
Prognostic Relevance of Thyroid-Hormone-Associated Proteins in Adenoid Cystic Carcinoma of the Head and Neck

 , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Study Design
2.2. Tissue Microarray and Immunohistochemistry
2.3. Statistical Analysis
3. Results
3.1. Analysis at Baseline
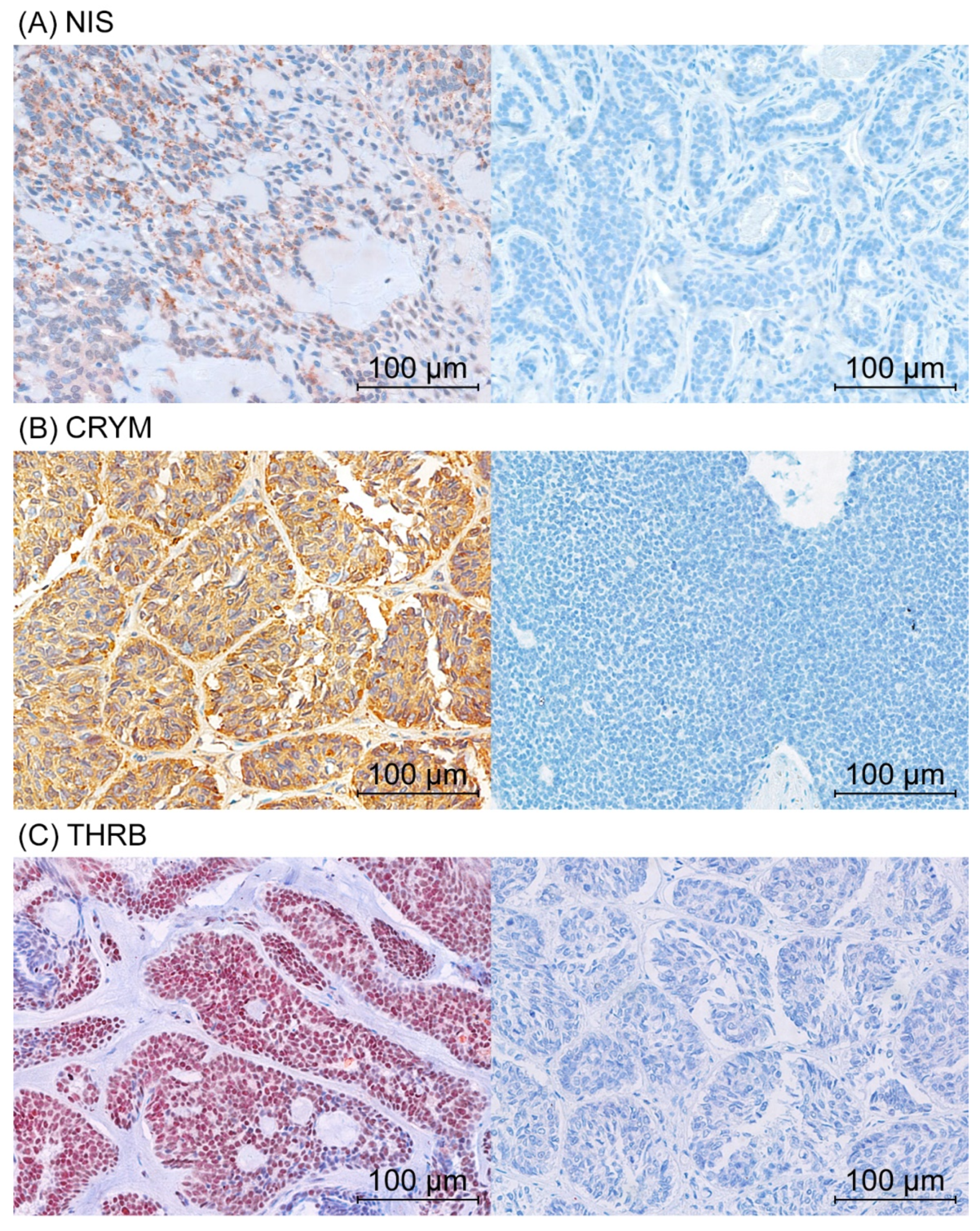
3.2. Protein Levels of CRYM, THRB, and NIS and Correlation with Clinicopathological Features
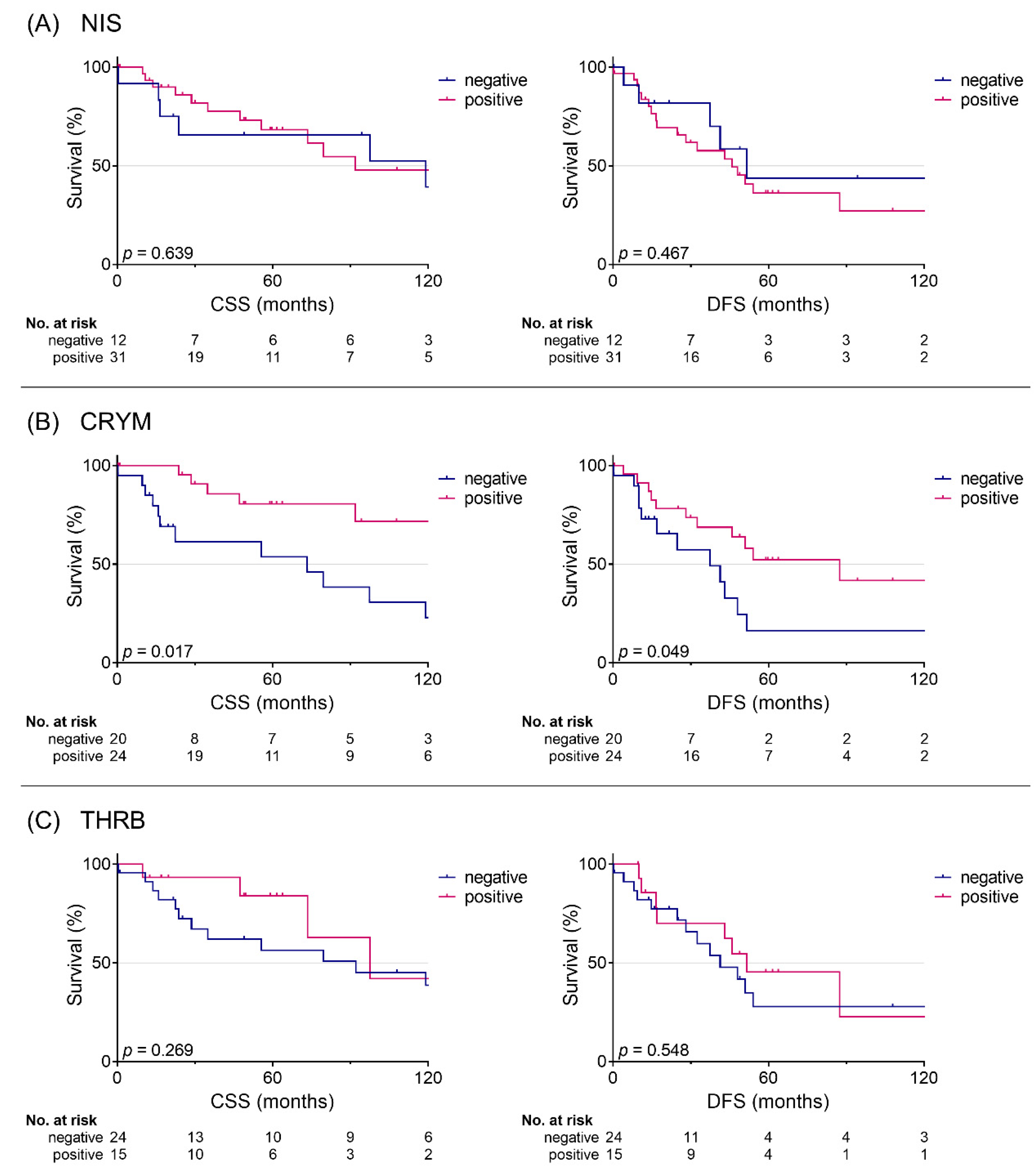
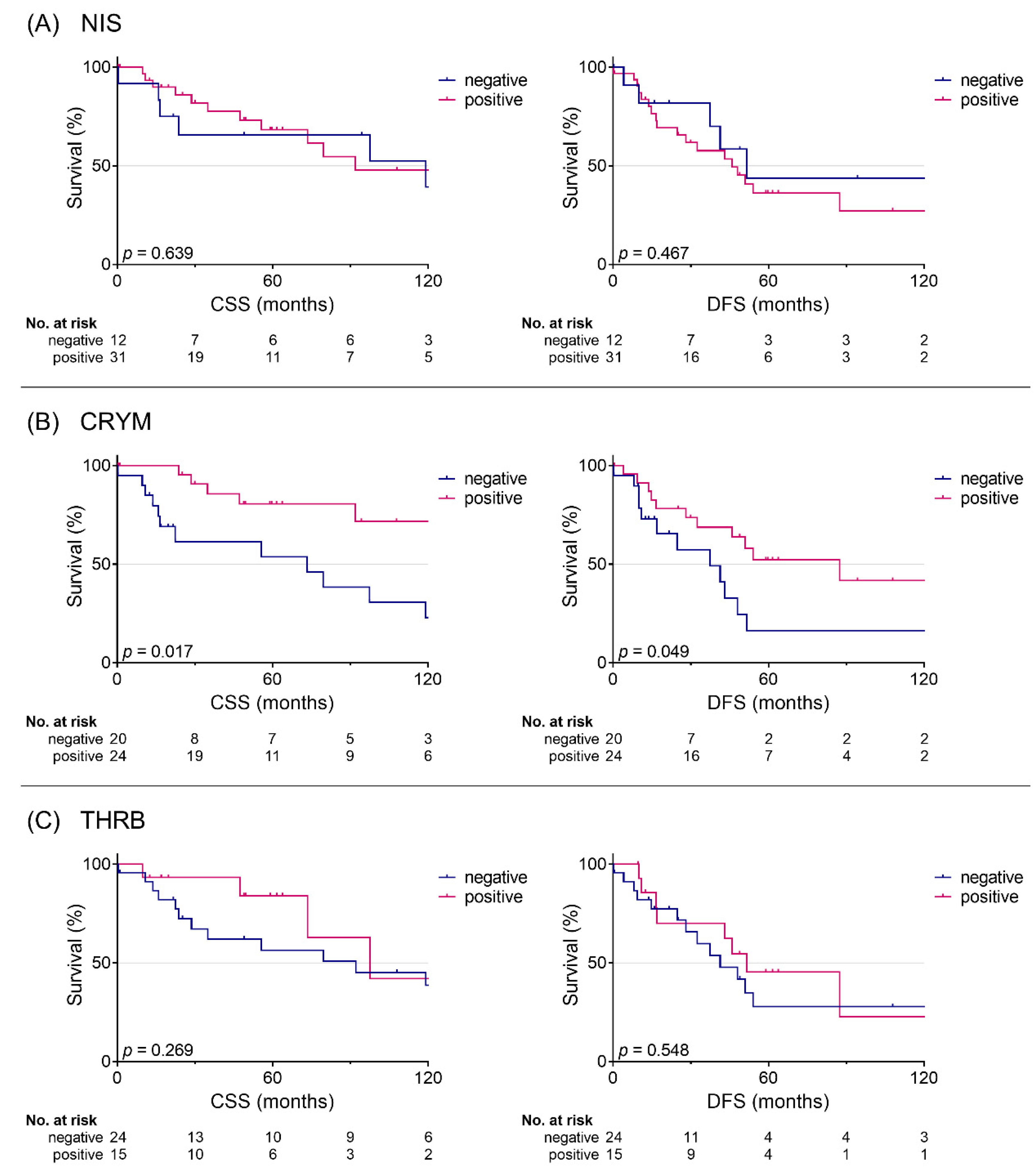
3.3. Analysis of Cause-Specific Survival and Disease-Free Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coca-Pelaz, A.; Rodrigo, J.P.; Bradley, P.J.; Vander Poorten, V.; Triantafyllou, A.; Hunt, J.L.; Strojan, P.; Rinaldo, A.; Haigentz, M.; Takes, R.P.; et al. Adenoid cystic carcinoma of the head and neck—An update. Oral Oncol. 2015, 51, 652–661. [Google Scholar] [CrossRef] [PubMed]
- Bradley, P.J. Adenoid cystic carcinoma evaluation and management: Progress with optimism! Curr. Opin. Otolaryngol. Head Neck Surg. 2017, 25, 147–153. [Google Scholar] [CrossRef]
- Lloyd, S.; Yu, J.B.; Wilson, L.D.; Decker, R.H. Determinants and patterns of survival in adenoid cystic carcinoma of the head and neck, including an analysis of adjuvant radiation therapy. Am. J. Clin. Oncol. Cancer Clin. Trials 2011, 34, 76–81. [Google Scholar] [CrossRef]
