
The Prevalence of β-Thalassemia and Other Hemoglobinopathies in Kuwaiti Premarital Screening Program: An 11-Year Experience

 ,
,
Abstract
:1. Introduction
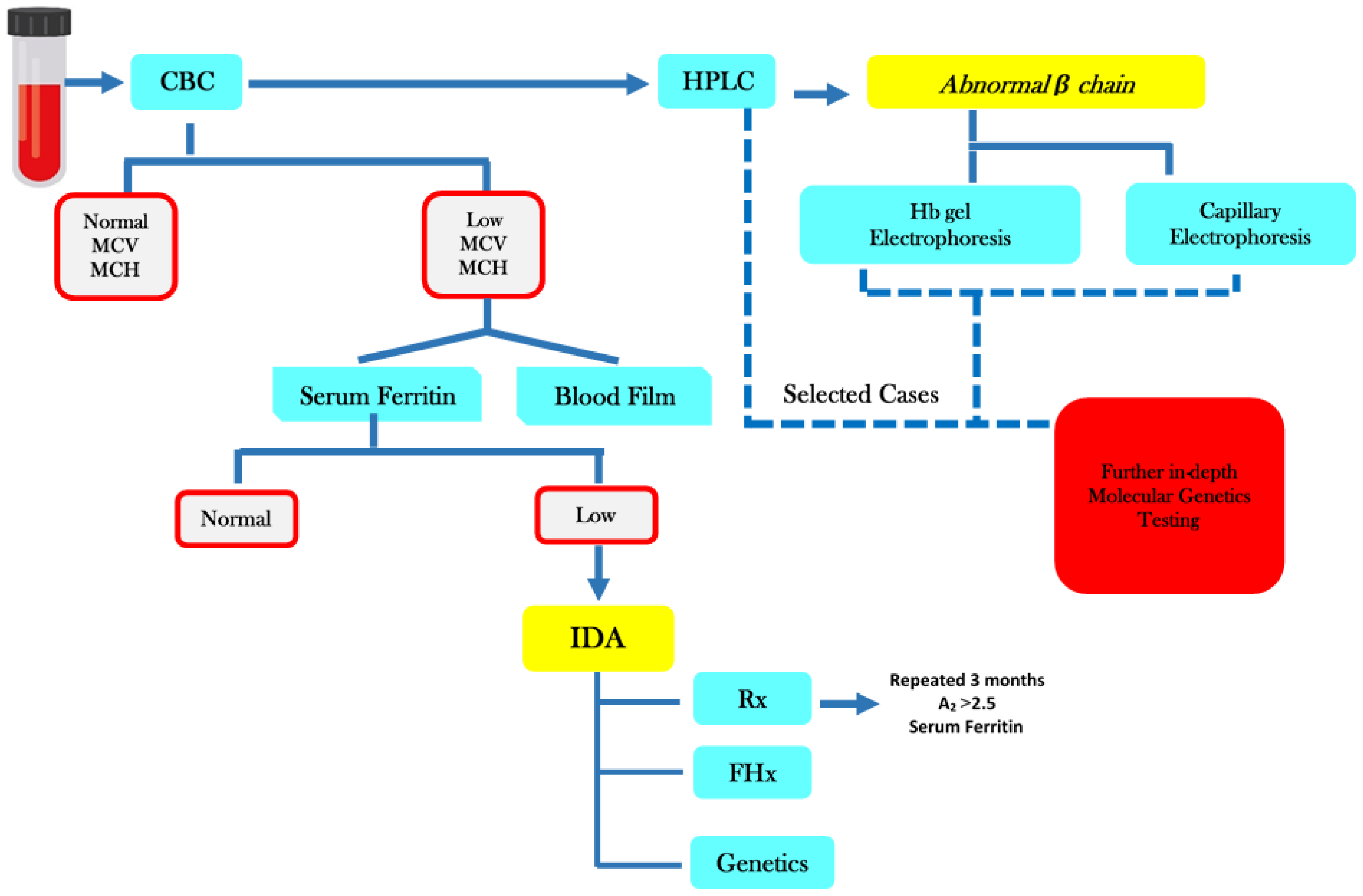
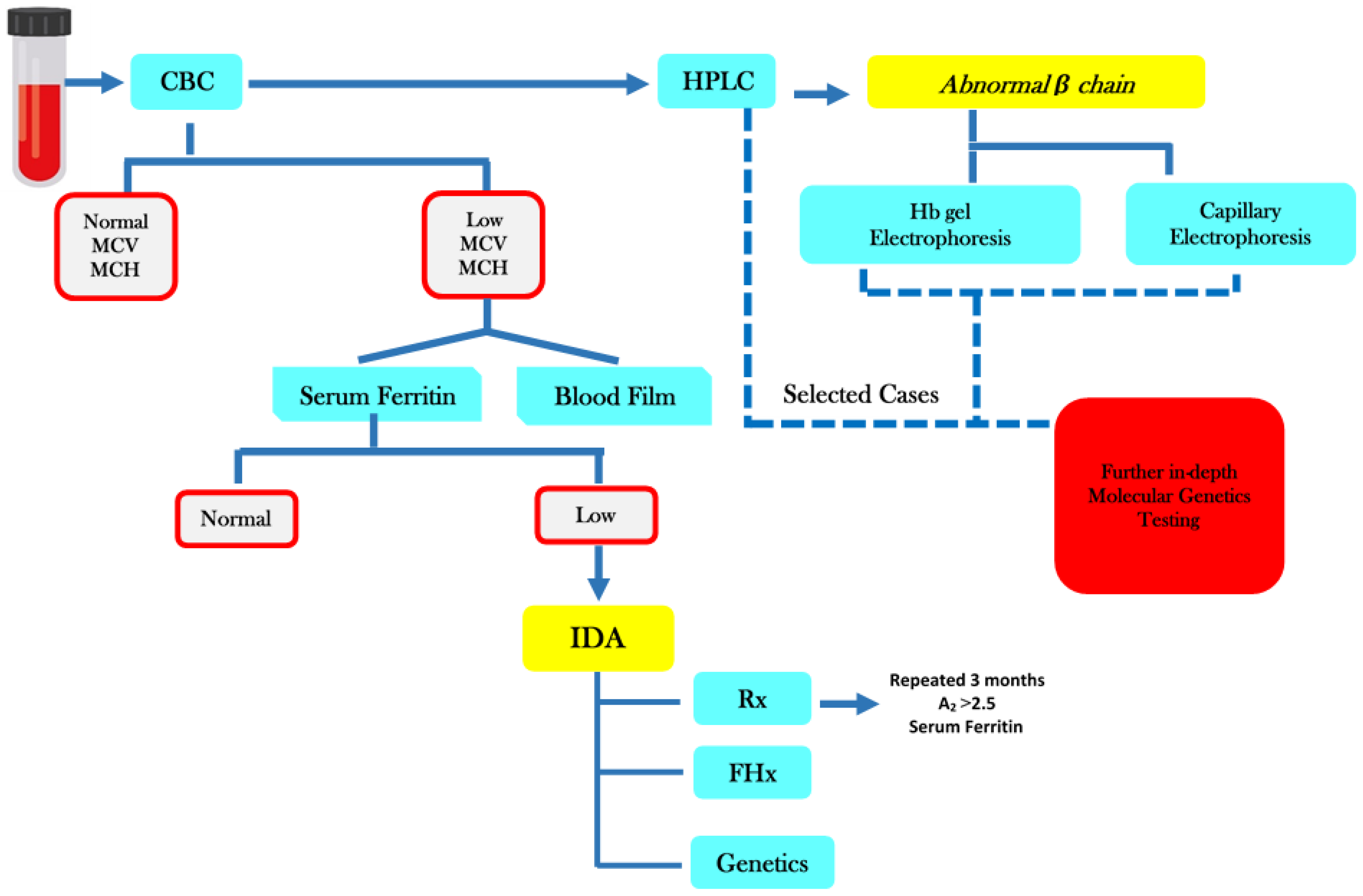
2. Materials and Methods
2.1. Premarital Screening Program
2.2. Ethical Consideration
2.3. Data Management and Statistical Analysis
3. Results
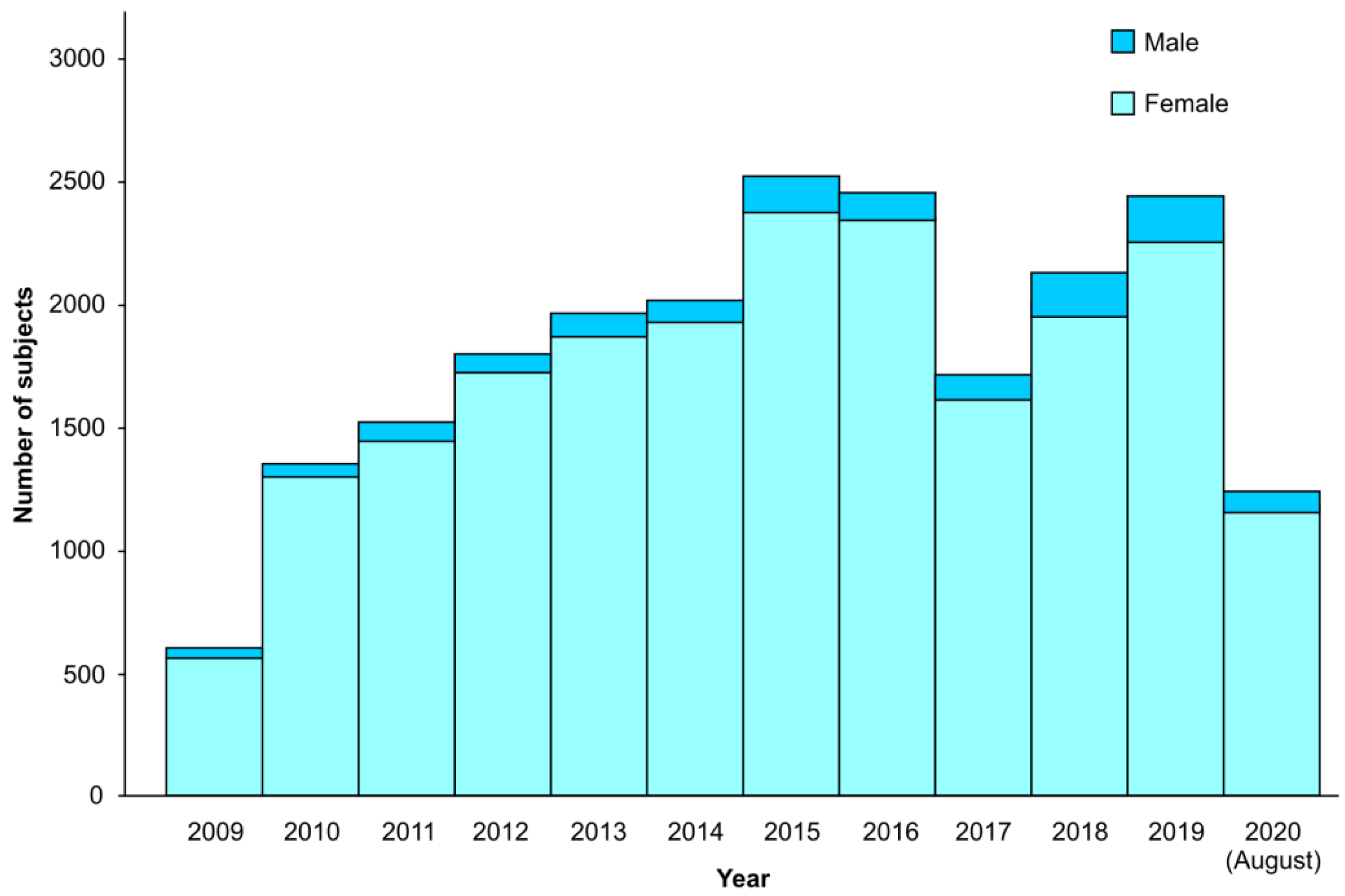
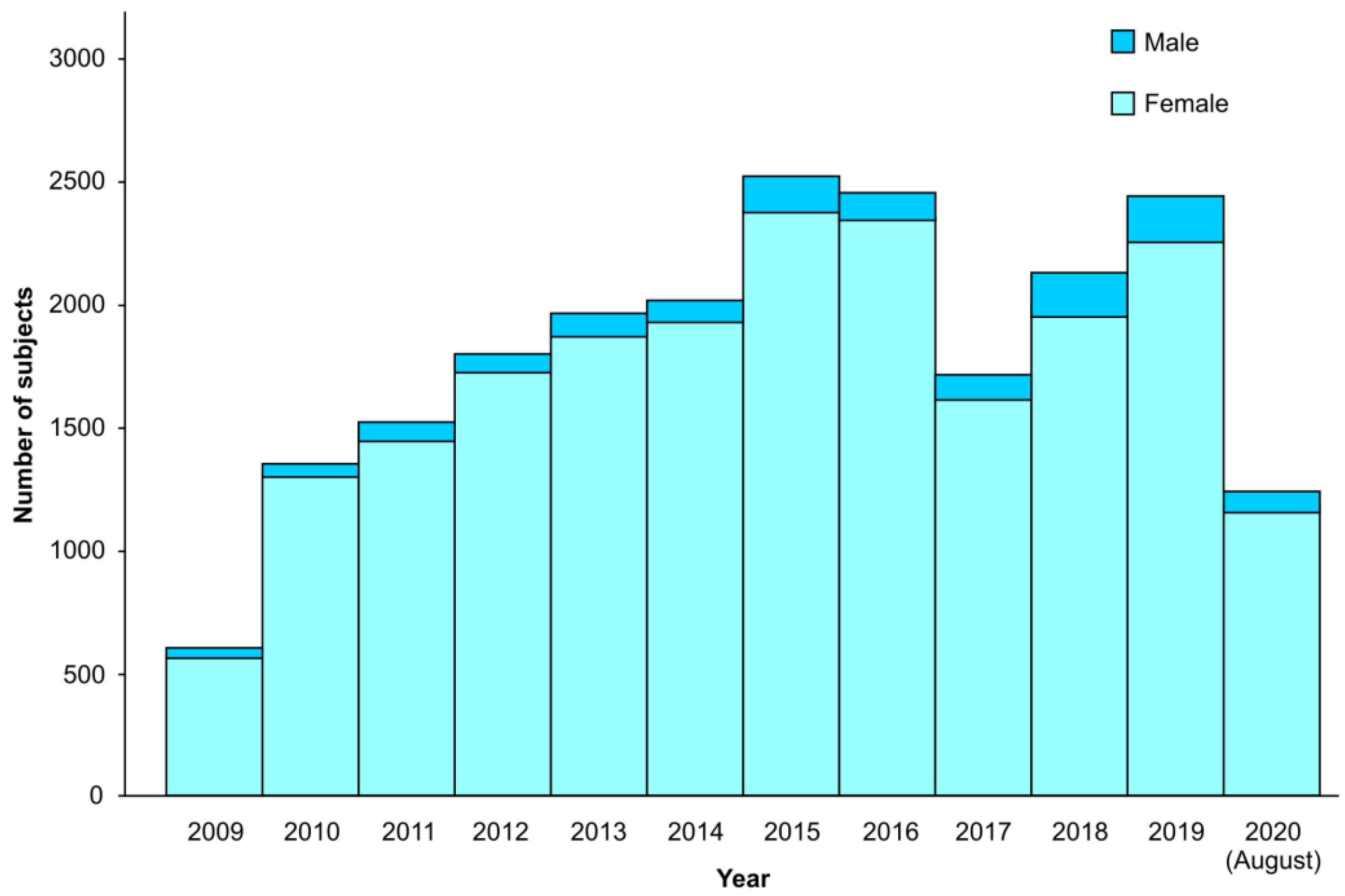
3.1. Population Characteristics
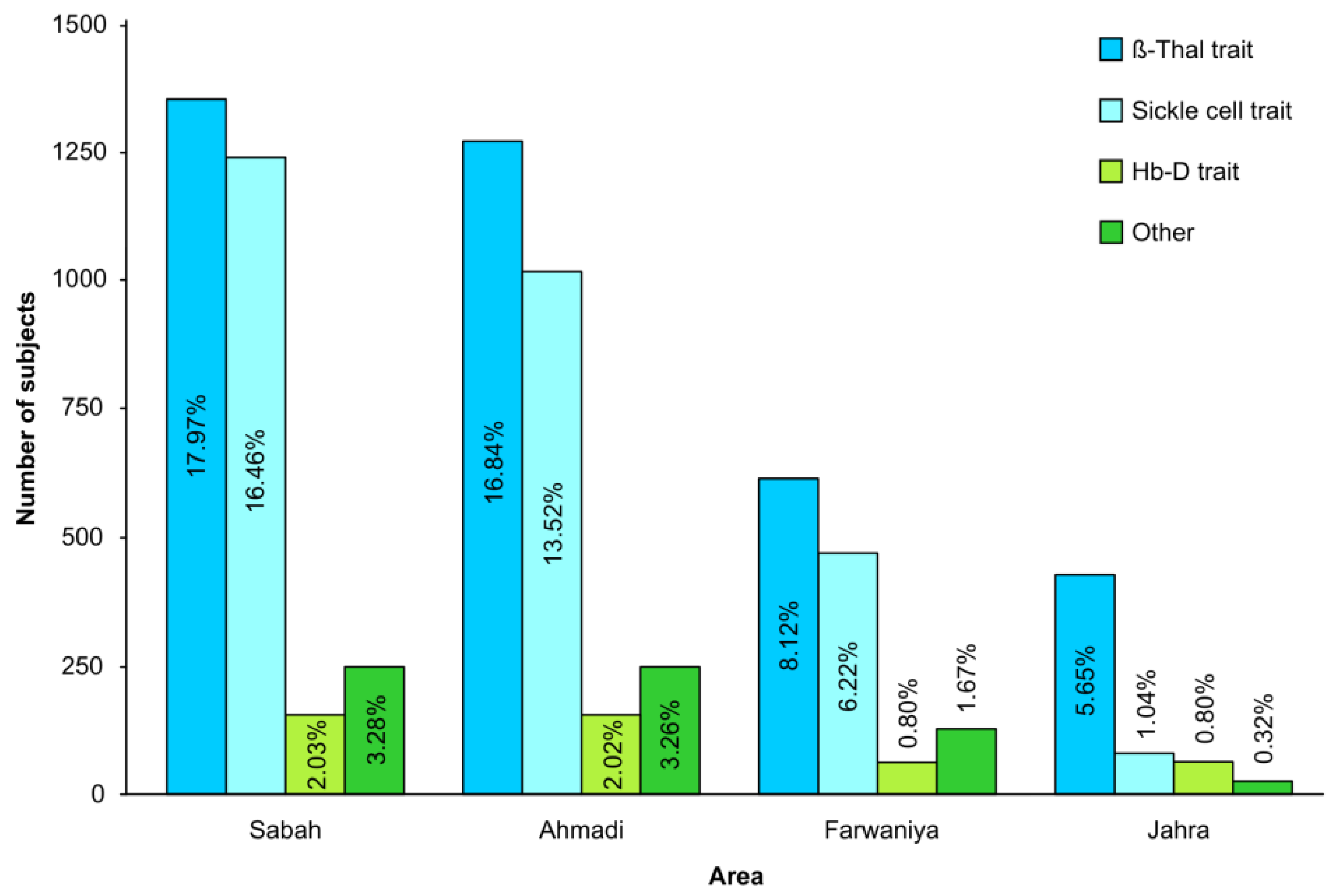
3.2. Prevalence Rate, Time Trends and Distribution of β-Thalassemia and Sickle Cell Hemoglobinopathies
3.3. Other Hemoglobin Abnormalities, Borderline HbA2 and Iron Deficiency Anemia Cases
3.4. Prevalence of Safe and Unsafe Marriage
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Tsamesidis, I.; Fozza, C.; Vagdatli, E.; Kalpaka, A.; Cirotto, C.; Pau, M.C.; Pantaleo, A.; Turrini, F.; Grigoriou, E.; Lymperaki, E. Total antioxidant capacity in Mediterranean β -thalassemic patients. Adv. Clin. Exp. Med. 2017, 26, 789–793. [Google Scholar] [CrossRef] [Green Version]
- Al-Sulaiman, A.; Suliman, A.; Al-Mishari, M.; Al-Sawadi, A.; Owaidah, T.M. Knowledge and attitude toward the hemoglobinopathies premarital screening program in Saudi Arabia: Population-based survey. Hemoglobin 2008, 32, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Alhamdan, N.A.; Almazrou, Y.Y.; Alswaidi, F.M.; Choudhry, A.J. Premarital screening for thalassemia and sickle cell disease in Saudi Arabia. Genet. Med. 2007, 9, 372–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weatherall, D.J.; Clegg, J.B. Inherited haemoglobin disorders: An increasing global health problem. Bull. World Health Organ. 2001, 79, 704–712. [Google Scholar] [PubMed]
