
Detection of Respiratory Disease Based on Surface-Enhanced Raman Scattering and Multivariate Analysis of Human Serum
 , , and
, , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Experimental Setup and Spectra Measurement
2.2. Blood Serum Samples
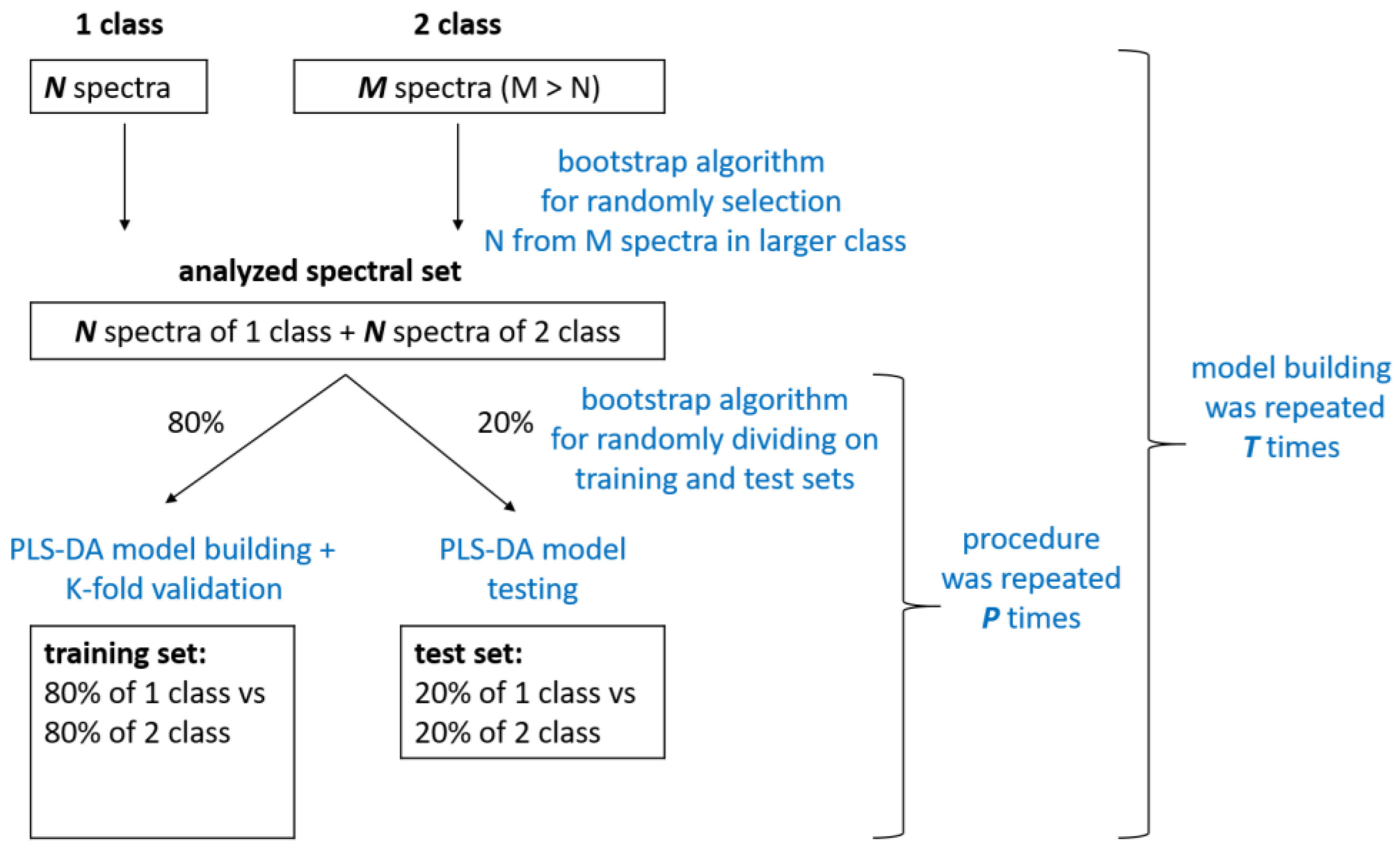
2.3. Spectra Preprocessing and Multivariate Statistical Analysis
- (1)
- “respiratory diseases (COPD + BA+ COPD&BA) vs. pathological referent group (CHF)”;
- (2)
- “COPD vs. BA”.
