
Maternal Psychological and Biological Factors Associated to Gestational Complications

 ,
, 
 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Cohort Selection
2.2. Maternal and Neonatal Data Collection and Group Classification
2.3. Maternal Plasma Variables in the First Trimester
2.4. Maternal Psychological Variables during Pregnancy
2.5. Statistical Analysis
3. Results
3.1. Maternal Characteristics and Development of Obstetric Complications
3.2. Maternal Plasma Variables in the First Trimester
3.3. Psychological Variables during Pregnancy
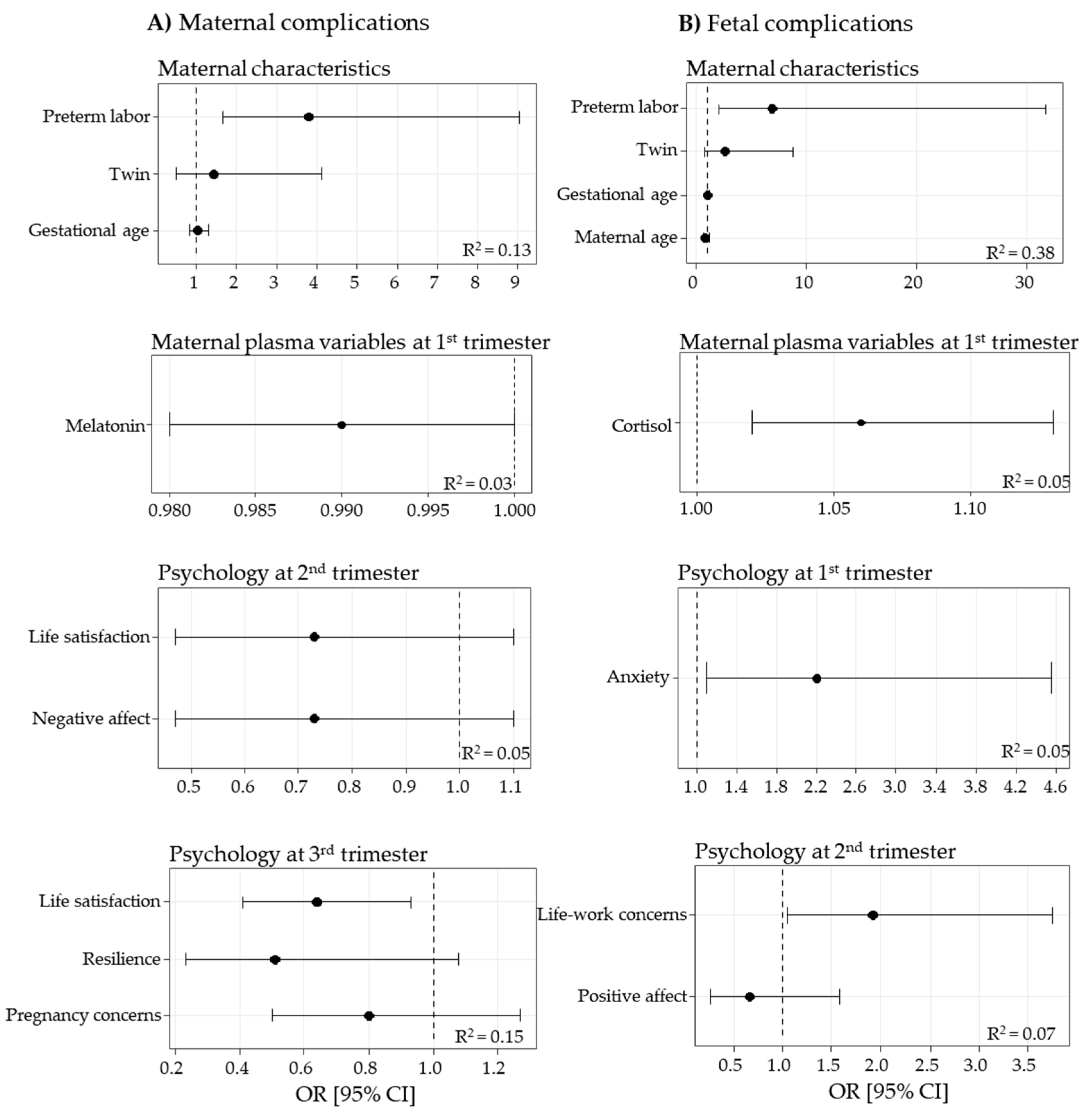
3.4. Logistic Regression Models Associated with Maternal and Fetal Complications
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Varea, C.; Teran, J.M.; Bernis, C.; Bogin, B. The impact of delayed maternity on foetal growth in Spain: An assessment by population attributable fraction. Women Birth 2018, 31, e190–e196. [Google Scholar] [CrossRef]
- Nicoloro-SantaBarbara, J.M.; Lobel, M.; Bocca, S.; Stelling, J.R.; Pastore, L.M. Psychological and emotional concomitants of infertility diagnosis in women with diminished ovarian reserve or anatomical cause of infertility. Fertil. Steril. 2017, 108, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Ramiro-Cortijo, D.; Herrera, T.; Rodriguez-Rodriguez, P.; Lopez De Pablo, A.L.; De La Calle, M.; Lopez-Gimenez, M.R.; Mora-Urda, A.I.; Gutierrez-Arzapalo, P.Y.; Gomez-Rioja, R.; Aguilera, Y.; et al. Maternal plasma antioxidant status in the first trimester of pregnancy and development of obstetric complications. Placenta 2016, 47, 37–45. [Google Scholar] [CrossRef]
- Cheong-See, F.; Schuit, E.; Arroyo-Manzano, D.; Khalil, A.; Barrett, J.; Joseph, K.S.; Asztalos, E.; Hack, K.; Lewi, L.; Lim, A.; et al. Prospective risk of stillbirth and neonatal complications in twin pregnancies: Systematic review and meta-analysis. BMJ 2016, 354, i4353. [Google Scholar] [CrossRef]
- APA. Pregnancy Statistics. Available online: https://americanpregnancy.org/ (accessed on 20 March 2019).
- Edozien, L.C. Beyond biology: The biopsychosocial model and its application in obstetrics and gynaecology. BJOG 2015, 122, 900–903. [Google Scholar] [CrossRef]
- Ng, D.M.; Jeffery, R.W. Relationships between perceived stress and health behaviors in a sample of working adults. Health Psychol. 2003, 22, 638–642. [Google Scholar] [CrossRef] [PubMed]
- Nicoloro-SantaBarbara, J.; Busso, C.; Moyer, A.; Lobel, M. Just relax and you'll get pregnant? Meta-analysis examining women's emotional distress and the outcome of assisted reproductive technology. Soc. Sci. Med. 2018, 213, 54–62. [Google Scholar] [CrossRef]
