
Low Preoperative Antithrombin III Level Is Associated with Postoperative Acute Kidney Injury after Liver Transplantation

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
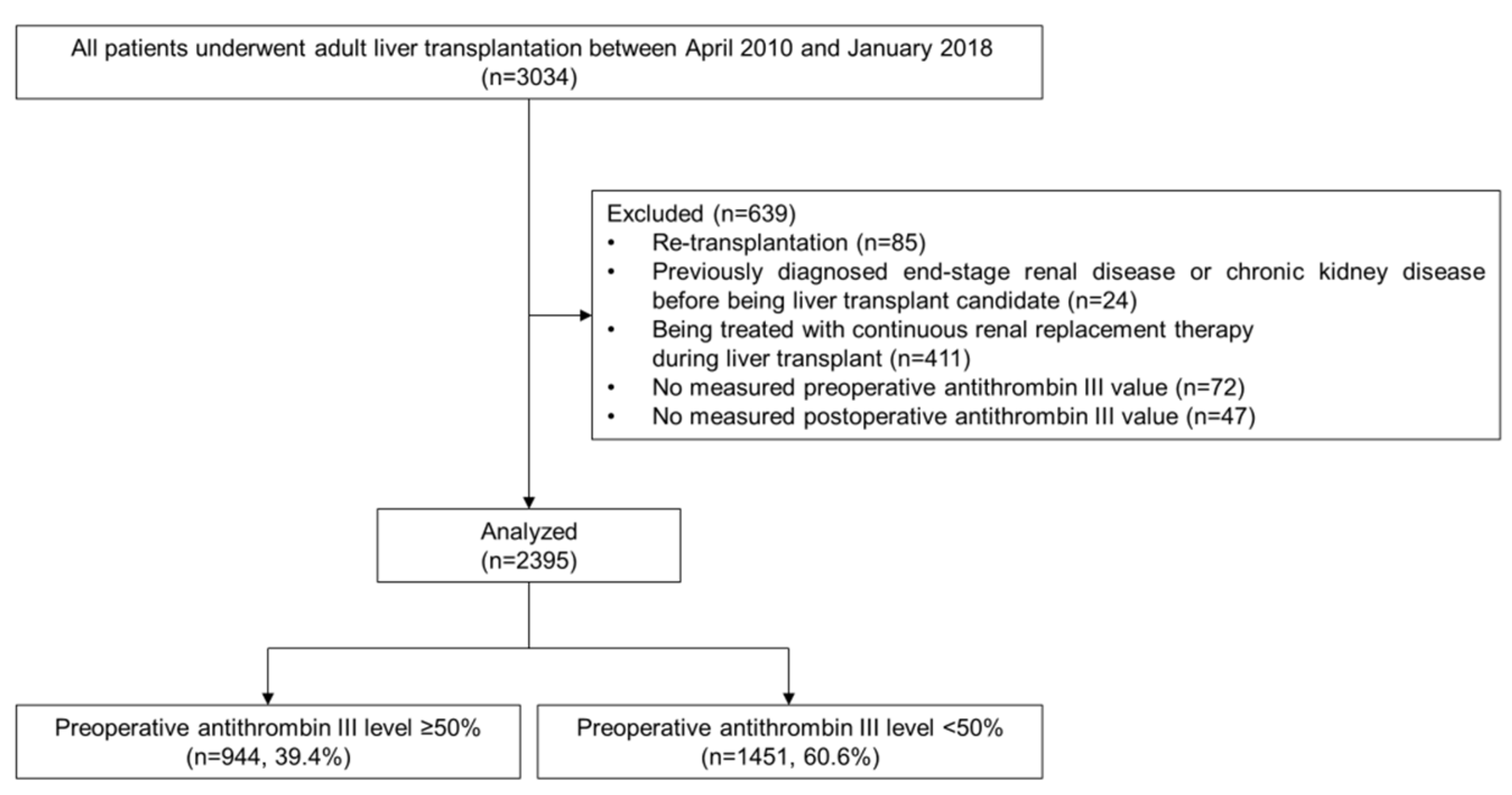
2.1. Study Population
2.2. Perioperative ATIII Administration and Measurement
2.3. Data Acquisition
2.4. Postoperative Outcomes
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Perioperative AT III Value
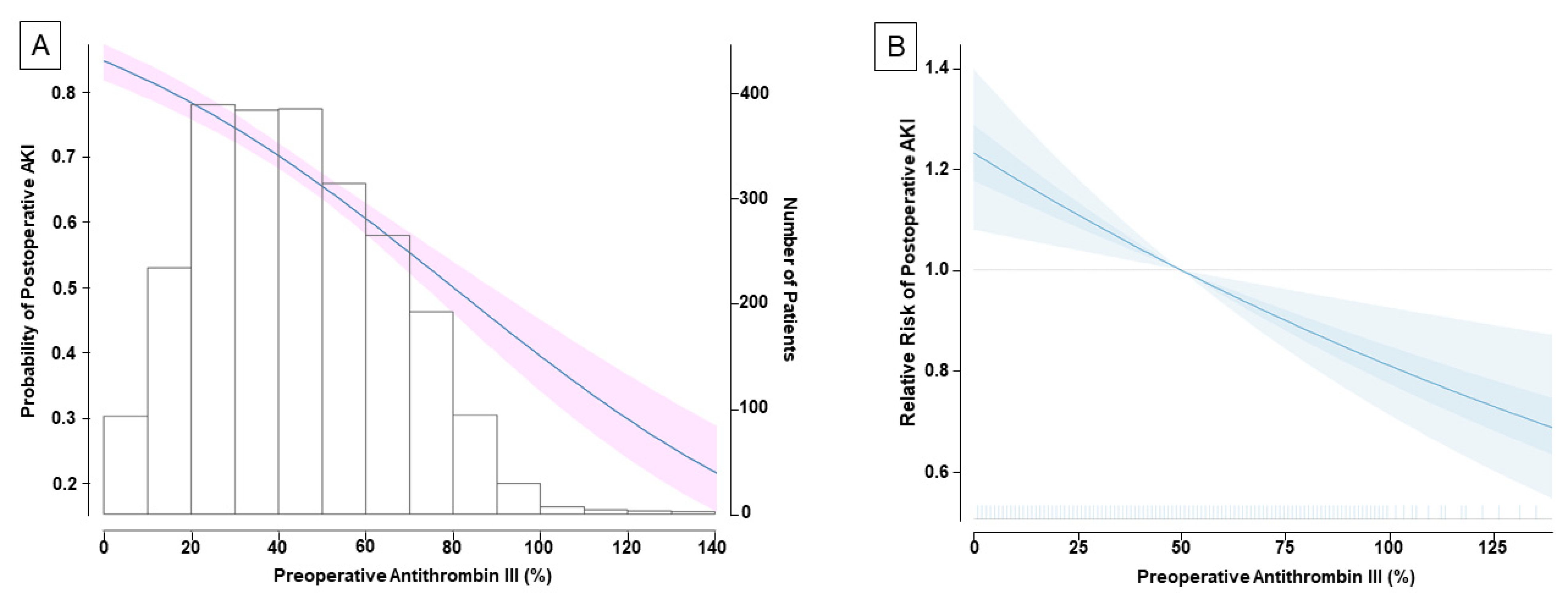
3.3. Incidence of Postoperative Acute Kidney Injury and Its Relationship with ATIII Value
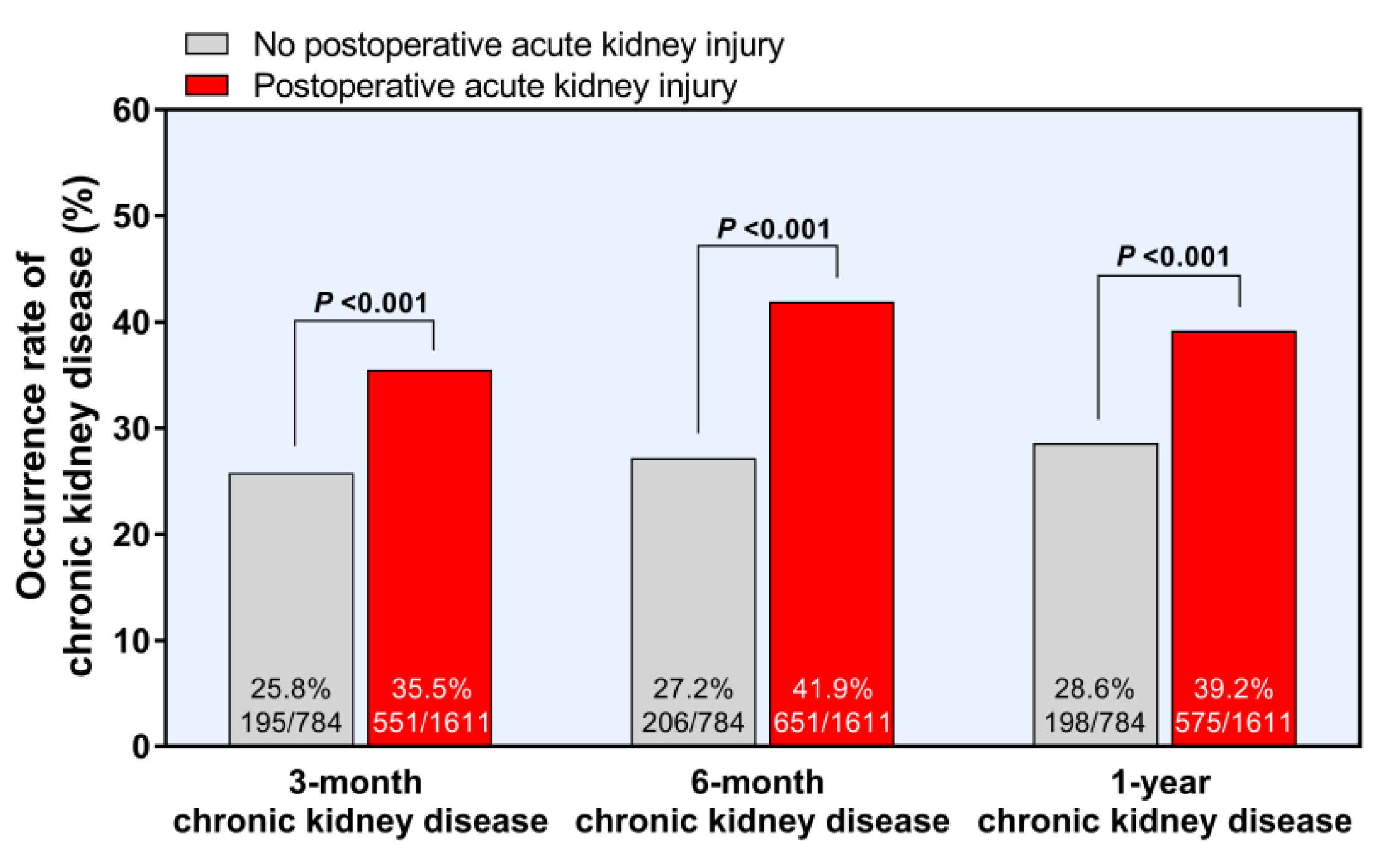
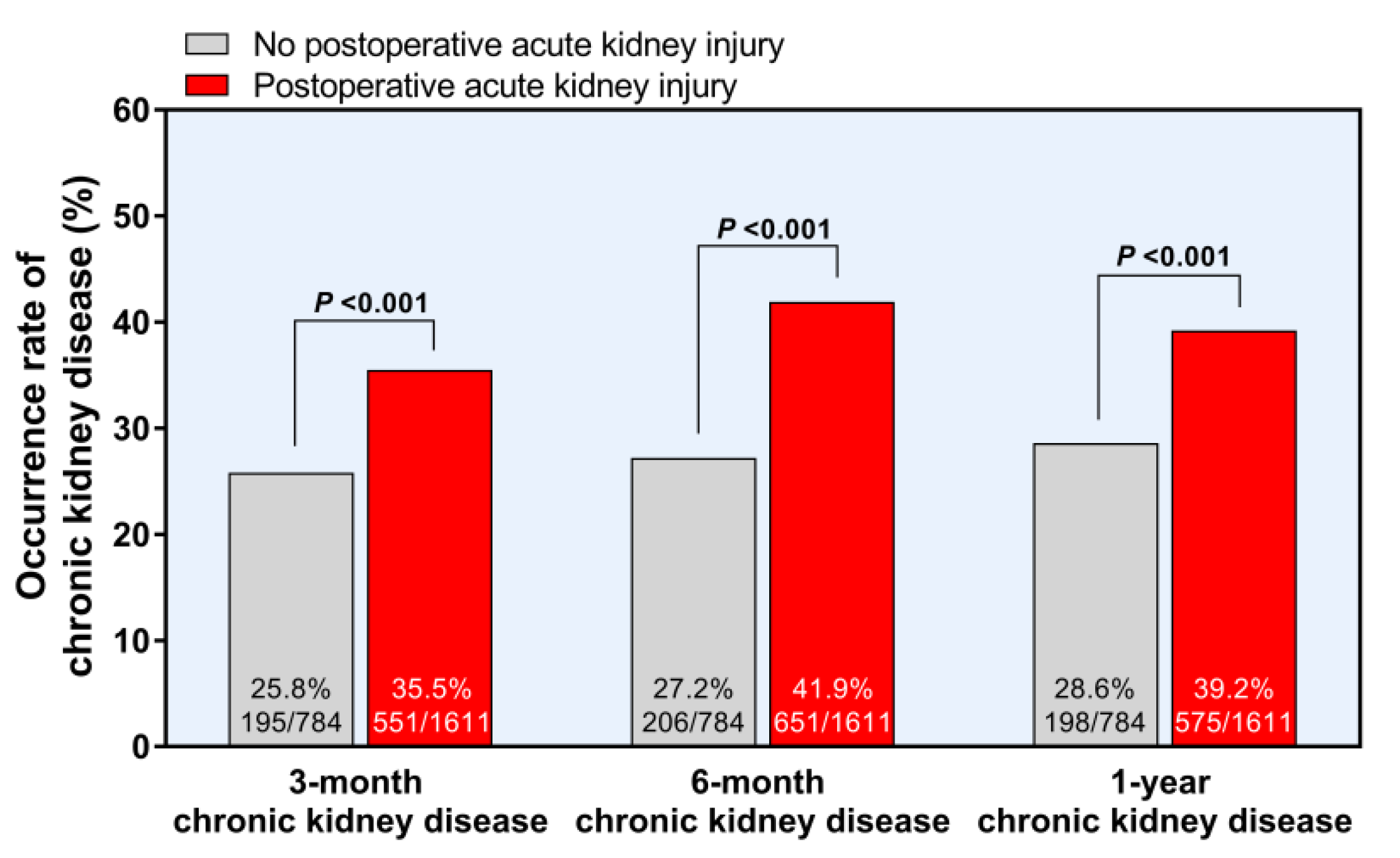
3.4. Development of Chronic Kidney Disease after Postoperative Acute Kidney Injury
3.5. Subgroup Analysis According to the MELD Scores and Donor Types
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chen, J.; Singhapricha, T.; Hu, K.Q.; Hong, J.C.; Steadman, R.H.; Busuttil, R.W.; Xia, V.W. Postliver transplant acute renal injury and failure by the RIFLE criteria in patients with normal pretransplant serum creatinine concentrations: A matched study. Transplantation 2011, 91, 348–353. [Google Scholar] [CrossRef]
- Hilmi, I.A.; Damian, D.; Al-Khafaji, A.; Planinsic, R.; Boucek, C.; Sakai, T.; Chang, C.C.; Kellum, J.A. Acute kidney injury following orthotopic liver transplantation: Incidence, risk factors, and effects on patient and graft outcomes. Br. J. Anaesth. 2015, 114, 919–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chawla, L.S.; Kimmel, P.L. Acute kidney injury and chronic kidney disease: An integrated clinical syndrome. Kidney Int. 2012, 82, 516–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inoue, Y.; Soyama, A.; Takatsuki, M.; Hidaka, M.; Muraoka, I.; Kanematsu, T.; Eguchi, S. Acute kidney injury following living donor liver transplantation. Clin. Transplant. 2012, 26, E530–E535. [Google Scholar] [CrossRef]
