
Sequential Changes in Circulating Tumor Cells in the Peripheral Blood of Pancreatic Cancer Patients with Preoperative Chemotherapy Using a New Immunocytology-Based, Light Microscopic CTC Detection Platform

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Reagents
2.2. Patients and Bloods
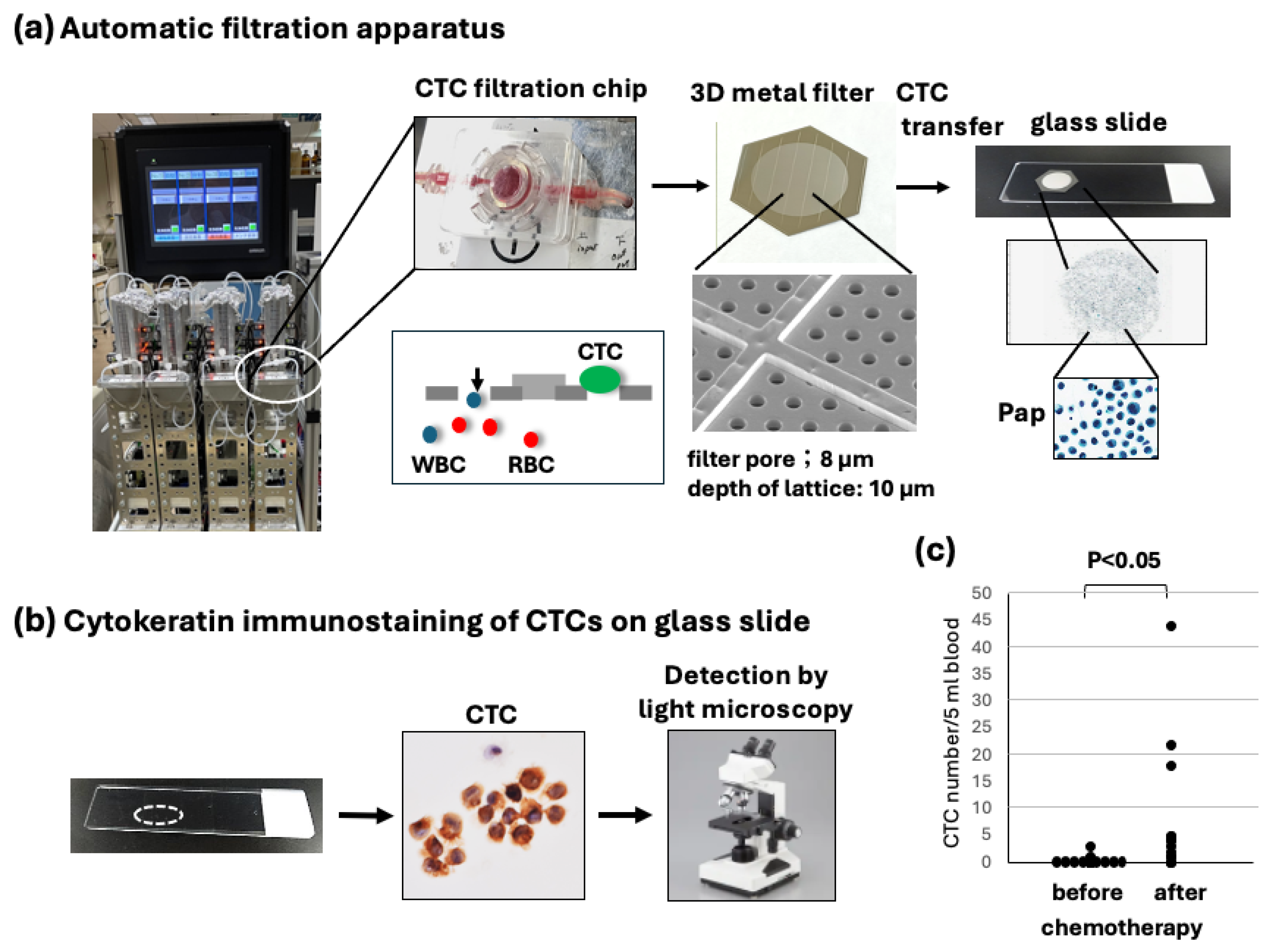
