Visceral Origin: An Underestimated Source of Neck Pain. A Systematic Scoping Review

 ,
,  , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Study Selection
2.3. Assessment of the Methodological Quality
2.4. Data Extraction
3. Results
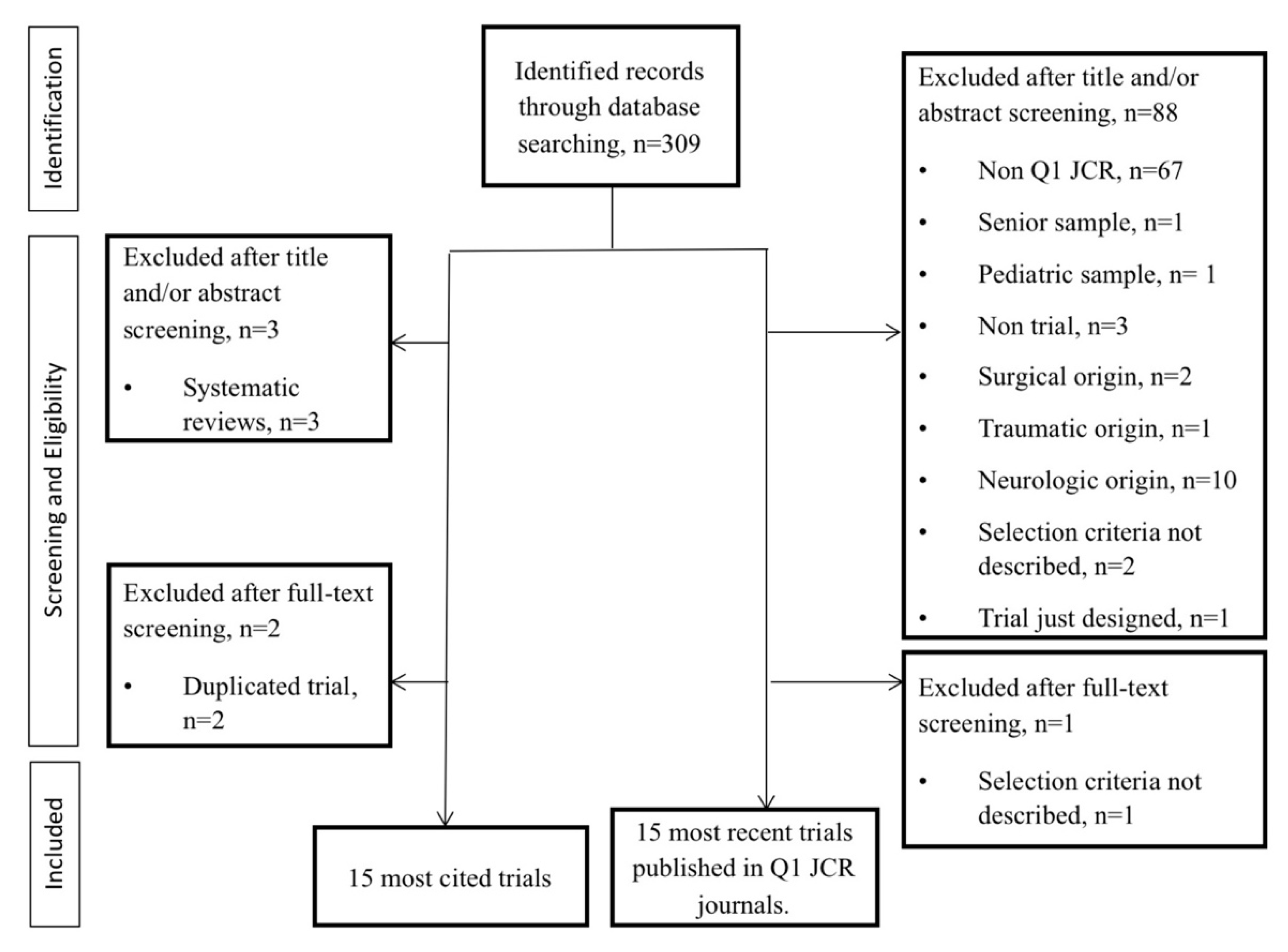
3.1. Study Selection
3.2. Study Characteristics
3.3. Methodological Quality of Studies
3.4. Eligibility Criteria (Inclusion and Exclusion Criteria) Used by Trials
4. Discussion
4.1. Eligibility Criteria Used by Trials to Select NP Patients
4.2. Somatic Consequences of Visceral Disorders
4.3. Needs for the Future
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hoy, D.G.; Protani, M.; De, R.; Buchbinder, R. The epidemiology of neck pain. Best Pract. Res. Clin. Rheumatol. 2010, 24, 783–792. [Google Scholar] [CrossRef] [PubMed]
- Hoy, D.; March, L.; Woolf, A.; Blyth, F.; Brooks, P.; Smith, E.; Vos, T.; Barendregt, J.; Blore, J.; Murray, C.; et al. The global burden of neck pain: Estimates from the global burden of disease 2010 study. Ann. Rheum. Dis. 2014, 73, 1309–1315. [Google Scholar] [CrossRef] [PubMed]
- Driessen, M.T.; Lin, C.W.; van Tulder, M.W. Cost-effectiveness of conservative treatments for neck pain: A systematic review on economic evaluations. Eur. Spine J. 2012, 21, 1441–1450. [Google Scholar] [CrossRef] [PubMed]
- Bono, C.M.; Ghiselli, G.; Gilbert, T.J.; Kreiner, D.D.; Reitman, C.; Summers, J.T.; Baisden, J.T.; Easa, J.; Fernand, R.; Lamer, T.; et al. An evidence-based clinical guideline for the diagnosis and treatment of cervical radiculopathy from degenerative disorders. Spine J. 2011, 11, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Kjaer, P.; Kongsted, A.; Hartvigsen, J.; Isenberg-Jorgensen, A.; Schiottz-Christensen, B.; Soborg, B.; Krog, C.; Moller, C.M.; Halling, C.M.B.; Lauridsen, H.H.; et al. National clinical guidelines for non-surgical treatment of patients with recent onset neck pain or cervical radiculopathy. Eur. Spine J. 2017, 26, 2242–2257. [Google Scholar] [CrossRef] [PubMed]
- Falco, F.J.; Erhart, S.; Wargo, B.W.; Bryce, D.A.; Atluri, S.; Datta, S.; Hayek, S.M. Systematic review of diagnostic utility and therapeutic effectiveness of cervical facet joint interventions. Pain Physician 2009, 12, 323–344. [Google Scholar] [PubMed]
- Ambrose, N.L.; Cunnane, G. Importance of full evaluation in patients who complain of neck pain. Ir. J. Med. Sci. 2009, 178, 209–210. [Google Scholar] [CrossRef] [PubMed]
- Childs, J.D.; Cleland, J.A.; Elliott, J.M.; Teyhen, D.S.; Wainner, R.S.; Whitman, J.M.; Sopky, B.J.; Godges, J.J.; Flynn, T.W. Neck pain: Clinical practice guidelines linked to the International Classification of Functioning, Disability, and Health from the Orthopaedic Section of the American Physical Therapy Association. J. Orthop. Sports Phys. Ther. 2008, 38, A1–A34. [Google Scholar] [CrossRef] [PubMed]
- Giamberardino, M.A.; Costantini, R.; Affaitati, G.; Fabrizio, A.; Lapenna, D.; Tafuri, E.; Mezzetti, A. Viscero-visceral hyperalgesia: Characterization in different clinical models. Pain 2010, 151, 307–322. [Google Scholar] [CrossRef] [PubMed]
- Giamberardino, M.; Affaitati, G.; Costantini, R. Visceral referred pain. J. Musculoskelet. Pain 2010, 18, 403–410. [Google Scholar] [CrossRef]
- Ruch, T.; Patton, H. Pathophysiology of Pain: Physiology and Biophysics; Saunders: Philadelpia, PA, USA, 1965. [Google Scholar]
- Luz, L.L.; Fernandes, E.C.; Sivado, M.; Kokai, E.; Szucs, P.; Safronov, B.V. Monosynaptic convergence of somatic and visceral C-fiber afferents on projection and local circuit neurons in lamina I: A substrate for referred pain. Pain 2015, 156, 2042–2051. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.D.; Russell, A.; Hodges, P.W. How common is back pain in women with gastrointestinal problems? Clin. J. Pain 2008, 24, 199–203. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.G.; Chang, M.C. Neck-to-shoulder pain as an unusual presentation of pulmonary embolism in a patient with cervical spinal cord injury: A case report. Medicine 2017, 96, e8288. [Google Scholar] [CrossRef] [PubMed]
- Goodman, C.C. Screening for gastrointestinal, hepatic/biliary, and renal/urologic disease. J. Hand Ther. 2010, 23, 140–156. [Google Scholar] [CrossRef] [PubMed]
- Jarrell, J.; Giamberardino, M.A.; Robert, M.; Nasr-Esfahani, M. Bedside testing for chronic pelvic pain: Discriminating visceral from somatic pain. Pain Res. Treat. 2011, 2011, 692102. [Google Scholar] [CrossRef] [PubMed]
- Head, H. On disturbances of sensation with especial reference to the pain of visceral disease. Brain 1893, 16, 1–133. [Google Scholar] [CrossRef]
- Amsterdam, E.A.; Wenger, N.K.; Brindis, R.G.; Casey, D.E.; Ganiats, T.G.; Holmes, D.R.; Jaffe, A.S.; Jneid, H.; Kelly, R.F.; Kontos, M.C.; et al. 2014 AHA/ACC Guideline for the management of patients with non-st-elevation acute coronary syndromes: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J. Am. Coll. Cardiol. 2014, 64, e139–e228. [Google Scholar] [CrossRef] [PubMed]
- Horne, R.; James, D.; Petrie, K.; Weinman, J.; Vincent, R. Patients’ interpretation of symptoms as a cause of delay in reaching hospital during acute myocardial infarction. Heart 2000, 83, 388–393. [Google Scholar] [CrossRef] [PubMed]
- Saad, A.; Rex, D.K. Colonoscopy-induced splenic injury: Report of 3 cases and literature review. Dig. Dis. Sci. 2008, 53, 892–898. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.W.L.; McPhee, R.W.; Stringer, M.D. An evidence-based approach to human dermatomes. Clin. Anat. 2008, 21, 363–373. [Google Scholar] [CrossRef] [PubMed]
- Khosa, F.; McNulty, J.G.; Hickey, N.; O’Brien, P.; Tobin, A.; Noonan, N.; Ryan, B.; Keeling, P.W.; Kelleher, D.P.; McDonald, G.S. Transvenous liver biopsy via the femoral vein. Clin. Radiol. 2003, 58, 487–491. [Google Scholar] [CrossRef]
- Flanagin, B.A.; Mitchell, M.T.; Thistlethwaite, W.A.; Alverdy, J.C. Diagnosis and treatment of atypical presentations of hiatal hernia following bariatric surgery. Obes. Surg. 2010, 20, 386–392. [Google Scholar] [CrossRef] [PubMed]
- Lehwald, N.; Krausch, M.; Franke, C.; Assmann, B.; Adam, R.; Knoefel, W.T. Sandifer syndrome: A multidisciplinary diagnostic and therapeutic challenge. Eur. J. Pediatr. Surg. 2007, 17, 203–206. [Google Scholar] [CrossRef] [PubMed]