- Robakis, T.K.; Williams, K.E.; Crowe, S.; Kenna, H.; Gannon, J.; Rasgon, N.L. Optimistic outlook regarding maternity protects against depressive symptoms postpartum. Arch Womens Ment. Health 2015, 18, 197–208. [Google Scholar] [CrossRef]
- Hermes, M.; Antonow-Schlorke, I.; Hollstein, D.; Kuehnel, S.; Rakers, F.; Frauendorf, V.; Dreiling, M.; Rupprecht, S.; Schubert, H.; Witte, O.W.; et al. Maternal psychosocial stress during early gestation impairs fetal structural brain development in sheep. Stress 2020, 23, 233–242. [Google Scholar] [CrossRef]
- Claustrat, B.; Brun, J.; Chazot, G. The basic physiology and pathophysiology of melatonin. Sleep Med. Rev. 2005, 9, 11–24. [Google Scholar] [CrossRef] [PubMed]
- Soliman, A.; Lacasse, A.A.; Lanoix, D.; Sagrillo-Fagundes, L.; Boulard, V.; Vaillancourt, C. Placental melatonin system is present throughout pregnancy and regulates villous trophoblast differentiation. J. Pineal Res. 2015, 59, 38–46. [Google Scholar] [CrossRef]
- Gomes, P.R.L.; Motta-Teixeira, L.C.; Gallo, C.C.; Carmo Buonfiglio, D.D.; Camargo, L.S.; Quintela, T.; Reiter, R.J.; Amaral, F.G.D.; Cipolla-Neto, J. Maternal pineal melatonin in gestation and lactation physiology, and in fetal development and programming. Gen. Comp. Endocrinol. 2020, 300, 113633. [Google Scholar] [CrossRef]
- Reiter, R.J.; Tamura, H.; Tan, D.X.; Xu, X.Y. Melatonin and the circadian system: Contributions to successful female reproduction. Fertil. Steril. 2014, 102, 321–328. [Google Scholar] [CrossRef]
- Ramiro-Cortijo, D.; Calle, M.; Rodriguez-Rodriguez, P.; Pablo, A.L.L.; Lopez-Gimenez, M.R.; Aguilera, Y.; Martin-Cabrejas, M.A.; Gonzalez, M.D.C.; Arribas, S.M. Maternal Antioxidant Status in Early Pregnancy and Development of Fetal Complications in Twin Pregnancies: A Pilot Study. Antioxidants (Basel) 2020, 9, 269. [Google Scholar] [CrossRef]
- Sundberg, I.; Rasmusson, A.J.; Ramklint, M.; Just, D.; Ekselius, L.; Cunningham, J.L. Daytime melatonin levels in saliva are associated with inflammatory markers and anxiety disorders. Psychoneuroendocrinology 2020, 112, 104514. [Google Scholar] [CrossRef]
- Abbott, S.M. Non-24-hour Sleep-Wake Rhythm Disorder. Neurol. Clin. 2019, 37, 545–552. [Google Scholar] [CrossRef]
- Quax, R.A.; Manenschijn, L.; Koper, J.W.; Hazes, J.M.; Lamberts, S.W.; van Rossum, E.F.; Feelders, R.A. Glucocorticoid sensitivity in health and disease. Nat. Rev. Endocrinol. 2013, 9, 670–686. [Google Scholar] [CrossRef]
- Shelton, M.M.; Schminkey, D.L.; Groer, M.W. Relationships among prenatal depression, plasma cortisol, and inflammatory cytokines. Biol. Res. Nurs. 2015, 17, 295–302. [Google Scholar] [CrossRef]