2.3. Filtration and Slide Glass-Based CTC Detection
2.4. Immunocytochemistry Using CTC Glass Slide Specimens
2.5. Statistical Analysis
3. Results
3.1. Sequential CTC Detection Using Immunocytology-Based Platform Under Microscopy
3.2. Patient Characteristics
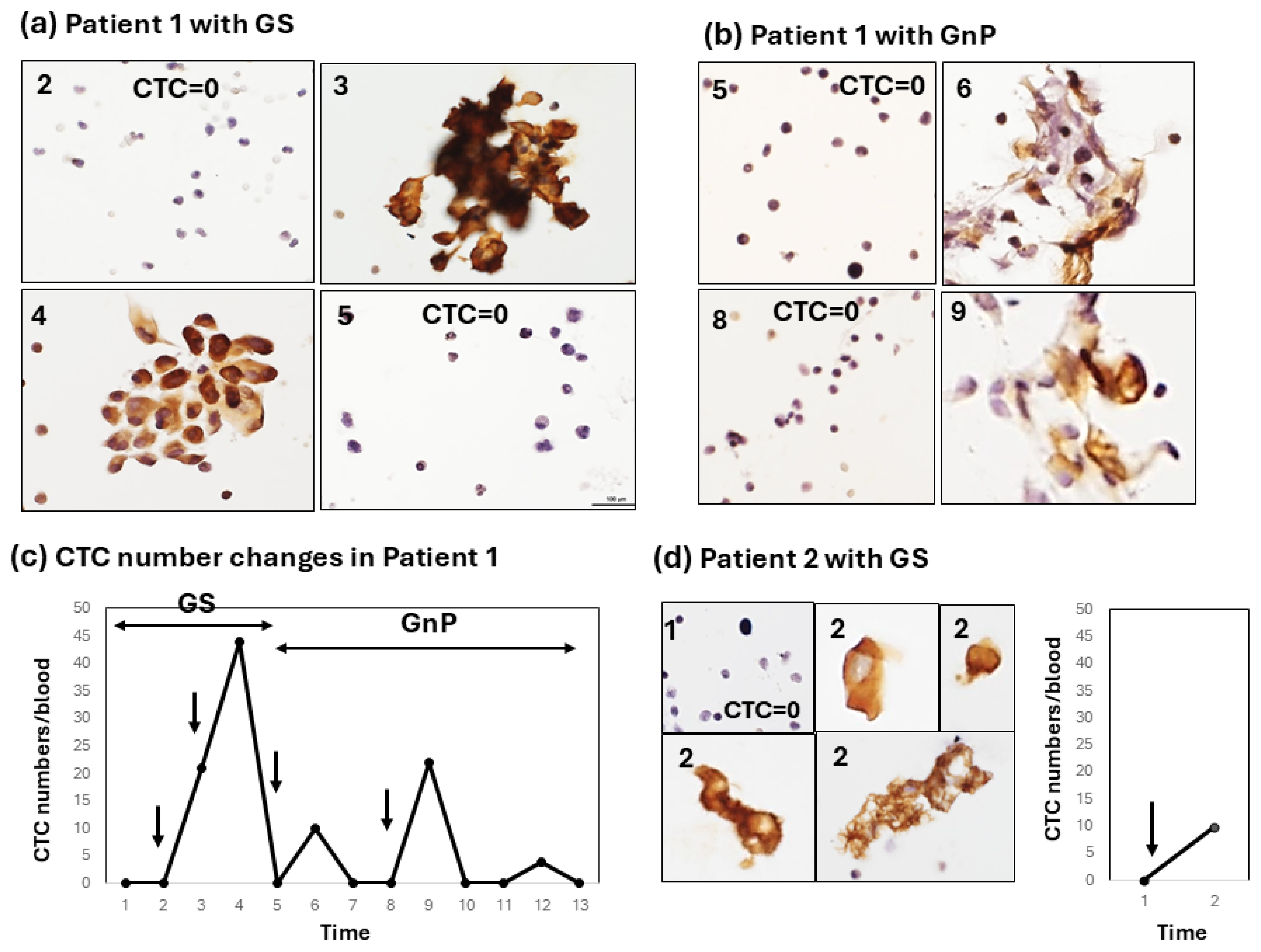
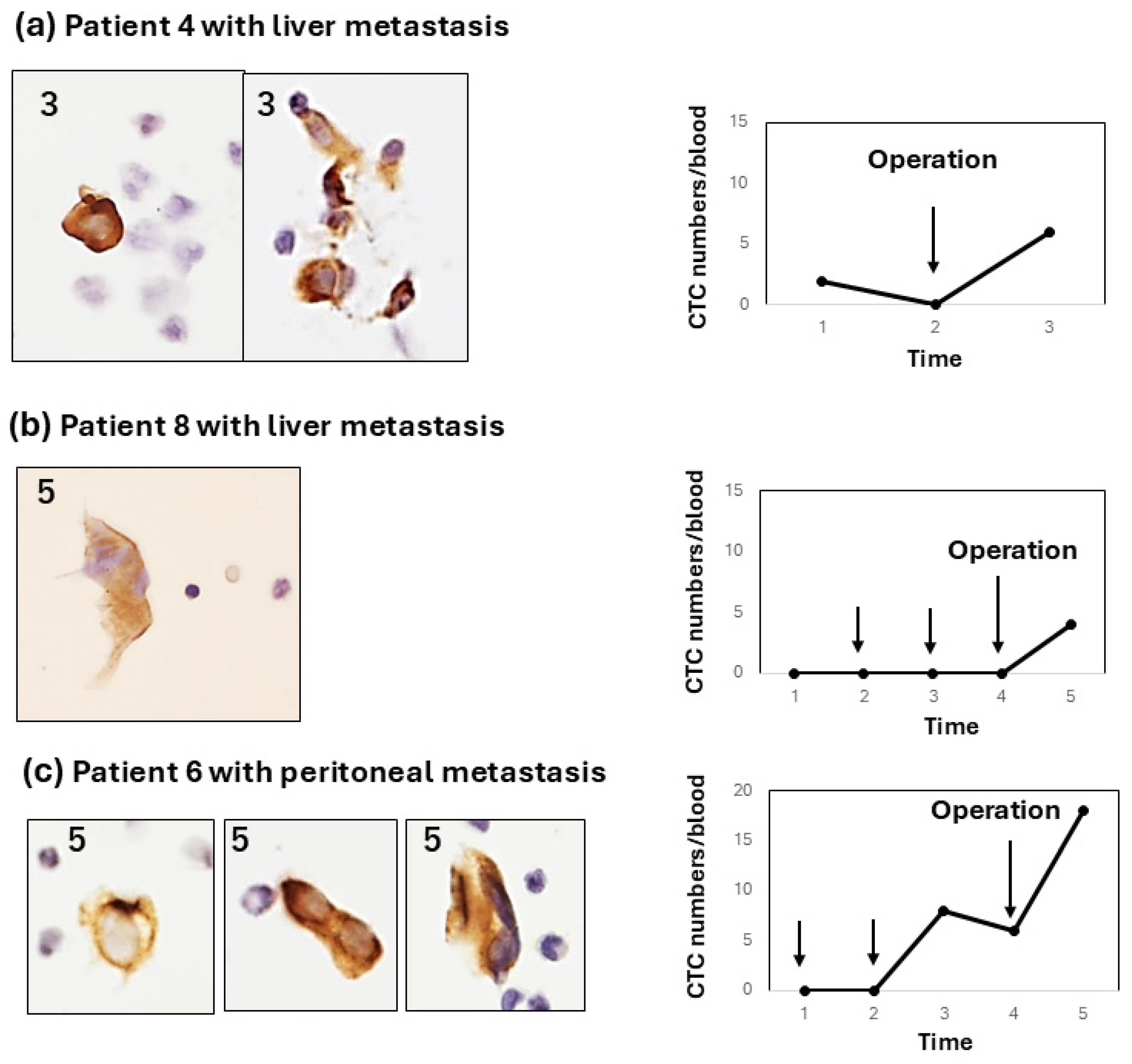
3.3. Enumeration of CTCs Before, During, and After Therapy in Pancreatic Cancer Patients
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CTC | Circulating tumor cells |
| PC | Pancreatic cancer |
References
- Global Cancer Observatory. Available online: https://gco.iarc.who.int/today (accessed on 12 March 2025).
