
The Risk of Bladder Cancer in Type 2 Diabetes Mellitus with Combination Therapy of SGLT-2 Inhibitors and Pioglitazone

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Patient Selection and Study Design
2.3. Exposure to the Study Drug
2.4. Covariates
2.5. Outcome Measurement
2.6. Statistical Analysis
3. Results
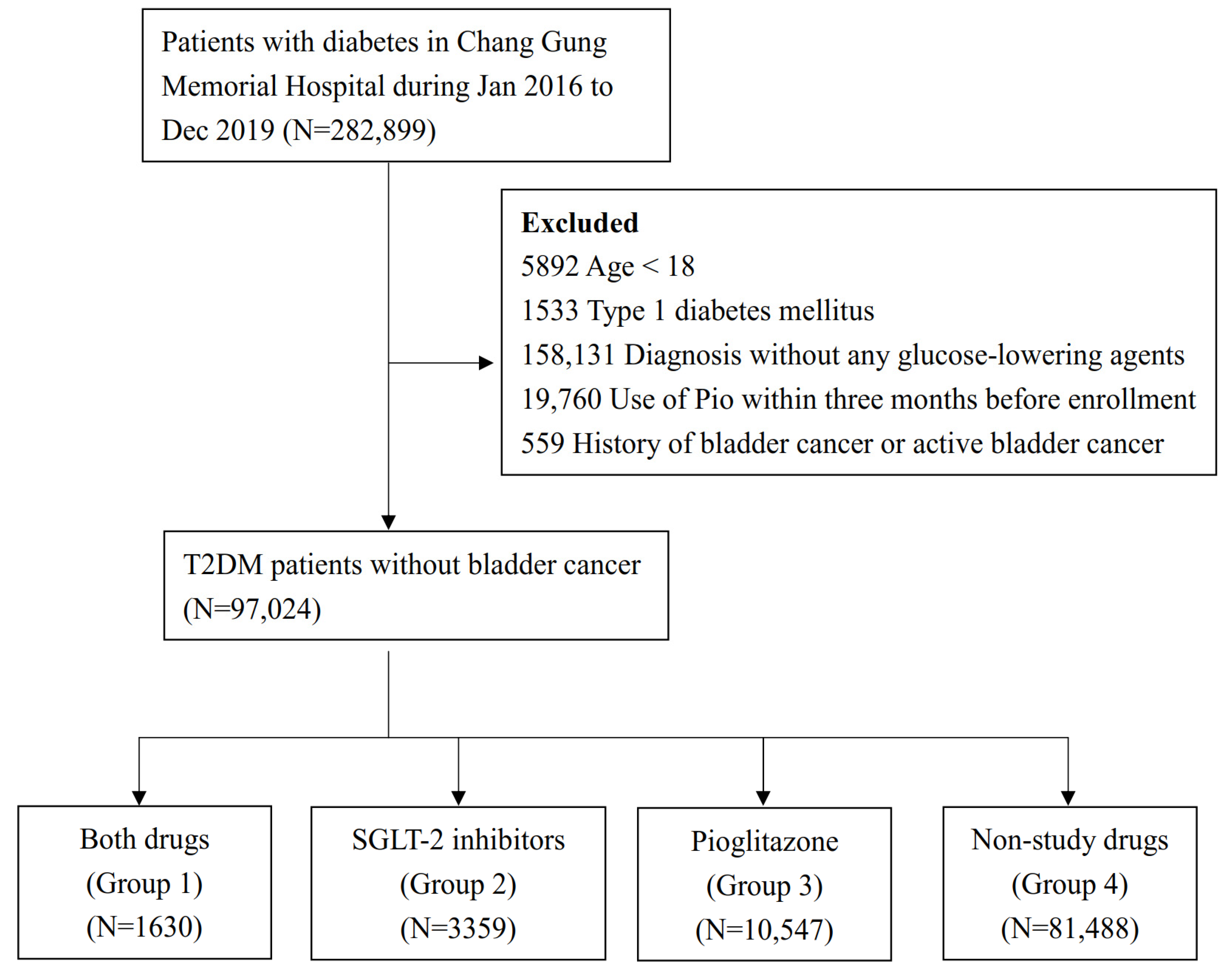
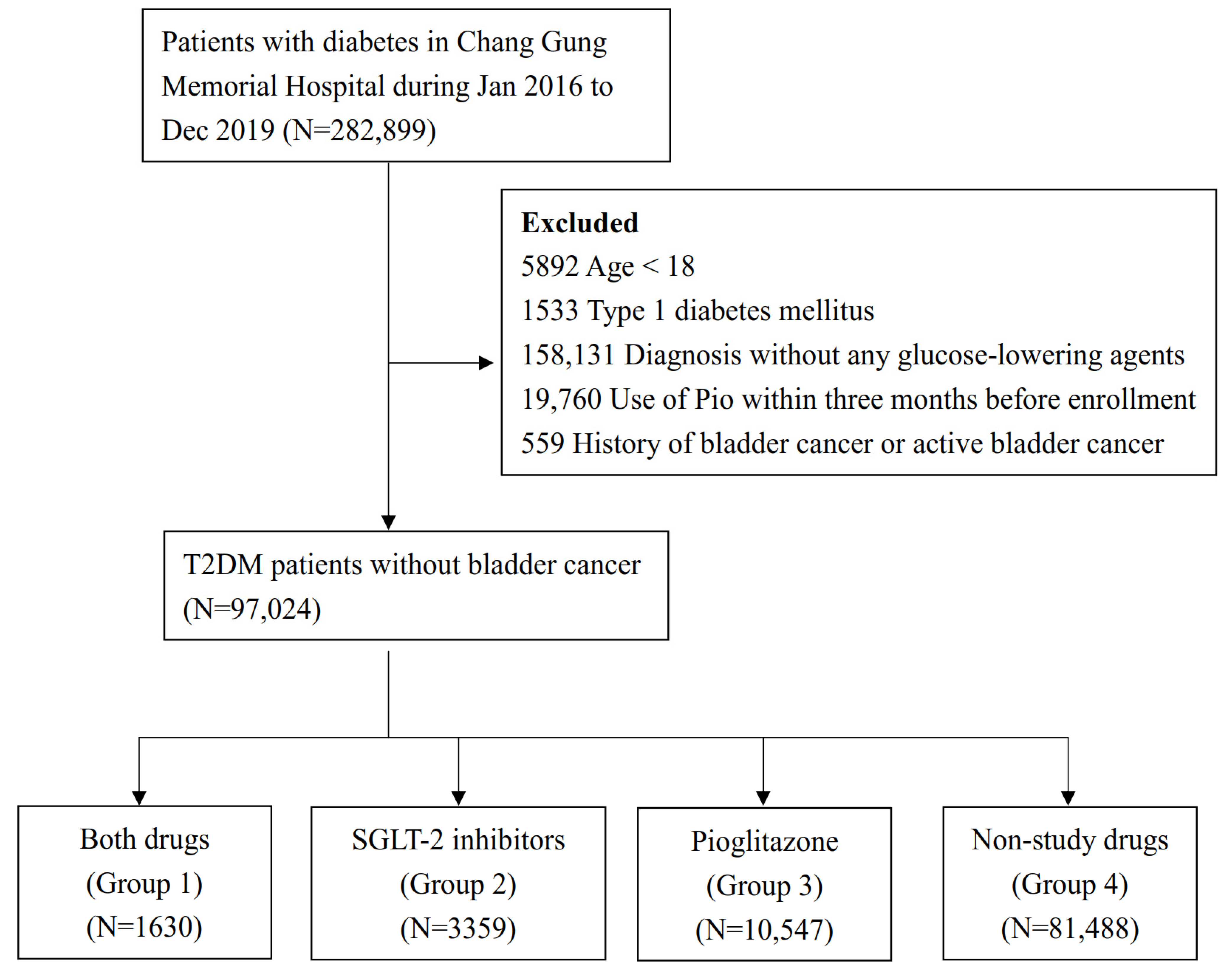
3.1. Study Patients
3.2. Baseline Characteristics
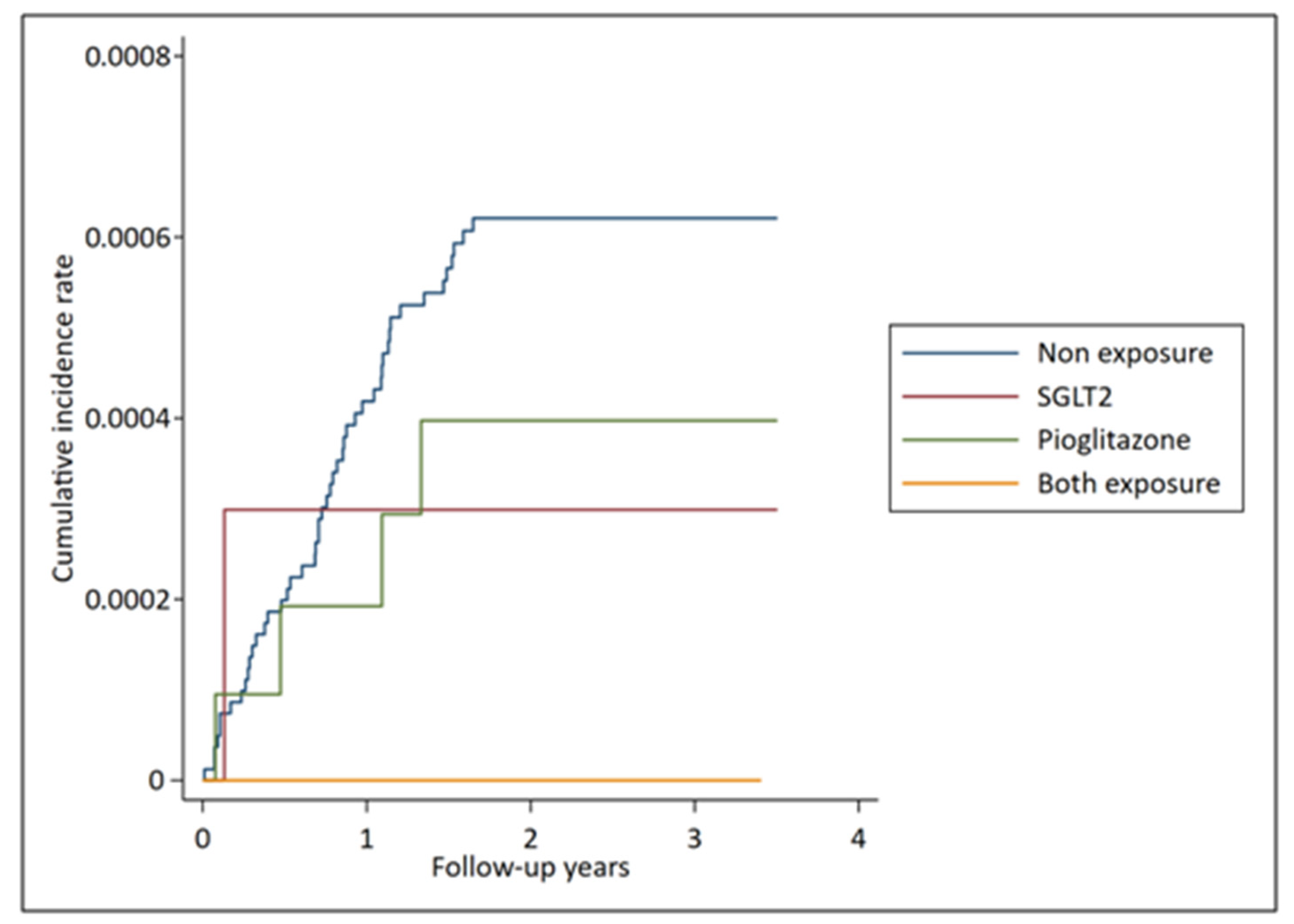
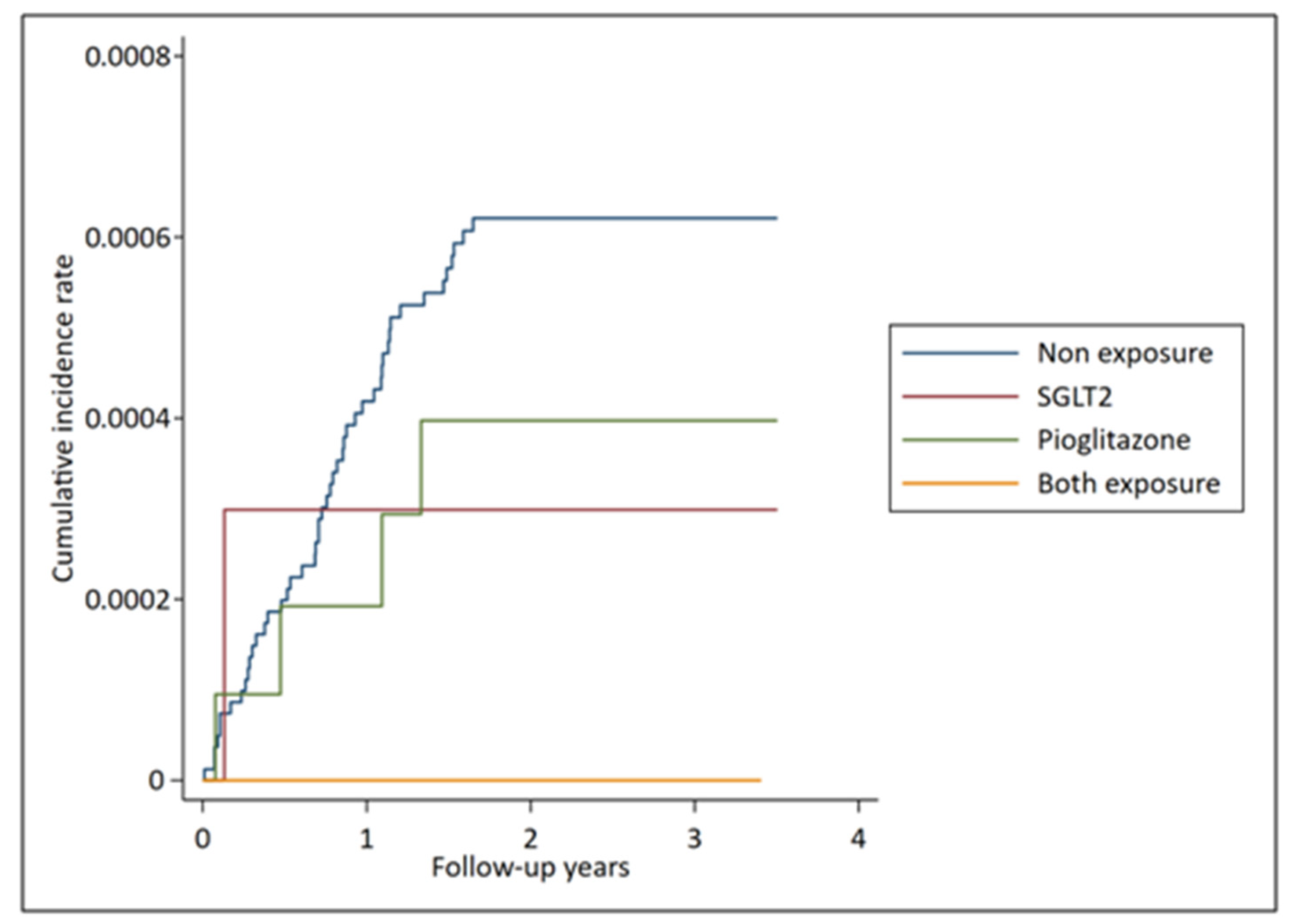
3.3. Primary and Secondary Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Juutilainen, A.; Lehto, S.; Rönnemaa, T.; Pyörälä, K.; Laakso, M. Type 2 Diabetes as a Coronary Heart Disease Equivalent: An 18-year prospective population-based study in Finnish subjects. Diabetes Care 2005, 28, 2901–2907. [Google Scholar] [CrossRef] [Green Version]
- Shah, A.D.; Langenberg, C.; Rapsomaniki, E.; Denaxas, S.; Rodriguez, M.P.; Gale, C.P.; Deanfield, J.; Smeeth, L.; Timmis, A.; Hemingway, H. Type 2 diabetes and incidence of cardiovascular diseases: A cohort study in 1·9 million people. Lancet Diabetes Endocrinol. 2015, 3, 105–113. [Google Scholar] [CrossRef] [Green Version]
- Emerging Risk Factors Collaboration; Sarwar, N.; Gao, P. Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: A collaborative meta-analysis of 102 prospective studies. Lancet 2010, 375, 2215–2222. [Google Scholar] [CrossRef] [Green Version]
- Zinman, B.; Wanner, C.; Lachin, J.M.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Devins, T.; Johansen, O.E.; Woerle, H.J.; et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N. Engl. J. Med. 2015, 373, 2117–2128. [Google Scholar] [CrossRef]
- Neal, B.; Perkovic, V.; Mahaffey, K.W.; De Zeeuw, D.; Fulcher, G.; Erondu, N.; Shaw, W.; Law, G.; Desai, M.; Matthews, D.R. Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes. N. Engl. J. Med. 2017, 377, 644–657. [Google Scholar] [CrossRef]
- Wiviott, S.D.; Raz, I.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Trimarco, B.; Zelniker, T.A.; Kuder, J.F.; Murphy, S.A.; et al. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2019, 380, 347–357. [Google Scholar] [CrossRef]
