
Diagnostic Accuracy of Deep Learning Models in Predicting Glioma Molecular Markers: A Systematic Review and Meta-Analysis
 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
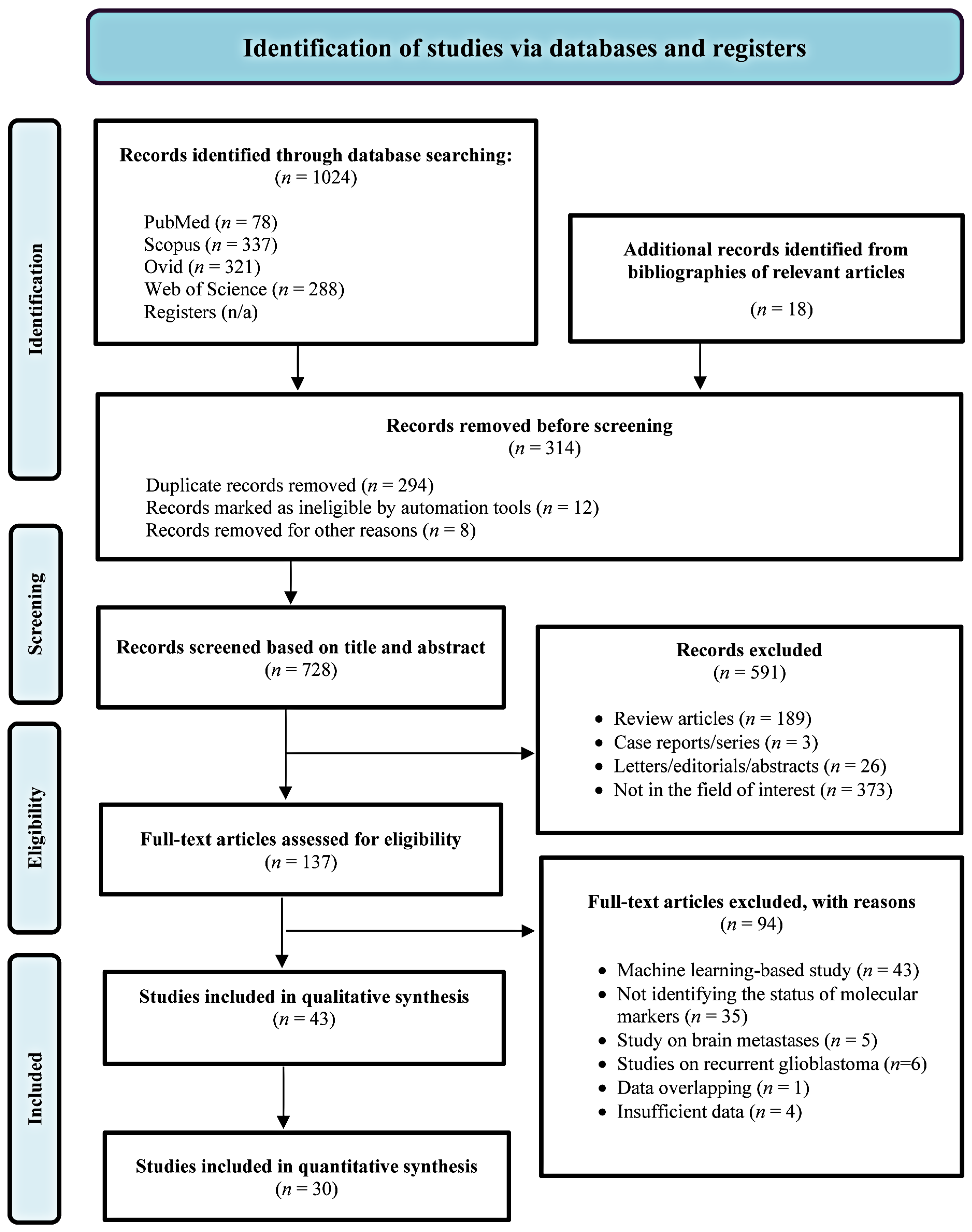
2.1. Search Strategy and Study Selection
2.2. Data Extraction
2.3. Quality Assessment
2.4. Statistical Analysis
3. Results
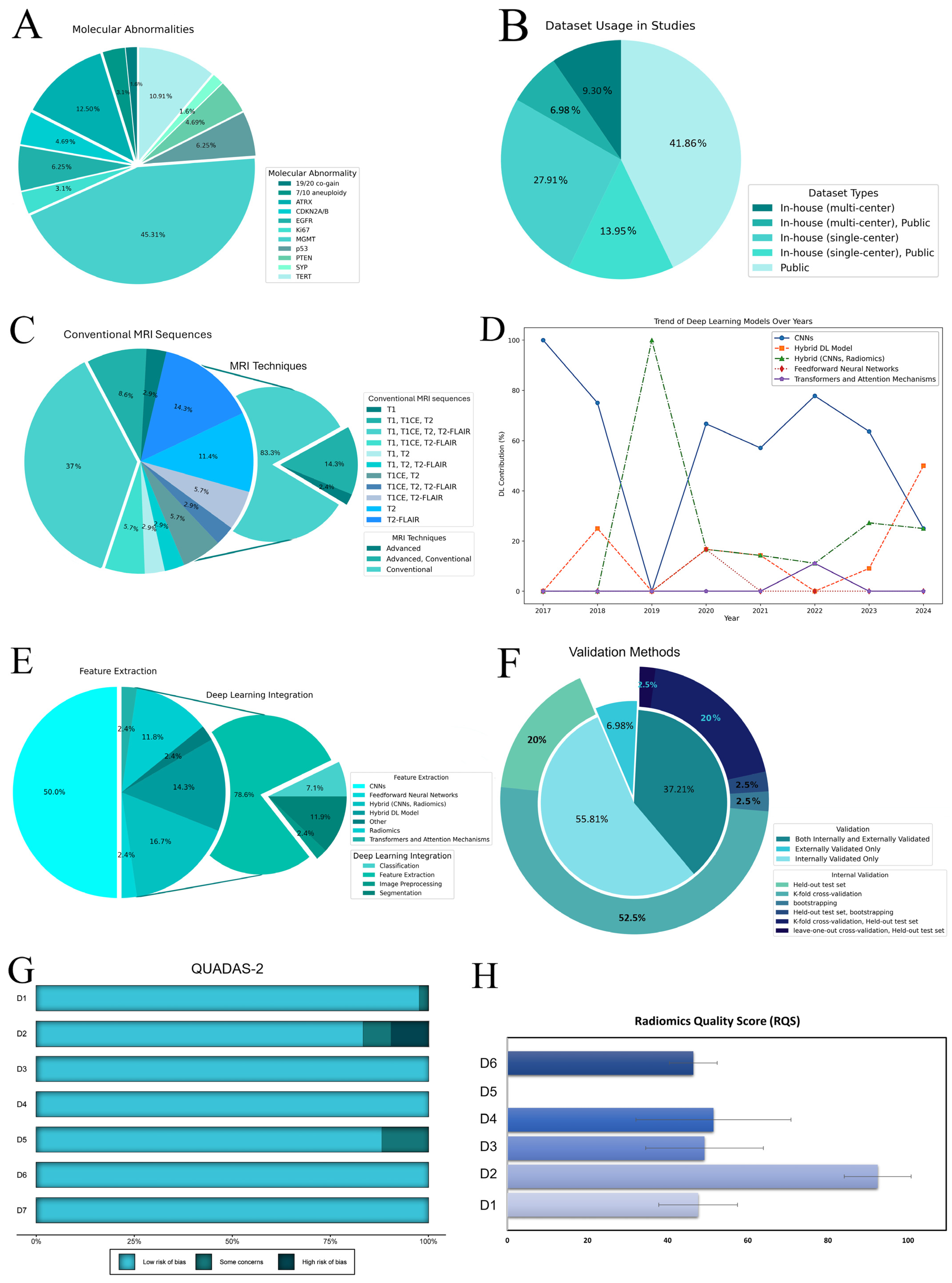
3.1. Study Characteristics
3.2. Quality Assessment
3.3. Publication Bias and Statistical Power
3.4. Sensitivity Analysis
3.5. Prediction of Molecular Marker Status
3.6. Meta-Regression and Subgroup Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| MGMT | O-6-methylguanine-DNA methyltransferase |
| PTEN | Phosphatase and tensin homolog |
| ATRX | alpha-thalassemia/mental retardation syndrome X-linked |
| TERT | telomerase reverse transcriptase |
| CDKN2A/B | cyclin-dependent kinase inhibitor 2A/B |
| EGFR | epidermal growth factor receptor |
| SYP | Synaptophysin |
| QUADAS-2 | Quality assessment of diagnostic accuracy studies-2 |
| RQS | Radiomics quality score |
References
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A Summary. Neuro-Oncology 2021, 23, 1231–1251. [Google Scholar] [CrossRef]
- Perakis, S.; Speicher, M.R. Emerging Concepts in Liquid Biopsies. BMC Med. 2017, 15, 75. [Google Scholar] [CrossRef]
- Guarnera, A.; Romano, A.; Moltoni, G.; Ius, T.; Palizzi, S.; Romano, A.; Bagatto, D.; Minniti, G.; Bozzao, A. The Role of Advanced MRI Sequences in the Diagnosis and Follow-Up of Adult Brainstem Gliomas: A Neuroradiological Review. Tomography 2023, 9, 1526–1537. [Google Scholar] [CrossRef]
- Wei, R.-L.; Wei, X.-T. Advanced Diagnosis of Glioma by Using Emerging Magnetic Resonance Sequences. Front. Oncol. 2021, 11, 694498. [Google Scholar] [CrossRef]
- Liu, Z.; Duan, T.; Zhang, Y.; Weng, S.; Xu, H.; Ren, Y.; Zhang, Z.; Han, X. Radiogenomics: A Key Component of Precision Cancer Medicine. Br. J. Cancer 2023, 129, 741–753. [Google Scholar] [CrossRef] [PubMed]
- Scalco, E.; Rizzo, G.; Mastropietro, A. The Stability of Oncologic MRI Radiomic Features and the Potential Role of Deep Learning: A Review. Phys. Med. Biol. 2022, 67, 09TR03. [Google Scholar] [CrossRef]
- Hosny, A.; Aerts, H.J.; Mak, R.H. Handcrafted versus Deep Learning Radiomics for Prediction of Cancer Therapy Response. Lancet Digit. Health 2019, 1, e106–e107. [Google Scholar] [CrossRef]
- Farahani, S.; Hejazi, M.; Tabassum, M.; Ieva, A.D.; Mahdavifar, N.; Liu, S. Diagnostic Performance of Deep Learning for Predicting Gliomas’ IDH and 1p/19q Status in MRI: A Systematic Review and Meta-Analysis. arXiv 2024, arXiv:2411.02426. [Google Scholar]
- Brat, D.J.; Aldape, K.; Bridge, J.A.; Canoll, P.; Colman, H.; Hameed, M.R.; Harris, B.T.; Hattab, E.M.; Huse, J.T.; Jenkins, R.B.; et al. Molecular Biomarker Testing for the Diagnosis of Diffuse Gliomas: Guideline From the College of American Pathologists in Collaboration With the American Association of Neuropathologists, Association for Molecular Pathology, and Society for Neuro-Oncology. Arch. Pathol. Lab. Med. 2022, 146, 547–574. [Google Scholar] [CrossRef]
- Huang, H.; Wang, F.; Luo, S.; Chen, G.; Tang, G. Diagnostic Performance of Radiomics Using Machine Learning Algorithms to Predict MGMT Promoter Methylation Status in Glioma Patients: A Meta-Analysis. Diagn. Interv. Radiol. 2021, 27, 716. [Google Scholar] [CrossRef]
- Samartha, M.V.S.; Dubey, N.K.; Jena, B.; Maheswar, G.; Lo, W.-C.; Saxena, S. AI-Driven Estimation of O6 Methylguanine-DNA-Methyltransferase (MGMT) Promoter Methylation in Glioblastoma Patients: A Systematic Review with Bias Analysis. J. Cancer Res. Clin. Oncol. 2023, 150, 57. [Google Scholar] [CrossRef] [PubMed]
- Doniselli, F.M.; Pascuzzo, R.; Mazzi, F.; Padelli, F.; Moscatelli, M.; Akinci D’Antonoli, T.; Cuocolo, R.; Aquino, D.; Cuccarini, V.; Sconfienza, L.M. Quality Assessment of the MRI-Radiomics Studies for MGMT Promoter Methylation Prediction in Glioma: A Systematic Review and Meta-Analysis. Eur. Radiol. 2024, 34, 5802–5815. [Google Scholar] [CrossRef] [PubMed]
- Robinet, L.; Siegfried, A.; Roques, M.; Berjaoui, A.; Cohen-Jonathan Moyal, E. MRI-Based Deep Learning Tools for MGMT Promoter Methylation Detection: A Thorough Evaluation. Cancers 2023, 15, 2253. [Google Scholar] [CrossRef] [PubMed]
- van Kempen, E.J.; Post, M.; Mannil, M.; Kusters, B.; ter Laan, M.; Meijer, F.J.A.; Henssen, D.J.H.A. Accuracy of Machine Learning Algorithms for the Classification of Molecular Features of Gliomas on MRI: A Systematic Literature Review and Meta-Analysis. Cancers 2021, 13, 2606. [Google Scholar] [CrossRef]
- Lasocki, A.; Abdalla, G.; Chow, G.; Thust, S.C. Imaging Features Associated with H3 K27-Altered and H3 G34-Mutant Gliomas: A Narrative Systematic Review. Cancer Imaging 2022, 22, 63. [Google Scholar] [CrossRef]