- Monticone, M.; Iovine, R.; de Sena, G.; Rovere, G.; Uliano, D.; Arioli, G.; Bonaiuti, D.; Brugnoni, G.; Ceravolo, G.; Cerri, C.; et al. The Italian Society of Physical and Rehabilitation Medicine (SIMFER) recommendations for neck pain. G. Ital. Med. Lav. Ergon. 2013, 35, 36–50. [Google Scholar] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O´Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Int. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- De Morton, N.A. The PEDro scale is a valid measure of the methodological quality of clinical trials: A demographic study. Aust. J. Physiother. 2009, 55, 129–133. [Google Scholar] [CrossRef]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [PubMed]
- Armijo-Olivo, S.; da Costa, B.R.; Cummings, G.G.; Ha, C.; Fuentes, J.; Saltaji, H.; Egger, M. PEDro or Cochrane to assess the quality of clinical trials? A Meta-Epidemiological Study. PLoS ONE 2015, 10, e0132634. [Google Scholar] [CrossRef] [PubMed]
- Cerezo-Téllez, E.; Torres-Lacomba, M.; Fuentes-Gallardo, I.; Perez-Munoz, M.; Mayoral-del-Moral, O.; Lluch-Girbes, E.; Prieto-Valiente, L.; Falla, D. Effectiveness of dry needling for chronic nonspecific neck pain: A randomized, single-blinded, clinical trial. Pain 2016, 157, 1905–1917. [Google Scholar] [CrossRef] [PubMed]
- Viljanen, M.; Malmivaara, A.; Uitti, J.; Rinne, M.; Palmroos, R.; Laippala, P. Effectiveness of dynamic muscle training, relaxation training, or ordinary activity for chronic neck pain: Randomised controlled trial. BMJ 2003, 327, 475. [Google Scholar] [CrossRef] [PubMed]
- Ylinen, J.; Takala, E.P.; Nykänen, M.; hakkinen, A.; Malkia, E.; Pohjolainen, T.; Karppi, S.-L.; Kautiainen, H.; Airaksinen, O. Active neck muscle training in the treatment of chronic neck pain in women: A randomized controlled trial. JAMA 2003, 289, 2509–2516. [Google Scholar] [CrossRef] [PubMed]
- Thompson, D.P.; Oldham, J.A.; Woby, S.R. Does adding cognitive-behavioural physiotherapy to exercise improve outcome in patients with chronic neck pain? A randomised controlled trial. Physiotherapy 2016, 102, 170–177. [Google Scholar] [CrossRef] [PubMed]
- De Araujo Cazotti, L.; Jones, A.; Roger-Silva, D.; Ribeiro, L.H.C.; Natour, J. Effectiveness of the Pilates method in the treatment of chronic mechanical neck pain: A randomized controlled trial. Arch. Phys. Med. Rehabil. 2018, 99, 1740–1746. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Carnero, J.; Sierra-Silvestre, E.; Beltran-Alacreu, H.; Gil-Martinez, A.; La Touche, R. Neural tension technique improves immediate conditioned pain modulation in patients with chronic neck pain: A randomized clinical trial. Pain Med. 2019, 20, 1227–1235. [Google Scholar] [CrossRef] [PubMed]
- Jordan, A.; Bendix, T.; Nielsen, H.; Hansen, F.R.; Host, D.; Winkel, A. Intensive training, physiotherapy, or manipulation for patients with chronic neck pain. A prospective, single-blinded, randomized clinical trial. Spine 1998, 23, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Essex, H.; Parrott, S.; Atkin, K.; Ballard, K.; Blanda, M.; Eldred, J.; Hewitt, C.; Hopton, A.; Keding, A.; Lansdown, H.; et al. An economic evaluation of Alexander Technique lessons or acupuncture sessions for patients with chronic neck pain: A randomized trial (ATLAS). PLoS ONE 2017, 12, e0178918. [Google Scholar] [CrossRef] [PubMed]
- Manchikanti, L.; Singh, V.; Falco, F.J.; Cash, K.A.; Fellows, B. Comparative outcomes of a 2-year follow-up of cervical medial branch blocks in management of chronic neck pain: A randomized, double-blind controlled trial. Pain Physician 2010, 13, 437–450. [Google Scholar] [PubMed]
- Viera, A.J.; Garrett, J.M. Understanding interobserver agreement: The kappa statistic. Fam. Med. 2005, 37, 360–363. [Google Scholar] [PubMed]
- Cleland, J.A.; Childs, J.D.; McRae, M.; palmer, J.A.; Stowell, T. Immediate effects of thoracic manipulation in patients with neck pain: A randomized clinical trial. Man. Ther. 2005, 10, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Irnich, D.; Behrens, N.; Molzen, H.; Konig, A.; Gleditsch, J.; Krauss, M.; Natalis, M.; Senn, E.; Beyer, A.; Schops, P. Randomised trial of acupuncture compared with conventional massage and “sham” laser acupuncture for treatment of chronic neck pain. BMJ 2001, 322, 1574–1578. [Google Scholar] [CrossRef] [PubMed]
- Korthals-de Bos, I.B.; Hoving, J.L.; van Tulder, M.W.; Rutten-van-Molken, M.P.M.H.; Ader, H.J.; de Vet, H.C.M.; Koes, B.W.; Vondeling, H.; Bouter, L.M. Cost effectiveness of physiotherapy, manual therapy, and general practitioner care for neck pain: Economic evaluation alongside a randomised controlled trial. BMJ 2003, 326, 911. [Google Scholar] [PubMed]
- Cleland, J.A.; Glynn, P.; Whitman, J.M.; Eberhart, S.L.; MacDonald, C.; Childs, J.D. Short-term effects of thrust versus nonthrust mobilization/manipulation directed at the thoracic spine in patients with neck pain: A randomized clinical trial. Phys. Ther. 2007, 87, 431–440. [Google Scholar] [CrossRef] [PubMed]
- Irnich, D.; Behrens, N.; Gleditsch, J.M.; Stor, W.; Schreiber, M.A.; Schops, P.; Vickers, A.J.; Beyer, A. Immediate effects of dry needling and acupuncture at distant points in chronic neck pain: Results of a randomized, double-blind, sham-controlled crossover trial. Pain 2002, 99, 83–89. [Google Scholar] [CrossRef]
- Hurwitz, E.L.; Morgenstern, H.; Harber, P.; Koniski, G.F.; Yu, F.; Adams, A.H. A randomized trial of chiropractic manipulation and mobilization for patients with neck pain: Clinical outcomes from the UCLA neck-pain study. Am. J. Public Health 2002, 92, 1634–1641. [Google Scholar] [CrossRef] [PubMed]
- White, P.; Lewith, G.; Prescott, P.; Conway, J. Acupuncture versus placebo for the treatment of chronic mechanical neck pain: A randomized, controlled trial. Ann. Intern. Med. 2004, 141, 911–919. [Google Scholar] [CrossRef] [PubMed]
- Evans, R.; Bronfort, G.; Nelson, B.; Goldsmith, C.H. Two-year follow-up of a randomized clinical trial of spinal manipulation and two types of exercise for patients with chronic neck pain. Spine 2002, 27, 2383–2389. [Google Scholar] [CrossRef] [PubMed]