- Rahman, S.; Davidson, B.R.; Mallett, S.V. Early acute kidney injury after liver transplantation: Predisposing factors and clinical implications. World J. Hepatol. 2017, 9, 823–832. [Google Scholar] [CrossRef] [PubMed]
- Claria, J.; Stauber, R.E.; Coenraad, M.J.; Moreau, R.; Jalan, R.; Pavesi, M.; Amoros, A.; Titos, E.; Alcaraz-Quiles, J.; Oettl, K.; et al. Systemic inflammation in decompensated cirrhosis: Characterization and role in acute-on-chronic liver failure. Hepatology 2016, 64, 1249–1264. [Google Scholar] [CrossRef] [Green Version]
- Chae, M.S.; Kim, Y.; Chung, H.S.; Park, C.S.; Lee, J.; Choi, J.H.; Hong, S.H. Predictive Role of Serum Cytokine Profiles in Acute Kidney Injury after Living Donor Liver Transplantation. Mediat. Inflamm. 2018, 2018, 8256193. [Google Scholar] [CrossRef] [Green Version]
- Levy, J.H.; Sniecinski, R.M.; Welsby, I.J.; Levi, M. Antithrombin: Anti-inflammatory properties and clinical applications. Thromb. Haemost. 2016, 115, 712–728. [Google Scholar] [CrossRef]
- Hashikura, Y.; Kawasaki, S.; Okumura, N.; Ishikawa, S.; Matsunami, H.; Ikegami, T.; Nakazawa, Y.; Makuuchi, M. Prevention of hepatic artery thrombosis in pediatric liver transplantation. Transplantation 1995, 60, 1109–1112. [Google Scholar] [CrossRef]
- Kawanaka, H.; Akahoshi, T.; Kinjo, N.; Konishi, K.; Yoshida, D.; Anegawa, G.; Yamaguchi, S.; Uehara, H.; Hashimoto, N.; Tsutsumi, N.; et al. Impact of antithrombin III concentrates on portal vein thrombosis after splenectomy in patients with liver cirrhosis and hypersplenism. Ann. Surg. 2010, 251, 76–83. [Google Scholar] [CrossRef]