- Strobel, O.; Lorenz, P.; Hinz, U.; Gaida, M.; König, A.K.; Hank, T.; Niesen, W.; Kaiser, J.Ö.R.; Al-Saeedi, M.; Bergmann, F.; et al. Actual five-year survival after upfront resection for pancreatic ductal adenocarcinoma: Who beats the odds? Ann. Surg. 2020, 275, 962–971. [Google Scholar] [CrossRef]
- Kolbeinsson, H.M.; Chandana, S.; Wright, G.P.; Chung, M. Pancreatic Cancer: A Review of Current Treatment and Novel Therapies. J. Investig. Surg. 2023, 36, 2129884. [Google Scholar] [CrossRef]
- Thalji, S.Z.; Aldakkak, M.; Christians, K.K.; Clarke, C.N.; George, B.; Kamgar, M.; Erickson, B.A.; Doucette, S.; Evans, D.B.; Tsai, S.; et al. Neoadjuvant chemotherapy for pancreatic cancer: Quality over quantity. J. Surg. Oncol. 2023, 128, 41–50. [Google Scholar] [CrossRef]
- Eshmuminov, D.; Aminjonov, B.; Palm, R.F.; Malleo, G.; Schmocker, R.K.; Abdallah, R.; Yoo, C.; Shaib, W.L.; Schneider, M.A.; Rangelova, E.; et al. FOLFIRINOX or gemcitabine-based chemotherapy for borderline resectable and locally advanced pancreatic cancer: A multi-institutional, patient-level, meta-analysis and systematic review. Ann. Surg. Oncol. 2023, 30, 4417–4428. [Google Scholar] [CrossRef]
- Janssen, Q.P.; van Dam, J.L.; Bonsing, B.A.; Bos, H.; Bosscha, K.P.; van Eijck, C.H.J.; de Hingh, I.H.J.; Karsten, T.M.; van der Kolk, M.B.; Patijn, G.A.; et al. Total neoadjuvant FOLFIRINOX versus neoadjuvant gemcitabine-based chemoradiotherapy and adjuvant gemcitabine for resectable and borderline resectable pancreatic cancer (PREOPANC-2 trial): Study protocol for a nationwide multicenter randomized controlled trial. BMC Cancer 2021, 21, 300. [Google Scholar] [CrossRef]
- Vasseur, A.; Kiavue, N.; Bidard, F.-C.; Pierga, J.-Y.; Cabel, L. Clinical utility of circulating tumor cells. Mol. Oncol. 2021, 15, 1647–1666. [Google Scholar] [CrossRef]
- Lawrence, R.; Watters, M.; Davies, C.R.; Pantel, K.; Lu, Y.J. Circulating tumor cells for early detection of clinical relevant cancer. Nat. Rev. Clin. Oncol. 2023, 20, 487–500. [Google Scholar] [CrossRef]
- Nikanjam, M.; Kato, S.; Kurzrock, R. Liquid biopsy: Current technology and clinical applications. J. Hematol. Oncol. 2022, 15, 131. [Google Scholar] [CrossRef]
- Freed, I.M.; Kasi, A.; Fateru, O.; Hu, M.; Gonzalez, P.; Weatherington, N.; Pathak, H.; Hyter, S.; Sun, W.; Al-Rajabi, R.; et al. Circulating tumor cell subpopulations predict treatment outcome in Pancreatic ductal adenocarcinoma (PDAC) patients. Cells 2023, 12, 2266. [Google Scholar] [CrossRef]
- Yeo, D.; Bastian, A.; Strauss, H.; Saxena, P.; Grimison, P.; Rasko, J.E.J. Exploring the clinical utility of pancreatic cancer circulating tumor cells. Int. J. Mol. Sci. 2022, 23, 1671. [Google Scholar] [CrossRef]