- Hoving, J.L.; de Vet, H.C.; Koes, B.W.; van Mameren, H.; Deville, W.L.J.M.; van der Windt, D.A.W.M.; Assendelft, W.J.J.; Pool, J.J.M.; Scholten, R.J.P.M.; Korthals-deBos, I.B.C.; et al. Manual therapy, physical therapy, or continued care by the general practitioner for patients with neck pain: Long-term results from a pragmatic randomized clinical trial. Clin. J. Pain 2006, 22, 370–377. [Google Scholar] [CrossRef] [PubMed]
- Chiu, T.T.; Lam, T.H.; Hedley, A.J. A randomized controlled trial on the efficacy of exercise for patients with chronic neck pain. Spine 2005, 30, E1–E7. [Google Scholar] [CrossRef] [PubMed]
- Bronfort, G.; Evans, R.; Anderson, A.V.; Svendsen, K.H.; Bracha, Y.; Grimm, R.H. Spinal manipulation, medication, or home exercise with advice for acute and subacute neck pain: A randomized trial. Ann. Intern. Med. 2012, 156, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Celenay, S.T.; Kaya, D.O.; Akbayrak, T. Cervical and scapulothoracic stabilization exercises with and without connective tissue massage for chronic mechanical neck pain: A prospective, randomised controlled trial. Man. Ther. 2016, 21, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Celenay, S.T.; Akbayrak, T.; Kaya, D.O. A comparison of the effects of stabilization exercises plus manual therapy to those of stabilization exercises alone in patients with nonspecific mechanical neck pain: A randomized clinical trial. J. Orthop. Sports Phys. Ther. 2016, 46, 44–55. [Google Scholar] [CrossRef] [PubMed]
- Griswold, D.; Learman, K.; Kolber, M.J.; O’Halloran, B.; Cleland, J.A. Pragmatically applied cervical and thoracic nonthrust manipulation versus thrust manipulation for patients with mechanical neck pain: A multicenter randomized clinical trial. J. Orthop. Sports Phys. Ther. 2018, 48, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Krøll, L.S.; Hammarlund, C.S.; Linde, M.; Gard, G.; Jensen, R.H. The effects of aerobic exercise for persons with migraine and co-existing tension-type headache and neck pain. A randomized, controlled, clinical trial. Cephalalgia 2018, 38, 1805–1816. [Google Scholar] [CrossRef] [PubMed]
- Lauche, R.; Stumpe, C.; Fehr, J.; Cramer, H.; Cheng, Y.W.; Wayne, P.M.; Rampp, T.; Langhorst, J.; Dobos, G. The effects of Tai Chi and neck exercises in the treatment of chronic nonspecific neck pain: A randomized controlled trial. J. Pain. 2016, 17, 1013–1027. [Google Scholar] [CrossRef] [PubMed]
- Lauche, R.; Schuth, M.; Schwickert, M.; Ludtke, R.; Musial, F.; Michalsen, A.; Dobos, G.; Choi, K.E. Efficacy of the Alexander Technique in treating chronic non-specific neck pain: A randomized controlled trial. Clin. Rehabil. 2016, 30, 247–258. [Google Scholar] [CrossRef] [PubMed]
- Monticone, M.; Ambrosini, E.; Rocca, B.; Cazzaniga, D.; Liquori, V.; Pedrocchi, A.; Vernon, H. Group-based multimodal exercises integrated with cognitive-behavioural therapy improve disability, pain and quality of life of subjects with chronic neck pain: A randomized controlled trial with one-year follow-up. Clin. Rehabil. 2017, 31, 742–752. [Google Scholar] [CrossRef] [PubMed]
- Pillastrini, P.; de Lima E Sá Resende, F.; Banchelli, F.; Burioli, A.; Di CIaccio, E.; Guccione, A.A.; Villafañe, J.H.; Vanti, C. Effectiveness of Global Postural Re-education in patients with chronic nonspecific neck pain: Randomized controlled trial. Phys. Ther. 2016, 96, 1408–1416. [Google Scholar] [CrossRef] [PubMed]
- Ris, I.; Søgaard, K.; Gram, B.; Agerbo, K.; Boyle, E.; Juul-Kristensen, B. Does a combination of physical training, specific exercises and pain education improve health-related quality of life in patients with chronic neck pain? A randomised control trial with a 4-month follow up. Man. Ther. 2016, 26, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Tunwattanapong, P.; Kongkasuwan, R.; Kuptniratsaikul, V. The effectiveness of a neck and shoulder stretching exercise program among office workers with neck pain: A randomized controlled trial. Clin. Rehabil. 2016, 30, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Giamberardino, M.A. Clinical Updates. Visceral Pain. Pain 2005, 12, 1–6. [Google Scholar]
- Giamberardino, M.A. Recent and forgotten aspects of visceral pain. Eur. J. Pain 1999, 3, 77–92. [Google Scholar] [CrossRef] [PubMed]
- Gerwin, R. Myofascial and visceral pain syndromes: Visceral-somatic pain representations. J. Musculoskelet. Pain 2002, 10, 65–75. [Google Scholar] [CrossRef]
- Srbely, J.Z. New trends in the treatment and management of myofascial pain syndrome. Curr. Pain Headache Rep. 2010, 14, 346–352. [Google Scholar] [CrossRef] [PubMed]
- Campos Kraychete, D.; Tesseroli de Siqueira, J.; Batista García, J.; Kimiko Sakata, R.; Sousa, A.M.; de Andrade, D.C.; Mariotto Zakka, T.R.; Jacobsen Teixeira, M. Clinical evidence on visceral pain. Systematic review. Rev. Dor 2017, 18, 65–71. [Google Scholar] [CrossRef]
- Rana, A.Q.; Yousuf, M.S.; Joian, S. A chronic case of adult-onset Sandifer syndrome. Neurol. Sci. 2013, 34, 405–406. [Google Scholar] [CrossRef] [PubMed]
- Han, D.G.; Lee, C.J. Headache associated with visceral disorders is “parasympathetic referred pain”. Med. Hypotheses 2009, 73, 561–563. [Google Scholar] [CrossRef] [PubMed]
- Williams, P.; Bannister, L.; Berry, M. Gray’s Anatomy, 38th ed.; Churchill Livingstone: New York, NY, USA, 1995. [Google Scholar]
- Kostreva, D.R.; Pontus, S.P. Pericardial mechanoreceptors with phrenic afferents. Am. J. Physiol. 1993, 264, H1836–H1846. [Google Scholar] [CrossRef] [PubMed]
- Loukas, M.; Du Plessis, M.; Louis, R.G.; Tubbs, R.S.; Wartmann, C.T.; Apaydin, N. The subdiaphragmatic part of the phrenic nerve—Morphometry and connections to autonomic ganglia. Clin. Anat. 2016, 29, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Rusu, M.C. Considerations on the phrenic ganglia. Ann. Anat. 2006, 188, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Netter, F. Atlas of Human Anatomy; Saunders/Elsevier: Philadelphia, PA, USA, 2011. [Google Scholar]
- Hartmann, H.; Beckh, K. Nerve supply and nervous control of liver function. In Textbook of Clinical Hematology; McIntyre, N., Benhamou, J., Bircher, J., Eds.; Oxford University Press: Oxford, UK, 1992; p. 93. [Google Scholar]
- Kostreva, D.R.; Pontus, S.P. Hepatic vein, hepatic parenchymal, and inferior vena caval mechanoreceptors with phrenic afferents. Am. J. Physiol. 1993, 265, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Misih, S.R.; Bloomston, M. Liver anatomy. Surg. Clin. N. Am. 2010, 90, 643–653. [Google Scholar] [CrossRef] [PubMed]