- McMurray, J.J.V.; Solomon, S.D.; Inzucchi, S.E. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N. Engl. J. Med. 2019, 381, 1995–2008. [Google Scholar] [CrossRef] [Green Version]
- Packer, M.; Anker, S.D.; Butler, J.; Filippatos, G.; Pocock, S.J.; Carson, P.; Januzzi, J.; Verma, S.; Tsutsui, H.; Brueckmann, M.; et al. Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure. N. Engl. J. Med. 2020, 383, 1413–1424. [Google Scholar] [CrossRef]
- Lee, M.; Saver, J.L.; Ovbiagele, B. Response by Lee et al to Letter Regarding Article, Pioglitazone for Secondary Stroke Prevention: A Systematic Review and Meta-Analysis. Stroke 2017, 48, e172. [Google Scholar] [CrossRef]
- Liu, C.-H.; Lee, T.-H.; Lin, Y.-S.; Sung, P.-S.; Wei, Y.-C.; Li, Y.-R. Pioglitazone and PPAR-γ modulating treatment in hypertensive and type 2 diabetic patients after ischemic stroke: A national cohort study. Cardiovasc. Diabetol. 2020, 19, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Lincoff, A.M.; Wolski, K.; Nicholls, S.J. Pioglitazone and risk of cardiovascular events in patients with type 2 diabetes mellitus: A meta-analysis of randomized trials. JAMA 2007, 12, 1180–1188. [Google Scholar] [CrossRef]
- Epstein, B.; Rosenwasser, R.; Sutton, D.; Choksi, R.; Sultan, S. SGLT-2 inhibitors and their potential in the treatment of diabetes. Diabetes Metab. Syndr. Obesity: Targets Ther. 2013, 6, 453–467. [Google Scholar] [CrossRef] [Green Version]
- Lewis, J.D.; Ferrara, A.; Peng, T.; Hedderson, M.; Bilker, W.B.; Quesenberry, C.P.; Vaughn, D.J.; Nessel, L.; Selby, J.; Strom, B.L. Risk of Bladder Cancer Among Diabetic Patients Treated with Pioglitazone: Interim report of a longitudinal cohort study. Diabetes Care 2011, 34, 916–922. [Google Scholar] [CrossRef] [Green Version]
- Shao, S.; Chan, Y.; Yang, Y.K.; Lin, S.; Hung, M.; Chien, R.; Lai, C.; Lai, E.C. The Chang Gung Research Database—A multi-institutional electronic medical records database for real-world epidemiological studies in Taiwan. Pharmacoepidemiol. Drug Saf. 2019, 28, 593–600. [Google Scholar] [CrossRef]
