
Evaluation of Social Cognition Measures for Japanese Patients with Schizophrenia Using an Expert Panel and Modified Delphi Method

 , , , , , ,
, , , , , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Expert Panel Members
2.2. Key Discussion Points and Candidate Social Cognition Measures
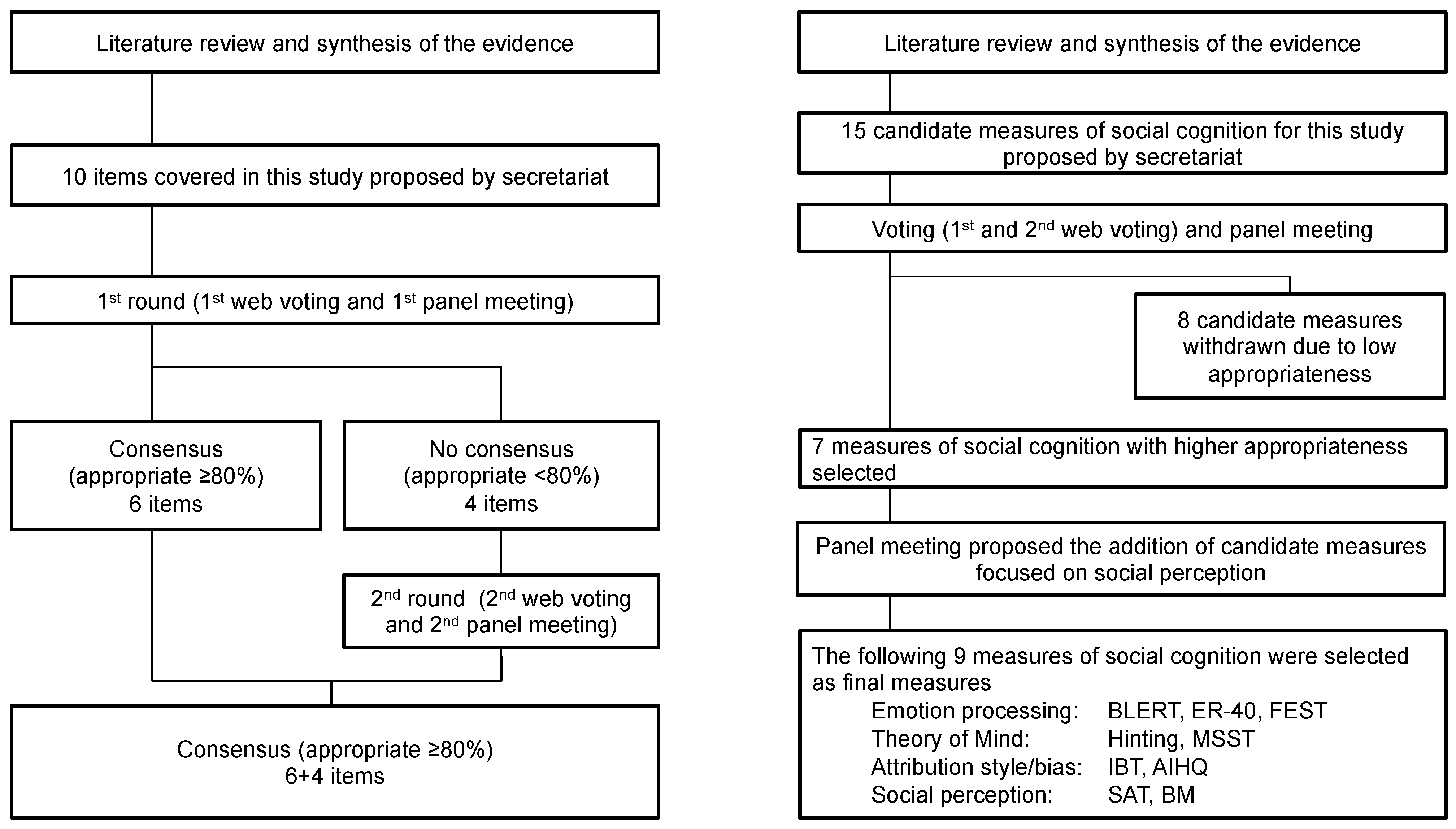
2.3. The Modified Delphi Process
3. Results
3.1. Definition and Core Domains of Social Cognition
3.2. Target Population, Purpose of Use, and Evaluation Criteria of Social Cognition Measures
3.3. Panel Ratings and Selection of Social Cognition Measures
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Green, M.F.; Penn, D.L.; Bentall, R.; Carpenter, W.T.; Gaebel, W.; Gur, R.C.; Kring, A.M.; Park, S.; Silverstein, S.M.; Heinssen, R. Social cognition in schizophrenia: An NIMH workshop on definitions, assessment, and research opportunities. Schizophr. Bull. 2008, 34, 1211–1220. [Google Scholar] [CrossRef] [PubMed]
- Pinkham, A.E.; Penn, D.L. Neurocognitive and social cognitive predictors of interpersonal skill in schizophrenia. Psychiatry Res. 2006, 143, 167–178. [Google Scholar] [CrossRef] [PubMed]
- Pinkham, A.E.; Penn, D.L.; Green, M.F.; Buck, B.; Healey, K.; Harvey, P.D. The social cognition psychometric evaluation study: Results of the expert survey and RAND panel. Schizophr. Bull. 2014, 40, 813–823. [Google Scholar] [CrossRef] [PubMed]
- Pinkham, A.E.; Penn, D.L.; Green, M.F.; Harvey, P.D. Social Cognition Psychometric Evaluation: Results of the Initial Psychometric Study. Schizophr. Bull. 2016, 42, 494–504. [Google Scholar] [CrossRef] [PubMed]
- Pinkham, A.E.; Harvey, P.D.; Penn, D.L. Social Cognition Psychometric Evaluation: Results of the Final Validation Study. Schizophr. Bull. 2018, 44, 737–748. [Google Scholar] [CrossRef]
- Corcoran, R.; Mercer, G.; Frith, C.D. Schizophrenia, symptomatology and social inference: Investigating “theory of mind” in people with schizophrenia. Schizophr. Res. 1995, 17, 5–13. [Google Scholar] [CrossRef]
- Bryson, G.; Bell, M.; Lysaker, P. Affect recognition in schizophrenia: A function of global impairment or a specific cognitive deficit. Psychiatry Res. 1997, 71, 105–113. [Google Scholar] [CrossRef]
- Kohler, C.G.; Turner, T.H.; Bilker, W.B.; Brensinger, C.M.; Siegel, S.J.; Kanes, S.J.; Gur, R.E.; Gur, R.C. Facial emotion recognition in schizophrenia: Intensity effects and error pattern. Am. J. Psychiatry 2003, 160, 1768–1774. [Google Scholar] [CrossRef]
- Hajdúk, M.; Achim, A.M.; Brunet-Gouet, E.; Mehta, U.M.; Pinkham, A.E. How to move forward in social cognition research? Put it into an international perspective. Schizophr. Res. 2020, 215, 463–464. [Google Scholar] [CrossRef]
- Wu, S.; Keysar, B. The effect of culture on perspective taking. Psychol. Sci. 2007, 18, 600–606. [Google Scholar] [CrossRef]
- Mehta, U.M.; Thirthalli, J.; Gangadhar, B.N.; Keshavan, M.S. Need for culture specific tools to assess social cognition in schizophrenia. Schizophr. Res. 2011, 133, 255–256. [Google Scholar] [CrossRef]
