
Personalized Healthcare: The Importance of Patients’ Rights in Clinical Practice from the Perspective of Nursing Students in Poland, Spain and Slovakia—A Cross-Sectional Study

 ,
,  ,
,
Abstract
1. Introduction
- Are there differences in the observance of patients’ rights in healthcare-providing institutions in the opinion of nursing students in Poland, Spain and Slovakia and to what extent?
- To what extent does knowledge of selected patients’ rights in clinical practice regarding an ill or healthy person differ among nursing students in Poland, Spain and Slovakia?
2. Materials and Methods
2.1. Settings and Design
2.2. Participants
2.3. Research Instruments
2.4. Statistical Analysis
3. Results
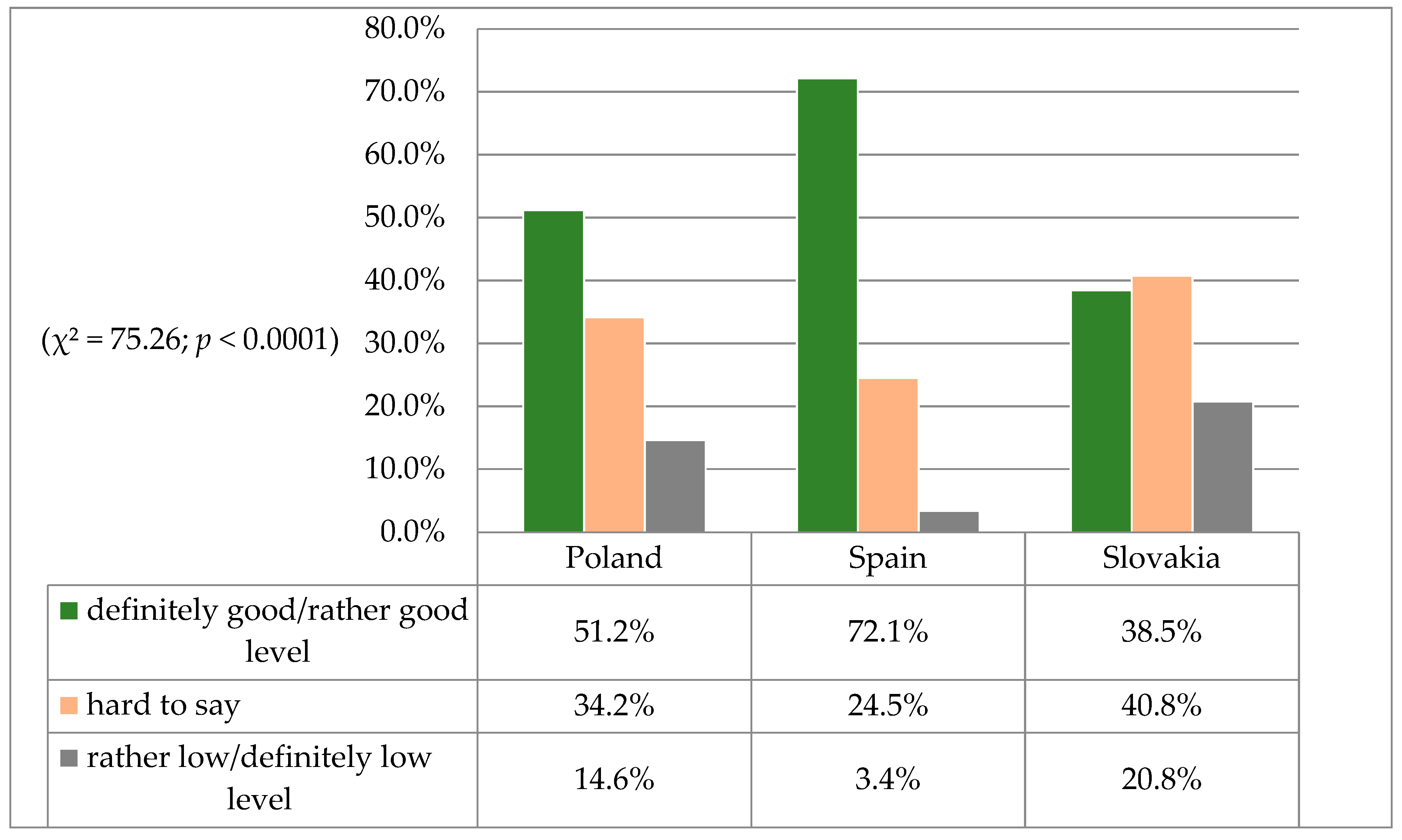
3.1. Observance of Patients’ Rights in Personalized Healthcare as Perceived by Nursing Students
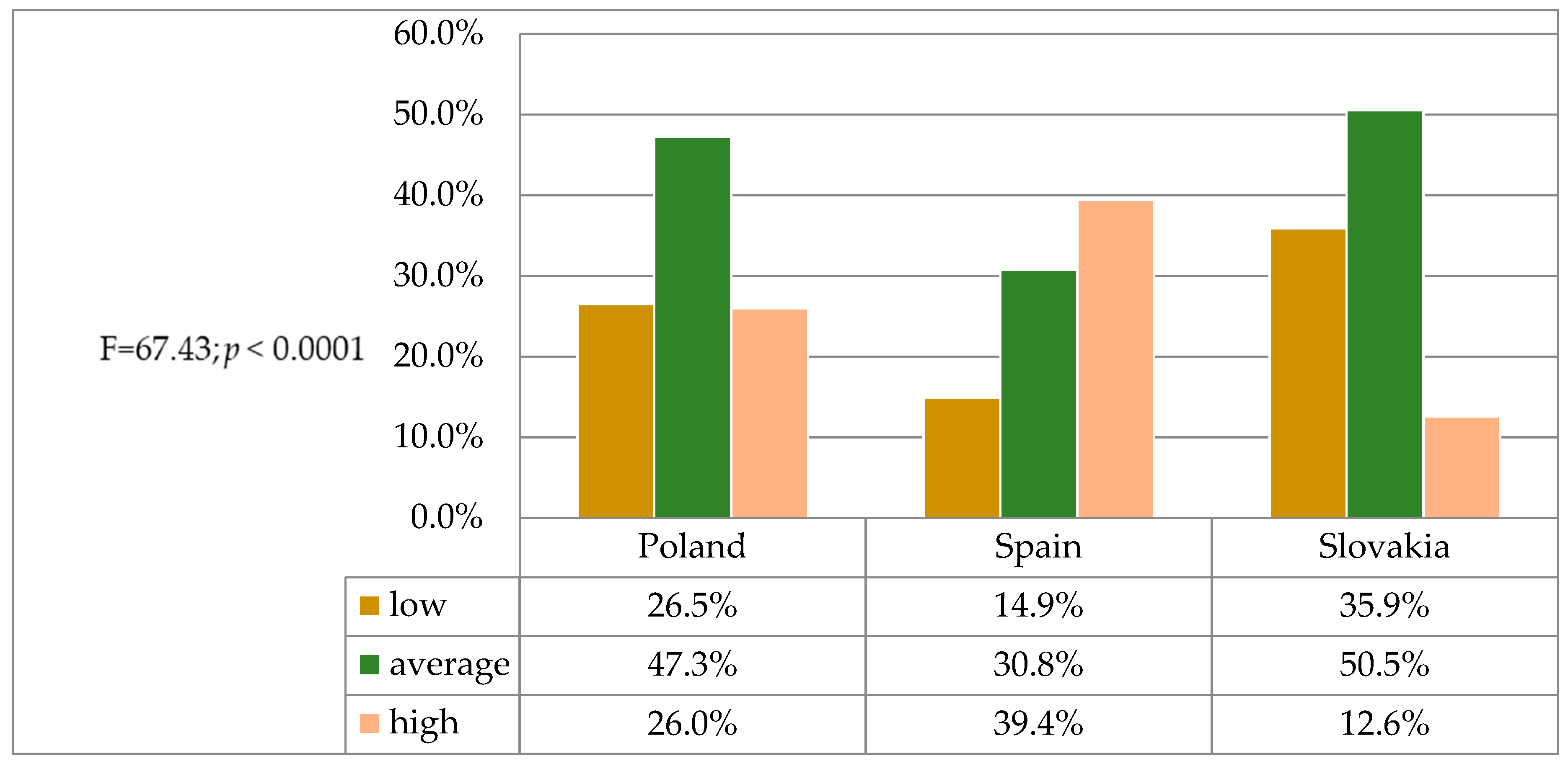
3.2. Differences in Nursing Students’ Knowledge of Selected Patients’ Rights in Personalized Healthcare
3.3. Assessing the Importance of the Patient’s Right to Dignity in Personalized Healthcare
4. Discussion
5. Limitations and Implications for Professional Practice
6. Conclusions
- The degree to which patients’ rights are respected in healthcare facilities in Poland, Spain and Slovakia in the subjective assessment of nursing students is significantly different and is not always favorable for the patient.