- Chen, T.-H.; Li, Y.-R.; Chen, S.-W.; Lin, Y.-S.; Sun, C.-C.; Chen, D.-Y.; Mao, C.-T.; Wu, M.; Chang, C.-H.; Chu, P.-H.; et al. Sodium-glucose cotransporter 2 inhibitor versus metformin as first-line therapy in patients with type 2 diabetes mellitus: A multi-institution database study. Cardiovasc. Diabetol. 2020, 19, 1–8. [Google Scholar] [CrossRef]
- Shao, S.-C.; Chang, K.-C.; Lin, S.-J.; Chien, R.-N.; Hung, M.-J.; Chan, Y.-Y.; Yang, Y.-H.K.; Lai, E.C.-C. Favorable pleiotropic effects of sodium glucose cotransporter 2 inhibitors: Head-to-head comparisons with dipeptidyl peptidase-4 inhibitors in type 2 diabetes patients. Cardiovasc. Diabetol. 2020, 19, 1–11. [Google Scholar] [CrossRef]
- Shao, S.C.; Chang, K.C.; Chien, R.N. Effects of sodium-glucose co-transporter-2 inhibitors on serum alanine aminotransferase levels in people with type 2 diabetes: A multi-institutional cohort study. Diabetes Obes. Metab. 2020, 22, 128–134. [Google Scholar] [CrossRef]
- Eberg, M.; Kahn, S.; Azoulay, L.; Tagalakis, V. Use of statins and reduced risk of recurrence of VTE in an older population. Thromb. Haemost. 2016, 115, 1220–1228. [Google Scholar] [CrossRef]
- Schmidt, M.; Cannegieter, S.C.; Johannesdottir, S.A. Statin use and venous thromboembolism recurrence: A combined na-tionwide cohort and nested case-control study. J. Thromb. Haemost. 2014, 12, 1207–1215. [Google Scholar] [CrossRef]
- Chen, D.; Li, Y.; Mao, C.; Tseng, C.; Hsieh, I.; Hung, M.; Chu, P.; Wang, C.; Wen, M.; Cherng, W.; et al. Cardiovascular outcomes of vildagliptin in patients with type 2 diabetes mellitus after acute coronary syndrome or acute ischemic stroke. J. Diabetes Investig. 2019, 11, 110–124. [Google Scholar] [CrossRef] [Green Version]
- Chen, T.-H.; Wang, C.-C.; Liu, C.-H.; Hsiao, C.-C.; Chen, S.-T.; Liu, F.-H.; Ho, M.-Y.; Li, Y.-R. Similar Cardiovascular Outcomes Between Insulin Detemir and Insulin Glargine In Type 2 Diabetic Patients With Extremely Atherosclerotic Cardiovascular Disease Risks. Endocr. Pr. 2020, 26, 818–829. [Google Scholar] [CrossRef]