- Chen, K.W.; Lee, S.C.; Chiang, H.Y.; Syu, Y.C.; Yu, X.X.; Hsieh, C.L. Psychometric properties of three measures assessing advanced theory of mind: Evidence from people with schizophrenia. Psychiatry Res. 2017, 257, 490–496. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.S.; Corbera, S.; Poltorak, A.; Park, K.; Assaf, M.; Bell, M.D.; Wexler, B.E.; Cho, Y.I.; Jung, S.; Brocke, S.; et al. Measuring theory of mind in schizophrenia research: Cross-cultural validation. Schizophr. Res. 2018, 201, 187–195. [Google Scholar] [CrossRef]
- Mehta, U.M.; Thirthalli, J.; Naveen Kumar, C.; Mahadevaiah, M.; Rao, K.; Subbakrishna, D.K.; Gangadhar, B.N.; Keshavan, M.S. Validation of Social Cognition Rating Tools in Indian Setting (SOCRATIS): A new test-battery to assess social cognition. Asian J. Psychiatry 2011, 4, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Lim, K.; Lee, S.A.; Pinkham, A.E.; Lam, M.; Lee, J. Evaluation of social cognitive measures in an Asian schizophrenia sample. Schizophr. Res. Cogn. 2020, 20, 100169. [Google Scholar] [CrossRef] [PubMed]
- Kerr, S.L.; Neale, J.M. Emotion perception in schizophrenia: Specific deficit or further evidence of generalized poor performance? J. Abnorm. Psychol. 1993, 102, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Minoshita, S.; Morita, N.; Yamashita, T.; Yoshikawa, M.; Kikuchi, T.; Satoh, S. Recognition of affect in facial expression using the Noh Mask Test: Comparison of individuals with schizophrenia and normal controls. Psychiatry Clin. Neurosci. 2005, 59, 4–10. [Google Scholar] [CrossRef]
- Stone, V.E.; Baron-Cohen, S.; Knight, R.T. Frontal lobe contributions to theory of mind. J. Cogn. Neurosci. 1998, 10, 640–656. [Google Scholar] [CrossRef] [PubMed]
- Adachi, T.; Koeda, T.; Hirabayashi, S.; Maeoka, Y.; Shiota, M.; Wright, E.C.; Wada, A. The metaphor and sarcasm scenario test: A new instrument to help differentiate high functioning pervasive developmental disorder from attention deficit/hyperactivity disorder. Brain Dev. 2004, 26, 301–306. [Google Scholar] [CrossRef]
- Baron-Cohen, S.; Wheelwright, S.; Hill, J.; Raste, Y.; Plumb, I. The “Reading the Mind in the Eyes” Test revised version: A study with normal adults, and adults with Asperger syndrome or high-functioning autism. J. Child Psychol. Psychiatry 2001, 42, 241–251. [Google Scholar] [CrossRef]
- McDonald, S.; Flanagan, S.; Rollins, J.; Kinch, J. TASIT: A new clinical tool for assessing social perception after traumatic brain injury. J. Head Trauma Rehabil. 2003, 18, 219–238. [Google Scholar] [CrossRef] [PubMed]
- Combs, D.R.; Penn, D.L.; Wicher, M.; Waldheter, E. The Ambiguous Intentions Hostility Questionnaire (AIHQ): A new measure for evaluating hostile social-cognitive biases in paranoia. Cogn. Neuropsychiatry 2007, 12, 128–143. [Google Scholar] [CrossRef] [PubMed]
- Rosset, E. It′s no accident: Our bias for intentional explanations. Cognition 2008, 108, 771–780. [Google Scholar] [CrossRef]
- Roberts, D.L.; Fiszdon, J.; Tek, C. Initial validity of the Social Cognition Screening Questionnaire (SCSQ). Schizophr. Bull. 2011, 37 (Suppl. 1), 280. [Google Scholar]