- Wang, F.; Zhang, G.; Lu, Z.; Geurts, A.M.; Usa, K.; Jacob, H.J.; Cowley, A.W.; Wang, N.; Liang, M. Antithrombin III/SerpinC1 insufficiency exacerbates renal ischemia/reperfusion injury. Kidney Int. 2015, 88, 796–803. [Google Scholar] [CrossRef] [Green Version]
- Yin, J.; Wang, F.; Kong, Y.; Wu, R.; Zhang, G.; Wang, N.; Wang, L.; Lu, Z.; Liang, M. Antithrombin III prevents progression of chronic kidney disease following experimental ischaemic-reperfusion injury. J. Cell. Mol. Med. 2017, 21, 3506–3514. [Google Scholar] [CrossRef]
- Knot, E.; Ten Cate, J.W.; Drijfhout, H.R.; Kahlé, L.H.; Tytgat, G.N. Antithrombin III metabolism in patients with liver disease. J. Clin. Pathol. 1984, 37, 523–530. [Google Scholar] [CrossRef] [Green Version]
- Goren, O.; Matot, I. Perioperative acute kidney injury. Br. J. Anaesth. 2015, 115 (Suppl. S2), ii3–ii14. [Google Scholar] [CrossRef] [Green Version]
- Rabb, H.; Griffin, M.D.; McKay, D.B.; Swaminathan, S.; Pickkers, P.; Rosner, M.H.; Kellum, J.A.; Ronco, C.; Acute Dialysis Quality Initiative Consensus, X.W.G. Inflammation in AKI: Current Understanding, Key Questions, and Knowledge Gaps. J. Am. Soc. Nephrol. 2016, 27, 371–379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inker, L.A.; Astor, B.C.; Fox, C.H.; Isakova, T.; Lash, J.P.; Peralta, C.A.; Kurella Tamura, M.; Feldman, H.I. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD. Am. J. Kidney Dis. 2014, 63, 713–735. [Google Scholar] [CrossRef] [Green Version]
- Levey, A.S.; de Jong, P.E.; Coresh, J.; El Nahas, M.; Astor, B.C.; Matsushita, K.; Gansevoort, R.T.; Kasiske, B.L.; Eckardt, K.U. The definition, classification, and prognosis of chronic kidney disease: A KDIGO Controversies Conference report. Kidney Int. 2011, 80, 17–28. [Google Scholar] [CrossRef] [Green Version]