- Liu, Y.-C.; Yeh, C.-T.; Lin, K.-H. Molecular Functions of Thyroid Hormone Signaling in Regulation of Cancer Progression and Anti-Apoptosis. Int. J. Mol. Sci. 2019, 20, 4986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De la Vieja, A.; Santisteban, P. Role of iodide metabolism in physiology and cancer. Endocr. Relat. Cancer 2018, 25, R225–R245. [Google Scholar] [CrossRef] [PubMed]
- Albano, D.; Bertagna, F.; Panarotto, M.B.; Giubbini, R. Early and late adverse effects of radioiodine for pediatric differentiated thyroid cancer. Pediatr. Blood Cancer 2017, 64, e26595. [Google Scholar] [CrossRef] [Green Version]
- La Perle, K.M.D.; Kim, D.C.; Hall, N.C.; Bobbey, A.; Shen, D.H.; Nagy, R.S.; Wakely, P.E.; Lehman, A.; Jarjoura, D.; Jhiang, S.M. Modulation of Sodium/Iodide Symporter Expression in the Salivary Gland. Thyroid 2013, 23, 1029–1036. [Google Scholar] [CrossRef]
- Gainor, D.L.; Chute, D.J.; Lorenz, R.R. Sodium Iodide Symporter Expression in Adenoid Cystic Carcinoma of the Head and Neck. JAMA Otolaryngol. Neck Surg. 2015, 141, 739. [Google Scholar] [CrossRef] [Green Version]
- Mishra, A.; Shrivastava, A. Prognostic significance of sodium iodide symporter and deiodinase enzymes mRNA expression in gastric cancer. Int. J. Appl. Basic Med. Res. 2020, 10, 43. [Google Scholar] [CrossRef]
- Shiozaki, A.; Ariyoshi, Y.; Iitaka, D.; Kosuga, T.; Shimizu, H.; Kudou, M.; Konishi, T.; Shoda, K.; Arita, T.; Konishi, H.; et al. Functional analysis and clinical significance of sodium iodide symporter expression in gastric cancer. Gastric Cancer 2019, 22, 