- Hashimoto, N.; Toyomaki, A.; Hirai, M.; Miyamoto, T.; Narita, H.; Okubo, R.; Kusumi, I. Absent activation in medial prefrontal cortex and temporoparietal junction but not superior temporal sulcus during the perception of biological motion in schizophrenia: A functional MRI study. Neuropsychiatry Dis. Treat. 2014, 10, 2221–2230. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Bell, M.D.; Fiszdon, J.M.; Greig, T.C.; Wexler, B.E. Social attribution test--multiple choice (SAT-MC) in schizophrenia: Comparison with community sample and relationship to neurocognitive, social cognitive and symptom measures. Schizophr. Res. 2010, 122, 164–171. [Google Scholar] [CrossRef]
- Corrigan, P.W.; Green, M.F. The Situational Feature Recognition Test: A Measure of Schema Comprehension for Schizophrenia; John Wiley & Sons: Hoboken, NJ, USA, 1993; pp. 29–35. [Google Scholar]
- Fitch, K.; Bernstein, S.J.; Aguilar, M.D.; Burnand, B.; LaCalle, J.R.; Lazaro, P.; van het Loo, M.; McDonnell, J.; Vader, J.; Kahan, J.P. The RAND/UCLA Appropriateness Method User′s Manual; RAND Corporation: Santa Monica, CA, USA, 2001. [Google Scholar]
- Hasson, F.; Keeney, S.; McKenna, H. Research guidelines for the Delphi survey technique. J. Adv. Nurs. 2000, 32, 1008–1015. [Google Scholar]
- Marder, S.R.; Fenton, W. Measurement and Treatment Research to Improve Cognition in Schizophrenia: NIMH MATRICS initiative to support the development of agents for improving cognition in schizophrenia. Schizophr. Res. 2004, 72, 5–9. [Google Scholar] [CrossRef]
- Leifker, F.R.; Patterson, T.L.; Heaton, R.K.; Harvey, P.D. Validating measures of real-world outcome: The results of the VALERO expert survey and RAND panel. Schizophr. Bull. 2011, 37, 334–343. [Google Scholar] [CrossRef]
- Green, B.; Jones, M.; Hughes, D.; Williams, A. Applying the Delphi technique in a study of GPs′ information requirements. Health Soc. Care Community 1999, 7, 198–205. [Google Scholar] [CrossRef]
- Kern, R.S.; Penn, D.L.; Lee, J.; Horan, W.P.; Reise, S.P.; Ochsner, K.N.; Marder, S.R.; Green, M.F. Adapting social neuroscience measures for schizophrenia clinical trials, Part 2: Trolling the depths of psychometric properties. Schizophr. Bull. 2013, 39, 1201–1210. [Google Scholar] [CrossRef] [PubMed]
- Olbert, C.M.; Penn, D.L.; Kern, R.S.; Lee, J.; Horan, W.P.; Reise, S.P.; Ochsner, K.N.; Marder, S.R.; Green, M.F. Adapting social neuroscience measures for schizophrenia clinical trials, part 3: Fathoming external validity. Schizophr. Bull. 2013, 39, 1211–1218. [Google Scholar] [CrossRef] [PubMed]
- Buck, B.; Iwanski, C.; Healey, K.M.; Green, M.F.; Horan, W.P.; Kern, R.S.; Lee, J.; Marder, S.R.; Reise, S.P.; Penn, D.L. Improving measurement of attributional style in schizophrenia; A psychometric evaluation of the Ambiguous Intentions Hostility Questionnaire (AIHQ). J. Psychiatry Res. 2017, 89, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Horan, W.P.; Nuechterlein, K.H.; Wynn, J.K.; Lee, J.; Castelli, F.; Green, M.F. Disturbances in the spontaneous attribution of social meaning in schizophrenia. Psychol. Med. 2009, 39, 635–643. [Google Scholar] [CrossRef] [PubMed]