- Olthoff, K.M.; Kulik, L.; Samstein, B.; Kaminski, M.; Abecassis, M.; Emond, J.; Shaked, A.; Christie, J.D. Validation of a current definition of early allograft dysfunction in liver transplant recipients and analysis of risk factors. Liver Transpl. 2010, 16, 943–949. [Google Scholar] [CrossRef] [PubMed]
- Wu, R.; Kong, Y.; Yin, J.; Liang, R.; Lu, Z.; Wang, N.; Zhao, Q.; Zhou, Y.; Yan, C.; Wang, F.; et al. Antithrombin is a Novel Predictor for Contrast Induced Nephropathy After Coronary Angiography. Kidney Blood Press. Res. 2018, 43, 170–180. [Google Scholar] [CrossRef]
- Lu, Z.; Cheng, D.; Yin, J.; Wu, R.; Zhang, G.; Zhao, Q.; Wang, N.; Wang, F.; Liang, M. Antithrombin III Protects against Contrast-Induced Nephropathy. EBioMedicine 2017, 17, 101–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.; Cho, S.; Cho, Y.J.; Choi, H.J.; Hong, S.H.; Chae, M.S. Predictive Utility of Antithrombin III in Acute Kidney Injury in Living-Donor Liver Transplantation: A Retrospective Observational Cohort Study. Transplant. Proc. 2020. [Google Scholar] [CrossRef]
- Park, M.H.; Shim, H.S.; Kim, W.H.; Kim, H.J.; Kim, D.J.; Lee, S.H.; Kim, C.S.; Gwak, M.S.; Kim, G.S. Clinical Risk Scoring Models for Prediction of Acute Kidney Injury after Living Donor Liver Transplantation: A Retrospective Observational Study. PLoS ONE 2015, 10, e0136230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaneko, J.; Sugawara, Y.; Tamura, S.; Togashi, J.; Matsui, Y.; Makuuchi, M. Antithrombin effect on coagulation and fibrinolytic profiles after living donor liver transplantation: A pilot study. Int. J. Lab. Hematol. 2009, 31, 81–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fourrier, F.; Chopin, C.; Goudemand, J.; Hendrycx, S.; Caron, C.; Rime, A.; Marey, A.; Lestavel, P. Septic shock, multiple organ failure, and disseminated intravascular coagulation. Compared patterns of antithrombin III, protein C, and protein S deficiencies. Chest 1992, 101, 816–823. [Google Scholar] [CrossRef]