- Jian, A.; Jang, K.; Manuguerra, M.; Liu, S.; Magnussen, J.; Di Ieva, A. Machine Learning for the Prediction of Molecular Markers in Glioma on Magnetic Resonance Imaging: A Systematic Review and Meta-Analysis. Neurosurgery 2021, 89, 31–44. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Moher, D. Updating Guidance for Reporting Systematic Reviews: Development of the PRISMA 2020 Statement. J. Clin. Epidemiol. 2021, 134, 103–112. [Google Scholar] [CrossRef]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M.M. the QUADAS-2 Group QUADAS-2: A Revised Tool for the Quality Assessment of Diagnostic Accuracy Studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Lambin, P.; Leijenaar, R.T.H.; Deist, T.M.; Peerlings, J.; de Jong, E.E.C.; van Timmeren, J.; Sanduleanu, S.; Larue, R.T.H.M.; Even, A.J.G.; Jochems, A.; et al. Radiomics: The Bridge between Medical Imaging and Personalized Medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef]
- Borenstein, M. Common Mistakes in Meta-Analysis and How to Avoid Them; Biostat, Incorporated: Englewood, NJ, USA, 2019; ISBN 978-1-7334367-1-7. [Google Scholar]
- Lee, J.; Kim, K.W.; Choi, S.H.; Huh, J.; Park, S.H. Systematic Review and Meta-Analysis of Studies Evaluating Diagnostic Test Accuracy: A Practical Review for Clinical Researchers-Part II. Statistical Methods of Meta-Analysis. Korean J. Radiol. 2015, 16, 1188–1196. [Google Scholar] [CrossRef]
- Deeks, J.J.; Higgins, J.P.; Altman, D.G.; Cochrane Statistical Methods Group. Analysing Data and Undertaking Meta-Analyses. In Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019; pp. 241–284. ISBN 978-1-119-53660-4. [Google Scholar]
- Quintana, D. A Guide for Calculating Study-Level Statistical Power for Meta-Analyses. Adv. Methods Pract. Psychol. Sci. 2023, 6, 25152459221147260. [Google Scholar]
- Cerullo, E.; Sutton, A.J.; Jones, H.E.; Wu, O.; Quinn, T.J.; Cooper, N.J. MetaBayesDTA: Codeless Bayesian Meta-Analysis of Test Accuracy, with or without a Gold Standard. BMC Med. Res. Methodol. 2023, 23, 127. [Google Scholar] [CrossRef]
- Chen, X.; Zhang, R.; Zhou, Y.; Liu, S.; Wang, Z.; Zhang, S.; Chen, Z. Multi-Sequence MRI-Based Convolutional Neural Network Predicts the Methylation Status of MGMT Promoter in Glioma. Chin. J. Magn. Reson. Imaging 2023, 14, 34–39, 78. [Google Scholar]
- Tang, Z.; Xu, Y.; Jin, L.; Aibaidula, A.; Lu, J.; Jiao, Z.; Wu, J.; Zhang, H.; Shen, D. Deep Learning of Imaging Phenotype and Genotype for Predicting Overall Survival Time of Glioblastoma Patients. IEEE Trans. Med. Imaging 2020, 39, 2100–2109. [Google Scholar] [CrossRef] [PubMed]
- Calabrese, E.; Villanueva-Meyer, J.E.; Cha, S. A Fully Automated Artificial Intelligence Method for Non-Invasive, Imaging-Based Identification of Genetic Alterations in Glioblastomas. Sci. Rep. 2020, 10, 11852. [Google Scholar] [CrossRef]
- Haubold, J.; Hosch, R.; Parmar, V.; Glas, M.; Guberina, N.; Catalano, O.A.; Pierscianek, D.; Wrede, K.; Deuschl, C.; Forsting, M.; et al. Fully Automated MR Based Virtual Biopsy of Cerebral Gliomas. Cancers 2021, 13, 6186. [Google Scholar] [CrossRef] [PubMed]
- Sohn, B.; An, C.; Kim, D.; Ahn, S.S.; Han, K.; Kim, S.H.; Kang, S.-G.; Chang, J.H.; Lee, S.-K. Radiomics-Based Prediction of Multiple Gene Alteration Incorporating Mutual Genetic Information in Glioblastoma and Grade 4 Astrocytoma, IDH-Mutant. J. Neuro-Oncol. 2021, 155, 267–276. [Google Scholar] [CrossRef]
- Calabrese, E.; Rudie, J.D.; Rauschecker, A.M.; Villanueva-Meyer, J.E.; Clarke, J.L.; Solomon, D.A.; Cha, S. Combining Radiomics and Deep Convolutional Neural Network Features from Preoperative MRI for Predicting Clinically Relevant Genetic Biomarkers in Glioblastoma. Neuro-Oncol. Adv. 2022, 4, vdac060. [Google Scholar] [CrossRef]
- Xu, Q.; Xu, Q.Q.; Shi, N.; Dong, L.N.; Zhu, H.; Xu, K. A Multitask Classification Framework Based on Vision Transformer for Predicting Molecular Expressions of Glioma. Eur. J. Radiol. 2022, 157, 110560. [Google Scholar] [CrossRef]
- Chaddad, A.; Hassan, L.; Katib, Y. A Texture-Based Method for Predicting Molecular Markers and Survival Outcome in Lower Grade Glioma. Appl. Intell. 2023, 53, 24724–24738. [Google Scholar] [CrossRef]
- Korfiatis, P.; Kline, T.L.; Lachance, D.H.; Parney, I.F.; Buckner, J.C.; Erickson, B.J. Residual Deep Convolutional Neural Network Predicts MGMT Methylation Status. J. Digit. Imaging 2017, 30, 622–628. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.-C.; Bai, H.; Sun, Q.; Li, Q.; Liu, L.; Zou, Y.; Chen, Y.; Liang, C.; Zheng, H. Multiregional Radiomics Features from Multiparametric MRI for Prediction of MGMT Methylation Status in Glioblastoma Multiforme: A Multicentre Study. Eur. Radiol. 2018, 28, 3640–3650. [Google Scholar] [CrossRef] [PubMed]