- Sarkar, P.; Bergman, K.; O.′Connor, T.G.; Glover, V. Maternal antenatal anxiety and amniotic fluid cortisol and testosterone: Possible implications for foetal programming. J. Neuroendocr. 2008, 20, 489–496. [Google Scholar] [CrossRef]
- Bleker, L.S.; Roseboom, T.J.; Vrijkotte, T.G.; Reynolds, R.M.; de Rooij, S.R. Determinants of cortisol during pregnancy—The ABCD cohort. Psychoneuroendocrinology 2017, 83, 172–181. [Google Scholar] [CrossRef]
- Aguilera, Y.; Rebollo-Hernanz, M.; Herrera, T.; Cayuelas, L.T.; Rodriguez-Rodriguez, P.; de Pablo, A.L.; Arribas, S.M.; Martin-Cabrejas, M.A. Intake of bean sprouts influences melatonin and antioxidant capacity biomarker levels in rats. Food Funct. 2016, 7, 1438–1445. [Google Scholar] [CrossRef]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Pers. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef]
- Moriondo, M.; Palma, P.; Medrano, L.A.; Murillo, P. Adaptación de la Escala de Afectividad Positiva y Negativa (PANAS) a la población de Adultos de la ciudad de Córdoba. Univ. Psychol. 2012, 11, 187–196. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Lopez-Roig, S.; Terol, C.M.; Pastor, M.A. Ansiedad y depresión. Validación de la Escala HAD en pacientes oncológicos. Rev. Psicol. Salud. 2000, 12, 127–155. [Google Scholar]
- Fernández, J.M.; Pedrero, E.F. Diez pasos para la construcción de un test. Psicothema 2019, 31, 7–16. [Google Scholar]
- Ramiro-Cortijo, D.; de la Calle, M.; Gila-Diaz, A.; Moreno-Jimenez, B.; Martin-Cabrejas, M.A.; Arribas, S.M.; Garrosa, E. Maternal Resources, Pregnancy Concerns, and Biological Factors Associated to Birth Weight and Psychological Health. J. Clin. Med. 2021, 10, 695. [Google Scholar] [CrossRef] [PubMed]
- Scheier, M.F.; Carver, C.S.; Bridges, M.W. Distinguishing optimism from neuroticism (and trait anxiety, self-mastery, and self-esteem): A reevaluation of the Life Orientation Test. J. Pers. Soc. Psychol. 1994, 67, 1063–1078. [Google Scholar] [CrossRef] [PubMed]
- Ferrando, P.J.; Chico, E.; Tous, J.M. Propiedades psicométricas del test de optimismo Life Orientation Test. Psicothema 2002, 14, 673–680. [Google Scholar]
- Wagnild, G.M.; Young, H.M. Development and psychometric evaluation of the Resilience Scale. J. Nurs. Meas. 1993, 1, 165–178. [Google Scholar]
- Rodriguez, M.; Pereyra, M.G.; Gil, E.; Jofre, M.; De Bortoli, M.; Labiano, L.M. Propiedades psicométricas de la escala de resiliencia versión argentina. Rev. Evaluar. 2009, 9, 72–82. [Google Scholar]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The Satisfaction with Life Scale. J. Pers. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef]