- Johannesen, J.K.; Lurie, J.B.; Fiszdon, J.M.; Bell, M.D. The Social Attribution Task-Multiple Choice (SAT-MC): A Psychometric and Equivalence Study of an Alternate Form. ISRN Psychiatry 2013, 2013, 830825. [Google Scholar] [CrossRef]


{kind=link}
| Domain/Measure | Original Citation | Total Citations (PubMed) | Citations Per Year (PubMed) |
|---|---|---|---|
| Emotion Processing | |||
| Bell Lysaker Emotion Recognition Task (BLERT) | Bryson et al., 1997 [7] | 44 | 1.91 |
| Face Emotion Identification Test (FEIT) | Kerr and Neale, 1993 [16] | 94 | 3.48 |
| Noh Mask Test | Minoshita et al., 2005 [17] | 2 | 0.13 |
| Penn Emotion Recognition Test (ER-40) | Kohler et al., 2003 [8] | 174 | 10.24 |
| Theory of Mind | |||
| Faux Pas Test | Stone et al., 1998 [18] | 212 | 9.64 |
| Hinting Task | Corcoran et al., 1995 [6] | 145 | 5.8 |
| Metaphor and Sarcasm Scenario Test (MSST) | Adachi et al., 2004 [19] | 9 | 0.56 |
| Reading the Mind in the Eyes Test (Eyes) | Baron-Cohen et al., 2001 [20] | 864 | 45.47 |
| The Awareness of Social Inference Test (TASIT) | McDonald et al., 2003 [21] | 100 | 5.88 |
| Attributional Style/Bias | |||
| Ambiguous Intentions and Hostility Questionnaire (AIHQ) | Combs et al., 2007 [22] | 59 | 4.54 |
| Intentionality Bias Task (IBT) | Rosset, 2008 [23] | 23 | 1.92 |
| Social Cognition Screening Questionnaire (SCSQ) * | Roberts et al., 2011 [24] | (N/A) | (N/A) |
| Social Perception | |||
| Biological Motion (BM) Task | Hashimoto et al., 2014 [25] | 5 | 0.83 |
| Social Attribution Task-Multiple Choice (SAT-MC) | Bell et al., 2010 [26] | 20 | 2 |
| Situational Feature Recognition Test (SFRT) | Corrigan and Green, 1993 [27] | (N/A) | (N/A) |
| Domain/Measure | Median, Mean (SD) | |
|---|---|---|
| 1st Round | 2nd Round | |
| Emotion Processing | ||
| ER-40 | 8, 7.1 (1.8) | 8, 7.1 (1.7) |
| FEST * | 7, 7.2 (0.8) | 8, 7.1 (1.9) |
| BLERT-J | 7, 7.1 (1.6) | 7, 7.3 (0.9) |
| Noh Mask Test | 4, 4.2 (1.7) | 3, 3.1 (0.9) |
| Theory of Mind | ||
| MSST | 8, 6.9 (1.9) | 8, 6.8 (1.9) |
| Hinting | 8, 7.2 (1.6) | 7, 7.1 (1.6) |
| Eyes | 5, 5.2 (2.4) | 5, 5.0 (1.6) |
| Faux Pas | 5, 5.0 (2.1) | 5, 4.8 (1.8) |
| TASIT | 5, 4.6 (2.8) | 5, 4.3 (1.5) |
| Attributional Style/Bias | ||
| AIHQ | 7, 6.4 (1.8) | 7, 6.2 (1.7) |
| IBT | 6, 6.0 (1.9) | 6, 5.8 (0.9) |
| SCSQ ** | 7, 7.2 (1.1) | 5, 5.2 (2.0) |
| Social Perception | ||
| SAT | 6, 5.7 (2.4) | 4, 5.1 (2.3) |
| SFRT | 6, 5.6 (2.1) | 4, 4.1 (1.7) |
| Biological Motion | 5, 4.6 (2.0) | 4, 4.0 (1.3) |
| Domain/Measure | Description |
|---|---|
| Emotion Processing | |
| Penn Emotion Recognition Test (ER-40) | Measures the ability to identify emotional state from facial expressions. Participants view 40 still photographs of people’s faces, each expressing a particular emotion (joy, sadness, anger, fear, or no emotion). Participants are then asked to answer, which emotion is expressed in each photograph. Performance is indexed as the number of correct answers. The estimated time required is 3–7 min. |