- Cao, A.; Rosatelli, M.C.; Monni, G.; Galanello, R. Screening for thalassemia: A model of success. Obstet. Gynecol. Clin. N. Am. 2002, 29, 305–328. [Google Scholar] [CrossRef]
- Al-Gazali, L.; Hamamy, H.; Al-Arrayad, S. Genetic disorders in the Arab world. BMJ 2006, 333, 831–834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saffi, M.; Howard, N. Exploring the effectiveness of mandatory premarital screening and genetic counselling programmes for beta-thalassaemia in the Middle East: A scoping review. Public Health Genom. 2015, 18, 193–203. [Google Scholar] [CrossRef]
- Al-Hosani, H.; Salah, M.; Osman, H.M.; Farag, H.M.; Anvery, S.M. Incidence of haemoglobinopathies detected through neonatal screening in the United Arab Emirates. EMHJ 2005, 11, 300–307. [Google Scholar]
- Al-Riyami, A.; Ebrahim, G.J. Genetic blood disorders survey in the sultanate of Oman. J. Trop. Pediatr. 2003, 49, 1–20. [Google Scholar]
- Bozkurt, G. Results from the north Cyprus thalassemia prevention program. Hemoglobin 2007, 31, 257–264. [Google Scholar] [CrossRef]
- Loukopoulos, D. Haemoglobinopathies in Greece: Prevention programme over the past 35 years. Indian J. Med. Res. 2011, 134, 572–576. [Google Scholar]