- A variation in the level of nursing students’ knowledge of selected patients’ rights in personalized healthcare was observed, requiring in-depth educational activities at the university level in respective countries.
- The degree of knowledge of patients’ rights among nursing students is not uniform and includes the right to information on the patient’s health, the confidentiality of patient-related information and medical records, to withdraw their objection to organ and tissue donation, to pastoral care and to deposit valuable items.
- The right to respect dignity, which also includes the right to die in peace and dignity in personalized medical care, was rated the highest by Spanish first-year students.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wium-Andersen, I.K.; Vinberg, M.; Lars Vedel Kessing, L.V.; McIntyre, R.S. Personalized medicine in psychiatry. Nord. J. Psychiat. 2017, 71, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Sigman, M. Introduction: Personalized medicine: What is it and what are the challenges? Fertil Steril. 2018, 109, 944–945. [Google Scholar] [CrossRef] [PubMed]
- Anaya, J.M.; Duarte-Rey, C.; Sarmiento-Monroy, J.C.; Bardey, D.; Castiblanco, J.; Rojas-Villarraga, A. Personalized medicine. Closing the gap between knowledge and clinical practice. Autoimmun Rev. 2016, 15, 833–842. [Google Scholar] [CrossRef]
- Markocka-Mączka, K.; Grabowski, K.; Taboła, R. Holistyczne Podejście do Pacjenta, Profilaktyka i Edukacja Zdrowotna [Holistic Approach to the Patient, Prevention and Health Education]; Wyd. Naukowe NeuroCentrum: Lublin, Poland, 2017; pp. 171–176. [Google Scholar]
- Jacek, A.; Ożóg, K. Przestrzeganie praw pacjenta przez personel medyczny [Respecting patient’s rights by medical staff]. Hygeia Public Health 2012, 47, 264–271. [Google Scholar]
- Olejniczak, M.; Michowska, M.; Basińska, K. Opinie studentów Gdańskiego Uniwersytetu Medycznego na temat przestrzegania praw pacjenta w czasie odbywania zajęć klinicznych [Opinions of Gdańsk Medical University students on respecting patients’ rights during their clinical practice]. Ann. Acad. Med. Gedan. 2011, 41, 79–87. [Google Scholar]
- WHO. Patients’ Rights. Available online: https://www.who.int/genomics/public/patientrights/en/ (accessed on 26 July 2020).
- Powszechna Deklaracja Praw Człowieka [Universal Declaration of Human Rights]. Available online: https://www.unesco.pl/fileadmin/user_upload/pdf/Powszechna_Deklaracja_Praw_Czlowieka.pdf (accessed on 26 July 2020).
- Convention for the Protection of Human Rights and Dignity of the Human Being with regard to the Application of Biology and Medicine: Convention of Human Rights and Biomedicine. Available online: http://conventions.coe.int/Treaty/en/Treaties/Html/164.htm (accessed on 26 July 2020).
- European Charter of Patients’ Rights. Available online: http://www.patienttalk.info/european_charter.pdf (accessed on 26 July 2020).
- European Charter of Patients’ Rights, Rome. 2002. Available online: http://ec.europa.eu/health/ph_overview/co_operation/mobility/docs/health_services_co108_en.pdf (accessed on 26 July 2020).
- Viberg, N.; Forsberg, B.C.; Borowitz, M.; Molin, R. International comparisons of waiting times in health care—Limitations and prospects. Health Policy 2013, 112, 53–61. [Google Scholar] [CrossRef]
- Dyrektywa Parlamentu Europejskiego i Rady 2011/24/UE z Dnia 9 marca 2011 r. w Sprawie Stosowania Praw Pacjentów w Transgranicznej Opiece Zdrowotnej (Dz. U. UE L z Dnia 4 Kwietnia 2011 r.) [Directive 2011/24 / EU of the European Parliament and of the Council of 9 March 2011 on the Application of Patients’ Rights in Cross-Border Healthcare (Journal of Laws UE L of 4 April 2011)]. Available online: http://www.kpk.nfz.gov.pl/images/downloads/dyrektywa.pdf (accessed on 30 July 2020).