- Iwahashi, K.; Matsuda, R.; Tsunekawa, K. Afferent innervation of the gallbladder in the cat, studied by the horseradish peroxidase method. J. Auton. Nerv. Syst. 1991, 32, 145–151. [Google Scholar] [CrossRef]
- Yi, S.Q.; Ohta, T.; Tsuchida, A.; Terayama, H.; Naito, M.; Li, J.; Wang, H.X.; Yi, N.; Tanaka, S.; Itoh, M. Surgical anatomy of innervation of the gallbladder in humans and Suncus murinus with special reference to morphological understanding of gallstone formation after gastrectomy. World J. Gastroenterol. 2007, 13, 2066–2071. [Google Scholar] [CrossRef] [PubMed]
- Yi, S.Q.; Ren, K.; Kinoshita, M.; Takano, M.; Itoh, M.; Ozaki, N. Innervation of extrahepatic biliary tract, with special reference to the direct bidirectional neural connections of the gall bladder, sphincter of Oddi and duodenum in Suncus murinus, in whole-mount immunohistochemical study. Anat. Histol. Embryol. 2016, 45, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Yin, W.; Bogduk, N. The nature of neck pain in a private pain clinic in the United States. Pain. Med. 2008, 9, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Eusebi, L.H.; Ratnakumaran, R.; Yuan, Y.; Solaymani-DOdaran, M.; Bazzoli, F.; Ford, A.C. Global prevalence of, and risk factors for, gastro-oesophageal reflux symptoms: A meta-analysis. Gut 2018, 67, 430–440. [Google Scholar] [CrossRef] [PubMed]
- Knab, L.M.; Boller, A.M.; Mahvi, D.M. Cholecystitis. Surg. Clin. N. Am. 2014, 94, 455–470. [Google Scholar] [CrossRef] [PubMed]
- Bedogni, G.; Miglioli, L.; Masutti, F.; Tiribelli, C.; Marchesini, G.; Bellentani, S. Prevalence of and risk factors for nonalcoholic fatty liver disease: The Dionysos nutrition and liver study. Hepatology 2005, 42, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Côté, P.; Cassidy, J.D.; Carroll, L. The factors associated with neck pain and its related disability in the Saskatchewan population. Spine 2000, 25, 1109–1117. [Google Scholar] [CrossRef] [PubMed]
- Ozaki, N.; Bielefeldt, K.; Sengupta, J.N.; Gebhart, G.F. Models of gastric hyperalgesia in the rat. Am. J. Physiol. Gastrointest. Liver Physiol. 2002, 283, G666–G676. [Google Scholar] [CrossRef] [PubMed]
- Palacios-Ceña, D.; Alonso-Blanco, C.; Hernández-Barrera, V.; Carrasco-Garrido, P.; Jimenez-Garcia, R.; Fernandez-de-las-Penas, C. Prevalence of neck and low back pain in community-dwelling adults in Spain: An updated population-based national study (2009/10–2011/12). Eur. Spine J. 2015, 24, 482–492. [Google Scholar] [CrossRef] [PubMed]
- Kumagai, G.; Wada, K.; Tanaka, T.; Kudo, H.; Asari, T.; Chiba, D.; Ota, S.; Nakaji, S.; Ishibayi, I. Associations between neck symptoms and LDL cholesterol in a cross-sectional population-based study. J. Orthop. Sci. 2018, 23, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Mäntyselkä, P.; Kautiainen, H.; Vanhala, M. Prevalence of neck pain in subjects with metabolic syndrome: A cross-sectional population-based study. BMC Musculoskelet. Disord. 2010, 11, 171. [Google Scholar] [CrossRef] [PubMed]
- Nair, J.; Streeter, K.A.; Turner, S.M.F.; Sunshine, M.D.; Bolser, D.C.; Fox, E.J.; Davenport, P.W.; Fuller, D.D. Anatomy and physiology of phrenic afferent neurons. J. Neurophysiol. 2017, 118, 2975–2990. [Google Scholar] [CrossRef] [PubMed]
- Rouzade, M.L.; Fioramonti, J.; Bueno, L. A model for evaluation of gastric sensitivity in awake rats. Neurogastroenterol. Motil. 1998, 10, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.H.; Hu, J.; Zhou, Y.L.; Hu, S.F.; Wang, Y.M.; Chen, W.; Xiao, Y.; Huang, L.Y.M.; Jiang, X.H.; Xu, G.Y. Promoted interaction of nuclear factor -kB with demethylated cystathione-β-synthetase gene contributes to gastric hypersensitivity in diabetic rats. J. Neurosci. 2013, 33, 9028–9038. [Google Scholar] [CrossRef] [PubMed]
- Giamberardino, M.A.; Affaitati, G.; Lerza, R.; fano, G.; Fulle, S.; Belia, S.; Lapenna, D.; Vecchiet, L. Evaluation of indices of skeletal muscle contraction in areas of referred hyperalgesia from an artificial ureteric stone in rats. Neurosci. Lett. 2003, 338, 213–216. [Google Scholar] [CrossRef]
- Sun, Y.; Tan, Y.; Song, G. Effects and mechanisms of gastric electrical stimulation on visceral pain in a rodent model of gastric hyperalgesia secondary to chemically induced mucosal ulceration. Neurogastroenterol. Motil. 2014, 26, 176–186. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Li, S.; Yin, J.; Chen, J.D.Z. Ameliorating effects of optimized gastric electrical stimulation and mechanisms involving nerve growth factor opioids in a rodent model of gastric hypersensitivity. Neurogastroenterol. Motil. 2019, 31, e13551. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.C.O.; Biasotto-Gonzalez, D.A.; Oliveira, F.H.M.; Andrade, A.O.; Gomes, C.A.F.D.; Lanza, F.D.; Amorim, C.F.; Politti, F. Effect of osteopathic visceral manipulation on pain, cervical range of motion, and upper trapezius muscle activity in patients with chronic nonspecific neck pain and functional dispepsia: A randomized, doublé-blind, placebo-controlled pilot study. Evid. Based Complement. Alternat. Med. 2018, 2018, 4929271. [Google Scholar] [CrossRef] [PubMed]
- Eguaras, N.; Rodriguez-Lopez, E.S.; Lopez-Dicastillo, O.; Franco-Sierra, M.A.; Ricard, F.; Oliva-Pascual-Vaca, A. Effects of osteopathic visceral treatment in patients with gastroesophageal reflux: A randomized controlled trial. J. Clin. Med. 2019, 8, 1738. [Google Scholar] [CrossRef] [PubMed]
- Sterling, M.; de Zoete, R.M.J.; Coppieters, I.; Farrell, S.C. Best evidence rehabilitation for chronic pain Part 4: Neck pain. J. Clin. Med. 2019, 8, 1219. [Google Scholar] [CrossRef] [PubMed]
- Sergent, S.R.; Johnson, S.M.; Ashurst, J.; Johnston, G. Epstein-Barr virus associated atraumatic spleen laceration presenting with neck and shoulder pain. Am. J. Case Rep. 2015, 16, 774–777. [Google Scholar] [CrossRef] [PubMed]
- Carter, C.T. Acute thoracolumbar pain due to pholecystitis: A case study. Chiropr. Man. Ther. 2015, 23, 34. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Srirangam, S.J.; Pollard, A.J.; Adeyoju, A.A.; O’Reilly, P.H. Nephroptosis: Seriously misunderstood? Bju Int. 2009, 103, 296–300. [Google Scholar] [CrossRef] [PubMed]