- Belhoul, K.M.; Abdulrahman, M.; Alraei, R.F. Hemoglobinopathy carrier prevalence in the United Arab Emirates: First analysis of the Dubai Health Authority premarital screening program results. Hemoglobin 2013, 37, 359–368. [Google Scholar] [CrossRef] [PubMed]
- El-Hazmi, M.A. The natural history and the national pre-marital screening program in Saudi Arabia. Saudi Med. J. 2004, 25, 1549–1554. [Google Scholar] [PubMed]
- Al-Kindi, R.; Al-Rujaibi, S.; Al-Kendi, M. Knowledge and attitude of university students towards premarital screening program. Oman Med. J. 2012, 27, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, N.K.; Al-Bar, H.; Al-Fakeeh, A.; Al-Ahmadi, J.; Qadi, M.; Al-Bar, A.; Milaat, W. An educational program about premarital screening for unmarried female students in King Abdul-Aziz University, Jeddah. J. Infect. Public Health 2011, 4, 30–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitchell, J.J.; Capua, A.; Clow, C.; Scriver, R.C. Twenty year outcome analysis of genetic screening programs for Tay-Sachs and B-thalassemia disease carriers in high schools. Am. J. Hum. Genet. 1996, 59, 793–798. [Google Scholar]
- Tadmouri, G.O.; Nair, P.; Obeid, T.; Al-Ali, M.T.; Al-Khaja, N.; Hamamy, H.A. Consanguinity and reproductive health among Arabs. Reprod. Health 2009, 6, 17. [Google Scholar] [CrossRef] [Green Version]
- Shawky, R.M.; Elsayed, N.S.; Ibrahim, D.S.; Seifeldin, N.S. Profile of genetic disorders prevalent in northeast region of Cairo, Egypt. Egypt. J. Med. Hum. Genet. 2012, 13, 45–62. [Google Scholar] [CrossRef] [Green Version]