- Chang, P.; Grinband, J.; Weinberg, B.D.; Bardis, M.; Khy, M.; Cadena, G.; Su, M.-Y.; Cha, S.; Filippi, C.G.; Bota, D.; et al. Deep-Learning Convolutional Neural Networks Accurately Classify Genetic Mutations in Gliomas. Am. J. Neuroradiol. 2018, 39, 1201–1207. [Google Scholar] [CrossRef] [PubMed]
- Han, L.; Kamdar, M.R. MRI to MGMT: Predicting Methylation Status in Glioblastoma Patients Using Convolutional Recurrent Neural Networks. In Proceedings of the Pacific Symposium on Biocomputing 2018 (PSB), The Big Island of Hawaii, HI, USA, 3–7 January 2018; Altman, R.B., Dunker, A.K., Hunter, L., Ritchie, M.D., Murray, T., Klein, T.E., Eds.; World Scientific Publ Co Pte Ltd.: Singapore, 2018; pp. 331–342. [Google Scholar]
- Korfiatis, P.; Kline, T.L.; Erickson, B.J. Evaluation of a Deep Learning Architecture for MR Imaging Prediction of ATRX in Glioma Patients. In Proceedings of the Medical Imaging 2018: Computer-Aided Diagnosis, Houston, TX, USA, 10–15 February 2018; Petrick, N., Mori, K., Eds.; Spie-Int Soc Optical Engineering: Bellingham, WA, USA, 2018; Volume 10575, p. UNSP 105752G. [Google Scholar]
- Fukuma, R.; Yanagisawa, T.; Kinoshita, M.; Shinozaki, T.; Arita, H.; Kawaguchi, A.; Takahashi, M.; Narita, Y.; Terakawa, Y.; Tsuyuguchi, N.; et al. Prediction of IDH and TERT Promoter Mutations in Low-Grade Glioma from Magnetic Resonance Images Using a Convolutional Neural Network. Sci. Rep. 2019, 9, 20311. [Google Scholar] [CrossRef]
- Crisi, G.; Filice, S. Predicting MGMT Promoter Methylation of Glioblastoma from Dynamic Susceptibility Contrast Perfusion: A Radiomic Approach. J. Neuroimaging 2020, 30, 458–462. [Google Scholar] [CrossRef]
- Hedyehzadeh, M.; Maghooli, K.; MomenGharibvand, M.; Pistorius, S. A Comparison of the Efficiency of Using a Deep CNN Approach with Other Common Regression Methods for the Prediction of EGFR Expression in Glioblastoma Patients. J. Digit. Imaging 2020, 33, 391–398. [Google Scholar] [CrossRef]
- Chen, X.; Zeng, M.; Tong, Y.; Zhang, T.; Fu, Y.; Li, H.; Zhang, Z.; Cheng, Z.; Xu, X.; Yang, R.; et al. Automatic Prediction of MGMT Status in Glioblastoma via Deep Learning-Based MR Image Analysis. BioMed Res. Int. 2020, 2020, 9258649. [Google Scholar] [CrossRef]
- Jonnalagedda, P.; Weinberg, B.; Allen, J.; Bhanu, B. Feature Disentanglement to Aid Imaging Biomarker Characterization for Genetic Mutations. In Proceedings of the Third Conference on Medical Imaging with Deep Learning, Montreal, QC, Canada, 6–8 July 2020; ML Research Press: Seattle, WA, USA, 2020; Volume 121, pp. 349–364. [Google Scholar]
- Yogananda, C.G.B.; Shah, B.R.; Nalawade, S.S.; Murugesan, G.K.; Yu, F.F.; Pinho, M.C.; Wagner, B.C.; Mickey, B.; Patel, T.R.; Fei, B.; et al. MRI-Based Deep-Learning Method for Determining Glioma MGMT Promoter Methylation Status. Am. J. Neuroradiol. 2021, 42, 845–852. [Google Scholar] [CrossRef]
- Tupe-Waghmare, P.; Malpure, P.; Kotecha, K.; Beniwal, M.; Santosh, V.; Saini, J.; Ingalhalikar, M. Comprehensive Genomic Subtyping of Glioma Using Semi-Supervised Multi-Task Deep Learning on Multimodal MRI. IEEE Access 2021, 9, 167900–167910. [Google Scholar] [CrossRef]
- Chen, H.; Lin, F.; Zhang, J.; Lv, X.; Zhou, J.; Li, Z.-C.; Chen, Y. Deep Learning Radiomics to Predict PTEN Mutation Status From Magnetic Resonance Imaging in Patients With Glioma. Front. Oncol. 2021, 11, 734433. [Google Scholar] [CrossRef]
- Lang, D.M.; Peeken, J.C.; Combs, S.E.; Wilkens, J.J.; Bartzsch, S. A Video Data Based Transfer Learning Approach for Classification of MGMT Status in Brain Tumor MR Images. In Proceedings of the Brainlesion: Glioma, Multiple Sclerosis, Stroke and Traumatic Brain Injuries, Brainles 2021, PT I, Virtual Event, 27 September 2021; Crimi, A., Bakas, S., Eds.; Springer International Publishing AG: Cham, Switzerland, 2022; Volume 12962, pp. 306–314. [Google Scholar]
- Xiao, Z.; Yao, S.; Wang, Z.; Zhu, D.; Bie, Y.; Zhang, S.; Chen, W. Multiparametric MRI Features Predict the SYP Gene Expression in Low-Grade Glioma Patients: A Machine Learning-Based Radiomics Analysis. Front. Oncol. 2021, 11, 663451. [Google Scholar] [CrossRef]
- Capuozzo, S.; Gravina, M.; Gatta, G.; Marrone, S.; Sansone, C. A Multimodal Knowledge-Based Deep Learning Approach for MGMT Promoter Methylation Identification. J. Imaging 2022, 8, 321. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Xu, Y.; Ye, M.; Li, Y.; Sun, Y.; Liang, J.; Lu, J.; Wang, Z.; Zhu, Z.; Zhang, X.; et al. Predicting MGMT Promoter Methylation in Diffuse Gliomas Using Deep Learning with Radiomics. J. Clin. Med. 2022, 11, 3445. [Google Scholar] [CrossRef]
