
Image-Guided Localization Techniques for Surgical Excision of Non-Palpable Breast Lesions: An Overview of Current Literature and Our Experience with Preoperative Skin Tattoo

 ,
,  ,
,  ,
,  ,
,  ,
,  , ,
, ,  , ,
, , 
Abstract
1. Introduction
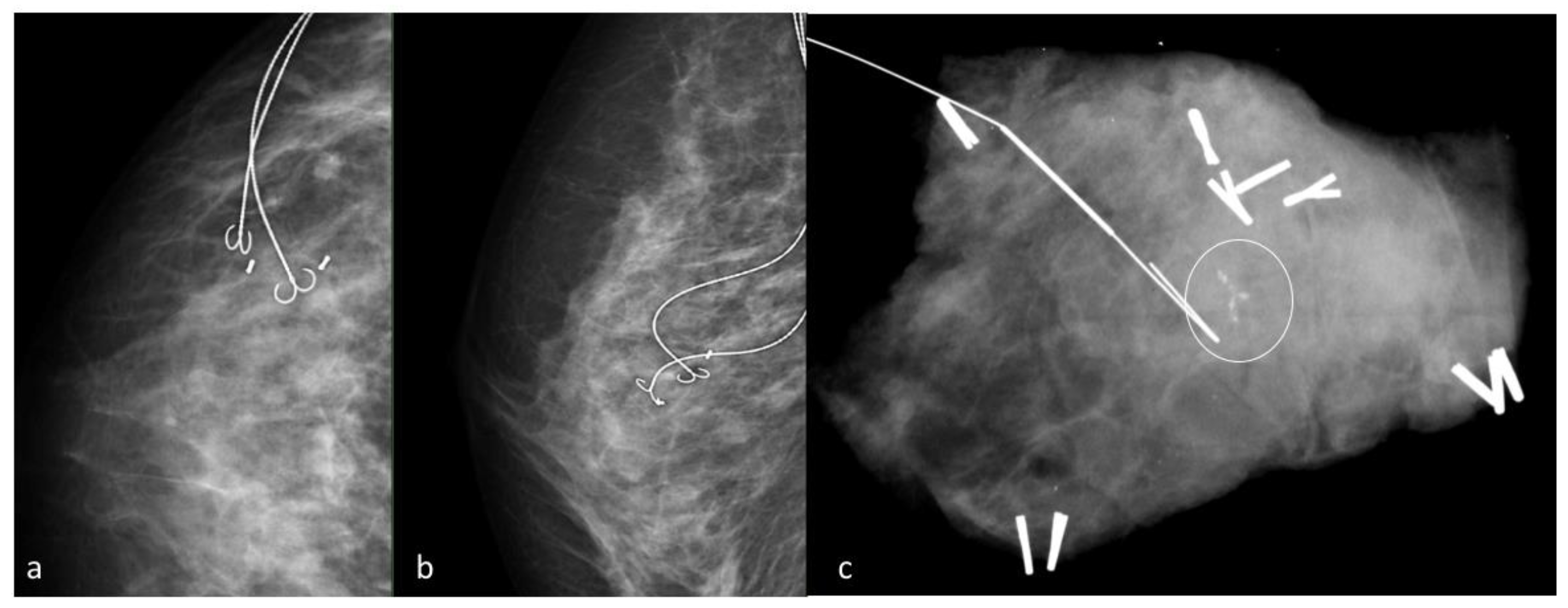
2. Wire Guided Localization
3. Carbon Marking
4. Radio-Guided Occult Lesion Localization
5. Radioactive Seed Localization
6. Magnetic Seed Localization
7. Radiofrequency Identification Tags
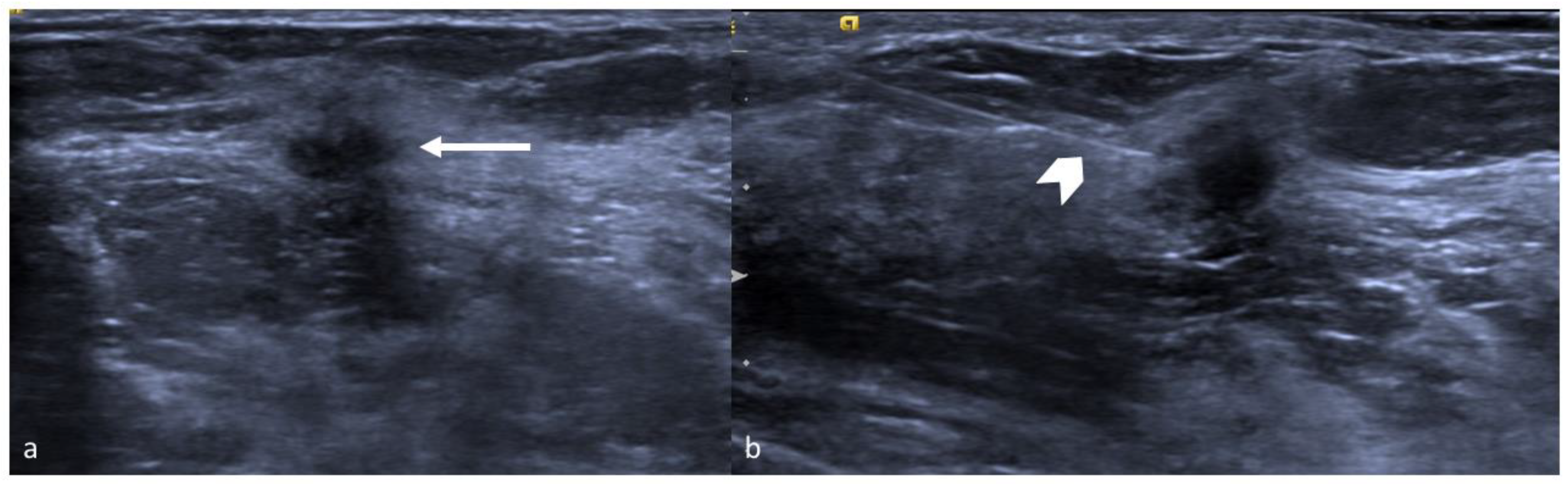
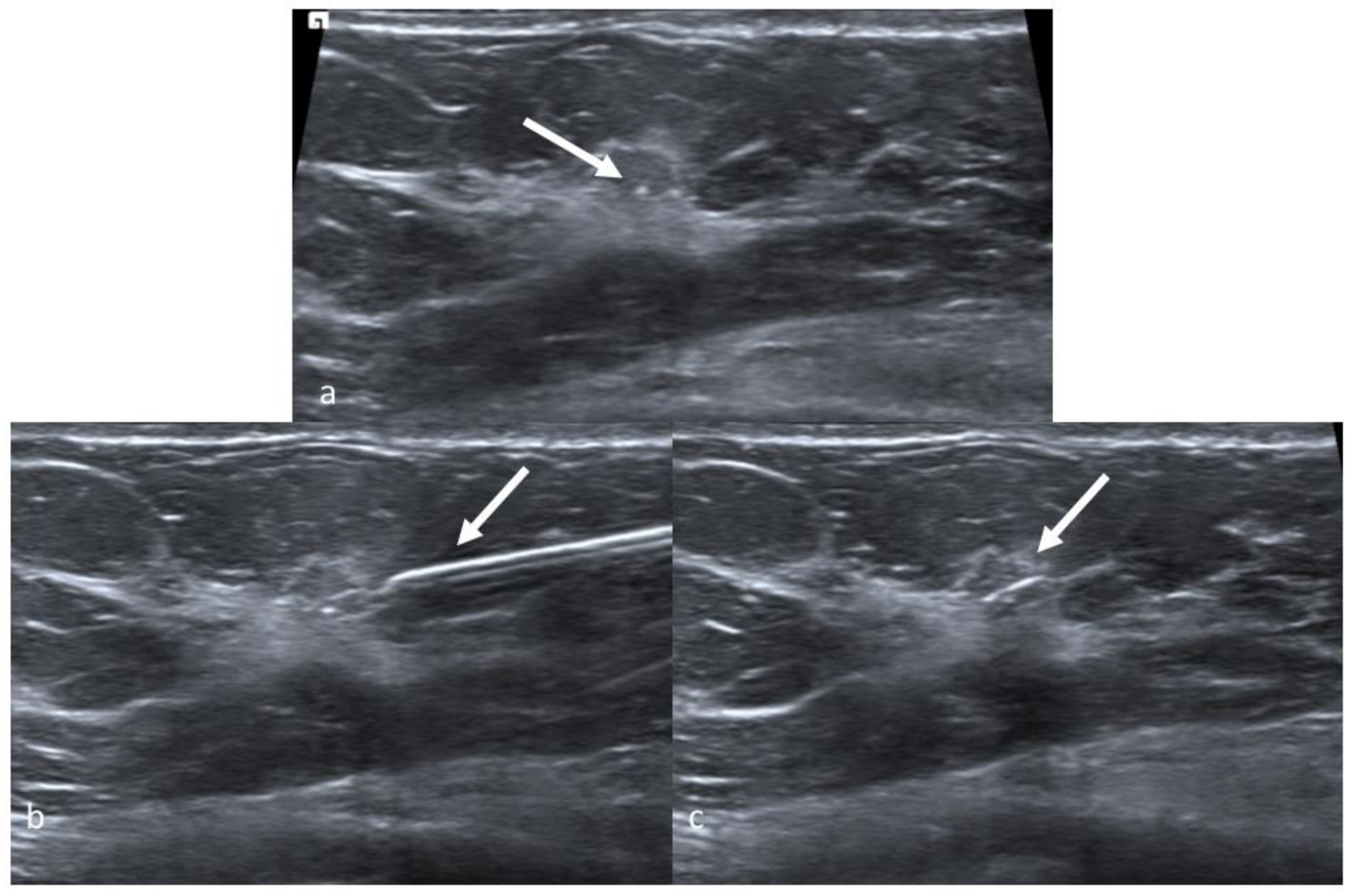
8. Intraoperative Ultrasound
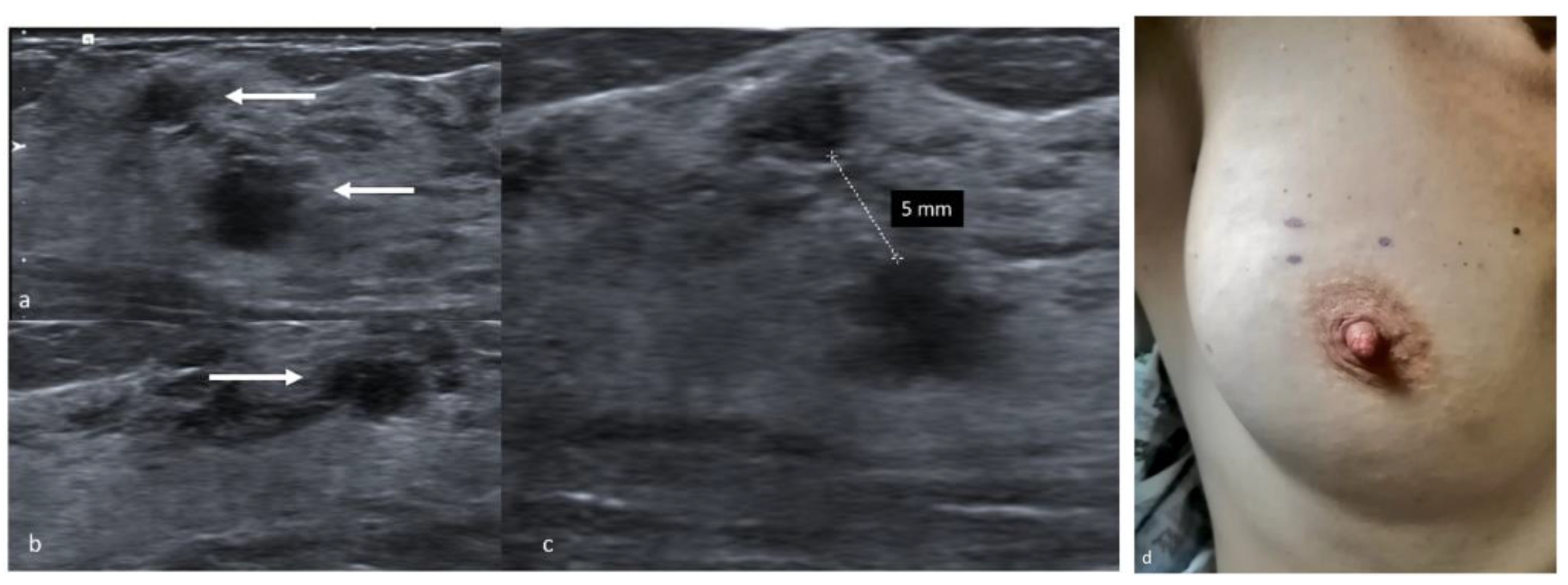
9. Preoperative Localization with a Skin Tattoo
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Sharma, R. Breast cancer incidence, mortality and mortality-to-incidence ratio (MIR) are associated with human development, 1990–2016: Evidence from Global Burden of Disease Study 2016. Breast Cancer 2019, 26, 428–445. [Google Scholar] [CrossRef] [PubMed]
- Moo, T.-A.; Sanford, R.; Dang, C.; Morrow, M. Overview of breast cancer therapy. PET Clin. 2018, 13, 339–354. [Google Scholar] [CrossRef] [PubMed]
- Franceschini, G.; Terribile, D.; Fabbri, C.; Magno, S.; D’Alba, P.; Chiesa, F.; Di Leone, A.; Masetti, R. Management of locally advanced breast cancer. Mini-review. Minerva Chir. 2007, 62, 249–255. Available online: http://europepmc.org/abstract/MED/17641585 (accessed on 8 November 2020). [PubMed]
- Fisher, B.; Anderson, S.; Bryant, J.; Margolese, R.G.; Deutsch, M.; Fisher, E.R.; Jeong, J.-H.; Wolmark, N. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N. Engl. J. Med. 2002, 347, 1233–1241. [Google Scholar] [CrossRef] [PubMed]