- Al-Sulaiman, A.; Saeedi, M.; Al-Suliman, A.; Owaidah, T. Postmarital follow-up survey on high risk patients subjected to premarital screening program in Saudi Arabia. Prenat. Diagn. 2010, 30, 478–481. [Google Scholar] [CrossRef]
- Cousens, N.E.; Gaff, C.L.; Metcalfe, S.A.; Delatycki, M.B. Carrier screening for beta thalassaemia: A review of international practice. Eur. J. Hum. Genet. 2010, 18, 1077–1083. [Google Scholar] [CrossRef]
- Stark, Z.; Massie, J.; McClaren, B.; Loannou, L.; Cousens, N.; Lewis, S.; Metcalfe, S.; Delatycki, M.B. Current practice and attitudes of Australian obstetricians toward population-based carrier screening for inherited conditions. Twin Res. Hum. Genet. 2013, 16, 601–607. [Google Scholar] [CrossRef] [PubMed]
- Canatan, D.; Aydinok, Y.; Kilinc, Y.; Karakaş, Z.; Şaşmaz, İ.; Apak, H.; Sarper, N. National thalassemia prevention campaign: The talotir project. Turk. J. Haematol. 2013, 30, 91–92. [Google Scholar] [CrossRef] [PubMed]
- Alswaidi, F.M.; O’Brien, S.J. Premarital screening programmes for haemoglobinopathies, HIV and hepatitis viruses: Review and factors affecting their success. J. Med. Screen. 2009, 16, 22–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, A.; Pintus, L.; Lecca, U.; Olla, G.; Cossu, P.; Rosatelli, C.; Galanello, R. Control of homozygous ß thalassemia by carrier screening and antenatal diagnosis in Sardinia. Clin. Genet. 1984, 26, 12–22. [Google Scholar] [CrossRef]
- Fessas, P. Prevention of thalassemia and haemoglobin S syndromes in Greece. Acta Haematol. 1987, 78, 168–172. [Google Scholar] [CrossRef] [PubMed]