- Farzana, W.; Temtam, A.G.; Shboul, Z.A.; Rahman, M.M.; Sadique, M.S.; Iftekharuddin, K.M. Radiogenomic Prediction of MGMT Using Deep Learning with Bayesian Optimized Hyperparameters. In Proceedings of the Brainlesion: Glioma, Multiple Sclerosis, Stroke and Traumatic Brain Injuries, Brainles 2021, PT II, Virtual Event, 27 September 2021; Crimi, A., Bakas, S., Eds.; Springer International Publishing AG: Cham, Switzerland, 2022; Volume 12963, pp. 357–366. [Google Scholar]
- Kim, B.-H.; Lee, H.; Choi, K.S.; Nam, J.G.; Park, C.-K.; Park, S.-H.; Chung, J.W.; Choi, S.H. Validation of MRI-Based Models to Predict MGMT Promoter Methylation in Gliomas: BraTS 2021 Radiogenomics Challenge. Cancers 2022, 14, 4827. [Google Scholar] [CrossRef] [PubMed]
- Nalawade, S.S.; Yu, F.F.; Bangalore Yogananda, C.G.; Murugesan, G.K.; Shah, B.R.; Pinho, M.C.; Wagner, B.C.; Xi, Y.; Mickey, B.; Patel, T.R.; et al. Brain Tumor IDH, 1p/19q, and MGMT Molecular Classification Using MRI-Based Deep Learning: An Initial Study on the Effect of Motion and Motion Correction. J. Med. Imaging 2022, 9, 016001. [Google Scholar] [CrossRef] [PubMed]
- Spoorthy, K.R.; Mahdev, A.R.; Vaishnav, B.; Shruthi, M.L. Deep Learning Approach for Radiogenomic Classification of Brain Tumor. In Proceedings of the 2022 IEEE 19th India Council International Conference (INDICON), Kochi, India, 24–26 November 2022; pp. 1–6. [Google Scholar]
- Kihira, S.; Mei, X.; Mahmoudi, K.; Liu, Z.; Dogra, S.; Belani, P.; Tsankova, N.; Hormigo, A.; Fayad, Z.A.; Doshi, A.; et al. U-Net Based Segmentation and Characterization of Gliomas. Cancers 2022, 14, 4457. [Google Scholar] [CrossRef]
- Faghani, S.; Khosravi, B.; Moassefi, M.; Conte, G.M.; Erickson, B.J. A Comparison of Three Different Deep Learning-Based Models to Predict the MGMT Promoter Methylation Status in Glioblastoma Using Brain MRI. J. Digit. Imaging 2023, 36, 837–846. [Google Scholar] [CrossRef]
- Chu, W.; Zhou, Y.; Cai, S.; Chen, Z.; Cai, C. A Comprehensive Multi-Modal Domain Adaptative Aid Framework for Brain Tumor Diagnosis. In Proceedings of the Pattern Recognition and Computer Vision: 6th Chinese Conference, PRCV 2023, Proceedings, Xiamen, China, 13–15 October 2023; Lecture Notes in Computer Science (14437). Liu, Q., Wang, H., Ma, Z., Zheng, W., Zha, H., Chen, X., Wang, L., Ji, R., Eds.; Springer Nature: Singapore, 2023; p. 94, ISBN 978-981-99-8558-6. [Google Scholar]
- Rui, W.; Zhang, S.; Shi, H.; Sheng, Y.; Zhu, F.; Yao, Y.; Chen, X.; Cheng, H.; Zhang, Y.; Aili, A.; et al. Deep Learning-Assisted Quantitative Susceptibility Mapping as a Tool for Grading and Molecular Subtyping of Gliomas. Phenomics 2023, 3, 243–254. [Google Scholar] [CrossRef]
- Saeed, N.; Ridzuan, M.; Alasmawi, H.; Sobirov, I.; Yaqub, M. MGMT Promoter Methylation Status Prediction Using MRI Scans? An Extensive Experimental Evaluation of Deep Learning Models. Med. Image Anal. 2023, 90, 102989. [Google Scholar] [CrossRef]
- Sakly, H.; Said, M.; Seekins, J.; Guetari, R.; Kraiem, N.; Marzougui, M. Brain Tumor Radiogenomic Classification of O6-Methylguanine-DNA Methyltransferase Promoter Methylation in Malignant Gliomas-Based Transfer Learning. Cancer Control. 2023, 30, 10732748231169149. [Google Scholar] [CrossRef]
- Zhang, H.; Zhang, H.; Zhang, Y.; Zhou, B.; Wu, L.; Lei, Y.; Huang, B. Deep Learning Radiomics for the Assessment of Telomerase Reverse Transcriptase Promoter Mutation Status in Patients With Glioblastoma Using Multiparametric MRI. J. Magn. Reson. Imaging 2023, 58, 1441–1451. [Google Scholar] [CrossRef]
- Saxena, S.; Jena, B.; Mohapatra, B.; Gupta, N.; Kalra, M.; Scartozzi, M.; Saba, L.; Suri, J.S. Fused Deep Learning Paradigm for the Prediction of O6-Methylguanine-DNA Methyltransferase Genotype in Glioblastoma Patients: A Neuro-Oncological Investigation. Comput. Biol. Med. 2023, 153, 106492. [Google Scholar] [CrossRef]
- Saxena, S.; Agrawal, A.; Dash, P.; Jena, B.; Khanna, N.N.; Paul, S.; Kalra, M.M.; Viskovic, K.; Fouda, M.M.; Saba, L.; et al. Prediction of O-6-Methylguanine-DNA Methyltransferase and Overall Survival of the Patients Suffering from Glioblastoma Using MRI-Based Hybrid Radiomics Signatures in Machine and Deep Learning Framework. Neural Comput. Appl. 2023, 35, 13647–13663. [Google Scholar] [CrossRef]
- Buz-Yalug, B.; Turhan, G.; Cetin, A.I.; Dindar, S.S.; Danyeli, A.E.; Yakicier, C.; Pamir, M.N.; Özduman, K.; Dincer, A.; Ozturk-Isik, E. Identification of IDH and TERTp Mutations Using Dynamic Susceptibility Contrast MRI with Deep Learning in 162 Gliomas. Eur. J. Radiol. 2024, 170, 111257. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Xu, X.; Zhang, W.; Zhang, L.; Wen, M.; Gao, J.; Yang, J.; Kan, Y.; Yang, X.; Wen, Z.; et al. A Fusion Model Integrating Magnetic Resonance Imaging Radiomics and Deep Learning Features for Predicting Alpha-Thalassemia X-Linked Intellectual Disability Mutation Status in Isocitrate Dehydrogenase–Mutant High-Grade Astrocytoma: A Multicenter Study. Quant. Imaging Med. Surg. 2024, 14, 251–263. [Google Scholar] [CrossRef]