3. Results and Discussion
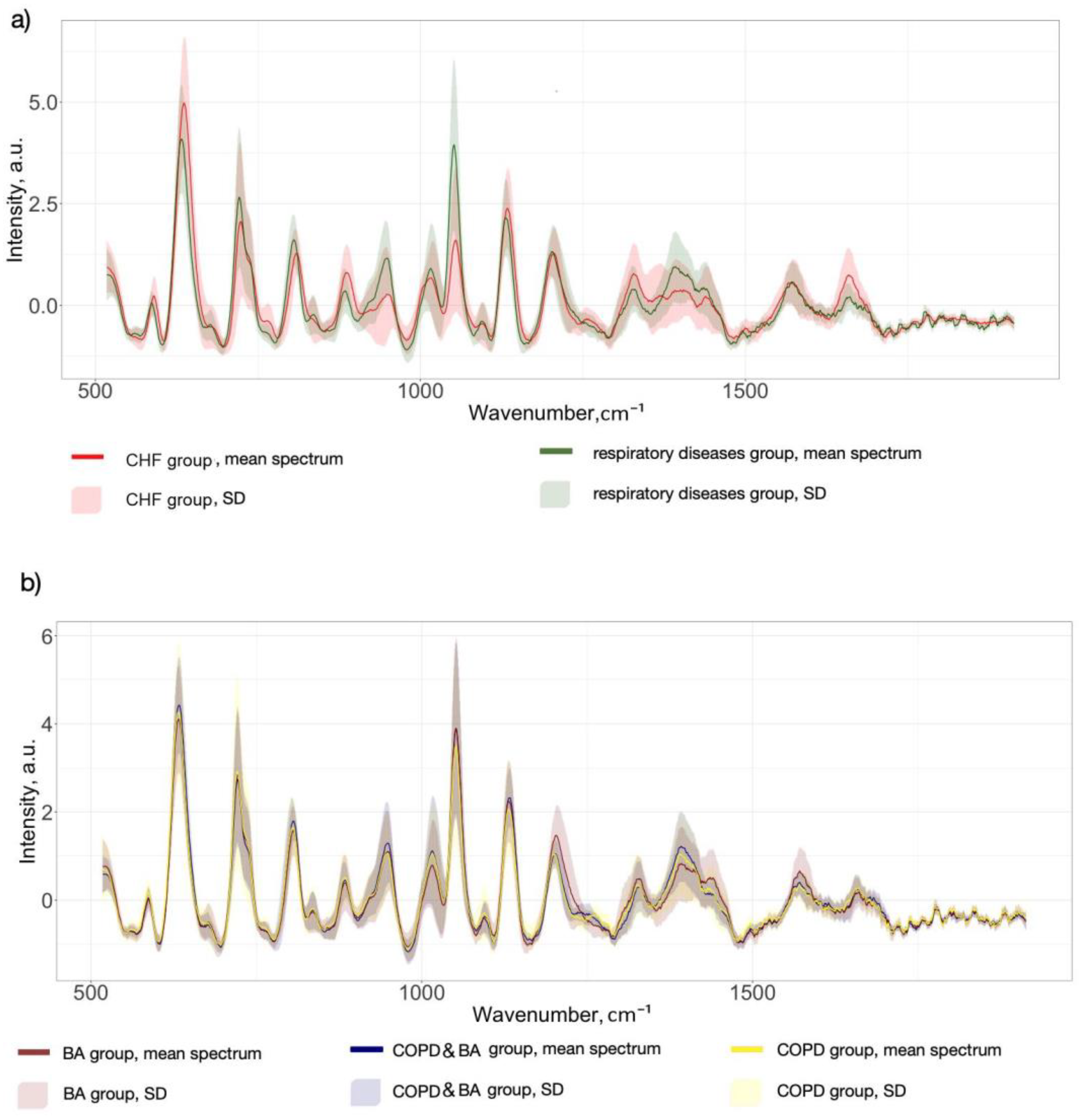
3.1. SERS Serum Spectra
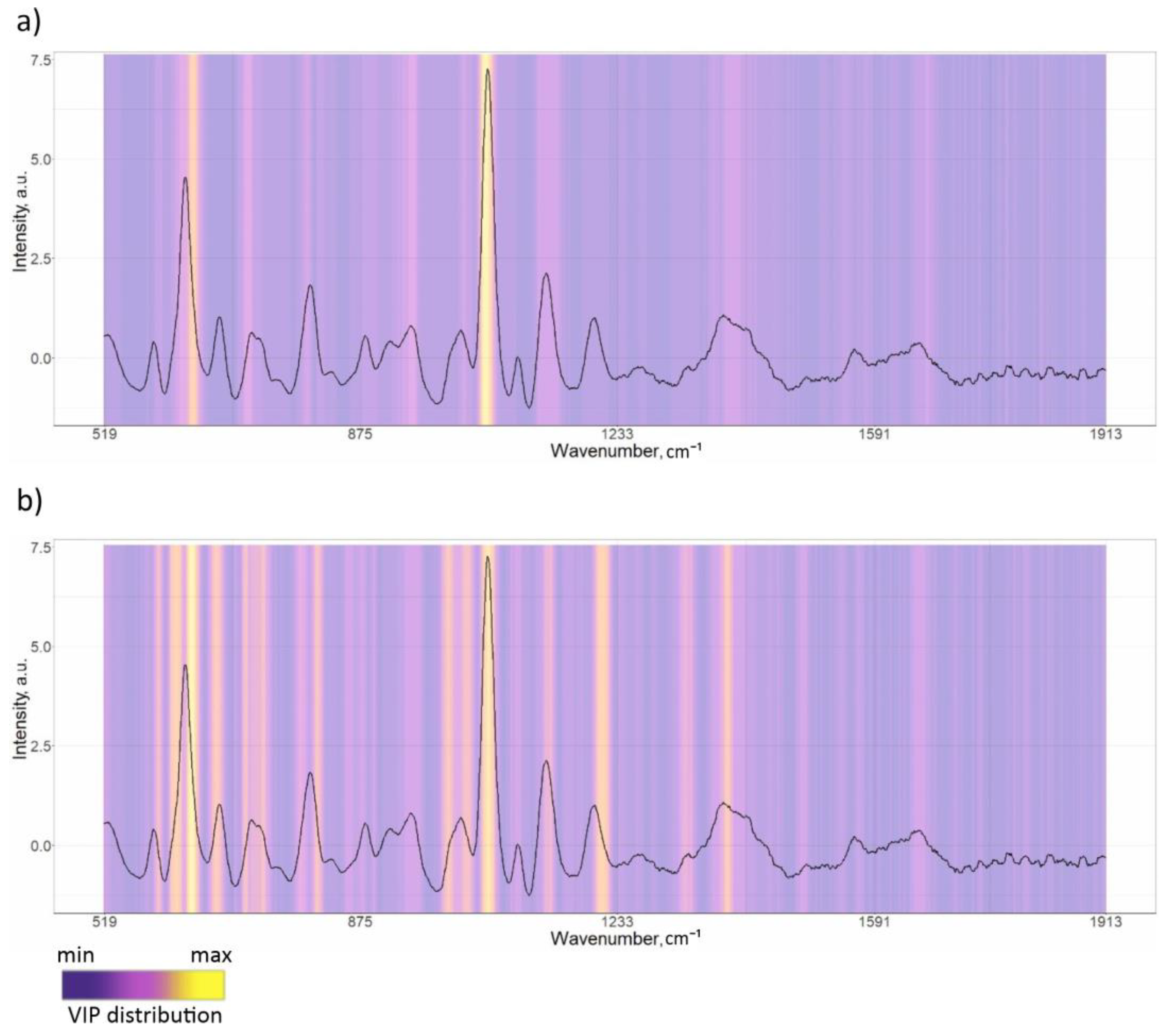
3.2. PLS-DA Classification Models
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chronic Obstructive Pulmonary Disease (COPD). Available online: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd) (accessed on 6 January 2024).
- Yoon, H.I. Biomarkers of COPD. In COPD: Heterogeneity and Personalized Treatment; Lee, S.-D., Ed.; Springer: Berlin, Heidelberg, 2017; pp. 129–143. ISBN 9783662471777. [Google Scholar]
- Agnew, M. Spirometry in Clinical Use: Practical Issues. Breathe 2010, 6, 196–203. [Google Scholar] [CrossRef]
- Vestbo, J.; Hurd, S.S.; Agustí, A.G.; Jones, P.W.; Vogelmeier, C.; Anzueto, A.; Barnes, P.J.; Fabbri, L.M.; Martinez, F.J.; Nishimura, M.; et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease: GOLD Executive Summary. Am. J. Respir. Crit. Care Med. 2013, 187, 347–365. [Google Scholar] [CrossRef] [PubMed]