- Cabañero Martínez, M.J.; Richart Martínez, M.R.; Cabrero García, J.; Orts Cortés, M.I.; Reig Ferrer, A.; Tosal Herrero, B. Fiabilidad y validez de la Escala de Satisfacción con la Vida de Diener en una muestra de mujeres embarazadas y puérperas. Psicothema 2004, 16, 448–455. [Google Scholar]
- Konnikova, Y.; Zaman, M.M.; Makda, M.; D'Onofrio, D.; Freedman, S.D.; Martin, C.R. Late Enteral Feedings Are Associated with Intestinal Inflammation and Adverse Neonatal Outcomes. PLoS ONE 2015, 10, e0132924. [Google Scholar] [CrossRef] [PubMed]
- Jackson, W.M.; O'Shea, T.M.; Allred, E.N.; Laughon, M.M.; Gower, W.A.; Leviton, A. Risk factors for chronic lung disease and asthma differ among children born extremely preterm. Pediatr. Pulmonol. 2018, 53, 1533–1540. [Google Scholar] [CrossRef]
- Ramiro-Cortijo, D.; Rodríguez-Rodríguez, P.; Lopez De Pablo, Á.L.; López-Giménez, M.R.; González, M.C.; Arribas, S.M. Fetal undernutrition and oxidative stress: Influence of sex and gender. In Handbook of Famine, Starvation and Nutrient Deprivation: From Biology to Policy; Preedy, V.R., Patel, V.B., Eds.; Springer International Publishing: Springer Nature Switzerland AG: London, UK, 2019; pp. 1–19. [Google Scholar]
- Avnon, T.; Haham, A.; Many, A. Twin pregnancy in women above the age of 45 years: Maternal and neonatal outcomes. J. Perinat. Med. 2017, 45, 787–791. [Google Scholar] [CrossRef]
- Berkman, L.F.; Soh, Y. Social Determinants of Health at Older Ages: The Long Arm of Early and Middle Adulthood. Perspect. Biol. Med. 2017, 60, 595–606. [Google Scholar] [CrossRef]
- Okun, N.; Sierra, S.; Genetics, C.; Special, C. Pregnancy outcomes after assisted human reproduction. J. Obstet. Gynaecol. Can. 2014, 36, 64–83. [Google Scholar] [CrossRef]
- Jauniaux, E.; Ben-Ami, I.; Maymon, R. Do assisted-reproduction twin pregnancies require additional antenatal care? Reprod. Biomed. Online 2013, 26, 107–119. [Google Scholar] [CrossRef]
- Glover, V. Maternal depression, anxiety and stress during pregnancy and child outcome; what needs to be done. Best Pract. Res. Clin. Obstet. Gynaecol. 2014, 28, 25–35. [Google Scholar] [CrossRef]
- Tani, F.; Castagna, V. Maternal social support, quality of birth experience, and post-partum depression in primiparous women. J. Matern. Fetal. Neonatal. Med. 2017, 30, 689–692. [Google Scholar] [CrossRef]
- Preis, H.; Chen, R.; Eisner, M.; Pardo, J.; Peled, Y.; Wiznitzer, A.; Benyamini, Y. Testing a biopsychosocial model of the basic birth beliefs. Birth 2018, 45, 79–87. [Google Scholar] [CrossRef]