- Dicembrini, I.; Nreu, B.; Mannucci, E. Sodium-glucose co-transporter-2 (SGLT-2) inhibitors and cancer: A meta-analysis of randomized controlled trials. Diabetes Obes. Metab. 2019, 21, 1871–1877. [Google Scholar] [CrossRef]
- García, M.; Arteche-Martinez, U.; Lertxundi, U.; Aguirre, C. SGLT2 Inhibitors and Bladder Cancer: Analysis of Cases Reported in the European Pharmacovigilance Database. J. Clin. Pharmacol. 2021, 61, 187–192. [Google Scholar] [CrossRef]
- Young, L.H.; Viscoli, C.M.; Schwartz, G.G. Heart Failure After Ischemic Stroke or Transient Ischemic Attack in Insu-lin-Resistant Patients Without Diabetes Mellitus Treated with Pioglitazone. Circulation 2018, 138, 1210–1220. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.D.; Habel, L.; Quesenberry, C.P.; Strom, B.L.; Peng, T.; Hedderson, M.M.; Ehrlich, S.; Mamtani, R.; Bilker, W.B.; Vaughn, D.J.; et al. Pioglitazone Use and Risk of Bladder Cancer and Other Common Cancers in Persons with Diabetes. JAMA 2015, 314, 265–277. [Google Scholar] [CrossRef]
- Ripamonti, E.; Azoulay, L.; Abrahamowicz, M.; Platt, R.; Suissa, S. A systematic review of observational studies of the association between pioglitazone use and bladder cancer. Diabet. Med. 2019, 36, 22–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silverii, G.A.; Monami, M.; Mannucci, E. Sodium-glucose co-transporter-2 inhibitors and all-cause mortality: A meta-analysis of randomized controlled trials. Diabetes Obes. Metab. 2021, 23, 1052–1056. [Google Scholar] [CrossRef]
- Dormandy, J.A.; Charbonnel, B.; Eckland, D.J.A.; Erdmann, E.; Massi-Benedetti, M.; Moules, I.K.; Skene, A.M.; Tan, M.H.; Lefèbvre, P.J.; Murray, G.D.; et al. Secondary prevention of macrovascular events in patients with type 2 diabetes in the PROactive Study (PROspectivepioglitAzone Clinical Trial In macroVascular Events): A randomised controlled trial. Lancet 2005, 366, 1279–1289. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Before Weighting | ASMD | ||||
|---|---|---|---|---|---|
