3 | 0.15 | |
| COPD | 5 | 2 | 3 | 0.591 | |
| ESRD | 1 | 0 | 1 | 0.545 |
| Total | SLU with Superficial Venous Reflux | SLU without Superficial Venous Reflux | p-Value | |
|---|---|---|---|---|
| Patient Number | 33 | 15 | 18 | |
| Wound Leg | 0.037 * | |||
| Right | 16 | 8 | 8 | |
| Left | 11 | 7 | 4 | |
| Both | 6 | 0 | 6 | |
| C in CEAP | 0.455 | |||
| C5 | 1 | 1 | 0 | |
| C6 | 32 | 14 | 18 | |
| E in CEAP | <0.001 * | |||
| Ec | 4 | 0 | 4 | |
| Ep | 17 | 15 | 2 | |
| Es | 11 | 0 | 11 | |
| En | 1 | 0 | 1 | |
| A in CEAP | <0.001 * | |||
| As | 15 | 15 | 0 | |
| Ad | 13 | 0 | 13 | |
| Ap | 1 | 0 | 1 | |
| An | 4 | 0 | 4 | |
| P in CEAP | <0.001 * | |||
| Pr | 15 | 15 | 0 | |
| Po | 18 | 0 | 18 | |
| Wound location | 0.583 | |||
| Gaiter area | 4 | 1 | 3 | |
| Medial ankle | 20 | 10 | 10 | |
| Lateral ankle | 5 | 3 | 2 | |
| Foot | 4 | 1 | 3 | |
| Surgical intervention | <0.001* | |||
| Conservative | 11 | 5 | 6 | |
| A.R.C catheter | 8 | 8 | 0 | |
| Venaseal | 2 | 2 | 0 | |
| NOAC | 12 | 0 | 12 | |
| Angioplasty | 2 | 0 | 2 |
| QFlow | Segments | SLU with Superficial Venous Reflux (Reflux Group, n = 15) | SLU without Superficial Venous Reflux (Nonreflux Group, n = 24) | Legs of Healthy Volunteer (HC Group, n = 28) | p Values of Pairwise Comparisons | ||
|---|---|---|---|---|---|---|---|
| Reflux and Nonreflux | Reflux and HC | Nonreflux and HC | |||||
| SV | IVC | 17.313 ± 6.029 | 16.437 ± 12.332 | 18.479 ± 6.518 | 0.823 | 0.599 | 0.475 |
| EIV | 5.651 ± 2.182 | 4.078 ± 2.717 | 3.849 ± 1.214 | 0.067 | 0.008 * | 0.705 | |
| FV | 1.738 ± 0.655 | 1.739 ± 1.260 | 1.234 ± 0.648 | 0.997 | 0.020 * | 0.085 | |
| PV | 1.109 ± 0.574 | 1.373 ± 1.050 | 0.599 ± 0.316 | 0.380 | 0.001 * | 0.002 * | |
| GSV | 0.681 ± 0.410 | 0.592 ± 0.604 | 0.379 ± 0.284 | 0.632 | 0.008 * | 0.157 | |
| FFV | IVC | 17.747 ± 5.699 | 17.321 ± 13.735 | 18.949 ± 6.485 | 0.921 | 0.581 | 0.596 |