473–485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riesco-Eizaguirre, G.; Leoni, S.G.; Mendiola, M.; Estevez-Cebrero, M.A.; Gallego, M.I.; Redondo, A.; Hardisson, D.; Santisteban, P.; De la Vieja, A. NIS Mediates Iodide Uptake in the Female Reproductive Tract and Is a Poor Prognostic Factor in Ovarian Cancer. J. Clin. Endocrinol. Metab. 2014, 99, E1199–E1208. [Google Scholar] [CrossRef] [Green Version]
- Kogai, T.; Taki, K.; Brent, G.A. Enhancement of sodium/iodide symporter expression in thyroid and breast cancer. Endocr. Relat. Cancer 2006, 13, 797–826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borel, F.; Hachi, I.; Palencia, A.; Gaillard, M.-C.; Ferrer, J.-L. Crystal structure of mouse mu-crystallin complexed with NADPH and the T3 thyroid hormone. FEBS J. 2014, 281, 1598–1612. [Google Scholar] [CrossRef] [PubMed]
- Aksoy, O.; Pencik, J.; Hartenbach, M.; Moazzami, A.A.; Schlederer, M.; Balber, T.; Varady, A.; Philippe, C.; Baltzer, P.A.; Mazumder, B.; et al. Thyroid and androgen receptor signaling are antagonized by μ-Crystallin in prostate cancer. Int. J. Cancer 2021, 148, 731–747. [Google Scholar] [CrossRef] [PubMed]
- Park, J.W.; Zhao, L.; Cheng, S. Inhibition of estrogen-dependent tumorigenesis by the thyroid hormone receptor β in xenograft models. Am. J. Cancer Res. 2013, 3, 302–311. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Iglesias, O.; Garcia-Silva, S.; Tenbaum, S.P.; Regadera, J.; Larcher, F.; Paramio, J.M.; Vennström, B.; Aranda, A. Thyroid Hormone Receptor β1 Acts as a Potent Suppressor of Tumor Invasiveness and Metastasis. Cancer Res. 2009, 69, 501–509. [Google Scholar] [CrossRef] [Green Version]