- Quinn, P.; De Hert, P. The Patients’ Rights Directive (2011/24/EU)—Providing (some) rights to EU residents seeking healthcare in other Member States. Comput. Law Secur. Rev. 2011, 27, 497–502. [Google Scholar] [CrossRef]
- Azzopardi-Muscat, N.; Baeten, R.; Clemens, T.; Habicht, T.; Keskimäki, I.; Kowalska-Bobko, I.; Sagan, A.; van Ginneken, E. The role of the 2011 patients’ rights in cross-border health care directive in shaping seven national health systems: Looking beyond patient mobility. Health Policy 2018, 122, 279–283. [Google Scholar] [CrossRef]
- Heinonen, N.; Tynkkynen, L.-K.; Keskimäki, I. The transposition of the patients’ rights directive in finland—Difficulties encountered. Health Policy 2019, 123, 526–531. [Google Scholar] [CrossRef]
- Minvielle, E. Toward Customized Care Comment on “(Re) Making the Procrustean Bed? Standardization and Customization as Competing Logics in Healthcare”. Int. J. Health Policy. Manag. 2018, 7, 272–274. [Google Scholar] [CrossRef]
- Elewa, A.H.; ElAlim, E.A.; Etway, E.G. Nursing interns’ perception regarding patients’ rights and patients’ advocacy. SOJ. Nur. Health Care 2016, 2, 1–6. [Google Scholar] [CrossRef][Green Version]
- Dyrektywa 2005/36/WE Parlamentu Europejskiego i Rady z dnia 7 Września 2005 r w Sprawie Uznawania Kwalifikacji Zawodowych (Dz.U. L 255 z 30.9.2005, s. 22). [Directive 2005/36 / EC of the European Parliament and of the Council of 7 September 2005 on the Recognition of Professional Qualifications (OJ L 255, 30.9.2005, p. 22). Available online: https://eur-lex.europa.eu/legal-content/PL/TXT/PDF/?uri=CELEX:02005L0036-20140117&from=EN (accessed on 31 July 2020).
- Rozporządzenie Ministra Zdrowia z Dnia 26 Lipca 2019 r. w Sprawie Standardów Kształcenia Przygotowującego Do Wykonywania Zawodu Lekarza, Lekarza Dentysty, Farmaceuty, Pielęgniarki, Położnej, Diagnosty Laboratoryjnego, Fizjoterapeuty i Ratownika Medycznego (Dz. U. z 21.08.2019 r., poz. 1573) [Regulation of the Minister of Health of 26 July 2019 on the Standards of Education Preparing for the Profession of a Doctor, Dentist, Pharmacist, Nurse, Midwife, Laboratory Diagnostician, Physiotherapist and Paramedic] (Journal of Laws of 21 August 2019, Item 1573). Available online: https://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU20190001573 (accessed on 31 July 2020).