| Variable | Both Drugs (N = 1630) | SGLT-2 Inhibitors (N = 3359) | Pioglitazone (N = 10,547) | Non-Study Drugs (N = 81,488) | |
| Age, years | 49.3 ± 10.5 | 50.3 ± 10.8 | 54.5 ± 10.5 | 58.0 ± 11.7 | 0.78 |
| Male sex | 959 (58.8) | 1839 (54.8) | 5958 (56.5) | 42,629 (52.3) | 0.13 |
| Hospital level | 0.17 | ||||
| Medical center | 1044 (64.1) | 1677 (49.9) | 6725 (63.8) | 45,367 (55.7) | |
| Regional/district hospital | 586 (36.0) | 1682 (50.1) | 3822 (36.2) | 36,121 (44.3) | |
| Diabetes duration, year | 10.5 ± 4.5 | 9.5 ± 4.6 | 10.8 ± 4.5 | 8.9 ± 4.7 | 0.41 |
| CCI | 0.41 | ||||
| 0 | 1044 (64.1) | 1923 (57.3) | 5681 (53.9) | 36,368 (44.6) | |
| 1 | 312 (19.1) | 823 (24.5) | 2273 (21.6) | 19,425 (23.8) | |
| 2+ | 274 (16.8) | 613 (18.3) | 2593 (24.6) | 25,695 (31.5) | |
| Comorbidity | |||||
| Previous stroke | 98 (6.0) | 205 (6.1) | 1286 (12.2) | 11,595 (14.2) | 0.28 |
| Gout | 64 (3.9) | 152 (4.5) | 512 (4.9) | 5061 (6.2) | 0.10 |
| Hypertension | 953 (58.5) | 2009 (59.8) | 6522 (61.8) | 50,879 (62.4) | 0.08 |
| Previous myocardial infarction | 26 (1.6) | 139 (4.1) | 219 (2.1) | 2767 (3.4) | 0.12 |
| Coronary artery disease | 249 (15.3) | 535 (15.9) | 1303 (12.4) | 11,573 (14.2) | 0.05 |
| Chronic kidney disease | 39 (2.4) | 87 (2.6) | 1018 (9.7) | 8292 (10.2) | 0.32 |
| COPD | 43 (2.6) | 93 (2.8) | 337 (3.2) | 3761 (4.6) | 0.11 |
| Dyslipidemia | 974 (59.8) | 2017 (60.1) | 5928 (56.2) | 39,531 (48.5) | 0.23 |
| Hx of malignancy (except for bladder cancer) | 91 (5.6) | 217 (6.5) | 730 (6.9) | 8298 (10.2) | 0.17 |
| Anti-hypertensive agents | |||||
| ACEI/ARB | 1030 (63.2) | 2147 (63.9) | 6892 (65.4) | 48,240 (59.2) | 0.13 |
| CCB | 346 (21.2) | 767 (22.8) | 2878 (27.3) | 26,386 (32.4) | 0.25 |
| Alpha-blocker | 123 (7.6) | 291 (8.7) | 1249 (11.8) | 11,224 (13.8) | 0.20 |
| Beta-blocker | 513 (31.5) | 1105 (32.9) | 3216 (30.5) | 26,045 (32.0) | 0.03 |
| Thiazide | 48 (2.9) | 68 (2.0) | 310 (2.9) | 2058 (2.5) | 0.03 |
| Loop diuretics | 88 (5.4) | 232 (6.9) | 1097 (10.4) | 9848 (12.1) | 0.24 |
| Spironolactone | 30 (1.8) | 102 (3.0) | 233 (2.2) | 2417 (3.0) | 0.07 |
| Anti-diabetic agents | |||||