- Hilmi, I.A.; Damian, D.; Al-Khafaji, A.; Sakai, T.; Donaldson, J.; Winger, D.G.; Kellum, J.A. Acute kidney injury after orthotopic liver transplantation using living donor versus deceased donor grafts: A propensity score-matched analysis. Liver Transpl. 2015, 21, 1179–1185. [Google Scholar] [CrossRef] [Green Version]
- Weber, M.L.; Ibrahim, H.N.; Lake, J.R. Renal dysfunction in liver transplant recipients: Evaluation of the critical issues. Liver Transpl. 2012, 18, 1290–1301. [Google Scholar] [CrossRef] [PubMed]
- Abelha, F.J.; Botelho, M.; Fernandes, V.; Barros, H. Determinants of postoperative acute kidney injury. Crit. Care 2009, 13, R79. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Antithrombin III < 50% (N = 1451, 60.6%) | Antithrombin III ≥ 50 % (N = 944, 39.4%) | Total (N = 2395) | p Value | |
|---|---|---|---|---|
| Demographic data | ||||
| Age (years) | 52.8 ± 8.6 | 53.5 ± 8.2 | 53.1 ± 8.5 | 0.036 |
| Sex (male sex) | 1059 (73.0%) | 730 (77.3%) | 1789 (74.7%) | 0.019 |
| Body mass index (m/kg2) | 24.0 ± 3.7 | 23.8 ± 3.2 | 23.9 ± 3.5 | 0.304 |
| Diabetes | 350 (24.1%) | 207 (21.9%) | 557 (23.3%) | 0.233 |
| Hypertension | 191 (13.2%) | 203 (21.5%) | 394 (16.5%) | <0.001 |
| Coronary artery disease | 13 (0.9%) | 13 (1.4%) | 26 (1.1%) | 0.363 |
| MELD score | 16 (12–23) | 8.5 (7–11) | 13 (9–18) | <0.001 |
| MELD score over 20 | 462 (31.8%) | 19 (2.0%) | 481 (20.1%) | <0.001 |
| Causes for liver transplant | <0.001 | |||
| HBV-related liver cirrhosis | 526 (67.1%) | 922 (57.2%) | 1448 (60.5%) | |
| HCV-related liver cirrhosis | 42 (5.4%) | 123 (7.6%) | 165 (6.9%) | |
