
The Impact of Sclerostin Levels on Long-Term Prognosis in Patients Undergoing Coronary Angiography: A Personalized Approach with 9-Year Follow-Up

 ,
,  ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Coronary Artery Disease Advancement
2.3. Clinical Data
2.4. Biochemical Data
2.5. Endpoints and Definitions
2.6. Statistical Analysis
3. Results
3.1. Study Population
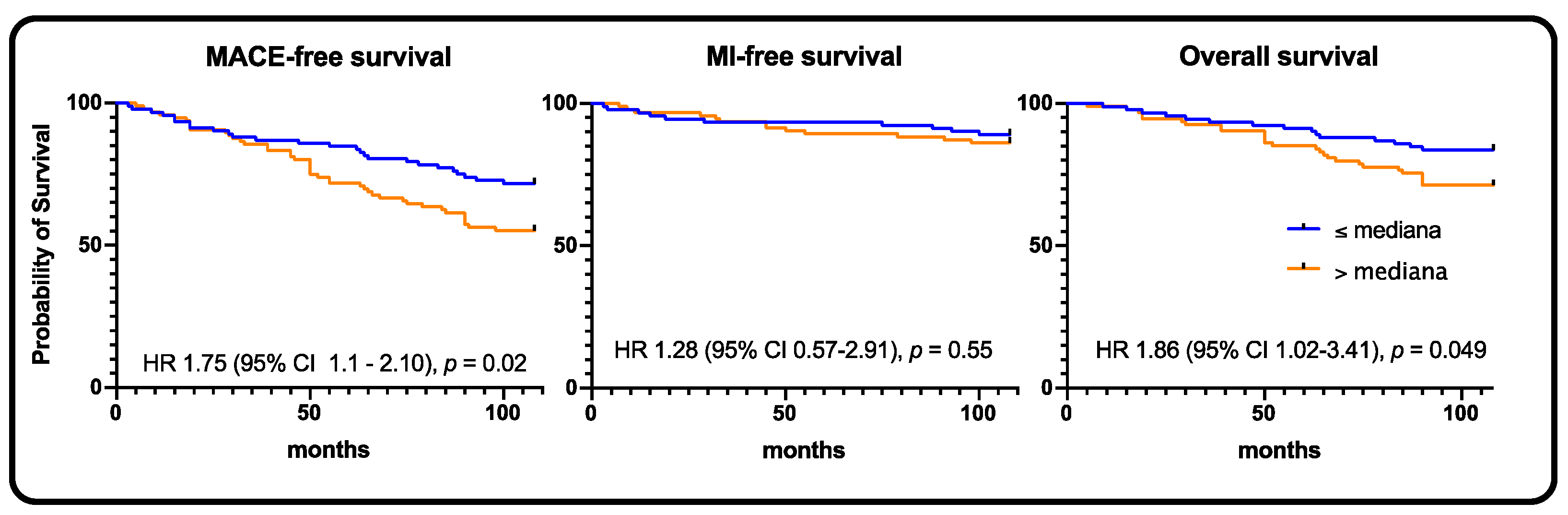
3.2. Whole Population Survival Analysis
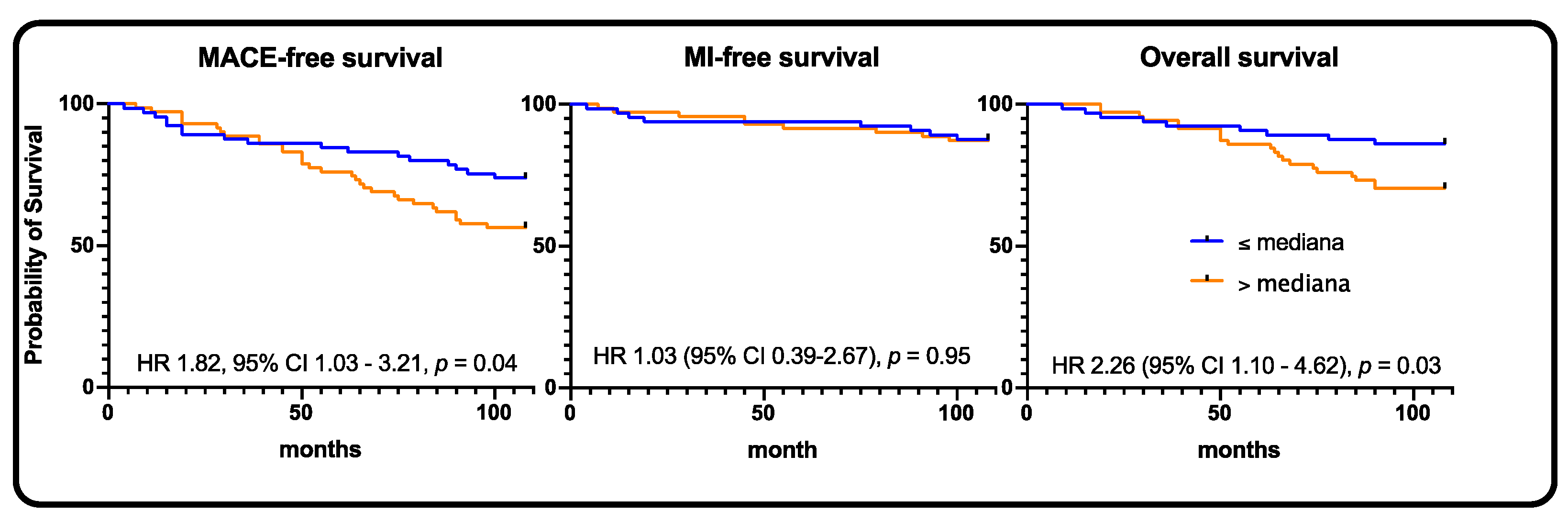
3.3. Chronic Coronary Syndrome and Acute Coronary Syndrome Subgroups Survival Analysis
3.4. SYNTAX Subgroups Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dallas, S.L.; Prideaux, M.; Bonewald, L.F. The osteocyte: An endocrine cell and more. Endocr. Rev. 2013, 34, 658–690. [Google Scholar] [CrossRef] [PubMed]
- Tresguerres, F.; Torres, J.; López-Quiles, J.; Hernández, G.; Vega, J.; Tresguerres, I. The osteocyte: A multifunctional cell within the bone. Ann. Anat.—Anat. Anz. 2020, 227, 151422. [Google Scholar] [CrossRef]
- Carlson, N.; Axelsen, M.; Mortensen, O.H.; Pedersen, R.S.; Heaf, J.G. Clearance of Sclerostin, Osteocalcin, Fibroblast Growth Factor 23, and Osteoprotegerin by Dialysis. Blood Purif. 2017, 44, 122–128. [Google Scholar] [CrossRef]
- Andrukhova, O.; Slavic, S.; Smorodchenko, A.; Zeitz, U.; Shalhoub, V.; Lanske, B.; E Pohl, E.; Erben, R.G. FGF 23 regulates renal sodium handling and blood pressure. EMBO Mol. Med. 2014, 6, 744–759. [Google Scholar] [CrossRef] [PubMed]
- Delanaye, P.; Cavalier, E.; Bouquegneau, A.; Khwaja, A. Sclerostin levels in CKD patients: An important, but not definitive, step on the way to clinical use. Kidney Int. 2015, 88, 1221–1223. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Evrard, S.; Delanaye, P.; Kamel, S.; Cristol, J.P.; Cavalier, E. Calcifications SSjwgov. Vascular calcification: From pathophysiology to biomarkers. Clin. Chim. Acta 2015, 438, 401–414. [Google Scholar] [CrossRef]
- Kirkpantur, A.; Balci, M.; Turkvatan, A.; Afsar, B. Independent association between serum sclerostin levels and carotid artery atherosclerosis in prevalent haemodialysis patients. Clin. Kidney J. 2015, 8, 737–743. [Google Scholar] [CrossRef]
- Muto, P.; Gullo, A.L.; Mandraffino, G.; Loddo, S.; Atteritano, M. High levels of serum sclerostin and DKK1 in a case of Klippel-Trénaunay syndrome. Osteoporos. Int. 2018, 29, 1679–1681. [Google Scholar] [CrossRef]
- Morales-Santana, S.; García-Fontana, B.; García-Martín, A.; Rozas-Moreno, P.; García-Salcedo, J.A.; Reyes-García, R.; Muñoz-Torres, M. Atherosclerotic Disease in Type 2 Diabetes Is Associated With an Increase in Sclerostin Levels. Diabetes Care 2013, 36, 1667–1674. [Google Scholar] [CrossRef] [PubMed]
