

Incidence and Risk Factors of White Matter Lesions in Moderate and Late Preterm Infants

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
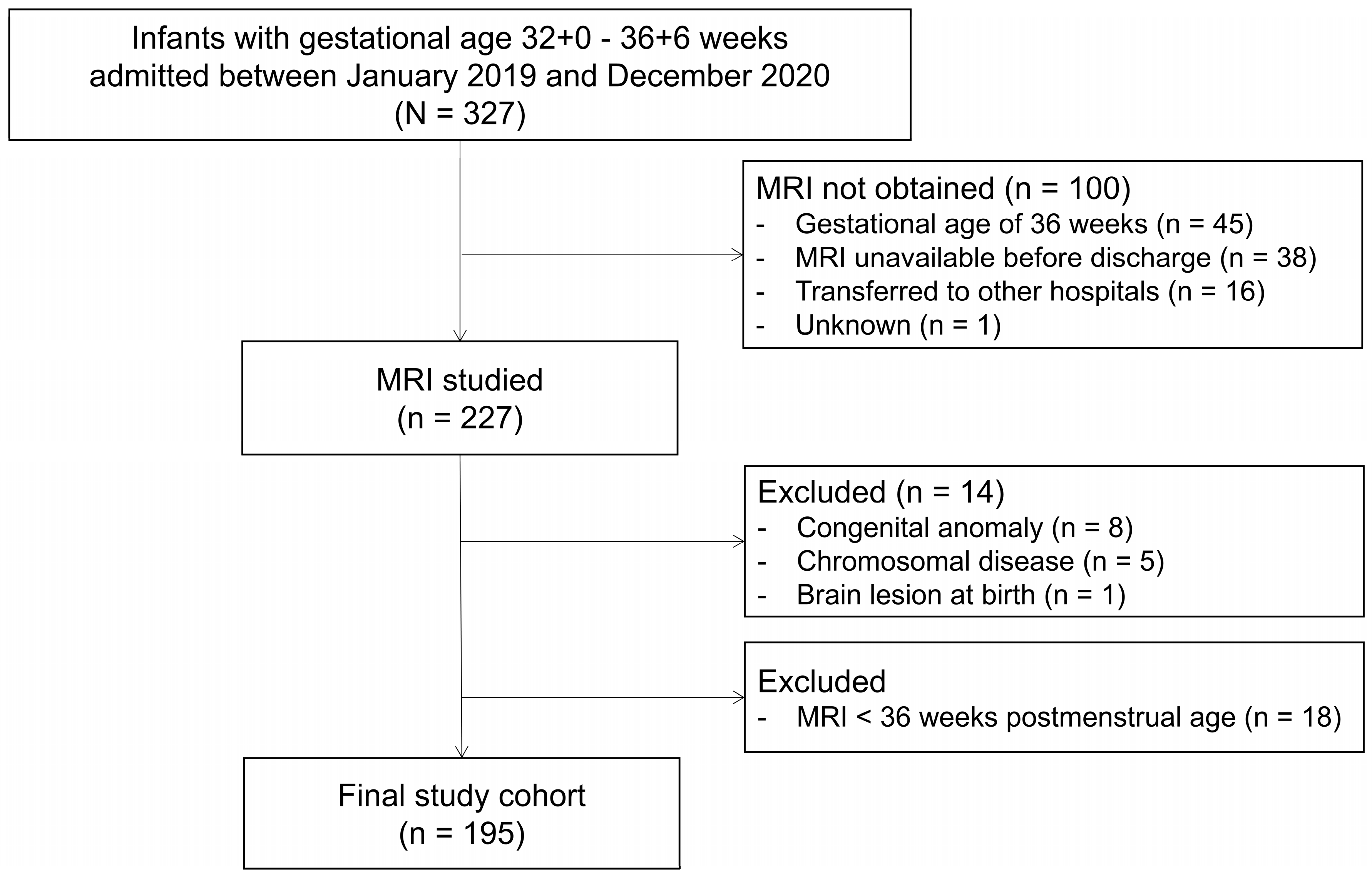
2.1. Study Population
2.2. MRI Acquisition and Assessment
2.3. Collection of Clinical Data
2.4. Data Analysis
3. Results
3.1. Participants
3.2. Incidence of Brain Lesions
3.3. Dependence of White Matter Lesions on Clinical Variables
3.4. Dependence of PWML on Clinical Variables
3.5. Dependence of Grey Matter Lesions on Clinical Variables
3.6. Dependence of Any Brain Lesions on Clinical Variables
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mathur, A.; Inder, T. Magnetic resonance imaging—Insights into brain injury and outcomes in premature infants. J. Commun. Disord. 2009, 42, 248–255. [Google Scholar] [PubMed]
- Pettinger, K.J.; Copper, C.; Boyle, E.; Blower, S.; Hewitt, C.; Fraser, L. Risk of Developmental Disorders in Children Born at 32 to 38 Weeks’ Gestation: A Meta-Analysis. Pediatrics 2023, 152, e2023061878. [Google Scholar] [PubMed]
- Rees, P.; Callan, C.; Chadda, K.R.; Vaal, M.; Diviney, J.; Sabti, S.; Harnden, F.; Gardiner, J.; Battersby, C.; Gale, C.; et al. Preterm Brain Injury and Neurodevelopmental Outcomes: A Meta-analysis. Pediatrics 2022, 150, e2022057442. [Google Scholar] [PubMed]
- Ng, N.S.; Razak, A.; Chandrasekharan, P.; McLean, G.; Sackett, V.; Zhou, L.; Pharande, P.; Malhotra, A. Early neurodevelopmental outcomes of preterm infants with intraventricular haemorrhage and periventricular leukomalacia. J. Paediatr. Child. Health. 2024, 60, 669–674. [Google Scholar]
- Inder, T.E.; Volpe, J.J.; Anderson, P.J. Defining the Neurologic Consequences of Preterm Birth. N. Engl. J. Med. 2023, 389, 441–453. [Google Scholar]
- Hamrick, S.E.; Miller, S.P.; Leonard, C.; Glidden, D.V.; Goldstein, R.; Ramaswamy, V.; Piecuch, R.; Ferriero, D.M. Trends in severe brain injury and neurodevelopmental outcome in premature newborn infants: The role of cystic periventricular leukomalacia. J. Pediatr. 2004, 145, 593–599. [Google Scholar] [CrossRef]
- Boswinkel, V.; Nijboer-Oosterveld, J.; Nijholt, I.M.; Edens, M.A.; de Tollenaer, S.M.M.; Boomsma, M.F.; de Vries, L.S.; van Wezel-Meijler, G. A systematic review on brain injury and altered brain development in moderate-late preterm infants. Early Hum. Dev. 2020, 148, 105094. [Google Scholar]
- Papile, L.A.; Burstein, J.; Burstein, R.; Koffler, H. Incidence and evolution of subependymal and intraventricular hemorrhage: A study of infants with birth weights less than 1500 gm. J. Pediatr. 1978, 92, 529–534. [Google Scholar]