- Veronesi, U.; Cascinelli, N.; Mariani, L.; Greco, M.; Saccozzi, R.; Luini, A.; Aguilar, M.; Marubini, E. Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. N. Engl. J. Med. 2002, 347, 1227–1232. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, A.M.; Franceschini, G.; D’Archi, S.; De Lauretis, F.; Scardina, L.; Di Giorgio, D.; Accetta, C.; Masetti, R. Results obtained with level II oncoplastic surgery spanning 20 years of breast cancer treatment: Do we really need further demonstration of reliability? Breast J. 2020, 26, 125–132. [Google Scholar] [CrossRef]
- Peterson, M.E.; Schultz, D.J.; Reynolds, C.; Solin, L.J. Outcomes in breast cancer patients relative to margin status after treatment with breast-conserving surgery and radiation therapy: The University of Pennsylvania experience. Int. J. Radiat. Oncol. Biol. Phys. 1999, 43, 1029–1035. [Google Scholar] [CrossRef]
- Singletary, S.E. Surgical margins in patients with early-stage breast cancer treated with breast conservation therapy. Am. J. Surg. 2002, 184, 383–393. [Google Scholar] [CrossRef]
- Corsi, F.; Sorrentino, L.; Bossi, D.; Sartani, A.; Foschi, D. preoperative localization and surgical margins in conservative breast surgery. Int. J. Surg. Oncol. 2013, 2013, 793819. [Google Scholar] [CrossRef]
- Park, C.C.; Mitsumori, M.; Nixon, A.; Recht, A.; Connolly, J.; Gelman, R.; Silver, B.; Hetelekidis, S.; Abner, A.; Harris, J.R.; et al. Outcome at 8 years after breast-conserving surgery and radiation therapy for invasive breast cancer: Influence of margin status and systemic therapy on local recurrence. J. Clin. Oncol. 2000, 18, 1668–1675. [Google Scholar] [CrossRef] [PubMed]