| Alcoholic liver cirrhosis | 118 (15.1%) | 327 (20.3%) | 445 (18.6%) | |
| Others | 98 (12.5%) | 239 (14.8%) | 337 (14.1%) | |
| Hepatocellular carcinoma | 452 (57.7%) | 782 (48.5%) | 1234 (51.5%) | |
| Comorbidities | ||||
| Varix bleeding | 386 (26.6%) | 248 (26.3%) | 634 (26.5%) | 0.895 |
| Hepatic encephalopathy | 273 (18.8%) | 22 (2.3%) | 295 (12.3%) | <0.001 |
| Pleural effusion | 252 (17.4%) | 51 (5.4%) | 303 (12.7%) | <0.001 |
| Preoperative laboratory variables | ||||
| Antithrombin III (%) | 30.2 ± 11.8 | 67.1 ± 13.2 | 44.8 ± 21.9 | <0.001 |
| Platelet count (×103/µL) | 65.3 ± 43.1 | 90.3 ± 58.4 | 75.1 ± 51.2 | <0.001 |
| Total bilirubin (mg/dL) | 8.3 ± 10.5 | 1.8 ± 4.0 | 5.7 ± 9.1 | <0.001 |
| Albumin (g/dL) | 3.0 ± 0.6 | 3.4 ± 0.5 | 3.1 ± 0.6 | <0.001 |
| Prothrombin time (INR) | 1.9 ± 1.2 | 1.2 ± 0.2 | 1.6 ± 1.0 | <0.001 |
| Creatinine (mg/dL) | 0.8 ± 0.5 | 0.8 ± 0.3 | 0.8 ± 0.4 | 0.502 |
| C-reactive protein (mg/L) | 0.8 ± 1.1 | 0.4 ± 0.9 | 0.7 ± 1.1 | <0.001 |
| Operative variables | ||||
| Deceased donor | 149 (10.3%) | 15 (1.6%) | 164 (6.8%) | <0.001 |
| Living donor | 762 (97.2%) | 1469 (91.2%) | 2231 (93.2%) | 0.001 |
| Duration of surgery (min) | 800.2 ± 151.0 | 758.0 ± 135.2 | 783.6 ± 146.4 | <0.001 |
| Graft-to-recipient weight ratio (g/kg) | 1.2 ± 0.5 | 1.1 ± 0.3 | 1.2 ± 0.4 | <0.001 |
| Total ischemic time (min) | 147.5 ± 71.7 | 130.5 ± 53.4 | 140.8 ± 65.6 | <0.001 |
| Transfusion | ||||
| pRBC (unit) | 10.4 ± 14.7 | 3.4 ± 6.8 | 7.7 ± 12.7 | <0.001 |
| * Massive transfusion | 535 (36.9%) | 104 (11.0%) | 639 (26.7%) | <0.001 |
| FFP (unit) | 10.8 ± 14.9 | 3.5 ± 7.0 | 7.9 ± 12.9 | <0.001 |
| Cryoprecipitate (unit) | 8.1 ± 8.9 | 2.8 ± 5.2 | 6.0 ± 8.1 | <0.001 |
| Platelet apheresis (unit) | 0.8 ± 1.0 | 0.3 ± 0.6 | 0.6 ± 0.9 | <0.001 |