- Adachi, Y.; Yoshimura, M.; Usuki, H.; Shibata, K.; Hattori, M.; Kondo, N.; Yatabe, Y.; Iwata, H.; Kikumori, T.; Nakanishi, H.; et al. Acute phase dynamics of circulating tumor cells after paclitaxel and doxorubicin chemotherapy in breast cancer mouse models. Breast Cancer Res. Treat. 2018, 167, 439–450. [Google Scholar] [CrossRef]
- Ito, Y.; Kobuchi, S.; Kawakita, A.; Tasaka, K.; Matsunaga, Y.; Yoshioka, S.; Hashimooto, K.; Kanda, M.; Saito, T.; Nakanishi, H.; et al. Mobilization of circulating tumor cells after short- and long-term FOLFIRINOX and GEM/nab-PTX chemotherapy in xenograft mouse models of human pancreatic cancer. Cancers 2023, 15, 5482. [Google Scholar] [CrossRef]
- Riethdorf, S.; Fritsche, H.; Müller, V.; Rau, T.; Schindlbeck, C.; Rack, B.; Janni, W.; Gornet, T.; Cristofanilli, M.; Pantel, K.; et al. Detection of circulating tumor cells in peripheral blood of patients with metastatic breast cancer: A validation study of the CellSearch system. Clin. Cancer Res. 2007, 13, 920–928. [Google Scholar] [CrossRef]
- Cristofanilli, M.; Budd, G.T.; Ellis, M.J.; Stopeck, A.; Matera, J.; Miller, M.C.; Reuben, J.M.; Allard, W.J.; Terstappen, L.W.; Hayes, D.F.; et al. Circulating tumor cells, disease progression, and survival in metastatic breast cancer. N. Engl. J. Med. 2004, 351, 781–791. [Google Scholar] [CrossRef]
- Desitter, I.; Gerridae, B.S.; Benali-Furet, N.; Wechsler, J.; Jänne, P.A.; Kuang, Y.; Yanagita, M.; Berkowitz, J.A.; Distel, R.J.; Cayre, Y.E. A new device for rapid isolation by size and characterization of rare circulating tumor cells. Anticancer Res. 2011, 31, 427–441. [Google Scholar]
- Tsutsuyama, M.; Nakanishi, H.; Yoshimura, M.; Oshiro, T.; Kinoshita, T.; Shimizu, Y.; Sakakibara, Y.; Yatabe, Y.; Ito, S.; Kodera, Y.; et al. Detection of circulating tumor cells in drainage venous blood from colorectal cancer patients using a new filtration and cytology-based automated platform. PLoS ONE 2019, 14, e021221. [Google Scholar] [CrossRef]
- Hattori, M.; Nakanishi, H.; Yoshimura, A.; Adachi, Y.; Gondo, N.; Kotani, H.; Sawaki, M.; Fujita, N.; Yatabe, Y.; Iwata, H. Circulating tumor cells detection in tumor draining vein of breast cancer patients. Sci. Rep. 2019, 9, 18195. [Google Scholar] [CrossRef]
- Dejima, H.; Nakanishi, H.; Takeyama, R.; Nishida, T.; Yamauchi, Y.; Saito, Y.; Sakao, Y. Detection of Circulating Tumor Cells and EGFR Mutation in Pulmonary Vein and Arterial Blood of Lung Cancer Patients Using a Newly Developed Immunocytology-Based Platform. Diagnostics 2024, 14, 2064. [Google Scholar] [CrossRef]
- Ozaka, M.; Matsumura, Y.; Ishii, H.; Omuro, Y.; Itoi, T.; Mouri, H.; Hanada, K.; Kimura, Y.; Maetani, I.; Okabe, Y.; et al. Randomized phase II study of gemcitabine and.; S-1 combination versus gemcitabine alone in the treatment of unresectable advanced pancreaticcancer (Japan Clinical Cancer Research Organization PC-01 study). Cancer Chemother. Pharmacol. 2012, 69, 1197–1204. [Google Scholar] [CrossRef]