| EIV | 5.736 ± 2.116 | 4.192 ± 2.859 | 4.033 ± 1.334 | 0.080 | 0.002 * | 0.805 | |
| FV | 1.743 ± 0.646 | 1.750 ± 1.257 | 1.256 ± 0.634 | 0.983 | 0.022 * | 0.090 | |
| PV | 1.117 ± 0.569 | 1.378 ± 1.049 | 0.611 ± 0.310 | 0.323 | <0.001 * | 0.002 * | |
| GSV | 0.687 ± 0.404 | 0.606 ± 0.596 | 0.392 ± 0.272 | 0.661 | 0.008 * | 0.147 | |
| BFV | IVC | 0.433 ± 0.938 | 0.884 ± 1.792 | 0.469 ± 0.968 | 0.435 | 0.914 | 0.322 |
| EIV | 0.085 ± 0.176 | 0.244 ± 0.580 | 0.182 ± 0.299 | 0.310 | 0.186 | 0.625 | |
| FV | 0.005 ± 0.018 | 0.010 ± 0.037 | 0.021 ± 0.043 | 0.583 | 0.094 | 0.365 | |
| PV | 0.007 ± 0.018 | 0.005 ± 0.021 | 0.010 ± 0.022 | 0.720 | 0.732 | 0.443 | |
| GSV | 0.005 ± 0.019 | 0.013 ± 0.036 | 0.015 ± 0.031 | 0.457 | 0.272 | 0.838 | |
| RF | IVC | 3.083 ± 6.540 | 3.319 ± 5.668 | 2.454 ± 4.982 | 0.919 | 0.741 | 0.601 |
| EIV | 2.044 ± 4.314 | 4.637 ± 9.739 | 3.887 ± 5.957 | 0.339 | 0.297 | 0.735 | |
| FV | 0.605 ± 2.344 | 1.189 ± 3.905 | 3.280 ± 6.963 | 0.605 | 0.073 | 0.181 | |
| PV | 1.203 ± 3.126 | 1.400 ± 5.556 | 3.906 ± 10.101 | 0.901 | 0.320 | 0.284 | |
| GSV | 1.562 ± 5.839 | 9.196 ± 19.809 | 11.890 ± 22.705 | 0.117 | 0.03 * | 0.671 | |
| ASV | IVC | 18.182 ± 5.508 | 18.206 ± 15.220 | 19.421 ± 6.595 | 0.996 | 0.572 | 0.714 |
| EIV | 5.815 ± 2.066 | 4.437 ± 2.920 | 4.219 ± 1.505 | 0.120 | 0.006 * | 0.744 | |
| FV | 1.748 ± 0.639 | 1.760 ± 1.255 | 1.279 ± 0.623 | 0.968 | 0.025 * | 0.097 | |
| PV | 1.127 ± 0.563 | 1.383 ± 1.049 | 0.622 ± 0.306 | 0.329 | <0.001 * | 0.002 * | |
| GSV | 0.693 ± 0.399 | 0.617 ± 0.593 | 0.408 ± 0.258 | 0.680 | 0.008 * | 0.152 | |
| MF | IVC | 21.117 ± 8.814 | 19.748 ± 12.251 | 20.986 ± 7.516 | 0.746 | 0.962 | 0.679 |
| EIV | 6.814 ± 3.331 | 4.797 ± 3.129 | 3.987 ± 1.213 | 0.064 | 0.006 * | 0.242 | |
| FV | 2.077 ± 0.904 | 1.994 ± 1.279 | 1.269 ± 0.682 | 0.829 | 0.002 * | 0.018 * | |