- Poorchangizi, B.; Borhani, F.; Abbaszadeh, A.; Mirzaee, M.; Farokhzadian, J. The importance of professional values from nursing students’ perspective. BMC Nurs. 2019, 18, 26. [Google Scholar] [CrossRef]
- Kupcewicz, E.; Grochans, E.; Mikla, M.; Kadučáková, H.; Jóźwik, M. Role of global self-esteem in predicting life satisfaction of nursing students in poland, spain and slovakia. Int. J. Environ. Res. Public Health 2020, 17, 5392. [Google Scholar] [CrossRef] [PubMed]
- Kupcewicz, E.; Grochans, E.; Kadučáková, H.; Mikla, M.; Jóźwik, M. Analysis of the relationship between stress intensity and coping strategy and the quality of life of nursing students in poland, spain and slovakia. Int. J. Environ. Res. Public Health 2020, 17, 4536. [Google Scholar] [CrossRef]
- Szymczak, W. Podstawy Statystyki Dla Psychologów [Fundamentals of Statistics for Psychologists]; DIFIN: Warszawa, Poland, 2018. [Google Scholar]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M.; For the STROBE Initiative. Strengthening the reporting of observational studies in epidemiology (strobe): Explanation and elaboration. Int. J. Surg. 2014, 12, 1500–1524. [Google Scholar] [CrossRef] [PubMed]
- Ansari, S.; Abeid, P.; Namvar, F.; Dorakvand, M.; Rokhafrooz, D. Respect to the bill of patients’ rights in the educational hospitals in Ahvaz, Iran. Middle East J. Sci. Res. 2013, 4, 440–444. [Google Scholar] [CrossRef]
- Mohammed, E.S.; Seedhom, A.E.; Ghazawy, E.R. Awareness and practice of patient rights from a patient perspective: An insight from Upper Egypt. Int. J. Qual Health Care 2018, 1, 145–151. [Google Scholar] [CrossRef] [PubMed]
- Abedi, G.; Shojaee, J.; Moosazadeh, M.; Rostami, F.; Nadi, A.; Abedini, E.; Palenik, C.J.; Askarian, M. Awareness and observance of patient rights from the perspective of iranian patients: A systematic review and meta-analysis. Iran. J. Med. Sci. 2017, 42, 227–234. [Google Scholar]
- Agrawal, U.; D’Souza, B.C.; Seetharam, A.M. Awareness of Patients’ Rights among Inpatients of a Tertiary Care Teaching Hospital- A Cross-sectional Study. J. Clin. Diagn. Res. 2017, 11, IC01–IC06. [Google Scholar] [CrossRef]
- Tabassum, T.; Ashraf, M.; Thaver, I. Hospitalized patients’ awareness of their rights-a cross sectional survey in a public and private tertiary care hospitals of punjab, pakistan. J. Ayub. Med. Coll. Abbottabad. 2016, 28, 582–586. [Google Scholar]
- Mohammadi, M.; Larijani, B.; Emami Razavi, S.H.; Fotouhi, A.; Ghaderi, A.; Madani, S.J.; Shafiee, M.N. Do patients know that physicians should be confidential? study on patients’ awareness of privacy and confidentiality. J. Med. Ethics Hist. Med. 2018, 11, 1. [Google Scholar]
- Hadian Jazi, Z.; Dehghan Nayeri, N. Barriers in the performance of patient’s rights in iran and appropriate offered solutions review article. J. Holist. Nurs. Midwifery 2014, 24, 69–79. [Google Scholar]
- Mousavi, S.M.; Mohammadi, N.; Ashghali Farahani, M.; Hosseini, A.F. Observing patients’ rights and the facilitating and deterrent organizational factors from the viewpoint of nurses working in intensive care units. J. Client Cent. Nurs. Care 2017, 3, 27–36. [Google Scholar] [CrossRef]
- Waddington, L.; Mesherry, B. Exceptions and exclusions: The right to informed consent for medical treatment of people with psychosocial disabilities in Europe. Eur. J. Health. Law. 2016, 23, 279–304. [Google Scholar] [CrossRef] [PubMed]