| Facial Emotion Selection Test (FEST) | Japanese version of the FEIT. Measures ability to infer emotions from the facial expressions of others. Participants view 21 photographs and answer which emotion (joy, sadness, anger, fear, surprise, disgust, or no emotion) it corresponds to. Performance is indexed as the total number of correct answers. The estimated time required is about 10 min. |
| Bell Lysaker Emotion Recognition Task-Japanese Version (BLERT-J) | Japanese version of the BLERT. Measures the ability to identify emotional state from facial expression, tone of speech, and body language. Participants view 21 short videos in which an actor portrays different emotional states (happiness, sadness, fear, disgust, surprise, anger, or no emotion) and must answer which emotion was portrayed in each video. Performance is indexed as the number of correct answers. The estimated time required is 7–10 min. |
| Theory of Mind | |
| Metaphor and Sarcasm Scenario Test (MSST) | Measures ability to understand metaphorical and sarcastic expressions in dialogue. Participants read short passages that provide context for a figurative or sarcastic statement and then choose what they think it means. There are five figurative and five sarcastic statements. The number of correct answers for each type is summed to produce metaphor and sarcasm scores. For each of the sarcasm scenarios, one of the incorrect answers is a “landmine answer” representing the statement’s meaning when taken at face value. The number of times the landmine answer was avoided is tallied as “the landmine avoidance score.” The estimated time required is 5–10 min. |
| Hinting Task | Measures the ability to detect sarcasm and indirect requests from others’ statements. Participants are read passages of dialogue between two characters in 10 different scenarios. In each conversation, one of the characters tries to indirectly convey a certain intention or request to the other. Participants are asked what the intention or request is. If the answer is incorrect, the participant is provided with additional dialogue that further clarifies the intention. First-time correct answers are awarded two points, and second-time correct answers are awarded one point. Performance is indexed as the total number of points. The estimated time required is about 7 min. |
| Attributional Style/Bias | |
| Ambiguous Intentions and Hostility Questionnaire (AIHQ) | Assesses hostile social cognitive biases. Participants read passages describing hypothetical, negative scenarios and answer why they think the situation occurred. Participants then rate the degree to which they perceived the action to be intentional, how angry it would make them feel, and how much they would blame the other person on separate Likert scales. Finally, participants answer how they would respond to the situation. Responses to the open-ended questions are coded by independent raters to compute Hostility Bias and Aggression Bias indexes, whereas the Likert ratings are averaged and summed to produce a Blame Score. The estimated time required is 5–10 min. |