| Tacrolimus trough level within POD 7 | 5.2 ± 2.6 | 6.0 ± 2.5 | 5.5 ± 2.6 | <0.001 |
| Preoperative Antithrombin III < 50% (N = 1451) | Preoperative Anithrombin III ≥ 50% (N = 944) | Total (N = 2395) | p Value | |
|---|---|---|---|---|
| Postoperative renal outcomes | ||||
| Acute kidney injury | 1095 (75.5%) | 516 (54.7%) | 1611 (67.3%) | <0.001 |
| Grades of acute kidney injury | <0.001 | |||
| 1 | 970 (66.9%) | 472 (50.0%) | 1442 (60.2%) | <0.001 |
| 2 | 49 (3.4%) | 34 (3.6%) | 83 (3.5%) | 0.858 |
| 3 | 76 (5.2%) | 10 (1.1%) | 86 (3.6%) | <0.001 |
| Chronic kidney disease | ||||
| At 3 months after liver transplant | 474 (34.1%) | 272 (29.6%) | 746 (32.3%) | 0.029 |
| At 6 months after liver transplant | 551 (39.6%) | 306 (33.3%) | 857 (37.1%) | 0.003 |
| At 1 year after liver transplant | 490 (37.6%) | 283 (33.1%) | 773 (35.8%) | 0.036 |
| Other postoperative outcomes | ||||
| Early allograft dysfunction | 222 (15.3%) | 38 (4.0%) | 260 (10.9%) | <0.001 |
| Overall graft failure | 115 (7.9%) | 67 (7.1%) | 182 (7.6%) | 0.504 |
| Overall mortality | 109 (7.5%) | 63 (6.7%) | 172 (7.2%) | 0.487 |
| All Patients (N = 2395) | ||||
|---|---|---|---|---|
| Crude OR (95% CI) | p Value | Multivariate OR (95% CI) | p Value | |
| Preoperative antithrombin III (per 10% increase) | 0.81 (0.78–0.84) | <0.001 | 0.86 (0.81–0.92) | <0.001 |
| Age | 1.00 (1.00–1.01) | 0.257 | ||
| Female sex | 1.23 (1.01–1.51) | 0.041 | 1.26 (1.01–1.57) | 0.035 |
| Body mass index | 1.09 (1.07–1.12) | <0.001 | 1.09 (1.06–1.12) | <0.001 |
| Diabetes mellitus | 1.30 (1.06–1.61) | 0.012 | ||
| Hypertension | 1.22 (0.96–1.54) | 0.101 | ||
| Hepatic encephalopathy | 1.66 (1.25–2.20) | <0.001 | ||
| MELD score | 1.04 (1.03–1.06) | <0.001 | ||