- Aranda, A.; Martínez-Iglesias, O.; Ruiz-Llorente, L.; García-Carpizo, V.; Zambrano, A. Thyroid receptor: Roles in cancer. Trends Endocrinol. Metab. 2009, 20, 318–324. [Google Scholar] [CrossRef]
- Heublein, S.; Mayr, D.; Meindl, A.; Angele, M.; Gallwas, J.; Jeschke, U.; Ditsch, N. Thyroid Hormone Receptors Predict Prognosis in BRCA1 Associated Breast Cancer in Opposing Ways. PLoS ONE 2015, 10, e0127072. [Google Scholar] [CrossRef]
- Jerzak, K.J.; Cockburn, J.G.; Dhesy-Thind, S.K.; Pond, G.R.; Pritchard, K.I.; Nofech-Mozes, S.; Sun, P.; Narod, S.A.; Bane, A. Thyroid hormone receptor beta-1 expression in early breast cancer: A validation study. Breast Cancer Res. Treat. 2018, 171, 709–717. [Google Scholar] [CrossRef] [PubMed]
- Schnoell, J.; Kadletz, L.; Jank, B.J.; Oberndorfer, F.; Brkic, F.F.; Gurnhofer, E.; Cede, J.; Seemann, R.; Kenner, L.; Heiduschka, G. Expression of inhibitors of apoptosis proteins in salivary gland adenoid cystic carcinoma: XIAP is an independent marker of impaired cause-specific survival. Clin. Otolaryngol. 2020, 45, 364–369. [Google Scholar] [CrossRef]
- Schemper, M.; Smith, T.L. A note on quantifying follow-up in studies of failure time. Control. Clin. Trials 1996, 17, 343–346. [Google Scholar] [CrossRef]