- Sabzevari, A.; Kiani, M.A.; Saeidi, M.; Jafari, S.A.; Kianifar, H.; Ahanchian, H.; Jarahi, L.; Zakerian, M. Evaluation of patients’ rights observance according to patients’ rights charter in educational hospitals affiliated to mashhad university of medical sciences: Medical staffs’ views. Electron. Physician. 2016, 8, 3102–3109. [Google Scholar] [CrossRef]
- Sheikhtaheri, A.; Jabali, M.S.; Dehaghi, Z.H. Nurses’ knowledge and performance of the patients’ bill of rights. Nurs. Ethics 2016, 23, 866–876. [Google Scholar] [CrossRef]
- Al-Saadi, A.N.; Slimane, S.B.A.; Al-Shibli, R.A.; Al-Jabri, F.Y. Awareness of the Importance of and Adherence to Patients’ Rights Among Physicians and Nurses in Oman: An analytical cross-sectional study across different levels of healthcare. Sultan. Qaboos Univ. Med. J. 2019, 19, e201–e208. [Google Scholar] [CrossRef] [PubMed]
- Water, T.; Ford, K.; Spence, D.; Rasmussen, S. Patient advocacy by nurses—Past, present and future. Contemp. Nurse 2016, 56, 696–709. [Google Scholar] [CrossRef]
- Aydin Er, R.; Ersoy, N.; Celik, S. The nursing students’ views about the patient’s rights at the west black sea universities in turkey. Nurs. Midwifery Stud. 2014, 3, e19136. [Google Scholar] [CrossRef] [PubMed]
- Suikkala, A.; Koskinen, S.; Leino-Kilpi, H. Patients’ involvement in nursing students’ clinical education: A scoping review. Int J. Nurs. Stud. 2018, 84, 40–51. [Google Scholar] [CrossRef]
- Kim, S.-Y. The Relationship between Human Rights Sensitivity, Interpersonal Caring Behavior, and Biomedical Ethics in Nursing Students Who Have Experienced Clinical Practice. J. Korea Acad. Industr. Coop. Soc. 2020, 21, 410–418. [Google Scholar] [CrossRef]
- Clavagnier, I. Patients’ rights. Rev. Infirm. 2017, 66, 47–48. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| No. | Patients’ Rights | Answer Scale | Responses-Number (%) | Chi-Squared Test (χ2) | p | ||
|---|---|---|---|---|---|---|---|
| Poland n = 404 | Spain n = 208 | Slovakia n = 390 | |||||
| 1 | The right to obtain comprehensive and understandable information on their health condition | Yes | 115 (28.5) | 193 (92.8) | 199 (51.0) | 315.61 | 0.0001 *** |
| No | 92 (22.8) | 9 (4.3) | 109 (28.0) | ||||
| I have no opinion | 133 (32.9) | 6 (2.9) | 32 (8.2) | ||||
| I don’t know | 64 (15.8) | 0 (0.0) | 50 (12.8) | ||||
| 2 | The patient’s right to pastoral care while staying in hospital | Yes | 262 (64.9) | 118 (56.7) | 210 (58.9) | 122.24 | 0.0001 *** |
| No | 13 (3.2) | 22 (10.6) | 62 (9.7) | ||||
| I have no opinion | 62 (15.4) | 67 (32.2) | 50 (17.9) | ||||
| I don’t know | 67 (16.6) | 1 (0.5) | 68 (13.6) | ||||
| 3 | The right to deposit valuables in a hospital depository during on-site (stationary) treatment | Yes | 310 (76.7) | 130 (62.5) | 356 (91.3) | 121.64 | 0.0001 *** |
| No | 26 (6.4) | 19 (9.1) | 13 (3.3) | ||||
| I have no opinion | 43 (10.6) | 59 (28.4) | 10 (2.6) | ||||
| I don’t know | 25 (6.2) | 0 (0.0) | 11 (2.8) | ||||
| 4 | Data protection and confidentiality of patient information by healthcare professionals | Yes | 346 (85.6) | 165 (79.3) | 356 (91.3) | 66.13 | 0.0001 *** |
| No | 14 (3.5) | 37 (17.8) | 11 (2.8) | ||||
| I have no opinion | 29 (7.2) | 4 (1.9) | 9 (2.3) | ||||
| I don’t know | 15 (3.7) | 2 (1.0) | 14 (3.6) | ||||
| 5 | Disclosure of information subject to professional secrecy by healthcare professionals | I don’t know | 59 (14,6) | 20 (9.6) | 89 (22.8) | 36.78 | 0.0001 *** |
| Yes, if the information covered could contribute to a risk to the health and life of others | 225 (55.7) | 141 (67.8) | 180 (46.2) | ||||
| Never | 40 (9.9) | 10 (4.8) | 26 (6.7) | ||||
| At the request of the court | 80 (19.8) | 37 (17.8) | 95 (24.4) | ||||