- Franceschini, G.; Sanchez, A.M.; Di Leone, A.; Magno, S.; Moschella, F.; Accetta, C.; Natale, M.; Di Giorgio, D.; Scaldaferri, A.; D’Archi, S.; et al. Update on the surgical management of breast cancer. Ann. Ital. Chir. 2015, 86, 89–99. [Google Scholar] [PubMed]
- Hayes, M.K. Update on preoperative breast localization. Radiol. Clin. N. Am. 2017, 55, 591–603. [Google Scholar] [CrossRef]
- Jeffries, D.O.; Dossett, L.A.; Jorns, J.M. Localization for breast surgery: The next generation. Arch. Pathol. Lab. Med. 2017, 141, 1324–1329. [Google Scholar] [CrossRef]
- Jackman, R.J.; Marzoni, F.A. Needle-localized breast biopsy: Why do we fail? Radiology 1997, 204, 677–684. [Google Scholar] [CrossRef]
- Bick, U.; Trimboli, R.M.; Athanasiou, A.; Balleyguier, C.; Baltzer, P.A.T.; Bernathova, M.; Borbély, K.; Brkljacic, B.; Carbonaro, L.A.; Clauser, P.; et al. Image-guided breast biopsy and localisation: Recommendations for information to women and referring physicians by the European Society of Breast Imaging. Insights Imaging 2020, 11, 1–18. [Google Scholar] [CrossRef]
- Riedl, C.C.; Pfarl, G.; Helbich, T.H.; Memarsadeghi, M.; Wagner, T.; Rudas, M.; Fuchsjäger, M. Comparison of wire versus carbon localization of non-palpable breast lesions. RöFo 2002, 174, 1126–1131. [Google Scholar] [CrossRef]
- Rose, A.; Collins, J.; Neerhut, P.; Bishop, C.; Mann, G.B. Carbon localisation of impalpable breast lesions. Breast 2003, 12, 264–269. [Google Scholar] [CrossRef]
- Tran, Q.; Mizumoto, R.; Tran, M.; Reintals, M.; Gounder, V. Carbon-track localisation as an adjunct to wire-guided excision of impalpable breast lesions: A retrospective cohort study. Int. J. Surg. Open 2019, 21, 7–11. [Google Scholar] [CrossRef]