- Cao, A.; Rosatelli, M.C. Screening and prenatal diagnosis of the haemoglobinopathies. Baillières Clin. Haematol. 1993, 6, 263–286. [Google Scholar] [CrossRef]
- Traeger-Synodinos, J.; Vrettou, C.; Palmer, G.; Tzetis, M.; Mastrominas, M.; Davies, S.; Kanavakis, E. An evaluation of PGD in clinical genetic services through 3 years application for prevention of B-thalassaemia major and sickle cell thalassaemia. Mol. Hum. Reprod. 2003, 9, 301–307. [Google Scholar] [CrossRef] [Green Version]
- Satirapod, C.; Sukprasert, M.; Panthan, B.; Charoenyingwattana, A.; Chitayanan, P.; Chantratita, W.; Choktanasiri, W.; Trachoo, O.; Hongeng, S. Clinical utility of combined preimplantation genetic testing methods in couples at risk of passing on beta thalassemia/hemoglobin E disease: A retrospective review from a single center. PLoS ONE 2019, 14, e0225457. [Google Scholar] [CrossRef]
- Vali, S.; Mukhtar, S.; Nandi, A.; Wilson, K.; Oakley, L.; El-Toukhy, T.; Eugene Oteng-Ntim, E. Cumulative outcome of pre-implantation genetic diagnosis for sickle cell disease: A 5-year review. Br. J. Haematol. 2020, 191, 875–879. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Percentage (%) | |
|---|---|
| Age Mean ± SD | |
| ≤15 Years | 0.02 |
| 15–24 Years | 13.78 |
| 25–34 Years | 58.96 |
| ≥35 Years | 27.23 |
| Nationality | |
| Kuwaiti (KN) | 89.84 |
| Non Kuwaiti (NKN) | 10.16 |
| Gender | |
| Female | 51.03 |
| Male | 48.97 |
| Level of Education | |
| Uneducated | 0.06 |
| Elementary | 1.58 |
| Intermediate | 14.2 |
| Secondary | 31 |
| Undergraduate and Post-Graduate | 53.06 |
| Marital Status | |
| Single | 76.32 |