- Bruzzese, A.; Lacquaniti, A.; Cernaro, V.; Ricciardi, C.A.; Loddo, S.; Romeo, A.; Montalto, G.; Costantino, G.; Torre, F.; Pettinato, G.; et al. Sclerostin levels in uremic patients: A link between bone and vascular disease. Ren. Fail. 2016, 38, 759–764. [Google Scholar] [CrossRef]
- Teng, I.-C.; Wang, J.-H.; Lee, C.-J.; Hou, J.-S.; Hsu, B.-G. Serum sclerostin as an independent marker of peripheral artery disease in elderly persons. Int J. Clin. Exp. Pathol 2018, 11, 2816–2821. [Google Scholar] [PubMed]
- He, W.; Li, C.; Chen, Q.; Xiang, T.; Wang, P.; Pang, J. Serum sclerostin and adverse outcomes in elderly patients with stable coronary artery disease undergoing percutaneous coronary intervention. Aging Clin. Exp. Res. 2020, 32, 2065–2072. [Google Scholar] [CrossRef]
- Kern, A.; Stompor, T.; Bil, J. Sclerostin and cardiovascular disease: Any prognostic implications? Authors’ reply. Kardiologia Polska 2021, 79, 100. [Google Scholar] [CrossRef] [PubMed]
- Kern, A.; Stompor, T.; Kiewisz, J.; Krazinski, B.E.; Kiezun, J.; Kiezun, M.; Gorny, J.; Sienkiewicz, E.; Drozdowska, B.; Bil, J. Association of serum sclerostin levels with atherosclerosis severity in patients referred for invasive coronary angiography. Kardiol. Pol. 2020, 78, 1271–1273. [Google Scholar] [PubMed]
- Neumann, F.-J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; A Byrne, R.; Collet, J.-P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Hear. J. 2018, 40, 87–165. [Google Scholar] [CrossRef]
- Williams, B.; Mancia, G.; Spiering, W.; Rosei, E.A.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.F.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef]
- Cosentino, F.; Grant, P.J.; Aboyans, V.; Bailey, C.J.; Ceriello, A.; Delgado, V.; Federici, M.; Filippatos, G.; Grobbee, D.E.; Hansen, T.B.; et al. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur. Heart J. 2020, 41, 255–323. [Google Scholar] [CrossRef] [PubMed]
- Aboyans, V.; Ricco, J.B.; Bartelink, M.E.L.; Bjorck, M.; Brodmann, M.; Cohnert, T.; Collet, J.P.; Czerny, M.; De Carlo, M.; Debus, S.; et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteriesEndorsed by: The European Stroke Organization (ESO)The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur. Heart J. 2018, 39, 763–816. [Google Scholar]
- Knuuti, J.; Wijns, W.; Achenbach, S.; Agewall, S.; Barbato, E.; Bax, J.J.; Capodanno, D.; Cuisset, T.; Deaton, C.; Dickstein, K.; et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef]