- Öcal, K.; Dag, A.; Turkmenoglu, M.O.; Günay, E.C.; Yûcel, E.; Duce, M.N. Radioguided occult lesion localization versus wire-guided localization for non-palpable breast lesions: Randomized controlled trial. Clinics 2011, 66, 1003–1007. [Google Scholar] [CrossRef] [PubMed]
- De Cicco, C.; Pizzamiglio, M.; Trifirò, G.; Luini, A.; Ferrari, M.; Prisco, G.; Galimberti, V.; Cassano, E.; Viale, G.; Intra, M.; et al. Radioguided occult lesion localisation (ROLL) and surgical biopsy in breast cancer. Technical aspects. Q. J. Nucl. Med. 2002, 46, 145–151. [Google Scholar] [PubMed]
- Luini, A.; Zurrida, S.; Paganelli, G.; Galimberti, V.; Sacchini, V.; Monti, S.; Veronesi, P.; Viale, G. Comparison of radioguided excision with wire localization of occult breast lesions. BJS 1999, 86, 522–525. [Google Scholar] [CrossRef] [PubMed]
- Gray, R.J.; Salud, C.; Nguyen, K.; Dauway, E.; Friedland, J.; Berman, C.; Peltz, E.; Whitehead, G.; Cox, C.E. Randomized prospective evaluation of a novel technique for biopsy or lumpectomy of nonpalpable breast lesions: Radioactive seed versus wire localization. Ann. Surg. Oncol. 2001, 8, 711–715. [Google Scholar] [CrossRef] [PubMed]
- Rao, R.; Moldrem, A.; Sarode, V.; White, J.; Amen, M.; Rao, M.; Andrews, V.; Euhus, D.; Radford, L.; Ulissey, M. Experience with seed localization for nonpalpable breast lesions in a public health care system. Ann. Surg. Oncol. 2010, 17, 3241–3246. [Google Scholar] [CrossRef] [PubMed]
- Gera, R.; Tayeh, S.; Al-Reefy, S.; Mokbel, K. Evolving role of magseed in wireless localization of breast lesions: Systematic review and pooled analysis of 1,559 procedures. Anticancer. Res. 2020, 40, 1809–1815. [Google Scholar] [CrossRef]
- Endomag. Available online: https://www.endomag.com/ (accessed on 11 November 2020).