| Albumin | 0.50 (0.43–0.58) | <0.001 | 0.62 (0.53–0.74) | <0.001 |
| C-reactive protein | 1.15 (1.05–1.26) | 0.003 | ||
| Deceased-donor LT | 3.35 (2.12–5.29) | <0.001 | 6.69 (3.22–13.93) | <0.001 |
| Operation time (per hour increase) | 1.14 (1.10–1.19) | <0.001 | 1.14 (1.09–1.20) | <0.001 |
| pRBC transfusion(per 5 units) | 1.20 (1.14–1.27) | <0.001 | 1.08 (1.02–1.14) | 0.009 |
| Graft-to-recipient weight ratio | 1.21 (0.98–1.49) | 0.082 | ||
| Total ischemic time (per 10 min) | 1.04 (1.02–1.05) | <0.001 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, K.-S.; Moon, Y.-J.; Kim, S.-H.; Kim, B.; Jun, I.-G.; Kwon, H.-M.; Song, J.-G.; Hwang, G.-S. Low Preoperative Antithrombin III Level Is Associated with Postoperative Acute Kidney Injury after Liver Transplantation. J. Pers. Med. 2021, 11, 716. https://doi.org/10.3390/jpm11080716
Kim K-S, Moon Y-J, Kim S-H, Kim B, Jun I-G, Kwon H-M, Song J-G, Hwang G-S. Low Preoperative Antithrombin III Level Is Associated with Postoperative Acute Kidney Injury after Liver Transplantation. Journal of Personalized Medicine. 2021; 11(8):716. https://doi.org/10.3390/jpm11080716
Chicago/Turabian StyleKim, Kyoung-Sun, Young-Jin Moon, Sung-Hoon Kim, Bomi Kim, In-Gu Jun, Hye-Mee Kwon, Jun-Gol Song, and Gyu-Sam Hwang. 2021. "Low Preoperative Antithrombin III Level Is Associated with Postoperative Acute Kidney Injury after Liver Transplantation" Journal of Personalized Medicine 11, no. 8: 716. https://doi.org/10.3390/jpm11080716
APA StyleKim, K.-S., Moon, Y.-J., Kim, S.-H., Kim, B., Jun, I.-G., Kwon, H.-M., Song, J.-G., & Hwang, G.-S. (2021). Low Preoperative Antithrombin III Level Is Associated with Postoperative Acute Kidney Injury after Liver Transplantation. Journal of Personalized Medicine, 11(8), 716. https://doi.org/10.3390/jpm11080716