- Hoenig, D.M.; Hemal, A.K.; Shalhav, A.L.; Clayman, R.V. Nephroptosis: A “disparaged” condition revisited. Urology 1999, 54, 590–596. [Google Scholar] [CrossRef]
- Luong, C.; Starovoytov, A.; Heydari, M.; Sedlak, T.; Aymong, E.; Saw, J. Clinical presentation of patients with spontaneous coronary artery dissection. Catheter. Cardiovasc. Interv. 2017, 89, 1149–1154. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Xu, C.; Deng, K.; Zhou, X.; Liu, Z.B.; Busse, J.W.; Ren, Y.; Zou, K.; Sun, X. The reporting of safety among drug systematic reviews was poor before the implementation of the PRISMA harms checklist. J. Clin. Epidemiol. 2019, 105, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Prasad, V.; Gall, V.; Cifu, A. The frequency of medical reversal. Arch. Intern. Med. 2011, 171, 1675–1676. [Google Scholar] [CrossRef] [PubMed]
- Crutzen, R.; Viechtbauer, W.; Spigt, M.; Kotz, D. Differential attrition in health behaviour change trials: A systematic review and meta-analysis. Psychol. Health. 2015, 30, 122–134. [Google Scholar] [CrossRef] [PubMed]
- Mbuagbaw, L.; Thabane, M.; Vanniyasingam, T.; Debono, V.B.; Kosa, S.; Zhang, S.Y.; Ye, C.L.; Parpia, S.; Dennis, B.B.; Thabane, L. Improvement in the quality of abstracts in major clinical journals since CONSORT extension for abstracts: A systematic review. Contemp. Clin. Trials 2014, 38, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Kho, M.E.; Duffet, M.; Willison, D.J.; Cook, D.J.; Brouwers, M.C. Written informed consent and selection bias in observational studies using medical records: Systematic review. BMJ 2009, 338, b866. [Google Scholar] [CrossRef] [PubMed]
- Hrobjartsson, A.; Skou, A.S.; Emanuelsson, F.; Tendal, B.; Hilden, J.; Boutron, I.; Ravaud, P.; Brorson, S. Observer bias in randomised clinical trials with binary outcomes: Systematic review of trials with both blinded and non-blinded outcome assessors. BMJ 2012, 334, e1119. [Google Scholar] [CrossRef] [PubMed]
- Hrobjartsson, A.; Skou, A.S.; Emanuelsson, F.; Tendal, B.; Hilden, J.; Boutron, I.; Ravaud, P.; Brorson, S. Observer bias in randomized clinical trials with measurement scale outcomes: A systematic review of trials with both blinded and nonblinded outcome assessors. CMAJ 2013, 185, E201–E211. [Google Scholar] [CrossRef] [PubMed]
- Grimm, N.L.; Shea, K.G.; Leaver, R.W.; Aoki, S.K.; Carey, J.L. Efficacy and degree of bias in knee injury prevention studies: A systematic review of RCTs. Clin. Orthop. Relat. Res. 2013, 471, 308–316. [Google Scholar] [CrossRef] [PubMed]
- Thaler, K.; Kien, C.; Nussbaumer, B.; Van Noord, M.G.; Griebler, U.; Klerings, I.; Gartlehner, G. Inadequate use and regulation of intervention against publication bias decreases their effectiveness: A systematic review. J. Clin. Epidemiol. 2015, 68, 792–802. [Google Scholar] [CrossRef] [PubMed]
- Farzanfar, D.; Abumuamar, A.; Kim, J.; Sirotich, E.; Wang, Y.; Pullenayegum, E. Longitudinal studies that use data collected as part of usual care risk reporting biased results: A systematic review. BMC Med. Res. Methodol. 2017, 17, 133. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Study Authors’ Institutions Number of Citations | PEDro Score | Aim | Participants (Sex and Mean Age) | Inclusion Criteria | Exclusion Criteria |
|---|---|---|---|---|---|
| Ylinen et al., 2003 [32] Clinical: 5 Non-Clinical: 4 Citations: 285 | 7/10 | Assess the efficacy of intensive isometric training and light endurance training in chronic NP | N = 180 All females 46 years | Females; aged 25 to 53 years; office worker; permanently employed; motivated to continue working and for rehabilitation; constant or frequently occurring NP > than 6 months | Severe neck disorders, e.g., disk prolapse and spinal stenosis; postoperative conditions in the neck-shoulder; severe trauma; instability; spasmodic torticollis; frequent migraine; peripheral nerve entrapment; fibromyalgia; shoulder tendonitis, bursitis, or capsulitis; inflammatory rheumatic disease; severe psychiatric illness; diseases that prevent physical loading; pregnancy |
| Cleland et al., 2005 [40] Clinical: 5 Non-Clinical: 0 Citations: 156 | 8/10 | Evaluate the immediate effects of thoracic SM in chronic NP | N = 36 27 females 9 males 35 years | Aged 18 to 60 years; primary complaint of mechanical NP, defined as non-specific pain in the cervicothoracic region and exacerbated by neck movements | Red flags for serious spinal conditions, e.g., infection, tumors, osteoporosis, fracture; positive signs or symptoms suggestive of nerve root involvement, e.g., altered upper limb reflexes, sensation, or strength; cervical or thoracic surgery; prior SM treatment; thoracic spine hypermobility; pregnancy |
| Jordan et al., 1998 [36] Clinical: 3 Non-Clinical: 3 Citations: 152 | 5/10 | Assess the effectiveness of intensive cervical training vs. PT vs. chiropractic treatment in chronic NP | N = 119 88 females 31 males 39 years | Aged 20 to 60 years; NP > 3 months with or without non-radicular pain; to live within a close distance to the hospital; X-ray examination of the cervical spine; to be able to speak and read Danish | Acute NP with no freedom of movement; PT, SM, or training for the neck-upper extremity within 6 months; neuropathy; systemic disease; inflammatory joint or muscle disease; headache dominating over NP; migraine; hypermobility; whiplash; primary shoulder or upper extremity problems; previous neck surgery |
| Irnich et al., 2001 [41] Clinical: 0 Non-Clinical: 10 Citations: 146 | 7/10 | Compare the efficacy of acupuncture vs. massage combined with “sham” laser acupuncture in chronic NP | N = 177 117 females 60 males 52 years | Aged 18 to 85 years; chronic NP; painful restriction of neck mobility > 1 month; had not received any treatment in the previous 2 weeks | Previous surgery, dislocation or fracture; neurological deficits; systemic disorders; contraindications to any of the applied treatments |
| Korthals-de Bos et al., 2003 [42] Clinical: 0 Non-Clinical: 9 Citations: 137 | 6/10 | Evaluate the cost effectiveness of PT, manual therapy, and GP care for acute, subacute and chronic NP | N = 183 121 females 62 males 45 years | Aged 18 to 70 years; NP > 2 weeks (confirmed during physical examination); willingness to comply with treatment and follow up | PT or manual therapy for NP in the previous 6 months; neck surgery; a specific cause for the NP (for example, malignancy, fracture, or inflammation) |