- Zacharioudakis, K.; Down, S.; Bholah, Z.; Lee, S.; Khan, T.; Howe, M.; Maxwell, A.; Harvey, J. Is the future magnetic? Magseed localisation of non palpable breast cancer—A multicentre comparative cohort study. Breast 2019, 44, S112. [Google Scholar] [CrossRef]
- Thekkinkattil, D.; Kaushik, M.; Hoosein, M.; Al-Attar, M.; Pilgrim, S.; Gvaramadze, A.; Hyklova, L.; Jibril, A. A prospective, single-arm, multicentre clinical evaluation of a new localisation technique using non-radioactive Magseeds for surgery of clinically occult breast lesions. Clin. Radiol. 2019, 74, 974.e7–974.e11. [Google Scholar] [CrossRef]
- Mango, V.L.; Wynn, R.T.; Feldman, S.; Friedlander, L.; Desperito, E.; Patel, S.N.; Gomberawalla, A.; Ha, R. Beyond wires and seeds: Reflector-guided breast lesion localization and excision. Radiology 2017, 284, 365–371. [Google Scholar] [CrossRef]
- Mango, V.; Ha, R.; Gomberawalla, A.; Wynn, R.; Feldman, S. Evaluation of the SAVI SCOUT surgical guidance system for localization and excision of nonpalpable breast lesions: A feasibility study. Am. J. Roentgenol. 2016, 207, W69–W72. [Google Scholar] [CrossRef]
- Cox, C.E.; Garcia-Henriquez, N.; Glancy, M.J.; Whitworth, P.; Cox, J.M.; Themar-Geck, M.; Prati, R.; Jung, M.; Russell, S.; Appleton, K.; et al. Pilot study of a new nonradioactive surgical guidance technology for locating nonpalpable breast lesions. Ann. Surg. Oncol. 2016, 23, 1824–1830. [Google Scholar] [CrossRef]
- Jadeja, P.H.; Mango, V.; Patel, S.; Friedlander, L.; Desperito, E.; Ayala-Bustamante, E.; Wynn, R.; Chen-Seetoo, M.; Taback, B.; Feldman, S.; et al. Utilization of multiple SAVI SCOUT surgical guidance system reflectors in the same breast: A single-institution feasibility study. Breast J. 2018, 24, 531–534. [Google Scholar] [CrossRef]
- Colakovic, N.; Zdravkovic, D.; Skuric, Z.; Mrda, D.; Gacic, J.; Ivanovic, N. Intraoperative ultrasound in breast cancer surgery—from localization of non-palpable tumors to objectively measurable excision. World J. Surg. Oncol. 2018, 16, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Haid, A.; Knauer, M.; Dunzinger, S.; Jasarevic, Z.; Köberle-Wührer, R.; Schuster, A.; Toeppker, M.; Haid, B.; Wenzl, E.; Offner, F. Intra-operative sonography: A valuable aid during breast-conserving surgery for occult breast cancer. Ann. Surg. Oncol. 2007, 14, 3090–3101. [Google Scholar] [CrossRef] [PubMed]
- Fortunato, L.; Penteriani, R.; Farina, M.; Vitelli, C.E.; Piro, F. Intraoperative ultrasound is an effective and preferable technique to localize non-palpable breast tumors. Eur. J. Surg. Oncol. (EJSO) 2008, 34, 1289–1292. [Google Scholar] [CrossRef]
- Ramos, M.; Díaz, J.C.; Ramos, T.; Ruano, R.; Aparicio, M.; Sancho, M.; González-Orús, J.M. Ultrasound-Guided Excision Combined with Intraoperative Assessment of Gross Macroscopic Margins Decreases the Rate of Reoperations for Non-Palpable Invasive Breast Cancer. Breast 2012, 22, 520–524. Available online: https://www.unboundmedicine.com/medline/citation/23110817/Ultrasound_guided_excision_combined_with_intraoperative_assessment_of_gross_macroscopic_margins_decreases_the_rate_of_reoperations_for_non_palpable_invasive_breast_cancer_ (accessed on 30 October 2020). [CrossRef]
- Hall, F.; Kopans, D.B.; Sadowsky, N.L.; Homer, M.J. Development of wire localization for occult breast lesions: Boston remembrances. Radiology 2013, 268, 622–627. [Google Scholar] [CrossRef]
- Homer, M.J.; Pile-Spellman, E.R. Needle localization of occult breast lesions with a curved-end retractable wire: Technique and pitfalls. Radiology 1986, 161, 547–548. [Google Scholar] [CrossRef]
- Liberman, L.; Kaplan, J.; Van Zee, K.J.; Morris, E.A.; LaTrenta, L.R.; Abramson, A.F.; Dershaw, D.D. Bracketing wires for preoperative breast needle localization. Am. J. Roentgenol. 2001, 177, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Chan, B.K.; Wiseberg-Firtell, J.A.; Jois, R.H.; Jensen, K.; Audisio, R.A. Localization techniques for guided surgical excision of non-palpable breast lesions. Cochrane Database Syst. Rev. 2015, CD009206. [Google Scholar] [CrossRef]