- Bil, J.; Możeńska, O.; Segiet-Święcicka, A.; Gil, R.J. Revisiting the use of the provocative acetylcholine test in patients with chest pain and nonobstructive coronary arteries: A five-year follow-up of the AChPOL registry, with special focus on patients with MINOCA. Transl. Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Catalano, A.; Bellone, F.; Morabito, N.; Corica, F. Sclerostin and Vascular Pathophysiology. Int. J. Mol. Sci. 2020, 21, 4779. [Google Scholar] [CrossRef] [PubMed]
- Figurek, A.; Spasovski, G. Is serum sclerostin a marker of atherosclerosis in patients with chronic kidney disease–mineral and bone disorder? Int. Urol. Nephrol. 2018, 50, 1863–1870. [Google Scholar] [CrossRef] [PubMed]
- Gaudio, A.; Fiore, V.; Rapisarda, R.; Sidoti, M.H.; Xourafa, A.; Catalano, A.; Tringali, G.; Zanoli, L.; Signorelli, S.S.; Fiore, C.E. Sclerostin is a possible candidate marker of arterial stiffness: Results from a cohort study in Catania. Mol. Med. Rep. 2017, 15, 3420–3424. [Google Scholar] [CrossRef] [PubMed]
- Zhao, B.; Chen, A.; Wang, H.; Cui, J.; Sun, Y.; Xu, L.; Mao, Y. The relationship between sclerostin and carotid artery atherosclerosis in patients with stage 3–5 chronic kidney disease. Int. Urol. Nephrol. 2020, 52, 1329–1336. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.; Sun, Y.; Cui, J.; Zhao, B.; Wang, H.; Chen, X.; Mao, Y. Associations of sclerostin with carotid artery atherosclerosis and all-cause mortality in Chinese patients undergoing maintenance hemodialysis. BMC Nephrol. 2018, 19, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Ghardashi-Afousi, A.; Davoodi, M.; Hesamabadi, B.K.-; Asvadi-Fard, M.; Bigi, M.A.B.; Izadi, M.R.; Gaeini, A.A. Improved carotid intima-media thickness-induced high-intensity interval training associated with decreased serum levels of Dkk-1 and sclerostin in type 2 diabetes. J. Diabetes Complicat. 2019, 34, 107469. [Google Scholar] [CrossRef]
- Jean, G.; Chazot, C.; Bresson, E.; Zaoui, E.; Cavalier, E. High Serum Sclerostin Levels Are Associated with a Better Outcome in Haemodialysis Patients. Nephron 2016, 132, 181–190. [Google Scholar] [CrossRef] [PubMed]
- Drechsler, C.; Evenepoel, P.; Vervloet, M.G.; Wanner, C.; Ketteler, M.; Marx, N.; Floege, J.; Dekker, F.W.; Brandenburg, V.M.; NECOSAD Study Group. High levels of circulating sclerostin are associated with better cardiovascular survival in incident dialysis patients: Results from the NECOSAD study. Nephrol. Dial. Transplant. 2014, 30, 288–293. [Google Scholar] [CrossRef]