- Zhang, L.; Wang, R.; Gao, J.; Tang, Y.; Xu, X.; Kan, Y.; Cao, X.; Wen, Z.; Liu, Z.; Cui, S.; et al. A Novel MRI-Based Deep Learning Networks Combined with Attention Mechanism for Predicting CDKN2A/B Homozygous Deletion Status in IDH-Mutant Astrocytoma. Eur. Radiol. 2024, 34, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Zhou, B.; Zhang, H.; Zhang, Y.; Lei, Y.; Huang, B. Peritumoural Radiomics for Identification of Telomerase Reverse Transcriptase Promoter Mutation in Patients With Glioblastoma Based on Preoperative MRI. Can. Assoc. Radiol. J. 2024, 75, 143–152. [Google Scholar] [CrossRef]
- Clark, K.; Vendt, B.; Smith, K.; Freymann, J.; Kirby, J.; Koppel, P.; Moore, S.; Phillips, S.; Maffitt, D.; Pringle, M.; et al. The Cancer Imaging Archive (TCIA): Maintaining and Operating a Public Information Repository. J. Digit. Imaging 2013, 26, 1045–1057. [Google Scholar] [CrossRef]
- Welcome to the Cancer Imaging Archive. Available online: https://www.cancerimagingarchive.net/ (accessed on 4 August 2024).
- Stamoulou, E.; Spanakis, C.; Manikis, G.C.; Karanasiou, G.; Grigoriadis, G.; Foukakis, T.; Tsiknakis, M.; Fotiadis, D.I.; Marias, K. Harmonization Strategies in Multicenter MRI-Based Radiomics. J. Imaging 2022, 8, 303. [Google Scholar] [CrossRef]
- Leithner, D.; Nevin, R.B.; Gibbs, P.; Weber, M.; Otazo, R.; Vargas, H.A.; Mayerhoefer, M.E. ComBat Harmonization for MRI Radiomics: Impact on Non-Binary Tissue Classification by Machine Learning. Investig. Radiol. 2023, 58, 697–701. [Google Scholar] [CrossRef]
- Evaluation of Conventional and Deep Learning Based Image Harmonization Methods in Radiomics Studies—IOPscience. Available online: https://iopscience.iop.org/article/10.1088/1361-6560/ac39e5/meta (accessed on 6 December 2024).
- Li, X.T.; Huang, R.Y. Standardization of Imaging Methods for Machine Learning in Neuro-Oncology. Neuro-Oncol. Adv. 2021, 2, iv49–iv55. [Google Scholar] [CrossRef] [PubMed]
- Lu, S.-C.; Swisher, C.L.; Chung, C.; Jaffray, D.; Sidey-Gibbons, C. On the Importance of Interpretable Machine Learning Predictions to Inform Clinical Decision Making in Oncology. Front. Oncol. 2023, 13, 1129380. [Google Scholar] [CrossRef]
- Cheng, P.M.; Montagnon, E.; Yamashita, R.; Pan, I.; Cadrin-Chênevert, A.; Perdigón Romero, F.; Chartrand, G.; Kadoury, S.; Tang, A. Deep Learning: An Update for Radiologists. RadioGraphics 2021, 41, 1427–1445. [Google Scholar] [CrossRef]
- Linardatos, P.; Papastefanopoulos, V.; Kotsiantis, S. Explainable AI: A Review of Machine Learning Interpretability Methods. Entropy 2021, 23, 18. [Google Scholar] [CrossRef] [PubMed]
- The Image Biomarker Standardization Initiative: Standardized Quantitative Radiomics for High-Throughput Image-Based Phenotyping|Radiology. Available online: https://pubs.rsna.org/doi/full/10.1148/radiol.2020191145 (accessed on 6 December 2024).
- Deep Learning|Nature. Available online: https://www.nature.com/articles/nature14539 (accessed on 8 March 2025).
- Afshar, P.; Mohammadi, A.; Plataniotis, K.N.; Oikonomou, A.; Benali, H. From Handcrafted to Deep-Learning-Based Cancer Radiomics: Challenges and Opportunities. IEEE Signal Process. Mag. 2019, 36, 132–160. [Google Scholar] [CrossRef]
- Huang, E.P.; O’Connor, J.P.B.; McShane, L.M.; Giger, M.L.; Lambin, P.; Kinahan, P.E.; Siegel, E.L.; Shankar, L.K. Criteria for the Translation of Radiomics into Clinically Useful Tests. Nat. Rev. Clin. Oncol. 2023, 20, 69–82. [Google Scholar] [CrossRef] [PubMed]
- Zhao, R.; Ouyang, W.; Li, H.; Wang, X. Saliency Detection by Multi-Context Deep Learning. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Boston, MA, USA, 7–12 June 2015; pp. 1265–1274. [Google Scholar]
- Mangalathu, S.; Hwang, S.-H.; Jeon, J.-S. Failure Mode and Effects Analysis of RC Members Based on Machine-Learning-Based SHapley Additive exPlanations (SHAP) Approach. Eng. Struct. 2020, 219, 110927. [Google Scholar] [CrossRef]
- Avesta, A.; Hossain, S.; Lin, M.; Aboian, M.; Krumholz, H.M.; Aneja, S. Comparing 3D, 2.5D, and 2D Approaches to Brain Image Auto-Segmentation. Bioengineering 2023, 10, 181. [Google Scholar] [CrossRef]
- Micikevicius, P.; Narang, S.; Alben, J.; Diamos, G.; Elsen, E.; Garcia, D.; Ginsburg, B.; Houston, M.; Kuchaiev, O.; Venkatesh, G.; et al. Mixed Precision Training. arXiv 2017, arXiv:1710.03740. [Google Scholar]
- Famili, A.; Lao, Y. Deep Neural Network Quantization Framework for Effective Defense against Membership Inference Attacks. Sensors 2023, 23, 7722. [Google Scholar] [CrossRef]
- A Survey of the Vision Transformers and Their CNN-Transformer Based Variants|Artificial Intelligence Review. Available online: https://link.springer.com/article/10.1007/s10462-023-10595-0 (accessed on 9 March 2025).