- Cornette, L.G.; Tanner, S.F.; A Ramenghi, L.; Miall, L.S.; Childs, A.M.; Arthur, R.J.; Martinez, D.; I Levene, M. Magnetic resonance imaging of the infant brain: Anatomical characteristics and clinical significance of punctate lesions. Arch. Dis. Child. Fetal Neonatal Ed. 2002, 86, F171–F177. [Google Scholar]
- Rutherford, M.A.; Supramaniam, V.; Ederies, A.; Chew, A.; Bassi, L.; Groppo, M.; Anjari, M.; Counsell, S.; Ramenghi, L.A. Magnetic resonance imaging of white matter diseases of prematurity. Neuroradiology 2010, 52, 505–521. [Google Scholar]
- Isojima, T.; Kato, N.; Ito, Y.; Kanzaki, S.; Murata, M. Growth standard charts for Japanese children with mean and standard deviation (SD) values based on the year 2000 national survey. Clin Pediatr Endocrinol. 2016, 25, 71–76. [Google Scholar] [PubMed]
- Wagenaar, N.; Chau, V.; Groenendaal, F.; Kersbergen, K.J.; Poskitt, K.J.; Grunau, R.E.; Synnes, A.; Duerden, E.G.; de Vries, L.S.; Miller, S.P.; et al. Clinical Risk Factors for Punctate White Matter Lesions on Early Magnetic Resonance Imaging in Preterm Newborns. J. Pediatr. 2017, 182, 34–40.e1. [Google Scholar] [PubMed]
- van Haastert, I.C.; de Vries, L.S.; Eijsermans, M.J.; Jongmans, M.J.; Helders, P.J.; Gorter, J.W. Gross motor functional abilities in preterm-born children with cerebral palsy due to periventricular leukomalacia. Dev. Med. Child. Neurol. 2008, 50, 684–689. [Google Scholar]
- van Haastert, I.C.; Groenendaal, F.; Uiterwaal, C.S.P.; Termote, J.U.; van der Heide-Jalving, M.; Eijsermans, M.J.; Gorter, J.W.; Helders, P.J.; Jongmans, M.J.; de Vries, L.S. Decreasing incidence and severity of cerebral palsy in prematurely born children. J. Pediatr. 2011, 159, 86–91.e1. [Google Scholar]
- Miller, S.P.; Cozzio, C.C.; Goldstein, R.B.; Ferriero, D.M.; Partridge, J.C.; Vigneron, D.B.; Barkovich, A.J. Comparing the diagnosis of white matter injury in premature newborns with serial MR imaging and transfontanel ultrasonography findings. AJNR Am. J. Neuroradiol. 2003, 24, 1661–1669. [Google Scholar]
- Parodi, A.; Malova, M.; Cardiello, V.; Raffa, S.; Re, M.; Calevo, M.G.; Severino, M.; Tortora, D.; Morana, G.; Rossi, A.; et al. Punctate white matter lesions of preterm infants: Risk factor analysis. Eur. J. Paediatr. Neurol. 2019, 23, 733–739. [Google Scholar]
- Leijser, L.M.; de Bruine, F.T.; Steggerda, S.J.; van der Grond, J.; Walther, F.J.; van Wezel-Meijler, G. Brain imaging findings in very preterm infants throughout the neonatal period: Part I. Incidences and evolution of lesions, comparison between ultrasound and MRI. Early Hum. Dev. 2009, 85, 101–109. [Google Scholar]