- Sheiham, A. Closing the gap in a generation: Health equity through action on the social determinants of health. A report of the WHO Commission on Social Determinants of Health (CSDH) 2008. Community Dent. Health 2009, 26, 2–3. [Google Scholar]
- Rowe, H. Biopsychosocial obstetrics and gynaecology—A perspective from Australia. J. Psychosom. Obstet. Gynaecol. 2016, 37, 1–5. [Google Scholar] [CrossRef]
- Lindquist, A.; Noor, N.; Sullivan, E.; Knight, M. The impact of socioeconomic position on severe maternal morbidity outcomes among women in Australia: A national case-control study. BJOG 2015, 122, 1601–1609. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, I.M.; Zimmerman, M.C.; Moore, T.A. Oxidative stress in early pregnancy and the risk of preeclampsia. Pregnancy Hypertens 2019, 18, 99–102. [Google Scholar] [CrossRef]
- Hobfoll, S.E. Conservation of Resources Theory: Its Implication for Stress, Health, and Resilience. In The Oxford Handbook of Stress, Health, and Coping; Folkman, S., Ed.; Oxford University Press: New York, NY, USA, 2011; pp. 1–38. [Google Scholar]
- Edwards, J.R.; Rothbard, N.P. Work and family stress and well-being: An integrative model of person-environment fit within and between the work and family domains. Organ. Behav. Hum. Decis. Process. 2004, 77, 85–129. [Google Scholar] [CrossRef]
- Ten Brummelhuis, L.L.; Bakker, A.B. A resource perspective on the work-home interface: The work-home resources model. Am. Psychol. 2012, 67, 545–556. [Google Scholar] [CrossRef]
- Mastorakos, G.; Ilias, I. Maternal and fetal hypothalamic-pituitary-adrenal axes during pregnancy and postpartum. Ann. N. Y. Acad. Sci. 2003, 997, 136–149. [Google Scholar] [CrossRef]
- Merlot, E.; Couret, D.; Otten, W. Prenatal stress, fetal imprinting and immunity. Brain Behav. Immun. 2008, 22, 42–51. [Google Scholar] [CrossRef]
- Brunton, P.J. Effects of maternal exposure to social stress during pregnancy: Consequences for mother and offspring. Reproduction 2013, 146, R175–R189. [Google Scholar] [CrossRef]
- Monk, C. Stress and mood disorders during pregnancy: Implications for child development. Psychiatr. Q. 2001, 72, 347–357. [Google Scholar] [CrossRef]
- Littleton, H.L.; Bye, K.; Buck, K.; Amacker, A. Psychosocial stress during pregnancy and perinatal outcomes: A meta-analytic review. J. Psychosom Obstet. Gynaecol. 2010, 31, 219–228. [Google Scholar] [CrossRef]
- Collins, C.S.; Stockton, C.M. The Central Role of Theory in Qualitative Research. Int. J. Qual. Methods 2018, 17, 1–10. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Cronbach’s α | 1T | 2T | 3T | |
|---|---|---|---|---|