- Lovrics, P.J.; Cornacchi, S.; Vora, R.; Goldsmith, C.; Kahnamoui, K. Systematic review of radioguided surgery for non-palpable breast cancer. Eur. J. Surg. Oncol. (EJSO) 2011, 37, 388–397. [Google Scholar] [CrossRef]
- Loving, V.A.; Edwards, D.B.; Roche, K.T.; Steele, J.R.; Sapareto, S.A.; Byrum, S.C.; Schomer, D.F. Monte Carlo simulation to analyze the cost-benefit of radioactive seed localization versus wire localization for breast-conserving surgery in fee-for-service health care systems compared with accountable care organizations. Am. J. Roentgenol. 2014, 202, 1383–1388. [Google Scholar] [CrossRef] [PubMed]
- Van Susante, J.; Barendregt, W.; Bruggink, E. Migration of the guide-wire into the pleural cavity after needle localization of breast lesions. Eur. J. Surg. Oncol. (EJSO) 1998, 24, 446–448. [Google Scholar] [CrossRef]
- Azoury, F.M.; Sayad, P.; Rizk, A. Thoracoscopic management of a pericardial migration of a breast biopsy localization wire. Ann. Thorac. Surg. 2009, 87, 1937–1939. [Google Scholar] [CrossRef]
- Volders, J.H.; Haloua, M.H.; Krekel, N.M.A.; Meijer, S.; Van Den Tol, P.M. Current status of ultrasound-guided surgery in the treatment of breast cancer. World J. Clin. Oncol. 2016, 7, 44–53. [Google Scholar] [CrossRef]
- Bronstein, A.D.; Kilcoyne, R.F.; Moe, R.E. Complications of needle localization of foreign bodies and nonpalpable breast lesions. Arch. Surg. 1988, 123, 775–779. [Google Scholar] [CrossRef]
- Svane, G. A Stereotaxic technique for preoperative marking of non-palpable breast lesions. Acta Radiol. Diagn. 1983, 24, 145–151. [Google Scholar] [CrossRef]
- Ruiz-Delgado, M.L.; López-Ruiz, J.A.; Sáiz-López, A. Abnormal mammography and sonography associated with foreign-body giant-cell reaction after stereotactic vacuum-assisted breast biopsy with carbon marking. Acta Radiol. 2008, 49, 1112–1118. [Google Scholar] [CrossRef]
- Salvador, G.L.O.; Barbieri, P.P.; Maschke, L.; Nunes, A.L.A.; Louveira, M.H.; Budel, V.M. Charcoal granuloma mimicking breast cancer: An emerging diagnosis. Acta Radiol. Open 2018, 7, 2058460118815726. [Google Scholar] [CrossRef]
- Luini, A.; Zurrida, S.; Galimberti, V.; Paganelli, G. Radioguided surgery of occult breast lesions. Eur. J. Cancer. 1998, 34, 204–205. [Google Scholar] [CrossRef]
- Grüning, T.; Brogsitter, C.; Jones, I.W.; Heales, J.C. Resolution recovery in planar bone scans: Diagnostic value in metastatic disease. Nucl. Med. Commun. 2012, 33, 1307–1310. Available online: https://journals.lww.com/nuclearmedicinecomm/Fulltext/2012/12000/Resolution_recovery_in_planar_bone_scans__.11.aspx (accessed on 27 October 2020). [CrossRef]
- Monti, S.; Galimberti, V.; Trifirò, G.; De Cicco, C.; Peradze, N.; Brenelli, F.; Fernandez-Rodriguez, J.; Rotmensz, N.; Latronico, A.; Berrettini, A.; et al. Occult breast lesion localization plus Sentinel Node Biopsy (SNOLL): Experience with 959 patients at the European Institute of Oncology. Ann. Surg. Oncol. 2007, 14, 2928–2931. [Google Scholar] [CrossRef] [PubMed]
- Follacchio, G.A.; Monteleone, F.; Anibaldi, P.; De Vincentis, G.; Iacobelli, S.; Merola, R.; D’Orazi, V.; Monti, M.; Pasta, V. A modified sentinel node and occult lesion localization (SNOLL) technique in non-palpable breast cancer: A pilot study. J. Exp. Clin. Cancer Res. 2015, 34, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Pavlicek, W.; Walton, H.A.; Karstaedt, P.J.; Gray, R.J. Radiation safety with use of I-125 seeds for localization of nonpalpable breast lesions. Acad. Radiol. 2006, 13, 909–915. [Google Scholar] [CrossRef]
- Goudreau, S.H.; Joseph, J.P.; Seiler, S.J. Preoperative radioactive seed localization for nonpalpable breast lesions: Technique, pitfalls, and solutions. Radiographics 2015, 35, 1319–1334. [Google Scholar] [CrossRef]