- Heinze, G.; Wallisch, C.; Dunkler, D. Variable selection—A review and recommendations for the practicing statistician. Biom. J. 2018, 60, 431–449. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Micali, S.; Bulotta, S.; Puppin, C.; Territo, A.; Navarra, M.; Bianchi, G.; Damante, G.; Filetti, S.; Russo, D. Sodium iodide symporter (NIS) in extrathyroidal malignancies: Focus on breast and urological cancer. BMC Cancer 2014, 14, 303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravera, S.; Reyna-Neyra, A.; Ferrandino, G.; Amzel, L.M.; Carrasco, N. The Sodium/Iodide Symporter (NIS): Molecular Physiology and Preclinical and Clinical Applications. Annu. Rev. Physiol. 2017, 79, 261–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
| Number of Patients | Percentage (%) | |
|---|---|---|
| Sex | ||
| Female | 26 | 59% |
| Male | 18 | 41% |
| T Stage | ||
| 1 | 6 | 14% |
| 2 | 6 | 14% |
| 3 | 8 | 18% |
| 4 | 24 | 55% |
| N Stage | ||
| 0 | 34 | 77% |
| 1 | 4 | 9% |
| 2 | 6 | 14% |
| M Stage | ||
| 0 | 41 | 93% |
| 1 | 3 | 7% |
| Stage | ||
| I | 5 | 11% |
| II | 7 | 15% |
| III | 4 | 9% |
| IV | 27 | 59% |
| x | 3 | 7% |
| Grading-Spiro | ||
| 1 | 29 | 66% |
| 2 | 13 | 30% |
| 3 | 2 | 5% |
| Grading-Perzin/Szanto | ||
| 1 | 10 | 23% |
| 2 | 25 | 57% |
| 3 | 9 | 20% |
| Localization | ||
| Minor | 15 | 34% |
| Major | 29 | 66% |
| Perineural Invasion | ||
| Yes | 23 | 52% |
| No | 21 | 48% |
| Lymphovascular Invasion | ||
| Yes | 38 | 86% |
| No | 6 | 14% |
| Univariable | |||
|---|---|---|---|
| HR | 95% CI | p-Value | |
| CSS | |||
| NIS | 0.08 | 0.31–2.06 | 0.645 |
| CRYM | 0.34 | 0.13–0.86 | 0.023 |
| THRB | 0.54 | 0.17–1.65 | 0.276 |
| DFS | |||