| Maternal and neonatal data | - | X | X | X |
| Maternal plasma variables | - | X | ||
| Maternal psychological variables | ||||
| Negative affect | 0.80 | X | X | X |
| Positive affect | 0.73 | X | X | X |
| Anxiety | 0.84 | X | X | X |
| Pregnancy concerns | 0.82 | X | X | X |
| Optimism | 0.66 | X | X | |
| Resilience | 0.66 | X | X | |
| Life satisfaction | 0.87 | X | X | |
| Life–work conflicts | 0.88 | X | ||
| Maternal Complications | Fetal Complications | |||||
|---|---|---|---|---|---|---|
| No (n = 98) | Yes (n = 84) | p-Value | No (n = 125) | Yes (n = 45) | p-Value | |
| Maternal age (years) | 35.0 (6.0) | 35.0 (7.0) | 0.51 | 34.0 (6.0) | 35.0 (5.0) | 0.039 |
| Civil status | ||||||
| Single | 26.6% (21) | 26.7% (24) | 0.40 | 28.3% (33) | 27.5% (11) | 0.87 |
| Married | 73.4% (58) | 71.1% (64) | 71.8% (84) | 72.5% (29) | ||
| Educational level | ||||||
| Undergraduate | 21.0% (17) | 34.5% (32) | 0.49 | 27.3% (33) | 29.2% (12) | 0.77 |
| Graduate | 77.7% (63) | 64.5% (60) | 71.1% (86) | 70.7% (29) | ||
| Employment situation | ||||||
| Working | 93.8% (76) | 87.1% (81) | 0.16 | 91.7% (111) | 85.4% (35) | 0.25 |
| Unemployment | 6.2% (5) | 9.7% (9) | 5.7% (7) | 14.6% (6) | ||
| Smoking habits | 14.8% (12) | 17.2% (16) | 0.61 | 14.0% (17) | 19.5% (8) | 0.35 |
| Alcohol intake | 42.0% (34) | 39.1% (36) | 0.70 | 38.3% (46) | 48.8% (20) | 0.24 |
| Gestational age (weeks) | 38.0 (3.0) | 37.5 (2.0) | 0.006 | 38.0 (2.4) | 35.8 (2.5) | 0.001 |
| Twin pregnancies | 38.1% (37) | 67.5% (56) | 0.001 | 41.9% (52) | 80.0% (36) | 0.001 |
| ART | 25.5% (25) | 49.4% (41) | 0.001 | 28.0% (35) | 60.0% (27) | 0.001 |
| Male 1 | 52.3% (46) | 60.8% (48) | 0.27 | 57.6% (68) | 51.3% (20) | 0.49 |
| Male 2 | 41.9% (13) | 52.9% (27) | 0.33 | 54.2% (26) | 42.9% (12) | 0.34 |
| Preterm labor | 17% (16) | 32.9% (26) | 0.015 | 0% (0) | 52.4% (22) | 0.001 |
| Fetal growth restriction | 4.3% (4) | 12.2% (9) | 0.060 | 0% (0) | 33.3% (15) | 0.001 |
| First Trimester | Second Trimester | Third Trimester | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ref. | Maternal Complic. | Fetal Complic. | Ref. | Maternal Complic. | Fetal Complic. | Ref. | Maternal Complic. | Fetal Complic. | |||||||||||||
| No | Yes | p-Value | No | Yes | p-Value | No | Yes | p-Value | No | Yes | p-Value | No | Yes | p-Value | No | Yes | p-Value | ||||
| Negative affect | 1.7 (0.7) | 1.8 (0.8) | 2.0 (1.0) | 0.16 | 1.8 (0.8) | 2.1 (0.7) | 0.13 | 1.7 (0.8) | 1.8 (0.8) | 2.0 (0.7) | 0.054 | 1.8 (0.9) | 2.0 (0.8) | 0.12 | 1.9 (1.1) | 1.9 (1.1) | 2.1 (1.0) | 0.15 | 2.0 (0.9) | 2.1 (1.1) | 0.49 |