- Boswinkel, V.; Kruse-Ruijter, M.F.; Nijboer-Oosterveld, J.; Nijholt, I.M.; Edens, M.A.; Mulder-de Tollenaer, S.M.; Smit-Wu, M.N.; Boomsma, M.F.; de Vries, L.S.; van Wezel-Meijler, G.; et al. Incidence of brain lesions in moderate-late preterm infants assessed by cranial ultrasound and MRI: The BIMP-study. Eur. J. Radiol. 2021, 136, 109500. [Google Scholar]
- Okumura, A.; Hayakawa, F.; Kato, T.; Itomi, K.; Maruyama, K.; Ishihara, N.; Kubota, T.; Suzuki, M.; Sato, Y.; Kuno, K.; et al. Hypocarbia in preterm infants with periventricular leukomalacia: The relation between hypocarbia and mechanical ventilation. Pediatrics 2001, 107, 469–475. [Google Scholar]
- Braithwaite, E.C.; Hill, J.; Pickles, A.; Glover, V.; O’Donnell, K.; Sharp, H. Associations between maternal prenatal cortisol and fetal growth are specific to infant sex: Findings from the Wirral Child Health and Development Study. J. Dev. Orig. Health Dis. 2018, 9, 425–431. [Google Scholar]
- Motavaf, M.; Piao, X. Oligodendrocyte Development and Implication in Perinatal White Matter Injury. Front. Cell Neurosci. 2021, 15, 764486. [Google Scholar] [CrossRef] [PubMed]
- Yokoi, K.; Iwata, O.; Kobayashi, S.; Jinnou, H.; Kato, S.; Saitoh, S.; Goto, H. Intrauterine Inflammation, Excessive Fetal Growth and Respiratory Morbidities in Moderate-To-Late Preterm Neonates. Neonatology 2024, 121, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Mortier, I.; Blanc, J.; Tosello, B.; Gire, C.; Bretelle, F.; Carcopino, X. Is gestational diabetes an independent risk factor of neonatal severe respiratory distress syndrome after 34 weeks of gestation? A prospective study. Arch. Gynecol. Obstet. 2017, 296, 1071–1077. [Google Scholar] [CrossRef] [PubMed]
- Glass, H.C.; Bonifacio, S.L.; Chau, V.; Glidden, D.; Poskitt, K.; Barkovich, A.J.; Ferriero, D.M.; Miller, S.P. Recurrent postnatal infections are associated with progressive white matter injury in premature infants. Pediatrics 2008, 122, 299–305. [Google Scholar] [CrossRef]
- Goldenberg, R.L.; Culhane, J.F.; Iams, J.D.; Romero, R. Epidemiology and causes of preterm birth. Lancet 2008, 371, 75–84. [Google Scholar] [CrossRef]
- Johnston, M.V.; Hoon, A.H., Jr. Possible mechanisms in infants for selective basal ganglia damage from asphyxia, kernicterus, or mitochondrial encephalopathies. J. Child. Neurol. 2000, 15, 588–591. [Google Scholar] [CrossRef]

{kind=link}
| Variables | Evaluated (n = 195) | Not Evaluated (n = 100) | p |