- Zhang, L.; LaBelle, W.; Unberath, M.; Chen, H.; Hu, J.; Li, G.; Dreizin, D. A Vendor-Agnostic, PACS Integrated, and DICOM-Compatible Software-Server Pipeline for Testing Segmentation Algorithms within the Clinical Radiology Workflow. Front. Med. 2023, 10, 1241570. [Google Scholar] [CrossRef]
- Pati, S.; Verma, R.; Akbari, H.; Bilello, M.; Hill, V.B.; Sako, C.; Correa, R.; Beig, N.; Venet, L.; Thakur, S.; et al. Reproducibility Analysis of Multi-Institutional Paired Expert Annotations and Radiomic Features of the Ivy Glioblastoma Atlas Project (Ivy GAP) Dataset. Med. Phys. 2020, 47, 6039–6052. [Google Scholar] [CrossRef]
- Brancato, V.; Cerrone, M.; Lavitrano, M.; Salvatore, M.; Cavaliere, C. A Systematic Review of the Current Status and Quality of Radiomics for Glioma Differential Diagnosis. Cancers 2022, 14, 2731. [Google Scholar] [CrossRef] [PubMed]
- A Systematic Review Reporting Quality of Radiomics Research in Neuro-Oncology: Toward Clinical Utility and Quality Improvement Using High-Dimensional Imaging Features|BMC Cancer. Available online: https://link.springer.com/article/10.1186/s12885-019-6504-5 (accessed on 8 March 2025).
- Yu, A.C.; Mohajer, B.; Eng, J. External Validation of Deep Learning Algorithms for Radiologic Diagnosis: A Systematic Review. Radiol. Artif. Intell. 2022, 4, e210064. [Google Scholar] [CrossRef]
- Muralidharan, V.; Adewale, B.A.; Huang, C.J.; Nta, M.T.; Ademiju, P.O.; Pathmarajah, P.; Hang, M.K.; Adesanya, O.; Abdullateef, R.O.; Babatunde, A.O.; et al. A Scoping Review of Reporting Gaps in FDA-Approved AI Medical Devices. NPJ Digit. Med. 2024, 7, 273. [Google Scholar] [CrossRef] [PubMed]
- Macheka, S.; Ng, P.Y.; Ginsburg, O.; Hope, A.; Sullivan, R.; Aggarwal, A. Prospective Evaluation of Artificial Intelligence (AI) Applications for Use in Cancer Pathways Following Diagnosis: A Systematic Review. BMJ Oncol. 2024, 3, e000255. [Google Scholar] [CrossRef] [PubMed]
- Khan, W.; Leem, S.; See, K.B.; Wong, J.K.; Zhang, S.; Fang, R. A Comprehensive Survey of Foundation Models in Medicine. arXiv 2024, arXiv:2406.10729. [Google Scholar] [CrossRef]
- Mei, X.; Liu, Z.; Robson, P.M.; Marinelli, B.; Huang, M.; Doshi, A.; Jacobi, A.; Cao, C.; Link, K.E.; Yang, T.; et al. RadImageNet: An Open Radiologic Deep Learning Research Dataset for Effective Transfer Learning. Radiol. Artif. Intell. 2022, 4, e210315. [Google Scholar] [CrossRef]
- Cox, J.; Liu, P.; Stolte, S.E.; Yang, Y.; Liu, K.; See, K.B.; Ju, H.; Fang, R. BrainSegFounder: Towards 3D Foundation Models for Neuroimage Segmentation. Med. Image Anal. 2024, 97, 103301. [Google Scholar] [CrossRef]
- Chen, M.; Zhang, M.; Yin, L.; Ma, L.; Ding, R.; Zheng, T.; Yue, Q.; Lui, S.; Sun, H. Medical Image Foundation Models in Assisting Diagnosis of Brain Tumors: A Pilot Study. Eur. Radiol. 2024, 34, 6667–6679. [Google Scholar] [CrossRef]
- Santra, S.; Kukreja, P.; Saxena, K.; Gandhi, S.; Singh, O.V. Navigating Regulatory and Policy Challenges for AI Enabled Combination Devices. Front. Med. Technol. 2024, 6, 1473350. [Google Scholar] [CrossRef] [PubMed]
- McKee, M.; Wouters, O.J. The Challenges of Regulating Artificial Intelligence in Healthcare. Int. J. Health Policy Manag. 2022, 12, 7261. [Google Scholar] [CrossRef] [PubMed]
- Hofer, I.S.; Burns, M.; Kendale, S.; Wanderer, J.P. Realistically Integrating Machine Learning into Clinical Practice: A Road Map of Opportunities, Challenges, and a Potential Future. Anesth. Analg. 2020, 130, 1115–1118. [Google Scholar] [CrossRef] [PubMed]
- Preti, L.M.; Ardito, V.; Compagni, A.; Petracca, F.; Cappellaro, G. Implementation of Machine Learning Applications in Health Care Organizations: Systematic Review of Empirical Studies. J. Med. Internet Res. 2024, 26, e55897. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Total no. pts | Genes | Grade | Dataset | MRI | Segmentation | Feature Extraction | Software (Framework) | Internal Validation | External Validation | RQS (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Korfiatis P, et al. (2017) [33] | 155 | MGMT | 4 | In-house (single-center) | T2 | Not undertaken | CNNs | Python (Keras) | K-fold cross-validation, held-out test set | No | 25.00 |
| Li ZC, et al. (2018) [34] | 193 | MGMT | 4 | In-house (multi-center), public | T1, T1CE, T2, T2-FLAIR | CNNs | Radiomics | Python (Keras) | Not mentioned | Yes | 38.64 |
| Chang P, et al. (2018) [35] | 259 | MGMT | 2, 3, 4 | Public | T1, T1CE, T2, T2-FLAIR | CNNs | CNNs | Python (TensorFlow) | K-fold cross-validation | No | 34.09 |
| Han L, et al. (2018) [36] | 262 | MGMT | 4 | Public | T1, T2, T2-FLAIR | Not reported | Hybrid DL Model | Python (Not reported) | Held-out test set | Yes | 38.64 |
| Korfiatis P, et al. (2018) [37] | 135 | ATRX | 2, 3, 4 | Public | T2-FLAIR | Semi-automatic | CNNs | Python (TensorFlow) | K-fold cross-validation, held-out test set | No | 36.36 |
| Fukuma R, et al. (2019) [38] | 164 | TERT | 2, 3 | In-house (multi-center) | T1, T1CE, T2, T2-FLAIR | Manually | Hybrid (CNNs, Radiomics) | Python (Keras) | K-fold cross-validation | No | 31.82 |
| Tang Z, et al. (2020) [26] | 120 | MGMT, TERT | 4 | In-house (single-center) | T1CE, DWI | Manually | CNNs | Chainer, Python (PyRadiomics) | K-fold cross-validation | No | 36.36 |
| Crisi G, et al. (2020) [39] | 59 | MGMT | 4 | In-house (single-center) | DSC | Manually | Radiomics | Python (Not reported) | K-fold cross-validation | No | 31.82 |
| Hedyehzadeh M, et al. (2020) [40] | 198 | EGFR | 4 | Public | T1, T1CE, T2-FLAIR | CNNs | CNNs | WEKA, Python (LIFEx) | K-fold cross-validation, held-out test set | No | 34.09 |