- Jakub, J.W.; Gray, R.J.; Degnim, A.C.; Boughey, J.C.; Gardner, M.; Cox, C.E. Current status of radioactive seed for localization of non palpable breast lesions. Am. J. Surg. 2010, 199, 522–528. [Google Scholar] [CrossRef]
- Sharek, D.; Zuley, M.L.; Zhang, J.Y.; Soran, A.; Ahrendt, G.M.; Ganott, M.A. Radioactive seed localization versus wire localization for lumpectomies: A comparison of outcomes. Am. J. Roentgenol. 2015, 204, 872–877. [Google Scholar] [CrossRef]
- Bloomquist, E.V.; Ajkay, N.; Patil, S.; Collett, A.E.; Frazier, T.G.; Barrio, A.V. A randomized prospective comparison of patient-assessed satisfaction and clinical outcomes with radioactive seed localization versus wire localization. Breast J. 2016, 22, 151–157. [Google Scholar] [CrossRef]
- Langhans, L.; Tvedskov, T.F.; Klausen, T.L.; Jensen, M.-B.; Talman, M.-L.; Vejborg, I.; Benian, C.; Roslind, A.; Hermansen, J.; Oturai, P.S.; et al. Radioactive seed localization or wire-guided localization of nonpalpable invasive and in situ breast cancer: A randomized, multicenter, open-label trial. Ann. Surg. 2017, 266, 29–35. [Google Scholar] [CrossRef]
- Harvey, J.R.; Lim, Y.; Murphy, J.; Howe, M.; Morris, J.; Goyal, A.; Maxwell, A.J. Safety and feasibility of breast lesion localization using magnetic seeds (Magseed): A multi-centre, open-label cohort study. Breast Cancer Res. Treat. 2018, 169, 531–536. [Google Scholar] [CrossRef]
- Haloua, M.H.; Volders, J.H.; Krekel, N.M.; Lopes Cardozo, A.M.F.; De Roos, W.K.; De Widt-Levert, L.M.; Van Der Veen, H.; Rijna, H.; Bergers, E.; Jóźwiak, K.; et al. Intraoperative ultrasound guidance in breast-conserving surgery improves cosmetic outcomes and patient satisfaction: Results of a Multicenter Randomized Controlled Trial (COBALT). Ann. Surg. Oncol. 2016, 23, 30–37. [Google Scholar] [CrossRef]
- James, T.A.; Harlow, S.; Sheehey-Jones, J.; Hart, M.; Gaspari, C.; Stanley, M.; Krag, D.; Ashikaga, T.; McCahill, L.E. Intraoperative ultrasound versus mammographic needle localization for ductal carcinoma in situ. Ann. Surg. Oncol. 2009, 16, 1164–1169. [Google Scholar] [CrossRef]
- Gerrard, A.D.; Shrotri, A. Surgeon-led intraoperative ultrasound localization for nonpalpable breast cancers: Results of 5 years of practice. Clin. Breast Cancer 2019, 19, e748–e752. [Google Scholar] [CrossRef] [PubMed]
- Krekel, N.M.; Cardozo, A.L.F.; Muller, S.; Bergers, E.; Meijer, S.; van den Tol, M. Optimising surgical accuracy in palpable breast cancer with intra-operative breast ultrasound—Feasibility and surgeons’ learning curve. Eur. J. Surg. Oncol. (EJSO) 2011, 37, 1044–1050. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Dogan, B.E.; Whitman, G.J. Intraoperative breast ultrasound. Semin. Roentgenol. 2011, 46, 280–284. [Google Scholar] [CrossRef]
- Carlino, G.; Rinaldi, P.; Giuliani, M.; Rella, R.; Bufi, E.; Padovano, F.; Ciardi, C.; Romani, M.; Belli, P.; Manfredi, R. Ultrasound-guided preoperative localization of breast lesions: A good choice. J. Ultrasound 2019, 22, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Franceschini, G.; Visconti, G.; Sanchez, A.M.; Di Leone, A.; Salgarello, M.; Masetti, R. Oxidized regenerated cellulose in breast surgery: Experimental model. J. Surg. Res. 2015, 198, 237–244. [Google Scholar] [CrossRef]
- Madeley, C.; Kessell, M.; Madeley, C.; Taylor, D.B. A comparison of stereotactic and tomosynthesis-guided localisation of impalpable breast lesions. J. Med. Radiat. Sci. 2019, 66, 170–176. [Google Scholar] [CrossRef]
- Fusco, R.; Petrillo, A.; Catalano, O.; Sansone, M.; Granata, V.; Filice, S.; D’Aiuto, M.; Pankhurst, Q.; Douek, M. Procedures for location of non-palpable breast lesions: A systematic review for the radiologist. Breast Cancer 2012, 21, 522–531. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Technique | Materials/Procedures | Advantages | Disadvantages | Success * Rate | Clear Margins Rate |