|---|---|---|---|
| Maternal and antenatal variables | |||
| Parity (multipara) | 86 (44.1) | 42 (42.0) | 0.730 |
| Multiple pregnancy | 61 (31.3) | 31 (31.0) | 0.961 |
| Caesarean section | 159 (81.5) | 71 (71.0) | 0.039 |
| Premature rupture of the membrane | 11 (5.6) | 2 (2.0) | 0.231 |
| Antenatal steroids | 73 (37.4) | 20 (20.2) | 0.003 |
| Clinical chorioamnionitis | 9 (4.8) | 1 (1.0) | 0.172 |
| Outborn | 9 (4.6) | 9 (9.0) | 0.136 |
| Variables at birth | |||
| Male sex | 97 (49.7) | 59 (59.0) | 0.132 |
| Gestational age (week) | 35.0 (1.2) | 35.7 (0.9) | <0.001 |
| 32 weeks | 11 (5.6) | 1 (1.0) | |
| 33 weeks | 31 (15.9) | 3 (3.0) | |
| 34 weeks | 54 (27.7) | 6 (6.0) | |
| 35 weeks | 47 (24.1) | 45 (45.0) | |
| 36 weeks | 52 (26.7) | 45 (45.0) | |
| Body weight at birth (g) | 2100 (379) | 2379 (348) | <0.001 |
| Body weight z score | −0.50 (1.07) | −0.07 (0.90) | <0.001 |
| Intrauterine growth restriction | 23 (11.8) | 2 (2.0) | 0.004 |
| Apgar score | |||
| 1 min. | 8 [8–8] | 8 [8–8] | 0.008 |
| 5 min. | 9 [8–9] | 9 [8–9] | 0.058 |
| Cord blood | |||
| pH | 7.312 (0.076) | 7.326 (0.038) | 0.021 |
| Base excess (mmol/L) | −2.01 (3.35) | −1.92 (1.52) | 0.291 |
| Need of resuscitation | 94 (48.2) | 41 (41.0) | 0.240 |
| Variables after admission | |||
| Oxygen supplement | 178 (91.3) | 80 (81.6) | 0.016 |
| Non-invasive mechanical ventilation | 148 (75.4) | 51 (51.0) | <0.001 |
| Need for intubation | 99 (50.8) | 46 (46.5) | 0.485 |
| Duration of mechanical ventilation | 1.4 (2.4) | 1.0 (1.4) | 0.070 |
| Any treatment for PDA | 7 (3.6) | 2 (2.0) | 0.723 |
| Inotropes use | 10 (5.1) | 1 (1.0) | 0.065 |
| Transfusion | 10 (5.1) | 0 (0.0) | 0.018 |
| Postnatal steroids | 5 (2.6) | 0 (0.0) | 0.171 |
| MRI scan | |||
| Postmenstrual age at scan (weeks) | 37.5 (1.2) | N/A | |
| Postnatal age at scan (days) | 18.0 (10.7) | N/A |
| Brain Lesions | n = 46 |
|---|---|
| Haemorrhages | |
| IVH | |
| Total | 4 (8.7) |
| Grade I | 3 |
| Grade II | 1 |
| Infarction | 5 (10.9) |
| Deep grey matter | |
| Small focal lesion | 4 (8.7) |
| White matter | |
| Punctate white matter lesions (PWML) | 30 (65.2) |
| <6 PWML | 22 |
| ≥6 PWML | 8 |
| Periventricular leukomalacia | 1 (2.2) |
| Small focal lesion | 3 (6.5) |
| Miscellaneous | |
| Subependymal cyst | 1 (2.2) |
| Cerebellum | 1 (2.2) |
| No Lesion n = 149 | White Matter Lesion n = 34 | OR | 95% CI | p | ||
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Univariate analysis | ||||||
| Maternal and antenatal variables | ||||||
| Vaginal delivery | 21 (14.1) | 11 (32.4) | 2.915 | 1.241 | 6.847 | 0.014 |