| 6 | Obligation to provide the patient with a copy of the records of hospital/ambulatory treatment by the medical facility | Yes | 289 (71.5) | 156 (75.0) | 264 (67.7) | 51.14 | 0.0001 *** |
| No | 30 (7.4) | 18 (8.7) | 53 (13.6) | ||||
| I have no opinion | 42 (10.4) | 34 (16.4) | 29 (7.4) | ||||
| I don’t know | 43 (10.6) | 0 (0.0) | 44 (11.3) | ||||
| 7 | Discharge of a patient from a hospital upon the patient’s own request | Yes | 321 (79.5) | 101 (48.6) | 296 (75.9) | 86.00 | 0.0001 *** |
| No | 10 (2.5) | 3 (1.4) | 20 (5.1) | ||||
| Only if their life is not in danger | 47 (11.6) | 73 (35.1) | 56 (14.4) | ||||
| I don’t know | 26 (6.4) | 31 (14.9) | 18 (4.6) | ||||
| 8 | Withdrawal of the patient’s objection to organ and tissue donation | Yes | 243 (60.2) | 150 (72.1) | 221 (56.7) | 15.17 | 0.004 ** |
| No | 52 (12.9) | 22 (10.6) | 54 (13.9) | ||||
| I don’t know | 109 (27.0) | 36 (17.3) | 115 (29.5) | ||||
| Variables | Country of Origin | ANOVA (F) | p Value | ||
|---|---|---|---|---|---|
| Poland n = 404 (40.3%) | Spain n = 208 (20.8%) | Slovakia n = 390 (38.9%) | |||
| M ± SD, Me, Min.–Max., 95% CI | M ± SD, Me, Min.–Max., 95% CI | M ± SD, Me, Min.–Max., 95% CI | |||
| Self-assessment of students’ knowledge of patients’ rights (rating scale 2–5) | 3.00 ± 0.73, 3.00, 2.00–5.00, 2.93 ± 3.07 | 3.54 ± 0.92, 4.00, 2.00–5.00, 3.42 ± 3.67 | 2.79 ± 0.69, 3.00, 2.00–5.00, 2.72 ± 2.86 | F = 67.43 | 0.0001 *** |
| Variables | Country of Origin | ANOVA (F) | p Value | ||
|---|---|---|---|---|---|
| Poland n = 404 (40.3%) | Spain n = 208 (20.8%) | Slovakia n = 390 (38.9%) | |||
| M ± SD, Me, Min.–Max., 95% CI | M ± SD, Me, Min.–Max., 95% CI | M ± SD, Me, Min.–Max., 95% CI | |||
| Ranking on a 2 to 5 scale given to the patient’s right to dignity by the respondents | 3.43 ± 0.77, 4.00, 2.00–4.00, 3.35–3.50 | 4.37 ± 0.92, 5.00, 2.00–5.00, 4.24–4.49 | 3.27 ± 0.79, 3.00, 2.00–4.00, 3.19–3.35 | F = 133.56 | 0.0001 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kupcewicz, E.; Grochans, E.; Kadučáková, H.; Mikla, M.; Bentkowska, A.; Kupcewicz, A.; Andruszkiewicz, A.; Jóźwik, M. Personalized Healthcare: The Importance of Patients’ Rights in Clinical Practice from the Perspective of Nursing Students in Poland, Spain and Slovakia—A Cross-Sectional Study. J. Pers. Med. 2021, 11, 191. https://doi.org/10.3390/jpm11030191
Kupcewicz E, Grochans E, Kadučáková H, Mikla M, Bentkowska A, Kupcewicz A, Andruszkiewicz A, Jóźwik M. Personalized Healthcare: The Importance of Patients’ Rights in Clinical Practice from the Perspective of Nursing Students in Poland, Spain and Slovakia—A Cross-Sectional Study. Journal of Personalized Medicine. 2021; 11(3):191. https://doi.org/10.3390/jpm11030191
Chicago/Turabian StyleKupcewicz, Ewa, Elżbieta Grochans, Helena Kadučáková, Marzena Mikla, Aleksandra Bentkowska, Adam Kupcewicz, Anna Andruszkiewicz, and Marcin Jóźwik. 2021. "Personalized Healthcare: The Importance of Patients’ Rights in Clinical Practice from the Perspective of Nursing Students in Poland, Spain and Slovakia—A Cross-Sectional Study" Journal of Personalized Medicine 11, no. 3: 191. https://doi.org/10.3390/jpm11030191
APA StyleKupcewicz, E., Grochans, E., Kadučáková, H., Mikla, M., Bentkowska, A., Kupcewicz, A., Andruszkiewicz, A., & Jóźwik, M. (2021). Personalized Healthcare: The Importance of Patients’ Rights in Clinical Practice from the Perspective of Nursing Students in Poland, Spain and Slovakia—A Cross-Sectional Study. Journal of Personalized Medicine, 11(3), 191. https://doi.org/10.3390/jpm11030191