| Married | 4.06 |
| Divorcee | 19 |
| Widow | 0.63 |
| Total Number = 275,819 | |
| β-Thalassemia Trait | Sickle Cell Trait | ||||||
|---|---|---|---|---|---|---|---|
| Year | Population Screened | Positive Cases | PR per 1000 | 95% CI PR per 1000 | Positive Cases | PR per 1000 | 95% CI PR per 1000 |
| 2009 | 9763 | 190 | 19.46 | 16.9–22.0 | 205 | 21.00 | 18.0–24.0 |
| 2010 | 23,761 | 415 | 17.47 | 15.9–19.2 | 446 | 18.77 | 17.0–21.0 |
| 2011 | 25,050 | 488 | 19.48 | 17.8–21.3 | 445 | 17.76 | 16.0–19.0 |
| 2012 | 26,030 | 559 | 21.48 | 19.8–23.3 | 507 | 19.48 | 17.9–21.0 |
| 2013 | 26,823 | 554 | 20.65 | 19–22.4 | 531 | 19.8 | 18.0–20.0 |
| 2014 | 25,698 | 572 | 22.26 | 20.5–24.1 | 493 | 19.18 | 17.6–21.0 |
| 2015 | 25,693 | 556 | 21.64 | 19.9–23.0 | 504 | 19.62 | 17.9–21.4 |
| 2016 | 24,304 | 562 | 23.12 | 21.3–25.0 | 489 | 20.12 | 18.4–22.0 |
| 2017 | 24,047 | 645 | 26.82 | 24.8–28.9 | 485 | 20.17 | 18.5–22.0 |
| 2018 | 24,573 | 480 | 19.53 | 17.8–21.0 | 349 | 14.20 | 12.8–15.8 |
| 2019 | 25,780 | 557 | 21.61 | 19.9–23.0 | 348 | 13.50 | 12.1–14.9 |
| 2020-August | 14,297 | 283 | 19.79 | 17.6–22.0 | 201 | 14.06 | 12.3–16.0 |
| Total | 275,819 | ||||||
| Total Number of Cases | Percentage % | |
|---|---|---|
| Hb D Trait | 747 | 0.271 |
| Hb D/D Disease | 27 | 0.010 |
| Hb D/B Disease | 4 | 0.001 |
| Hb D/C Disease | 2 | 0.001 |
| Hb S/D Disease | 8 | 0.003 |
| Hb S/E Disease | 1 | 0 |
| Hb S/C Disease | 2 | 0.001 |
| Hb E Trait | 145 | 0.053 |
| Hb E/E Disease | 6 | 0.002 |
| Hb C Trait | 49 | 0.018 |
| Hb C/C Disease | 3 | 0.001 |