| Cleland et al., 2007 [43] Clinical: 4 Non-Clinical: 2 Citations: 133 | 7/10 | Compare the effect of thoracic nonthrust vs. mobilization/SM, and compare frequencies, side effects, and durations in acute and subacute NP | N = 60 33 females 27 males 43 years | Aged 18 to 60 years; a primary complaint of NP with or without unilateral upper-extremity symptoms; a baseline Neck Disability Index score ≥ 10% | Signs suggestive of a non-musculoskeletal aetiology; whiplash within 6 weeks; cervical spinal stenosis; signs of nerve root compression (decrease of at least 2 of the following: myotomal strength, sensation, or reflexes); central nervous system involvement; previous cervicothoracic surgery; pending legal action |
| Irnich et al., 2002 [44] Clinical: 0 Non-Clinical: 8 Citations: 127 | 6/10 | Evaluate immediate effects of 2 different modes of acupuncture vs. sham procedure in chronic NP | N = 34 25 females 9 males 52 years | NP > 2 months; diagnosis of myofascial syndrome or irritation syndrome based on history, pain characteristics, radiological findings and manual examination | Radicular cervical syndrome; segmental instability; fracture or surgery of the cervical spine; contradictions to acupuncture; drug, PT or manual treatment in the last 4 weeks |
| Viljanen et al., 2003 [31] Clinical: 6 Non-Clinical: 0 Citations: 117 | 8/10 | Assess the effectiveness of dynamic muscle training and relaxation training in chronic NP | N = 393 All females 45 years | Female sex; aged 30 to 60 years; suffer from chronic non-specific NP > 12 weeks | Cancer; major trauma; rheumatic disease; neural entrapment; major rehabilitation in the previous 3 months |
| Hurwitz et al., 2002 [45] Clinical: 0 Non-Clinical: 6 Citations: 112 | 7/10 | Compare the relative effectiveness of cervical SM and mobilization in acute, subacute and chronic NP | N = 336 231 females 105 males 46 years | Aged 18 to 70 years; NP, defined as pain within the upper thoracic spine to the occiput and the surrounding musculature; members of health maintenance organization; had sought care at one of the study sites; had not received NP treatment in the past month | NP due to fracture, severe spondyloarthropathy, tumor, infection, or other non-mechanical cause; progressive neurological deficit, myelopathy, herniated nucleus pulposus, or severe incapacitating pain; severe coexisting disease; previous electrotherapy treatment; blood coagulation disorder; use of anticoagulant or corticosteroids; stroke or transient ischemic attacks; inability to read English; pain involving third-party liability or compensation |
| White et al., 2004 [46] Clinical: 2 Non-Clinical: 2 Citations: 104 | 7/10 | Compare acupuncture and placebo in chronic NP | N = 135 87 females 48 males 53 years | Aged 18 to 80 years; mechanical NP > 2 months; pain score > 30 mm on a Visual Analogue Scale for 5 of 7 days before treatment | Previous neck fracture or surgery; cervical congenital abnormality; uncontrolled low back pain; contraindication to acetaminophen; systemic illness, e.g., rheumatoid arthritis; ongoing litigation or disability claims; current or recent manual neck treatment or steroid use (oral or local injection); or pregnancy |
| Evans et al., 2002 [47] Clinical: 1 Non-Clinical: 3 Citations: 102 | 7/10 | Compare the effects of SM combined with low-tech rehabilitative exercise, MedX rehabilitative exercise, or SM alone in chronic NP | N = 191 113 females 78 males 44 years | Aged 20 to 65 years; mechanical NP > 12 weeks; no specific, identifiable aetiology (i.e., inflammatory disease, infection); pain reproduced by neck movement or provocation tests and localized between the most inferior part of the occipital bone and T1 spinous process | NP referred from peripheral joints or viscera; progressive neurologic deficits; severe osteopenia; vascular disease of the neck or upper extremity; significant infectious disease or other severe disabling health conditions; previous neck surgery; inability to work because of NP; current or pending litigation, SM or exercise therapy within 3 months; concurrent treatment for NP by other health care providers |
| Manchikanti et al., 2010 [38] Clinical: 3 Non-Clinical: 1 Citations: 96 | 10/10 | Evaluate the clinical outcomes of therapeutic cervical medial branch blocks with local anesthetic with or without steroids in chronic NP of facet joint origin | N = 120 89 females 31 males 45 years | Function-limiting NP > 6 months; 18 years or older; to provide written informed consent; positive results with controlled diagnostic cervical facet joint nerve blocks (80% pain relief and the ability to perform previously painful movements) | Disc herniation with radicular pain; symptomatic spinal stenosis; neck surgery within 3 months; uncontrolled major depression or psychiatric disorders; heavy opioid usage; acute or uncontrolled medical illness; chronic severe conditions; inability to stay in a prone position; history of adverse reactions to local anesthetics or steroids; or pregnant or lactating women |
| Hoving et al., 2006 [48] Clinical: 0 Non-Clinical: 11 Citations: 92 | 8/10 | Compare the effectiveness of manual therapy, PT and continued care by the GP over a 1 year period | N = 183 111 females 72 males 45 years | Aged 18 to 70 years; pain and/or stiffness in the neck > 2 weeks; nonspecific neck complaints reproducible during active or passive range of motion; willingness to participate | No specific cause for the pain, e.g., systemic disease, fracture, or organic disorders; a history of trauma or additional dominant complaints, such as headache or nonradicular pain; previous neck surgery; manual or physiotherapy in the previous 6 months |
| Chiu et al., 2005 [49] Clinical: 0 Non-clinical: 3 Citations: 86 | 7/10 | Evaluate the efficacy of a neck exercise program in chronic NP | N = 145 100 females 45 males 44 years | Aged 20 to 70 years; NP (of various intensity of pain) > 3 months; able to read Chinese | Previous neck or upper back (T1-T6) injury; inflammatory condition, e.g., rheumatoid arthritis; former neck surgery; a malignancy or congenital spinal abnormality; parallel NP treatment; contraindication for infrared irradiation; neurologic symptoms, e.g., muscle weakness or changes in spinal reflex jerks; other musculoskeletal problems; acute NP with no freedom of movement; training or SM for NP within 6 months; work-related injuries |