| Biguanide (Metformin) | 1257 (77.1) | 2009 (59.8) | 5950 (56.4) | 38,961 (47.8) | 0.63 |
| Sulfonylurea | 1054 (64.7) | 2175 (64.8) | 6845 (64.9) | 37,759 (46.3) | 0.38 |
| Glinide | 60 (3.7) | 114 (3.4) | 553 (5.2) | 4952 (6.1) | 0.13 |
| DPP-4 I | 1222 (75.0) | 2348 (69.9) | 6066 (57.5) | 35,657 (43.8) | 0.67 |
| GLP-1 RA | 28 (1.7) | 74 (2.2) | 129 (1.2) | 445 (0.6) | 0.14 |
| Insulin | 303 (18.6) | 1088 (32.4) | 1964 (18.6) | 19,915 (24.4) | 0.18 |
| Alpha glucosidase inhibitors | 467 (28.7) | 823 (24.5) | 2243 (21.3) | 11,323 (13.9) | 0.37 |
| Other medications | |||||
| Aspirin | 576 (35.3) | 995 (29.6) | 3571 (33.9) | 24,275 (29.8) | 0.12 |
| Clopidogrel | 66 (4.1) | 220 (6.6) | 709 (6.7) | 6915 (8.5) | 0.18 |
| Cilostazol | 25 (1.5) | 59 (1.8) | 262 (2.5) | 2495 (3.1) | 0.10 |
| Statin | 987 (60.6) | 1998 (59.5) | 6331 (60.0) | 40,648 (49.9) | 0.22 |
| Fibrate | 177 (10.9) | 373 (11.1) | 1052 (10.0) | 6909 (8.5) | 0.09 |
| NSAIDs | 252 (15.5) | 665 (19.8) | 2055 (19.5) | 19,607 (24.1) | 0.22 |
| Steroid | 169 (10.4) | 396 (11.8) | 1524 (14.5) | 15,320 (18.8) | 0.24 |
| Lab (baseline) | |||||
| HbA1c, % | 8.5 ± 1.5 | 8.5 ± 1.6 | 7.7 ± 1.5 | 7.4 ± 1.4 | 0.73 |
| Creatinine | 0.9 ± 0.3 | 0.9 ± 0.3 | 1.3 ± 1.3 | 1.3 ± 1.6 | 0.39 |
| eGFR | 78.7 ± 17.3 | 78.2 ± 18.0 | 65.9 ± 23.8 | 65.4 ± 24.5 | 0.63 |
| ALT | 29.3 ± 22.7 | 32.9 ± 30.7 | 26.0 ± 37.0 | 29.0 ± 31.9 | 0.13 |
| Follow-up year | 2.8 ± 0.8 | 3.0 ± 0.6 | 2.9 ± 0.8 | 2.9 ± 0.7 | 0.21 |
| After Weighting | ASMD | ||||
|---|---|---|---|---|---|
| Variable | Both Drugs (N =1630) | SGLT-2 Inhibitors (N =3359) | Pioglitazone (N =10,547) | Non-Study Drugs (N =81,488) | |
| Age, years | 56.5 ± 10.5 | 56.1 ± 10.7 | 57.2 ± 11.3 | 57.2 ± 11.8 | 0.10 |
| Male sex | 55.2% | 54.0% | 54.4% | 53.0% | 0.04 |
| Hospital level | 0.12 | ||||
| Medical center | 50.4% | 58.5% | 53.5% | 56.5% | |
| Regional/district hospital | 49.6% | 41.5% | 46.5% | 43.5% | |
| Diabetes duration, year | 8.9 ± 4.5 | 8.9 ± 4.6 | 9.1 ± 4.8 | 9.2 ± 4.7 | 0.05 |
| CCI | 0.13 | ||||
| 0 | 50.4% | 48.2% | 44.7% | 46.5% | |