- Kalousová, M.; Dusilová-Sulková, S.; Kuběna, A.; Zakiyanov, O.; Tesař, V.; Zima, T. Sclerostin levels predict cardiovascular mortality in long-term hemodialysis patients: A prospective observational cohort study. Physiol. Res. 2019, 68, 547–558. [Google Scholar] [CrossRef]
- Zou, Y.; Yang, M.; Wang, J.; Cui, L.; Jiang, Z.; Ding, J.; Li, M.; Zhou, H. Association of sclerostin with cardiovascular events and mortality in dialysis patients. Ren. Fail. 2020, 42, 282–288. [Google Scholar] [CrossRef]
- Klingenschmid, G.; Tschiderer, L.; Himmler, G.; Rungger, G.; Brugger, S.; Santer, P.; Willeit, J.; Kiechl, S.; Willeit, P. Associations of Serum Dickkopf-1 and Sclerostin With Cardiovascular Events: Results From the Prospective Bruneck Study. J. Am. Hear. Assoc. 2020, 9. [Google Scholar] [CrossRef] [PubMed]
- Morena, M.; Jaussent, I.; Dupuy, A.-M.; Bargnoux, A.-S.; Kuster, N.; Chenine, L.; Leray-Moragues, H.; Klouche, K.; Vernhet, H.; Canaud, B.; et al. Osteoprotegerin and sclerostin in chronic kidney disease prior to dialysis: Potential partners in vascular calcifications. Nephrol. Dial. Transplant. 2015, 30, 1345–1356. [Google Scholar] [CrossRef] [PubMed]
- Papaioannou, T.G.; Kalantzis, C.; Katsianos, E.; Sanoudou, D.; Vavuranakis, M.; Tousoulis, D. Personalized Assessment of the Coronary Atherosclerotic Arteries by Intravascular Ultrasound Imaging: Hunting the Vulnerable Plaque. J. Pers. Med. 2019, 9, 8. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Patients n = 205 |
|---|---|
| Baseline characteristics | |
| male | 144 (70.2%) |
| age (years) | 62.9 ± 0.6 |
| BMI (kg/m2) | 27.6 ± 0.3 |
| arterial hypertension | 154 (75.1) |
| dyslipidemia | 107 (52.2) |
| diabetes | 74 (36.1) |
| metabolic syndrome * | 85 (41.5) |
| chronic coronary syndrome | 129 (62.9) |
| acute coronary syndrome | 76 (37.1) |
| left ventricle ejection fraction (%) | 54.8 ± 0.7 |
| SYNTAX score | 15.1 ± 0.8 |
| Laboratory findings | |
| Total cholesterol (mg/dL) | 188.9 ± 3.8 |
| Glucose (mg/dL) | 117.5 ± 2.8 |
| Creatinine (mg/dL) | 0.9 ± 0.01 |
| eGFR (mL/min/1.73 m2) | 86.5 ± 1.6 |
| Phosphate (mg/dL) | 3.15 ± 0.1 |
| Calcium (mg/dL) | 9.06 ± 0.04 |
| Ca x P (mg2/dL2) | 28.6 ± 0.5 |
| Sclerostin (pg/mL) ** | 133.21 (64.0–276.17) |
| iPTH (pg/mL) | 36.1 ± 2.1 |
| KLOTHO (pg/mL) | 232.1 ± 15.0 |
| FGF23 (pg/mL) | 1.37 ± 0.05 |
| Whole Group | Low Sclerostin Group | High Sclerostin Group | |
|---|---|---|---|
| whole population | n = 205 | n = 103 | n = 102 |
| MACE | 70 (34.1) | 26 (25.2) | 44 (43.1) * |
| MI | 23 (11.2) | 10 (9.7) | 13 (12.7) |
| stroke | 5 (2.4) | 1 (0.9) | 4 (3.9) |
| death | 42 (20.5) | 15 (14.6) | 27 (26.5) * |
| chronic coronary syndrome | n = 129 | n = 65 | n = 64 |