| PV | 1.346 ± 0.831 | 1.574 ± 1.141 | 0.606 ± 0.315 | 0.508 | 0.004 * | <0.001 * | |
| GSV | 0.781 ± 0.423 | 0.682 ± 0.662 | 0.394 ± 0.310 | 0.625 | 0.002 * | 0.083 | |
| SD | IVC | 9.384 ± 3.808 | 9.384 ± 3.808 | 10.294 ± 4.027 | 0.142 | 0.510 | 0.019 * |
| EIV | 7.740 ± 3.046 | 4.439 ± 3.921 | 3.629 ± 0.823 | 0.006 * | <0.001 * | 0.330 | |
| FV | 3.271 ± 1.241 | 3.938 ± 1.933 | 3.904 ± 3.068 | 0.242 | 0.345 | 0.964 | |
| PV | 1.551 ± 0.538 | 2.613 ± 1.450 | 1.166 ± 0.750 | 0.003 * | 0.087 | <0.001 * | |
| GSV | 2.896 ± 1.593 | 2.644 ± 2.052 | 1.941 ± 1.552 | 0.702 | 0.070 | 0.183 | |
| MV | IVC | 11.275 ± 5.008 | 9.424 ± 2.875 | 11.707 ± 4.477 | 0.228 | 0.789 | 0.074 |
| EIV | 8.640 ± 5.092 | 5.381 ± 4.504 | 14.584 ± 56.729 | 0.043 * | 0.689 | 0.432 | |
| FV | 3.836 ± 1.448 | 4.553 ± 2.052 | 4.111 ± 3.531 | 0.246 | 0.775 | 0.593 | |
| PV | 1.863 ± 0.792 | 2.996 ± 1.560 | 1.191 ± 0.814 | 0.013 * | 0.013 * | <0.001 * | |
| GSV | 3.483 ± 1.772 | 3.030 ± 2.137 | 1.982 ± 1.604 | 0.520 | 0.009 * | 0.058 | |
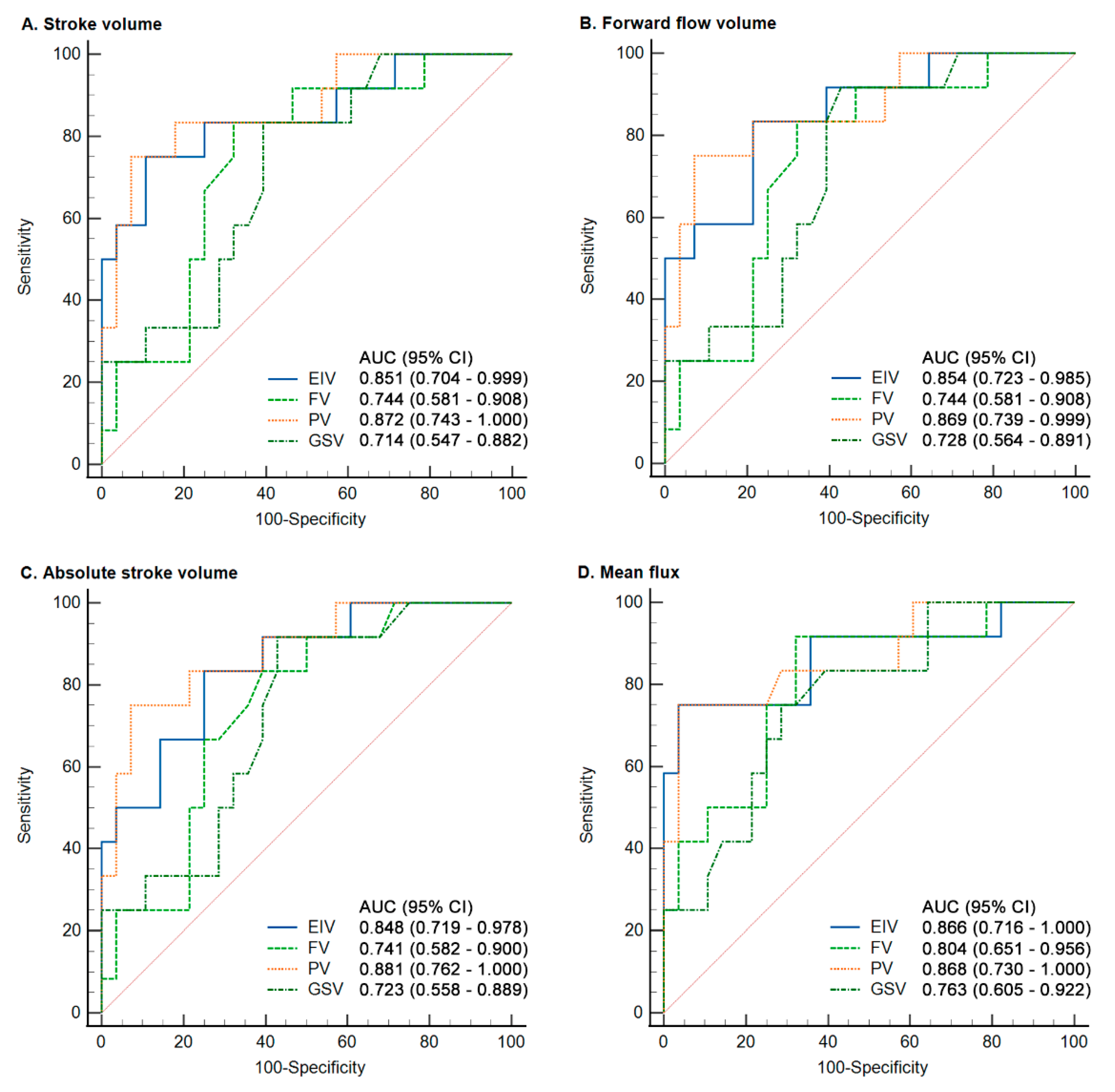
| Qflow | Segments | AUC | 95% CI | p-Value | Cutoff # | Sensitivity | Specificity |
|---|---|---|---|---|---|---|---|
| SV | EIV | 0.851 | 0.704 to 0.999 | <0.0001 | >5.23 | 75 | 89.29 |
| FV | 0.744 | 0.581 to 0.908 | 0.0034 | >1.37 | 83.33 | 67.86 | |
| PV | 0.872 | 0.743 to 1.000 | <0.0001 | >0.99 | 75 | 92.86 | |
| GSV | 0.714 | 0.547 to 0.882 | 0.0122 | >0.33 | 83.33 | 60.71 | |
| FFV | EIV | 0.854 | 0.723 to 0.985 | <0.0001 | >5.22 | 83.33 | 78.57 |
| FV | 0.744 | 0.581 to 0.908 | 0.0034 | >1.44 | 83.33 | 67.86 | |
| PV | 0.869 | 0.739 to 0.999 | <0.0001 | >0.99 | 75 | 92.86 | |
| GSV | 0.728 | 0.564 to 0.891 | 0.0064 | >0.33 | 91.67 | 57.14 | |
| ASV | EIV | 0.848 | 0.719 to 0.978 | <0.0001 | >5.31 | 83.33 | 75 |
| FV | 0.741 | 0.582 to 0.900 | 0.003 | >1.36 | 83.33 | 60.71 | |