| 1 | 25.1% | 23.7% | 24.3% | 23.5% | |
| 2+ | 24.5% | 28.2% | 31.0% | 30.0% | |
| Comorbidity | |||||
| Previous stroke | 15.7% | 12.4% | 13.4% | 13.6% | 0.06 |
| Gout | 7.8% | 9.3% | 5.6% | 6.0% | 0.13 |
| Hypertension | 60.7% | 60.2% | 63.7% | 62.2% | 0.04 |
| Previous myocardial infarction | 2.9% | 3.8% | 3.3% | 3.3% | 0.03 |
| Coronary artery disease | 13.8% | 13.5% | 14.2% | 14.1% | 0.02 |
| Chronic kidney disease | 3.4% | 8.2% | 11.5% | 9.7% | 0.26 |
| COPD | 6.3% | 3.5% | 4.9% | 4.4% | 0.09 |
| Dyslipidemia | 53.5% | 48.6% | 49.0% | 49.9% | 0.07 |
| Hx of malignancy (except for bladder cancer) | 6.1% | 7.5% | 9.1% | 9.6% | 0.13 |
| Anti-hypertensive agents | |||||
| ACEI/ARB | 60.7% | 56.7% | 62.0% | 60.1% | 0.07 |
| CCB | 29.5% | 32.3% | 32.5% | 31.3% | 0.04 |
| Alpha-blocker | 14.2% | 13.2% | 14.3% | 13.3% | 0.03 |
| Beta-blocker | 33.1% | 29.5% | 33.3% | 31.9% | 0.05 |
| Thiazide | 2.8% | 2.7% | 2.3% | 2.6% | 0.02 |
| Loop diuretics | 11.6% | 12.2% | 12.4% | 11.6% | 0.02 |
| Spironolactone | 4.2% | 3.3% | 3.1% | 2.9% | 0.07 |
| Anti-diabetic agents | |||||
| Biguanide (Metformin) | 41.4% | 43.1% | 46.6% | 49.7% | 0.17 |
| Sulfonylurea | 64.3% | 49.6% | 51.5% | 49.5% | 0.30 |
| Glinide | 2.8% | 6.2% | 7.0% | 5.9% | 0.15 |
| DPP-4 I | 42.6% | 43.7% | 47.8% | 46.9% | 0.09 |
| GLP-1 RA | 0.9% | 0.8% | 0.8% | 0.7% | 0.02 |
| Insulin | 26.9% | 27.7% | 26.3% | 24.2% | 0.08 |
| Alpha glucosidase inhibitors | 15.4% | 19.5% | 16.9% | 15.4% | 0.11 |
| Other medications | |||||
| Aspirin | 27.5% | 29.4% | 30.6% | 30.3% | 0.06 |
| Clopidogrel | 11.8% | 6.4% | 8.6% | 8.2% | 0.12 |
| Cilostazol | 2.6% | 3.1% | 3.4% | 2.9% | 0.03 |
| Statin | 52.5% | 48.3% | 52.7% | 51.5% | 0.07 |
| Fibrate | 12.5% | 8.5% | 9.1% | 8.8% | 0.12 |
| NSAIDs including | 25.6% | 22.4% | 24.5% | 23.3% | 0.05 |
| Steroid | 16.0% | 17.7% | 19.8% | 17.9% | 0.05 |
| Lab (baseline) | |||||
| HbA1c, % | 8.1 ± 1.3 | 8.0 ± 1.8 | 7.6 ± 1.7 | 7.5 ± 1.6 | 0.42 |
| Creatinine | 1.0 ± 0.4 | 1.2 ± 1.0 | 1.4 ± 1.9 | 1.3 ± 1.6 | 0.24 |
| eGFR | 67.8 ± 19.4 | 66.2 ± 23.4 | 65.4 ± 25.8 | 66.2 ± 24.4 | 0.07 |