| Bronfort et al., 2012 [50] Clinical: 3 Non-clinical: 3 Citations: 81 | 7/10 | Determine the relative efficacy of SM, medication, and home exercise with advice for acute and subacute NP in the short and long term. | N = 272 178 females 94 males 48 years | Aged 18 to 65 years; primary symptom of mechanical, nonspecific NP equivalent to grades I or II of the Bone and Joint Decade 2000–2010 Task Force on NP and Its Associated Disorders classification; NP between 2–12 weeks duration; NP ≥ 3 on a 0 to 10 scale; not seeking additional NP treatment | Cervical spine instability; fracture; NP referred from peripheral joints or viscera; progressive neurologic deficits: cardiac disease requiring medical treatment; blood clotting disorders; diffuse idiopathic hyperostosis; inflammatory or destructive tissue changes of the cervical spine; infectious disease; substance abuse; cervical spine surgery; severe disabling health problems; pending or current litigation; having received any of the study treatments within 3 months; pregnancy or breastfeeding |
| Study Authors’ Institutions Number of Citations | PEDro Score | Aim | Participants | Inclusion Criteria | Exclusion Criteria |
|---|---|---|---|---|---|
| Celenay et al., 2016 [51] Clinical: 0 Non-Clinical: 3 Citations: 13 | 6/10 | Assess the effect of neck stabilization and scapulo-thoracic treatment with and without connective tissue massage in chronic NP | N = 60 39 females 21 males 48 years | Aged 18 to 65 years; NP > 3 months; baseline NDI ≥ 20% | Stenosis; traumatic injury history; previous neck surgery; cancer; hypermobility; inflammatory rheumatologic diseases; severe psychological disorders; exercise or PT intervention in the last 3 months; pregnancy |
| Celenay et al., 2016 [52] Clinical: 0 Non-Clinical: 3 Citations: 8 | 7/10 | Compare the effect of stabilization exercises with or without manual therapy in patients with mechanical chronic NP | N = 102 74 females 28 males 46 years | Aged 18 to 65 years; NP > 3 months, with symptoms provoked by postures, movements, or palpation | Inflammatory rheumatologic diseases, structural deformity, or malignity; previous cervical surgery; spinal stenosis; bilateral upper extremity symptoms; ≥ 2 positive radicular signs of nerve root compression; referred pain > than 7 on a 0-10 VAS in the related dermatome in the upper extremities; capsular pattern of arthritis; severe psychological disorder; pregnancy; any intervention including exercise or PT within 3 months |
| Cerezo et al., 2016 [30] Clinical: 4 Non-Clinical: 4 Citations: 10 | 6/10 | Assess the effect of deep dry needling of myofascial trigger points in chronic nonspecific NP | N = 128 Sex distribution: N/S 50 years | NP (with or without radiation) > 6 months, with no known pathological basis (neurological, trauma); having myofascial pain syndrome | Major trauma; widespread pain; inflammatory, hormonal, or neurological disorders; upper limbs tendinopathy; severe psychiatric illness; inability to speak or write Spanish; use of muscle relaxant, analgesic, antidepressant, or anticoagulant medication in the last week; fibromyalgia; any contraindication to PT (infection, fever, hypothyroidism, wounds, metal allergy, cancer or systemic disease, fear of needles); or pregnancy |
| De Araujo et al., 2018 [34] Clinical: 0 Non-Clinical: 5 Citations: 0 | 8/10 | Assess the effectiveness of the Pilates method in chronic NP | N = 64 14 females 50 males 49 years | Aged 18 to 65 years; non-specific NP according to the Neck Pain Task Force; pain > 3 months; and pain intensity between 3–8 cm on a 0 to 10 cm rating scale | Fibromyalgia; spine trauma, infection or inflammation; NP radiating to the upper limbs; having started or changed physical activity > 2/week within 3 months; visual impairments and no use of glasses; new or changed pain medication, or injections in the last 3 months; neurological diseases; musculoskeletal diseases hindering the practice of Pilates; pregnancy |
| Essex et al., 2017 [37] Clinical: 1 Non-Clinical: 16 Citations: 0 | 4/10 | Assess the cost-effectiveness of usual care vs. acupuncture and usual care vs. Alexander Technique and usual care for chronic NP | N = 517 347 females 170 males 53 years | NP > 3 months; score > 28% on the Northwick Park Neck Pain Questionnaire | Current acupuncture treatment for NP or attended Alexander lessons in the last 2 years; litigation; serious underlying pathology; prior neck surgery; alcohol or drug dependency; involvement in other trial; history of psychosis, rheumatoid arthritis, osteoporosis, hemophilia, ankylosing spondylitis, cancer, HIV or hepatitis; inability to speak English; pregnancy |
| Fernández-Carnero et al., 2018 [35] Clinical: 3 Non-Clinical: 2 Citations: 0 | 8/10 | Assess the immediate effect of neural tension technique in chronic NP | N = 54 41 females 13 males 21 years | Aged 18 to 65 years; NP within the nuchal line and T1 spinous process > 12 weeks; no radicular symptoms to head, trunk, or upper limbs; ability to write and speak Spanish | Systemic or degenerative diseases; headache and/or low back pain within 9 months; NP linked with whiplash; moderate or severe depression; red flags (metabolic diseases, tumor, fracture, rheumatoid arthritis, osteoporosis); fibromyalgia; neck surgery; cervical radiculopathy; disc herniation; neck or face pain within 6 months; NP with vertigo caused by vertebrobasilar insufficiency; non-cervicogenic headache after trauma within last year |
| Griswold et al., 2018 [53] Clinical: 1 Non-Clinical: 4 Citations: 0 | 7/10 | Compare the effect of concordant cervical and thoracic non-thrust vs. thrust SM for chronic mechanical NP | N = 103 76 females 27 males 47 years | Aged 18 to 70 years; having mechanical NP; NDI ≥ 20%; and NP > 2 on a 0 to 10 rating scale in the last 24 h | Contraindications to manual therapy (fracture, malignancy, rheumatoid arthritis, myelopathy, osteoporosis); prior cervical or thoracic spine surgery; seeking litigation; nerve root compression (at least 2 or more neurological signs); receiving other nonsurgical care; inability to reproduce the concordant sign in the cervical or thoracic spine during testing |