| Hb H Disease | 70 | 0.025 |
| Hb H Disease + Sickle Cell Trait | 4 | 0.001 |
| HPFH | 20 | 0.007 |
| Hb DELTA/ B-Thal Trait * | 22 | 0.008 |
| Hb Lepore Trait | 2 | 0.001 |
| Hb Delta Thalassemia * | 20 | 0.007 |
| Hb C/B Thal Disease | 1 | 0 |
| Year | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | Total | % | N.B | |
| All Issued Certificates | Safe Marriage | 11,632 | 12,319 | 12,856 | 13,315 | 12,747 | 12,752 | 12,039 | 11,937 | 12,209 | 12,782 | 13,156 | 137,744 | 98% | 140,293% out of total issued and stop certificates |
| Unsafe Marriage | 186 | 129 | 159 | 132 | 124 | 143 | 141 | 118 | 108 | 121 | 124 | 1485 | 1% | ||
| Total | 11,818 | 12,448 | 13,015 | 13,447 | 12,871 | 12,895 | 12,180 | 12,055 | 12,317 | 12,903 | 13,280 | 139,229 | 99% | ||
| All Stop Certificates according to A reason | Age below 21 years | 56 | 43 | 50 | 33 | 23 | 50 | 22 | 23 | 12 | 59 | 16 | 387 | 0.28% | |
| Disagreement | 47 | 46 | 61 | 46 | 55 | 23 | 40 | 50 | 43 | 16 | 83 | 510 | 0.4% | ||
| Referred for vaccination | X | 27 | 34 | 17 | 20 | 18 | 12 | 9 | 12 | 11 | 7 | 167 | 0.33% | ||
| Total | 103 | 116 | 145 | 96 | 98 | 91 | 74 | 82 | 67 | 86 | 106 | 1064 | 1% | ||
| Unsafe Issue Certificates | Blood Diseases | 18 | 23 | 36 | 30 | 25 | 39 | 41 | 32 | 36 | 41 | 37 | 358 | 0.3% | % out of total all issued certificates |
| Stop Certificates—Blood Diseases | Age < 21 years | 12 | 14 | 22 | 10 | 10 | 14 | 16 | 18 | 11 | 12 | 5 | 144 | 13.5% | 1064% out of total all stop certificates |