| ALT | 30.6 ± 22.1 | 30.0 ± 23.7 | 52.9 ± 223.5 | 28.9 ± 30.6 | 0.15 |
| Follow-up year | 2.8 ± 0.8 | 2.8 ± 0.8 | 2.8 ± 0.8 | 2.9 ± 0.7 | 0.06 |
| Exposure Status | No. of Patients | No. of Patients with Bladder Cancer (%) | AHR (95% CI) ab for Bladder Cancer | p Value | No. of Death (%) | AHR (95% CI) a for Death | p Value | ||
|---|---|---|---|---|---|---|---|---|---|
| No exposure | 81,488 | 48 | (0.06%) | 1.00 (Reference) | 4846 | (5.95%) | |||
| SGLT-2 I | 3359 | 1 | (0.03%) | 0.49 (0.05–4.94) | 0.546 | 62 | (1.85%) | 0.83 (0.70–0.99) | 0.034 |
| Pioglitazone | 10,547 | 4 | (0.04%) | 0.48 (0.15–1.58) | 0.227 | 413 | (3.92%) | 0.90 (0.83–0.99) | 0.024 |
| Both drugs | 1630 | 0 | (0%) | NA | NA | 33 | (2.02%) | 0.70 (0.54–0.92) | 0.010 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Y.-R.; Liu, C.-H.; Sun, W.-C.; Fan, P.-Y.; Liu, F.-H.; Chen, T.-H.; Wu, V.C.-C.; Lin, C.; Hsiao, C.-C. The Risk of Bladder Cancer in Type 2 Diabetes Mellitus with Combination Therapy of SGLT-2 Inhibitors and Pioglitazone. J. Pers. Med. 2021, 11, 828. https://doi.org/10.3390/jpm11090828
Li Y-R, Liu C-H, Sun W-C, Fan P-Y, Liu F-H, Chen T-H, Wu VC-C, Lin C, Hsiao C-C. The Risk of Bladder Cancer in Type 2 Diabetes Mellitus with Combination Therapy of SGLT-2 Inhibitors and Pioglitazone. Journal of Personalized Medicine. 2021; 11(9):828. https://doi.org/10.3390/jpm11090828
Chicago/Turabian StyleLi, Yan-Rong, Chi-Hung Liu, Wei-Chiao Sun, Pei-Yi Fan, Feng-Hsuan Liu, Tien-Hsing Chen, Victor Chien-Chia Wu, Chihung Lin, and Ching-Chung Hsiao. 2021. "The Risk of Bladder Cancer in Type 2 Diabetes Mellitus with Combination Therapy of SGLT-2 Inhibitors and Pioglitazone" Journal of Personalized Medicine 11, no. 9: 828. https://doi.org/10.3390/jpm11090828
APA StyleLi, Y.-R., Liu, C.-H., Sun, W.-C., Fan, P.-Y., Liu, F.-H., Chen, T.-H., Wu, V. C.-C., Lin, C., & Hsiao, C.-C. (2021). The Risk of Bladder Cancer in Type 2 Diabetes Mellitus with Combination Therapy of SGLT-2 Inhibitors and Pioglitazone. Journal of Personalized Medicine, 11(9), 828. https://doi.org/10.3390/jpm11090828