|---|---|---|---|---|---|
| Wire localization | Wire Preloaded needle introducer | Simple Cost-effective Different kinds of image-guidance | Wire migration Scheduling difficulties Limits surgical decisions | 97.5% [14] | 70.8–87.4% [15] |
| Carbon marking | Diluted charcoal powder | Simple Different kinds of image-guidance Cost-effective Cannot dislodge Scheduling flexibility | Carbon can distort or obscure lesion Unfit for large breasts Unfit for multifocal or extensive lesions | 99% [16] | 61–85% [17,18] |
| ROLL | Nuclear radiotracer Technetium 99 Gamma ray probe | Different kinds of image-guidance Does not limit surgeon | Scheduling difficulties Radiation Cost | 95–99% [19] | 92% [20,21] |
| RSL | Iodine 125 seed Preloaded needle introducer Gamma probe set for I-125 | Scheduling flexibility Does not limit surgeon Different kinds of image-guidance | Radiation Not repositionable after deployment | 100% [22,23] | 73.5–96.7% [22,23] |
| Magseed | Paramagnetic seed Preloaded needle introducer | Scheduling flexibility No radiation Does not limit surgeon | Cost Not repositionable after deployment Non magnetizable surgical equipment MRI artifacts | 99.86% [24,25,26,27] | 88.75% [24] |
| Radiofrequency identification tags | Radiofrequency reflector Needle introducer Detector | Scheduling flexibility No radiation Does not limit surgeon | Cost Depth limit Not repositionable after deployment Interference with halogen lights in the OR | 97–100% [28,29] | 85–100% [28,29,30] |
| IOUS | Portable or OR-stationed US machine and sterile transducer cover | Scheduling flexibility No radiation Does not limit surgeon Non-invasive | Unemployable in US-invisible lesions Surgeon learning curve Interference with air during dissection | 100% [31,32,33,34,35] | 81–97% [32,34] |
| Skin tattoo | Dermographic marker Lead markers | Simple and safe Cost-effective Non-invasive Different kinds of image-guidance Does not limit surgeon | Scheduling difficulties Inability to depict marker | 99.5% ** | 95.9% ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franceschini, G.; Mason, E.J.; Grippo, C.; D’Archi, S.; D’Angelo, A.; Scardina, L.; Sanchez, A.M.; Conti, M.; Trombadori, C.; Terribile, D.A.; et al. Image-Guided Localization Techniques for Surgical Excision of Non-Palpable Breast Lesions: An Overview of Current Literature and Our Experience with Preoperative Skin Tattoo. J. Pers. Med. 2021, 11, 99. https://doi.org/10.3390/jpm11020099
Franceschini G, Mason EJ, Grippo C, D’Archi S, D’Angelo A, Scardina L, Sanchez AM, Conti M, Trombadori C, Terribile DA, et al. Image-Guided Localization Techniques for Surgical Excision of Non-Palpable Breast Lesions: An Overview of Current Literature and Our Experience with Preoperative Skin Tattoo. Journal of Personalized Medicine. 2021; 11(2):99. https://doi.org/10.3390/jpm11020099
Chicago/Turabian StyleFranceschini, Gianluca, Elena Jane Mason, Cristina Grippo, Sabatino D’Archi, Anna D’Angelo, Lorenzo Scardina, Alejandro Martin Sanchez, Marco Conti, Charlotte Trombadori, Daniela Andreina Terribile, and et al. 2021. "Image-Guided Localization Techniques for Surgical Excision of Non-Palpable Breast Lesions: An Overview of Current Literature and Our Experience with Preoperative Skin Tattoo" Journal of Personalized Medicine 11, no. 2: 99. https://doi.org/10.3390/jpm11020099
APA StyleFranceschini, G., Mason, E. J., Grippo, C., D’Archi, S., D’Angelo, A., Scardina, L., Sanchez, A. M., Conti, M., Trombadori, C., Terribile, D. A., Di Leone, A., Carnassale, B., Belli, P., Manfredi, R., & Masetti, R. (2021). Image-Guided Localization Techniques for Surgical Excision of Non-Palpable Breast Lesions: An Overview of Current Literature and Our Experience with Preoperative Skin Tattoo. Journal of Personalized Medicine, 11(2), 99. https://doi.org/10.3390/jpm11020099