| MACE | 42 (32.6) | 14 (21.5) | 28 (43.8) * |
| MI | 13 (10.1) | 6 (9.2) | 7 (10.9) |
| stroke | 1 (0.8) | 0 | 1 (1.6) |
| death | 28 (21.7) | 8 (12.3) | 20 (31.3) * |
| acute coronary syndrome | n = 76 | n = 39 | n = 37 |
| MACE | 28 (36.8) | 12 (30.8) | 16 (43.2) |
| MI | 10 (13.2) | 4 (10.3) | 6 (16.2) |
| stroke | 4 (5.3) | 1 (2.6) | 3 (8.1) |
| death | 14 (18.4) | 7 (17.9) | 7 (18.9) |
| SYNTAX 0–22 | n = 145 | n = 73 | n = 72 |
| MACE | 49 (33.8) | 17 (23.3) | 32 (44.4) * |
| MI | 17 (11.7) | 8 (10.9) | 9 (12.5) |
| stroke | 2 (13.8) | 0 | 2 (2.8) |
| death | 30 (20.7) | 9 (12.3) | 21 (29.2) * |
| SYNTAX 23–32 | n = 38 | n = 20 | n = 18 |
| MACE | 14 (36.8) | 5 (25) | 9 (50) |
| MI | 4 (10.5) | 1 (5.0) | 3 (16.7) |
| stroke | 2 (5.3) | 1 (5.0) | 1 (5.6) |
| death | 8 (21.1) | 3 (15.0) | 5 (27.8) |
| SYNTAX ≥ 33 | n = 22 | n = 12 | n = 10 |
| MACE | 7 (31.8) | 4 (33.3) | 3 (30) |
| MI | 2 (9.1) | 1 (8.3) | 1 (10) |
| stroke | 1 (4.5) | 0 | 1 (10) |
| death | 4 (18.2) | 3 (25) | 1 (10) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kern, A.; Stompór, T.; Kiewisz, J.; Kraziński, B.E.; Kiezun, J.; Kiezun, M.; Górny, J.; Sienkiewicz, E.; Gromadziński, L.; Onichimowski, D.; et al. The Impact of Sclerostin Levels on Long-Term Prognosis in Patients Undergoing Coronary Angiography: A Personalized Approach with 9-Year Follow-Up. J. Pers. Med. 2021, 11, 186. https://doi.org/10.3390/jpm11030186
Kern A, Stompór T, Kiewisz J, Kraziński BE, Kiezun J, Kiezun M, Górny J, Sienkiewicz E, Gromadziński L, Onichimowski D, et al. The Impact of Sclerostin Levels on Long-Term Prognosis in Patients Undergoing Coronary Angiography: A Personalized Approach with 9-Year Follow-Up. Journal of Personalized Medicine. 2021; 11(3):186. https://doi.org/10.3390/jpm11030186
Chicago/Turabian StyleKern, Adam, Tomasz Stompór, Jolanta Kiewisz, Bartłomiej E. Kraziński, Jacek Kiezun, Marta Kiezun, Jerzy Górny, Ewa Sienkiewicz, Leszek Gromadziński, Dariusz Onichimowski, and et al. 2021. "The Impact of Sclerostin Levels on Long-Term Prognosis in Patients Undergoing Coronary Angiography: A Personalized Approach with 9-Year Follow-Up" Journal of Personalized Medicine 11, no. 3: 186. https://doi.org/10.3390/jpm11030186
APA StyleKern, A., Stompór, T., Kiewisz, J., Kraziński, B. E., Kiezun, J., Kiezun, M., Górny, J., Sienkiewicz, E., Gromadziński, L., Onichimowski, D., & Bil, J. (2021). The Impact of Sclerostin Levels on Long-Term Prognosis in Patients Undergoing Coronary Angiography: A Personalized Approach with 9-Year Follow-Up. Journal of Personalized Medicine, 11(3), 186. https://doi.org/10.3390/jpm11030186