| Disagree after counseling | 4 | 11 | 13 | 10 | 12 | 17 | 15 | 17 | 18 | 23 | 28 | 168 | 15.8% | ||
| Total | 16 | 25 | 35 | 20 | 22 | 31 | 31 | 35 | 29 | 35 | 33 | 312 | 29% | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rouh AlDeen, N.; Osman, A.A.; Alhabashi, M.J.; Al Khaldi, R.; Alawadi, H.; Alromh, M.K.; Alyafai, E.G.; Akbulut-Jeradi, N. The Prevalence of β-Thalassemia and Other Hemoglobinopathies in Kuwaiti Premarital Screening Program: An 11-Year Experience. J. Pers. Med. 2021, 11, 980. https://doi.org/10.3390/jpm11100980
Rouh AlDeen N, Osman AA, Alhabashi MJ, Al Khaldi R, Alawadi H, Alromh MK, Alyafai EG, Akbulut-Jeradi N. The Prevalence of β-Thalassemia and Other Hemoglobinopathies in Kuwaiti Premarital Screening Program: An 11-Year Experience. Journal of Personalized Medicine. 2021; 11(10):980. https://doi.org/10.3390/jpm11100980
Chicago/Turabian StyleRouh AlDeen, Najat, Asmaa A Osman, Monira J Alhabashi, Rasha Al Khaldi, Hassan Alawadi, Maha K Alromh, Eiman G Alyafai, and Nagihan Akbulut-Jeradi. 2021. "The Prevalence of β-Thalassemia and Other Hemoglobinopathies in Kuwaiti Premarital Screening Program: An 11-Year Experience" Journal of Personalized Medicine 11, no. 10: 980. https://doi.org/10.3390/jpm11100980
APA StyleRouh AlDeen, N., Osman, A. A., Alhabashi, M. J., Al Khaldi, R., Alawadi, H., Alromh, M. K., Alyafai, E. G., & Akbulut-Jeradi, N. (2021). The Prevalence of β-Thalassemia and Other Hemoglobinopathies in Kuwaiti Premarital Screening Program: An 11-Year Experience. Journal of Personalized Medicine, 11(10), 980. https://doi.org/10.3390/jpm11100980