| Positive affect | 3.4 (0.7) | 3.4 (0.7) | 3.3 (0.8) | 0.76 | 3.3 (0.8) | 3.3 (0.9) | 0.63 | 3.5 (0.8) | 3.4 (0.8) | 3.4 (0.8) | 0.80 | 3.4 (0.7) | 3.2 (0.7) | 0.056 | 3.6 (0.7) | 3.5 (0.7) | 3.5 (0.8) | 0.36 | 3.5 (0.8) | 3.5 (0.7) | 0.81 |
| Anxiety | 0.9 (0.6) | 0.9 (0.7) | 0.9 (0.7) | 0.90 | 0.9 (0.6) | 1.1 (0.7) | 0.041 | 1.0 (0.9) | 1.0 (0.9) | 1.0 (0.9) | 0.62 | 1.0 (0.7) | 1.1 (1.1) | 0.18 | 0.9 (0.7) | 1.0 (0.7) | 1.1 (1.0) | 0.14 | 1.0 (0.9) | 1.1 (1.0) | 0.36 |
| Pregnancy concerns | 1.6 (0.1) | 1.6 (0.7) | 1.7 (0.7) | 0.96 | 1.7 (0.8) | 1.6 (0.7) | 0.52 | 1.8 (0.1) | 1.8 (0.9) | 1.8 (0.8) | 0.68 | 1.7 (0.8) | 1.9 (0.8) | 0.78 | 1.9 (0.1) | 1.9 (0.7) | 1.8 (0.8) | 0.063 | 1.9 (0.8) | 1.8 (0.8) | 0.83 |
| Optimism | 3.4 (0.9) | 3.4 (1.4) | 3.2 (1.2) | 0.28 | 3.2 (1.2) | 3.6 (1.4) | 0.28 | - | - | - | - | - | - | - | 3.4 (0.9) | 3.4 (0.9) | 3.2 (1.0) | 0.49 | 3.2 (0.8) | 3.5 (1.0) | 0.17 |
| Resilience | 6.0 (0.1) | 6.2 (0.7) | 6.0 (1.0) | 0.20 | 6.0 (0.8) | 6.2 (0.7) | 0.35 | - | - | - | - | - | - | - | 3.0 (0.1) | 6.0 (0.9) | 5.3 (1.8) | 0.001 | 5.7 (1.2) | 5.7 (1.5) | 0.47 |
| Life satisfaction | - | - | - | - | - | - | - | 5.8 (0.9) | 5.8 (0.9) | 5.5 (1.0) | 0.015 | 5.8 (1.1) | 5.6 (1.2) | 0.59 | 5.8 (0.8) | 5.8 (1.0) | 5.4 (1.2) | 0.010 | 5.8 (1.0) | 5.6 (1.8) | 0.61 |
| Life–work conflicts | - | - | - | - | - | - | - | 0.8 (0.1) | 0.8 (1.0) | 1.0 (1.3) | 0.70 | 0.8 (1.2) | 1.2 (1.2) | 0.061 | - | - | - | - | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramiro-Cortijo, D.; de la Calle, M.; Benitez, V.; Gila-Diaz, A.; Moreno-Jiménez, B.; Arribas, S.M.; Garrosa, E. Maternal Psychological and Biological Factors Associated to Gestational Complications. J. Pers. Med. 2021, 11, 183. https://doi.org/10.3390/jpm11030183
Ramiro-Cortijo D, de la Calle M, Benitez V, Gila-Diaz A, Moreno-Jiménez B, Arribas SM, Garrosa E. Maternal Psychological and Biological Factors Associated to Gestational Complications. Journal of Personalized Medicine. 2021; 11(3):183. https://doi.org/10.3390/jpm11030183
Chicago/Turabian StyleRamiro-Cortijo, David, Maria de la Calle, Vanesa Benitez, Andrea Gila-Diaz, Bernardo Moreno-Jiménez, Silvia M. Arribas, and Eva Garrosa. 2021. "Maternal Psychological and Biological Factors Associated to Gestational Complications" Journal of Personalized Medicine 11, no. 3: 183. https://doi.org/10.3390/jpm11030183
APA StyleRamiro-Cortijo, D., de la Calle, M., Benitez, V., Gila-Diaz, A., Moreno-Jiménez, B., Arribas, S. M., & Garrosa, E. (2021). Maternal Psychological and Biological Factors Associated to Gestational Complications. Journal of Personalized Medicine, 11(3), 183. https://doi.org/10.3390/jpm11030183