| PV | 0.881 | 0.762 to 1.000 | <0.0001 | >1.01 | 75 | 92.86 | |
| GSV | 0.723 | 0.558 to 0.889 | 0.0082 | >0.33 | 91.67 | 57.14 | |
| MF | EIV | 0.866 | 0.716 to 1.000 | <0.0001 | >5.83 | 75 | 96.43 |
| FV | 0.804 | 0.651 to 0.956 | 0.0001 | >1.35 | 91.67 | 67.86 | |
| PV | 0.868 | 0.730 to 1.000 | <0.0001 | >1.11 | 75 | 96.43 | |
| GSV | 0.763 | 0.605 to 0.922 | 0.0011 | >0.45 | 75 | 71.43 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.-W.; Fang, Y.-F.; Tseng, Y.-H.; Wong, M.-Y.; Lin, Y.-H.; Hsu, Y.-C.; Lin, B.-S.; Huang, Y.-K. A Novel Tool for a Challenging Disease: Stasis Leg Ulcers Assessed Using QFlow in Triggered Angiography Noncontrast Enhanced Magnetic Resonance Imaging. J. Pers. Med. 2021, 11, 857. https://doi.org/10.3390/jpm11090857
Chen C-W, Fang Y-F, Tseng Y-H, Wong M-Y, Lin Y-H, Hsu Y-C, Lin B-S, Huang Y-K. A Novel Tool for a Challenging Disease: Stasis Leg Ulcers Assessed Using QFlow in Triggered Angiography Noncontrast Enhanced Magnetic Resonance Imaging. Journal of Personalized Medicine. 2021; 11(9):857. https://doi.org/10.3390/jpm11090857
Chicago/Turabian StyleChen, Chien-Wei, Yueh-Fu Fang, Yuan-Hsi Tseng, Min-Yi Wong, Yu-Hui Lin, Yin-Chen Hsu, Bor-Shyh Lin, and Yao-Kuang Huang. 2021. "A Novel Tool for a Challenging Disease: Stasis Leg Ulcers Assessed Using QFlow in Triggered Angiography Noncontrast Enhanced Magnetic Resonance Imaging" Journal of Personalized Medicine 11, no. 9: 857. https://doi.org/10.3390/jpm11090857
APA StyleChen, C.-W., Fang, Y.-F., Tseng, Y.-H., Wong, M.-Y., Lin, Y.-H., Hsu, Y.-C., Lin, B.-S., & Huang, Y.-K. (2021). A Novel Tool for a Challenging Disease: Stasis Leg Ulcers Assessed Using QFlow in Triggered Angiography Noncontrast Enhanced Magnetic Resonance Imaging. Journal of Personalized Medicine, 11(9), 857. https://doi.org/10.3390/jpm11090857