| NIS | 1.37 | 0.51–3.75 | 0.530 |
| CRYM | 0.44 | 0.19–1.02 | 0.054 |
| THRB | 0.76 | 0.32–1.85 | 0.549 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schnoell, J.; Kotowski, U.; Jank, B.J.; Stoiber, S.; Gurnhofer, E.; Schlederer, M.; Heiduschka, G.; Kenner, L.; Kadletz-Wanke, L. Prognostic Relevance of Thyroid-Hormone-Associated Proteins in Adenoid Cystic Carcinoma of the Head and Neck. J. Pers. Med. 2021, 11, 1352. https://doi.org/10.3390/jpm11121352
Schnoell J, Kotowski U, Jank BJ, Stoiber S, Gurnhofer E, Schlederer M, Heiduschka G, Kenner L, Kadletz-Wanke L. Prognostic Relevance of Thyroid-Hormone-Associated Proteins in Adenoid Cystic Carcinoma of the Head and Neck. Journal of Personalized Medicine. 2021; 11(12):1352. https://doi.org/10.3390/jpm11121352
Chicago/Turabian StyleSchnoell, Julia, Ulana Kotowski, Bernhard J. Jank, Stefan Stoiber, Elisabeth Gurnhofer, Michaela Schlederer, Gregor Heiduschka, Lukas Kenner, and Lorenz Kadletz-Wanke. 2021. "Prognostic Relevance of Thyroid-Hormone-Associated Proteins in Adenoid Cystic Carcinoma of the Head and Neck" Journal of Personalized Medicine 11, no. 12: 1352. https://doi.org/10.3390/jpm11121352
APA StyleSchnoell, J., Kotowski, U., Jank, B. J., Stoiber, S., Gurnhofer, E., Schlederer, M., Heiduschka, G., Kenner, L., & Kadletz-Wanke, L. (2021). Prognostic Relevance of Thyroid-Hormone-Associated Proteins in Adenoid Cystic Carcinoma of the Head and Neck. Journal of Personalized Medicine, 11(12), 1352. https://doi.org/10.3390/jpm11121352