- Sai, S.; Toyoda, M.; Tobimatsu, K.; Satake, H.; Yasui, H.; Kimbara, S.; Koyama, T.; Fujishima, Y.; Imamura, Y.; Funakoshi, Y.; et al. Phase 1 study of Gemcitabine/Nab-paclitaxel/S-1 in patients with unresectable pancreatic cancer (GeNeS1S trial). Cancer Chemother. Pharmacol. 2021, 87, 65–71. [Google Scholar] [CrossRef]
- Teja, M.; Ocanto, A.; Couñago, F. Circulating tumor cells in pancreatic cancer: The prognostic impact in surgical patients. World J. Clin. Oncol. 2024, 15, 987–991. [Google Scholar] [CrossRef] [PubMed]
- He, W.; Hou, M.; Zhang, H.; Zeng, C.; He, S.; Li, M.; Zhang, Y.; Wang, L.; Lin, M.; Ke, Z.; et al. Clinical significance of circulating tumor cells in predicting disease progression and chemotherapy resistance in patients with gestational choriocarcinoma. Int. J. Cancer 2018, 144, 1421–1431. [Google Scholar] [CrossRef]
- Kitahata, Y.; Kawai, M.; Hirono, S.; Okada, K.I.; Miyazawa, M.; Motobayashi, H.; Ueno, M.; Hayami, S.; Miyamoto, A.; Yamaue, H. Circulating tumor DNA as a potential prognostic marker in patients with borderline-resectable pancreatic cancer undergoing neoadjuvant chemotherapy followed by pancreatectomy. Ann. Surg. Oncol. 2021, 29, 1596–1605. [Google Scholar] [CrossRef]
- Demyan, L.; Habowski, A.N.; Plenker, D.; King, D.A.; Standring, O.J.; Tsang, C.; St Surin, L.; Talamini, M.A.; Tuveson, D.A.; Weiss, M.J.; et al. Pancreatic Cancer Patient-Derived Organoids Can Predict Response to Neoadjuvant Chemotherapy. Ann. Surg. 2022, 276, 450–462. [Google Scholar] [CrossRef]
- Habib, J.R.; Javed, A.A.; Wolfgang, C.L. The Significance of Circulating Tumor Cells in Pancreatic Cancer. Adv. Surg. 2024, 58, 135–142. [Google Scholar] [CrossRef]
- Radfar, P.; Es, H.A.; Salomon, R.; Kulasinghe, A.; Ramalingam, N.; Sarafraz-Yazdi, E.; Thiery, J.P.; Warkiani, M.E. Single-cell analysis of circulating tumour cells: Enabling technologies and clinical applications. Trends Biotechnol. 2022, 40, 1041–1060. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Number (n = 14) | |
|---|---|---|
| Age | Median (range) | 72 (52–86) |
| Sex | Male | 7 (50%) |
| Female | 7 (50%) | |
| Location | Head | 8 (57%) |
| Body | 4 (29%) | |
| Tail | 2 (14%) | |
| Neoadjuvant chemotherapy (NAC) | GS | 7 (50%) |
| GnP | 4 (29%) | |
| GS→GnP | 1 (7%) | |
| None | 2 (14%) | |
| Tumor size | T1 | 2 (14%) |
| T2 | 3 (21%) | |
| T3 | 9 (64%) | |
| Lymph node metastasis | N0 | 12 (86%) |
| N1 | 2 (14%) | |
| Pathological stage (pStage) | I | 1 (7%) |
| II | 5 (36%) | |
| III | 0 (0%) | |
| IV | 8 (57%) | |