| PROM | 10 (6.7) | 1 (2.9) | 0.421 | 0.052 | 3.407 | 0.418 |
| Antenatal steroids | 53 (35.6) | 14 (41.2) | 1.268 | 0.592 | 2.714 | 0.541 |
| Clinical chorioamnionitis | 5 (3.4) | 3 (9.4) | 2.917 | 0.660 | 12.894 | 0.158 |
| Threatened preterm labour | 79 (53.0) | 19 (55.9) | 1.122 | 0.530 | 2.375 | 0.763 |
| Foetal distress | 10 (6.7) | 1 (2.9) | 0.421 | 0.052 | 3.407 | 0.418 |
| Placenta praevia | 6 (4.0) | 0 (0.0) | N/A | N/A | ||
| Hypertensive disorders in pregnancy | 20 (13.4) | 1 (2.9) | 0.195 | 0.025 | 1.510 | 0.118 |
| Variables at birth | ||||||
| Male sex | 68 (45.6) | 22 (64.7) | 2.184 | 1.007 | 4.734 | 0.048 |
| Gestational age (week) | 35.0 (1.3) | 35.1 (1.1) | 1.076 | 0.793 | 1.459 | 0.639 |
| Body weight at birth (per 100g) | 2067 (371) | 2277 (372) | 1.163 | 1.048 | 1.292 | 0.005 |
| Body weight z score | −0.60 (1.10) | −0.06 (0.92) | 1.640 | 1.122 | 2.397 | 0.011 |
| Apgar score | ||||||
| 1 min. | 8 [8–8] | 8 [8–8] | 0.882 | 0.712 | 1.093 | 0.251 |
| 5 min. | 9 [8–9] | 9 [8–9] | 0.710 | 0.526 | 0.958 | 0.025 |
| Cord blood | ||||||
| pH (per 0.1) | 7.318 (0.051) | 7.308 (0.087) | 0.766 | 0.433 | 1.355 | 0.359 |
| Base excess (mmol/L) | −1.7 (2.6) | −2.8 (4.2) | 0.891 | 0.790 | 1.005 | 0.061 |
| Need of resuscitation | 66 (44.3) | 19 (55.9) | 1.593 | 0.752 | 3.373 | 0.224 |
| Need for intubation | 68 (45.6) | 23 (67.6) | 2.491 | 1.133 | 5.474 | 0.023 |
| Duration of intubation | 1.2 (1.8) | 2.4 (3.9) | 1.192 | 1.019 | 1.393 | 0.028 |
| Any treatment for PDA | 7 (4.7) | 0 (0.0) | N/A | N/A | ||
| Inotropes use | 5 (3.4) | 3 (8.8) | 2.787 | 0.633 | 12.281 | 0.176 |
| Transfusion | 7 (4.7) | 3 (8.8) | 1.963 | 0.481 | 8.018 | 0.347 |
| Postnatal steroid | 1 (0.7) | 3 (8.8) | 14.323 | 1.442 | 142.292 | 0.023 |
| MRI scan | ||||||
| Postmenstrual age at scan (weeks) | 37.6 (1.3) | 37.2 (1.1) | 0.716 | 0.477 | 1.074 | 0.107 |
| Postnatal age at scan (days) | 18.5 (10.9) | 14.9 (10.1) | 0.962 | 0.921 | 1.005 | 0.083 |
| Multivariate analysis | ||||||
| Gestational age (week) | 1.184 | 0.855 | 1.639 | 0.309 | ||
| Vaginal delivery | 3.102 | 1.250 | 7.696 | 0.015 | ||
| Body weight at birth (z score) | 1.702 | 1.118 | 2.591 | 0.013 | ||
| Need for intubation | 2.948 | 1.269 | 6.850 | 0.012 | ||
| OR | 95% CI | p | ||
|---|---|---|---|---|
| Lower | Upper | |||
| Univariate analysis | ||||
| Maternal and antenatal variables | ||||
| Vaginal delivery | 3.048 | 1.254 | 7.409 | 0.014 |
| PROM | 2.824 | 1.088 | 7.329 | 0.033 |
| Antenatal steroids | 1.385 | 0.625 | 3.071 | 0.423 |