| Intentionality Bias Task (IBT) | Assesses tendency to assign intentionality to the actions of others. Up to 80 short sentences (fewer in some versions) depicting another person’s action (such as “He broke the window”) are presented on a screen. Participants answer whether the behavior is “intentional” or “accidental” within a short time limit. Performance is indexed as the number of questions answered “intentional” to the total number of questions. The estimated time required is about 5 min. |
| Social Perception | |
| Social Attribution Task-Multiple Choice (SAT-MC) | Assesses implicit social attribution formation. Participants view a 64-s, animated video of anthropomorphized geometric shapes enacting a social drama. The video does not include dialogue. After viewing the video twice, participants answer 19 multiple-choice questions about what happens or how the shapes feel. Performance is indexed as the total number of correct answers. The estimated time required is about 10 min. |
| Biological Motion (BM) Task | Measures capacity to perceive human body motion at high speed. Participants are presented with images of moving light spots, either moving in coordination to mimic human body movements (Biological Motion) or at random (Scrambled Motion). Participants view multiple images and answer whether each is either Biological Motion or Scrambled Motion. In later parts of the task, random light spots are added/removed in response to correct/incorrect responses to adjust difficulty and determine participants’ level of performance. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okano, H.; Kubota, R.; Okubo, R.; Hashimoto, N.; Ikezawa, S.; Toyomaki, A.; Miyazaki, A.; Sasaki, Y.; Yamada, Y.; Nemoto, T.; et al. Evaluation of Social Cognition Measures for Japanese Patients with Schizophrenia Using an Expert Panel and Modified Delphi Method. J. Pers. Med. 2021, 11, 275. https://doi.org/10.3390/jpm11040275
Okano H, Kubota R, Okubo R, Hashimoto N, Ikezawa S, Toyomaki A, Miyazaki A, Sasaki Y, Yamada Y, Nemoto T, et al. Evaluation of Social Cognition Measures for Japanese Patients with Schizophrenia Using an Expert Panel and Modified Delphi Method. Journal of Personalized Medicine. 2021; 11(4):275. https://doi.org/10.3390/jpm11040275
Chicago/Turabian StyleOkano, Hiroki, Ryotaro Kubota, Ryo Okubo, Naoki Hashimoto, Satoru Ikezawa, Atsuhito Toyomaki, Akane Miyazaki, Yohei Sasaki, Yuji Yamada, Takahiro Nemoto, and et al. 2021. "Evaluation of Social Cognition Measures for Japanese Patients with Schizophrenia Using an Expert Panel and Modified Delphi Method" Journal of Personalized Medicine 11, no. 4: 275. https://doi.org/10.3390/jpm11040275
APA StyleOkano, H., Kubota, R., Okubo, R., Hashimoto, N., Ikezawa, S., Toyomaki, A., Miyazaki, A., Sasaki, Y., Yamada, Y., Nemoto, T., & Mizuno, M. (2021). Evaluation of Social Cognition Measures for Japanese Patients with Schizophrenia Using an Expert Panel and Modified Delphi Method. Journal of Personalized Medicine, 11(4), 275. https://doi.org/10.3390/jpm11040275