| Histology | Adenocarcinoma | 14 (100%) |
| Others | 0 (0%) | |
| Clinical effect of chemotherapy | PR | 5 (36%) |
| SD | 3 (21%) | |
| PD | 3 (21%) | |
| ND | 3 (21%) |
| Patient | Regime | Type (Response to Chemotherapy) | Clinical Effect of Chemotherapy | pStage | Metastasis | Post Operative CTC |
|---|---|---|---|---|---|---|
| 1 | GS + GnP | Type 1 (Early/strong) | PR | T3N0M1 | Peritoneum | Negative |
| 2 | GS | Type 1 (Early/moderate) | ND | T3N0M1 | Liver | Negative |
| 3 | GS | Type 2 (Early/weak) | SD | T1N1M0 | Negative | |
| 4 | GS | Type 2 (Early/weak) + Type 3 | PR | T3N0M1 | Liver | Positive |
| 5 | GS | Type 2 (Late/weak) | PR | T3N0M0 | Negative | |
| 6 | GS | Type 2 (Late/weak) + Type 3 | PR | T3N0M1 | Peritoneum | Positive |
| 7 | GS | Type 2 (Late/weak) | SD | T3N0M0 | Negative | |
| 8 | GS | Type 3 (No response) | PR | T3N0M1 | Liver | Positive |
| 9 | GnP | No response | PD | T3N0M1 | Lung | Negative |
| 10 | GnP | Late/weak | PD | T3N0M0 | Negative | |
| 11 | GnP | No response | PD | T2N0M1 | Peritoneum | Negative |
| 12 | GnP | No response | SD | T2N0M0 | Negative | |
| 13 | None | ND | ND | T1N0M0 | Negative | |
| 14 | None | ND | ND | T2N1M0 | Negative |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yasui, K.; Saito, T.; Ueda, S.; Shinohara, K.; Fukami, Y.; Sano, T.; Nakanishi, H. Sequential Changes in Circulating Tumor Cells in the Peripheral Blood of Pancreatic Cancer Patients with Preoperative Chemotherapy Using a New Immunocytology-Based, Light Microscopic CTC Detection Platform. Diagnostics 2025, 15, 752. https://doi.org/10.3390/diagnostics15060752
Yasui K, Saito T, Ueda S, Shinohara K, Fukami Y, Sano T, Nakanishi H. Sequential Changes in Circulating Tumor Cells in the Peripheral Blood of Pancreatic Cancer Patients with Preoperative Chemotherapy Using a New Immunocytology-Based, Light Microscopic CTC Detection Platform. Diagnostics. 2025; 15(6):752. https://doi.org/10.3390/diagnostics15060752
Chicago/Turabian StyleYasui, Kohei, Takuya Saito, Sho Ueda, Kentaro Shinohara, Yasuyuki Fukami, Tsuyoshi Sano, and Hayao Nakanishi. 2025. "Sequential Changes in Circulating Tumor Cells in the Peripheral Blood of Pancreatic Cancer Patients with Preoperative Chemotherapy Using a New Immunocytology-Based, Light Microscopic CTC Detection Platform" Diagnostics 15, no. 6: 752. https://doi.org/10.3390/diagnostics15060752
APA StyleYasui, K., Saito, T., Ueda, S., Shinohara, K., Fukami, Y., Sano, T., & Nakanishi, H. (2025). Sequential Changes in Circulating Tumor Cells in the Peripheral Blood of Pancreatic Cancer Patients with Preoperative Chemotherapy Using a New Immunocytology-Based, Light Microscopic CTC Detection Platform. Diagnostics, 15(6), 752. https://doi.org/10.3390/diagnostics15060752