| Clinical chorioamnionitis | 3.384 | 0.760 | 15.063 | 0.110 |
| Threatened preterm labour | 1.013 | 0.461 | 2.223 | 0.975 |
| Foetal distress | N/A | N/A | ||
| Placenta praevia | N/A | N/A | ||
| Hypertensive disorders in pregnancy | 0.222 | 0.029 | 1.725 | 0.150 |
| Variables at birth | ||||
| Male sex | 2.382 | 1.044 | 5.435 | 0.039 |
| Gestational age (week) | 1.040 | 0.757 | 1.430 | 0.808 |
| Body weight at birth (per 100g) | 1.172 | 1.050 | 1.309 | 0.005 |
| Body weight z score | 1.749 | 1.167 | 2.621 | 0.007 |
| Apgar score | ||||
| 1 min. | 1.056 | 0.482 | 2.314 | 0.892 |
| 5 min. | 0.697 | 0.513 | 0.945 | 0.020 |
| Cord blood | ||||
| pH (per 0.1) | 1.056 | 0.482 | 2.314 | 0.892 |
| Base excess (mmol/L) | 0.910 | 0.784 | 1.057 | 0.217 |
| Need of resuscitation | 1.645 | 0.745 | 3.628 | 0.218 |
| Need for intubation | 2.779 | 1.194 | 6.469 | 0.018 |
| Duration of intubation | 1.191 | 1.015 | 1.396 | 0.032 |
| Any treatment for PDA | N/A | N/A | ||
| Inotropes use | 2.057 | 0.380 | 11.138 | 0.403 |
| Transfusion | 1.449 | 0.286 | 7.343 | 0.654 |
| Postnatal steroid | 10.571 | 0.927 | 120.585 | 0.058 |
| MRI scan | ||||
| Postmenstrual age at scan (weeks) | 0.659 | 0.420 | 1.034 | 0.069 |
| Postnatal age at scan (days) | 0.960 | 0.917 | 1.006 | 0.087 |
| Multivariate analysis | ||||
| Gestational age (week) | 1.160 | 0.827 | 1.628 | 0.390 |
| Body weight at birth (z score) | 1.890 | 1.215 | 2.940 | 0.005 |
| Need for intubation | 3.094 | 1.274 | 7.513 | 0.013 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ueda, K.; Tsuda, K.; Yamada, T.; Kato, S.; Iwata, S.; Saitoh, S.; Iwata, O. Incidence and Risk Factors of White Matter Lesions in Moderate and Late Preterm Infants. Diagnostics 2025, 15, 881. https://doi.org/10.3390/diagnostics15070881
Ueda K, Tsuda K, Yamada T, Kato S, Iwata S, Saitoh S, Iwata O. Incidence and Risk Factors of White Matter Lesions in Moderate and Late Preterm Infants. Diagnostics. 2025; 15(7):881. https://doi.org/10.3390/diagnostics15070881
Chicago/Turabian StyleUeda, Kentaro, Kennosuke Tsuda, Takaharu Yamada, Shin Kato, Sachiko Iwata, Shinji Saitoh, and Osuke Iwata. 2025. "Incidence and Risk Factors of White Matter Lesions in Moderate and Late Preterm Infants" Diagnostics 15, no. 7: 881. https://doi.org/10.3390/diagnostics15070881
APA StyleUeda, K., Tsuda, K., Yamada, T., Kato, S., Iwata, S., Saitoh, S., & Iwata, O. (2025). Incidence and Risk Factors of White Matter Lesions in Moderate and Late Preterm Infants. Diagnostics, 15(7), 881. https://doi.org/10.3390/diagnostics15070881