| Krøll et al., 2018 [54] Clinical: 4 Non-Clinical: 1 Citations: 1 | 5/10 | Evaluate the efficacy of aerobic exercise in migraine and coexisting tension-type headache and chronic NP | N = 70 62 females 8 males 37 years | A minimum of 2 attacks of migraine; a minimum of 1 day with tension-type headache; a minimum of 1 day with NP per month | Whiplash; significant neck trauma, (fracture, distortion, or violent attack); neck nerve root compression; persistent headache linked with trauma; medication overuse; severe physical and/or mental illness; trigeminal neuralgia; cluster headache; alcohol and drugs abuse; breastfeeding; inability to speak Danish; pregnancy |
| Lauche et al., 2016 [55] Clinical: 1 Non-Clinical: 8 Citations: 7 | 7/10 | Evaluate the efficacy of Tai Chi for treating chronic NP | N = 114 91 females 23 males 49 years | Age > 18 years; nonspecific NP > 3 consecutive months for at least 5 days a week; NP > 45 mm on a 0 to 100 mm VAS | NP caused by trauma, disc protrusion, whiplash, spinal deformity, stenosis, neoplasm, neurological disorder, rheumatic or active severe affective disorder, addiction, psychosis, or oncologic disease; invasive spinal treatment within 4 weeks; spinal surgery in the last year; new or modified drug regimen; opioids intake; regular practice of Tai Chi, Qigong, or Yoga within 6 months; any disability precluding exercise; pregnancy |
| Lauche et al., 2016 [56] Clinical: 3 Non-Clinical: 5 Citations: 3 | 6/10 | Assess the efficacy of the Alexander Technique, local heat and guided imagery in patients with chronic non-specific NP | N = 72 65 females 7 males 41 years | Aged 18 to 50 years; non-specific NP > 3 months; NP intensity > 40 mm on a 100 mm VAS | NP caused by disc protrusion or prolapse; spinal congenital deformity; spinal stenosis; whiplash; neoplasm, inflammatory rheumatic disease; neurological disorder; active oncologic disease; affective disorder; addiction; psychosis; previous spinal surgery or invasive spinal treatment within 3 weeks; ongoing application for disability pension; previous Alexander technique experience; participation in other clinical trials; pregnancy |
| Monticone et al., 2017 [57] Clinical: 6 Non-Clinical: 1 Citations: 3 | 8/10 | Evaluate the effect of a group based multidisciplinary rehabilitation programme in chronic NP | N = 170 121 females 49 males 53 years | Age >18 years; documented history of non-specific NP >3 months; a good understanding of Italian | Acute and subacute NP; cognitive impairment; clear aetiology for their NP, e.g., previous spinal surgery, deformity, disc herniation, infection, fracture, myelopathy or malignancy, whiplash, and systemic or neuromuscular diseases; having received cognitive-behavioral therapy |
| Pillastrini et al., 2016 [58] Clinical: 1 Non-Clinical: 7 Citations: 6 | 8/10 | Evaluate the effectiveness of global postural reeducation vs. manual therapy in chronic NP | N = 96 72 females 22 males 48 years | Nonspecific NP > 3 months; aged 18 to 80 years; ability to read and speak Italian | Acute or subacute NP; specific cause of NP, e.g., systemic, rheumatic, neuromuscular diseases; central or peripheral neurological signs; cognitive impairment, spinal surgery; or PT treatments in the prior 6 months |
| Ris et al., 2016 [59] Clinical: 1 Non-Clinical: 5 Citations: 7 | 6/10 | Assess the effect of pain education, exercises and graded physical activity vs. pain education alone in chronic NP | N = 200 149 females 51 males 45 years | Aged >18 years; traumatic or non-traumatic NP > half a year; NDI >10; NP, primary pain; complete medical diagnostic procedures | Clinically confirmed radiculopathies; progressive medical treatment; unstable social/working conditions; current fractures; score > 29 in the Beck Depression Inventory-II; conditions limiting participation; pregnancy |
| Thompson et al., 2016 [33] Clinical: 2 Non-Clinical: 1 Citations: 4 | 5/10 | Evaluate the effect of physiotherapist led cognitive—behavioral intervention plus exercise in chronic NP | N = 57 27 females 28 males 48 years | Non-specific NP > 3 months; fluency in English; have not received PT for NP in the past 3 months | Serious pathology (fracture, dislocation, carcinoma or infection); radiculopathy; myelopathy; rheumatological disorder; diagnosed major psychiatric illness |
| Tunwattanapong et al., 2016 [60] Clinical: 1 Non-clinical: 2 Citations: 10 | 8/10 | Determine the effect of neck and shoulder stretching exercises for chronic NP among office workers | N = 96 87 females 9 males 35 years | Office workers who rated themselves with moderate to severe neck or shoulder pain (VAS ≥ 5 of 10 cm) for more than 3 months | Performing regular stretching exercise; a history of severe neck injury, or neck or shoulder contracture (defined by a limitation range of motion in all directions); previous neck or shoulder surgery; abnormal neurological signs |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oliva-Pascual-Vaca, Á.; González-González, C.; Oliva-Pascual-Vaca, J.; Piña-Pozo, F.; Ferragut-Garcías, A.; Fernández-Domínguez, J.C.; Heredia-Rizo, A.M. Visceral Origin: An Underestimated Source of Neck Pain. A Systematic Scoping Review. Diagnostics 2019, 9, 186. https://doi.org/10.3390/diagnostics9040186
Oliva-Pascual-Vaca Á, González-González C, Oliva-Pascual-Vaca J, Piña-Pozo F, Ferragut-Garcías A, Fernández-Domínguez JC, Heredia-Rizo AM. Visceral Origin: An Underestimated Source of Neck Pain. A Systematic Scoping Review. Diagnostics. 2019; 9(4):186. https://doi.org/10.3390/diagnostics9040186
Chicago/Turabian StyleOliva-Pascual-Vaca, Ángel, Carlos González-González, Jesús Oliva-Pascual-Vaca, Fernando Piña-Pozo, Alejandro Ferragut-Garcías, Juan Carlos Fernández-Domínguez, and Alberto Marcos Heredia-Rizo. 2019. "Visceral Origin: An Underestimated Source of Neck Pain. A Systematic Scoping Review" Diagnostics 9, no. 4: 186. https://doi.org/10.3390/diagnostics9040186
APA StyleOliva-Pascual-Vaca, Á., González-González, C., Oliva-Pascual-Vaca, J., Piña-Pozo, F., Ferragut-Garcías, A., Fernández-Domínguez, J. C., & Heredia-Rizo, A. M. (2019). Visceral Origin: An Underestimated Source of Neck Pain. A Systematic Scoping Review. Diagnostics, 9(4), 186. https://doi.org/10.3390/diagnostics9040186