| Calabrese E, et al. (2020) [27] | 199 | 7/10 aneuploidy, MGMT, ATRX, EGFR, TERT, PTEN, CDKN2A/B, p53 | 4 | In-house (single-center) | T1, T1CE, T2, T2-FLAIR, SWI, DWI, ASL, 2D 55-direction HARDI | CNNs | Radiomics | Python (PyTorch) | K-fold cross-validation | Yes | 40.91 |
| Chen X, et al. (2020) [41] | 106 | MGMT | 4 | Public | T1CE, T2-FLAIR | CNNs | CNNs | Python (TensorFlow, PyRadiomics) | K-fold cross-validation | No | 34.09 |
| Jonnalagedda P, et al. (2020) [42] | 190 | 19/20 co-gain | 4 | In-house (single-center), public | T2-FLAIR | Manually | Hybrid DL Model | Python (Keras, scikit-learn) | K-fold cross-validation | Yes | 36.36 |
| Haubold J, et al. (2021) [28] | 217 | MGMT, ATRX | 2, 3, 4 | In-house (single-center) | T1, T1CE, T2-FLAIR | CNNs | Radiomics | Python (Not reported) | Held-out test set | No | 34.09 |
| Yogananda CGB, et al. (2021) [43] | 247 | MGMT | 2, 3, 4 | Public | T2 | CNNs | CNNs | Python, DeepMedic (PyRadiomics) | K-fold cross-validation | No | 38.64 |
| Tupe-Waghmare P, et al. (2021) [44] | 307 | MGMT | 4 | In-house (multi-center), public | T1CE, T2, T2-FLAIR | CNNs | Hybrid DL Model | Python (Keras) | Held-out test set | Yes | 40.91 |
| Chen H, et al. (2021) [45] | 244 | PTEN | 2, 3, 4 | In-house (single-center), public | T1, T1CE, T2, T2-FLAIR | CNNs | Hybrid (CNNs, Radiomics) | Python (Not reported) | bootstrapping | Yes | 47.73 |
| Lang DM, et al. (2021) [46] | 585 | MGMT | 4 | Public | T1, T1CE, T2, T2-FLAIR | Not reported | C3D Network | Python (PyTorch, scikit-learn, PyRadiomics) | Held-out test set, bootstrapping | Yes | 38.64 |
| Xiao Z, et al. (2021) [47] | 108 | SYP | 2, 3 | Public | T1, T1CE, T2 | Manually | CNNs | Python (Not reported) | K-fold cross-validation | No | 43.18 |
| Sohn B, et al. (2021) [29] | 418 | MGMT, ATRX, EGFR | 4 | In-house (single-center) | T1, T1CE, T2, T2-FLAIR | CNNs | Radiomics | Python (PyTorch) | Held-out test set | No | 31.82 |
| Capuozzo S, et al. (2022) [48] | 864 | MGMT | 4 | In-house (single-center), public | T1, T1CE, T2, T2-FLAIR | Knowledge-based filtering | CNNs | Python (Scikit-Learn, PyRadiomics) | K-fold cross-validation | Yes | 43.18 |
| Chen S, et al. (2022) [49] | 111 | MGMT | 2, 3, 4 | In-house (single-center) | T1CE, ADC | Manually | CNNs | Python (PyTorch) | K-fold cross-validation | No | 31.82 |
| Calabrese E, et al. (2022) [30] | 400 | 7/10 aneuploidy, MGMT, ATRX, EGFR, TERT, PTEN, CDKN2A/B, p53 | 4 | In-house (single-center), public | T1, T1CE, T2, T2-FLAIR, SWI, ASL | CNNs | Hybrid (CNNs, Radiomics) | Python (PyTorch) | K-fold cross-validation | No | 38.64 |
| Farzana W, et al. (2022) [50] | 672 | MGMT | 4 | Public | T1, T1CE, T2, T2-FLAIR | Not undertaken | CNNs | Python (TensorFlow, scikit-learn) | Not mentioned | Yes | 34.09 |
| Kim BH, et al. (2022) [51] | 985 | MGMT | 2, 3, 4 | In-house (single-center), public | T1, T1CE, T2, T2-FLAIR | Not reported | CNNs | Python (Not reported) | Held-out test set | Yes | 45.45 |
| Nalawade SS, et al. (2022) [52] | 829 | MGMT | 2, 3, 4 | Public | T2 | Not reported | CNNs | Python (PyTorch, MONAI, scikit-learn) | K-fold cross-validation | No | 31.82 |
| Xu Q, et al. (2022) [31] | 188 | MGMT, p53, Ki67 | 2, 3, 4 | In-house (single-center) | T1CE, T2 | Not reported | Transformers and Attention Mechanisms | Python (Keras) | K-fold cross-validation, held-out test set | No | 31.82 |
| Spoorthy KR, et al. (2022) [53] | 585 | MGMT | 4 | Public | T1, T1CE, T2, T2-FLAIR | Not reported | CNNs | Python (Keras) | Not mentioned | Yes | 36.36 |
| Kihira S, et al. (2022) [54] | 239 | MGMT | 2, 3, 4 | In-house (multi-center) | T2-FLAIR | CNNs | Radiomics | Python (Keras) | K-fold cross-validation | Yes | 31.82 |
| Chaddad A, et al. (2023) [32] | 83 | ATRX, p53 | 2, 3 | Public | T1, T2 | Semi-automatic | Hybrid (CNNs, Radiomics) | Python (Not reported) | leave-one-out cross-validation, held-out test set | No | 50.00 |
| Faghani S, et al. (2023) [55] | 576 | MGMT | 4 | Public | T2 | Not undertaken | CNNs | MATLAB | K-fold cross-validation | No | 38.64 |
| Chu W, et al. (2023) [56] | 200 | Ki67 | 2, 3, 4 | In-house (single-center) | T1, T1CE, T2, T2-FLAIR | U-Net | CNNs | Python (PyTorch, MONAI, scikit-learn) | Held-out test set | No | 27.27 |
| Rui W, et al. (2023) [57] | 42 | ATRX | 2, 3, 4 | In-house (single-center) | T1CE, T2-FLAIR, QSM | Semi-automatic | CNNs | Python (PyTorch) | K-fold cross-validation, held-out test set | No | 34.09 |
| Saeed N, et al. (2023) [58] | 585 | MGMT | 3, 4 | Public | T1, T1CE, T2, T2-FLAIR | Manually | CNNs | Python (Not reported) | K-fold cross-validation | Yes | 38.64 |
| Sakly H, et al. (2023) [59] | 985 | MGMT | 4 | Public | T2-FLAIR | Not reported | CNNs | Python (PyTorch, MONAI) | K-fold cross-validation | Yes | 43.18 |
| Zhang H, et al. (2023) [60] | 274 | TERT | 4 | In-house (multi-center), public | T1, T1CE, T2 | Manually | Hybrid (CNNs, Radiomics) | MATLAB | K-fold cross-validation | Yes | 47.73 |
| Saxena S, et al. (2023) [61] | 585 | MGMT | 4 | Public | T1 | Manually | Hybrid DL Model | Python (Not reported, PyRadiomics) | K-fold cross-validation | Yes | 40.91 |
| Saxena S, et al. (2023) [62] | 555 | MGMT | 4 | Public | T1, T1CE, T2, T2-FLAIR | Manually | Hybrid (CNNs, Radiomics) | Python (PyTorch) | K-fold cross-validation | Yes | 50.00 |
| Robinet, et al. (2023) [13] | 574 | MGMT | 4 | In-house (single-center), public | T1CE, T2-FLAIR | CNNs | CNNs | Python (Not reported) | Held-out test set | Yes | 43.18 |
| Buz-Yalug B, et al. (2024) [63] | 162 | TERT | 2, 3, 4 | In-house (single-center) | T1, T1CE, DSC | Semi-automatic | Hybrid DL Model | Python (PyTorch) | K-fold cross-validation, held-out test set | No | 29.55 |
| Liu Z, et al. (2024) [64] | 234 | ATRX | 3, 4 | In-house (multi-center) | T1CE, T2-FLAIR | Semi-automatic | Hybrid (CNNs, Radiomics) | Python (TensorFlow, Keras) | K-fold cross-validation, held-out test set | Yes | 45.45 |
| Zhang L, et al. (2024) [65] | 234 | CDKN2A/B | 2, 3 | Public | T1CE, T2 | Semi-automatic | Hybrid DL model | Python (PyTorch) | K-fold cross-validation, held-out test set | No | 38.64 |
| Zhang H, et al. (2024) [66] | 229 | TERT | 4 | In-house (multi-center) | T1, T1CE, T2 | Manually | CNNs | Python (PyTorch) | K-fold cross-validation | Yes | 34.09 |
| Chen X, et al. (2023) [25] | 161 | MGMT | 2, 3, 4 | In-house (single-center) | T1CE, T2, T2-FLAIR | Manually | CNNs | Python (scikit-learn, PyRadiomics) | Held-out test set | No | 25 |
| Gene | Dataset | No. of Studies | Sensitivity (95% CI) | PI (95% CI) | I2 | p-Value | Specificity (95% CI) | PI (95% CI) | I2 | p-Value | AUC |
|---|---|---|---|---|---|---|---|---|---|---|---|
| MGMT | Training | 7 | 0.83 [0.72; 0.90] | [0.39; 0.97] | 85.30% | 0.00 | 0.79 [0.68; 0.88] | [0.33; 0.97] | 83.6% | 0.00 | 0.88 |
| Validation | 23 | 0.74 [0.66; 0.80] | [0.35; 0.94] | 80.90% | 0.00 | 0.75 [0.65; 0.82] | [0.27; 0.96] | 84.5% | 0.00 | 0.81 | |
| ATRX | Validation | 7 | 0.79 [0.67; 0.87] | [0.64; 0.89] | 0.00% | 0.79 | 0.85 [0.78; 0.91] | [0.62; 0.95] | 40.7% | 0.12 | 0.87 |
| TERT | Validation | 6 | 0.81 [0.72; 0.87] | [0.51; 0.94] | 60.20% | 0.03 | 0.70 [0.61; 0.77] | [0.46; 0.86] | 40.0% | 0.14 | 0.81 |
| 7/10 aneuploidy * | Validation | 2 | 0.82–0.89 | - | - | - | 0.71–0.88 | - | - | - | - |
| CDKN2A/B * | Validation | 2 | 0.76–0.83 | - | - | - | 0.81–0.86 | - | - | - | - |
| EGFR * | Validation | 3 | 0.66–0.81 | - | - | - | 0.59–0.70 | - | - | - | - |
| Ki67 * | Validation | 1 | 0.98 | - | - | - | 0.81 | - | - | - | - |
| p53 * | Validation | 3 | 0.57–0.98 | - | - | - | 0.59–0.86 | - | - | - | - |
| PTEN * | Validation | 2 | 0.63–0.76 | - | - | - | 0.66–0.68 | - | - | - | - |
| SYP * | Validation | 1 | 0.90 | - | - | - | 0.95 | - | - | - | - |
| Covariates | Subgroup | No. of Studies | Sensitivity (95% CI) | p-Value (Between Study) | Specificity (95% CI) | p-Value (Between Study) |
|---|---|---|---|---|---|---|
| Tumor grade | HGG | 20 | 0.68 [0.63; 0.73] | 0.05 | 0.71 [0.62; 0.78] | 0.13 |
| LGG & HGG | 9 | 0.85 [0.68; 0.94] | 0.83 [0.68; 0.92] | |||
| Clinical information | Included | 9 | 0.71 [0.56; 0.83] | 0.69 | 0.80 [0.67; 0.89] | 0.25 |
| Not included | 20 | 0.74 [0.67; 0.80] | 0.71 [0.62; 0.79] | |||
| Data augmentation | Included | 18 | 0.77 [0.68; 0.85] | 0.12 | 0.75 [0.64; 0.84] | 0.81 |
| Not included | 11 | 0.68 [0.61; 0.75] | 0.73 [0.62; 0.82] | |||
| Dataset | In-house (single center) | 11 | 0.80 [0.67; 0.89] | 0.01 | 0.87 [0.76; 0.93] | 0.00 |
| In-house (single center), Public | 6 | 0.61 [0.55; 0.67] | 0.59 [0.49; 0.68] | |||
| Segmentation method | DL | 13 | 0.69 [0.58; 0.79] | 0.26 | 0.77 [0.66; 0.85] | 0.76 |
| Manually | 6 | 0.76 [0.70; 0.81] | 0.79 [0.66; 0.88] | |||
| Feature extraction | CNNs | 12 | 0.81 [0.71; 0.89] | 0.00 | 0.74 [0.57; 0.86] | 0.70 |
| Radiomics | 6 | 0.56 [0.50; 0.62] | 0.78 [0.59; 0.90] | |||
| Pretrained model | Employed | 11 | 0.73 [0.60; 0.84] | 0.94 | 0.64 [0.51; 0.75] | 0.03 |
| Not employed | 18 | 0.73 [0.65; 0.80] | 0.80 [0.71; 0.87] | |||
| DL integration | Feature extraction | 20 | 0.79 [0.71; 0.85] | 0.00 | 0.72 [0.63; 0.79] | 0.68 |
| Tumor Segmentation | 6 | 0.56 [0.50; 0.62] | 0.78 [0.59; 0.90] | |||
| Classification | 3 | 0.72 [0.47; 0.88] | 0.81 [0.47; 0.95] | |||
| No. of MRI sequences | One Sequence | 15 | 0.83 [0.71; 0.91] | 0.03 | 0.75 [0.61; 0.85] | 0.54 |
| Four Sequences | 7 | 0.66 [0.53; 0.76] | 0.82 [0.60; 0.93] | |||
| MRI technique | Conventional | 10 | 0.70 [0.60; 0.79] | 0.44 | 0.75 [0.62; 0.85] | 0.90 |
| Advanced, Conventional | 21 | 0.75 [0.66; 0.83] | 0.74 [0.64; 0.82] | |||
| Validation method | Internally Validated Only | 18 | 0.66 [0.58; 0.73] | 0.03 | 0.82 [0.74; 0.88] | 0.00 |
| Both Internally and Externally Validated | 10 | 0.79 [0.70; 0.86] | 0.58 [0.50; 0.65] | |||
| Internal validation | Held-out test set | 7 | 0.60 [0.55; 0.65] | 0.01 | 0.73 [0.48; 0.89] | 0.91 |
| K-fold cross-validation | 16 | 0.74 [0.65; 0.82] | 0.71 [0.62; 0.79] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farahani, S.; Hejazi, M.; Moradizeyveh, S.; Di Ieva, A.; Fatemizadeh, E.; Liu, S. Diagnostic Accuracy of Deep Learning Models in Predicting Glioma Molecular Markers: A Systematic Review and Meta-Analysis. Diagnostics 2025, 15, 797. https://doi.org/10.3390/diagnostics15070797
Farahani S, Hejazi M, Moradizeyveh S, Di Ieva A, Fatemizadeh E, Liu S. Diagnostic Accuracy of Deep Learning Models in Predicting Glioma Molecular Markers: A Systematic Review and Meta-Analysis. Diagnostics. 2025; 15(7):797. https://doi.org/10.3390/diagnostics15070797
Chicago/Turabian StyleFarahani, Somayeh, Marjaneh Hejazi, Sahar Moradizeyveh, Antonio Di Ieva, Emad Fatemizadeh, and Sidong Liu. 2025. "Diagnostic Accuracy of Deep Learning Models in Predicting Glioma Molecular Markers: A Systematic Review and Meta-Analysis" Diagnostics 15, no. 7: 797. https://doi.org/10.3390/diagnostics15070797
APA StyleFarahani, S., Hejazi, M., Moradizeyveh, S., Di Ieva, A., Fatemizadeh, E., & Liu, S. (2025). Diagnostic Accuracy of Deep Learning Models in Predicting Glioma Molecular Markers: A Systematic Review and Meta-Analysis. Diagnostics, 15(7), 797. https://doi.org/10.3390/diagnostics15070797