- Carlomagno, C.; Gualerzi, A.; Picciolini, S.; Rodà, F.; Banfi, P.I.; Lax, A.; Bedoni, M. Characterization of the COPD Salivary Fingerprint through Surface Enhanced Raman Spectroscopy: A Pilot Study. Diagnostics 2021, 11, 508. [Google Scholar] [CrossRef]
- Zhang, W.; Zhao, Y.; Tian, Y.; Liang, X.; Piao, C. Early Diagnosis of High-Risk Chronic Obstructive Pulmonary Disease Based on Quantitative High-Resolution Computed Tomography Measurements. Int. J. Chronic Obstr. Pulm. Dis. 2023, 18, 3099–3114. [Google Scholar] [CrossRef] [PubMed]
- Dong, T.; Santos, S.; Yang, Z.; Yang, S.; Kirkhus, N.E. Sputum and Salivary Protein Biomarkers and Point-of-Care Biosensors for the Management of COPD. Analyst 2020, 145, 1583–1604. [Google Scholar] [CrossRef]
- Khristoforova, Y.; Bratchenko, L.; Bratchenko, I. Raman-Based Techniques in Medical Applications for Diagnostic Tasks: A Review. Int. J. Mol. Sci. 2023, 24, 15605. [Google Scholar] [CrossRef] [PubMed]
- Ralbovsky, N.M.; Lednev, I.K. Raman Spectroscopy and Chemometrics: A Potential Universal Method for Diagnosing Cancer. Spectrochim. Acta Part A Mol. Biomol. Spectrosc. 2019, 219, 463–487. [Google Scholar] [CrossRef]
- Chisanga, M.; Muhamadali, H.; Ellis, D.I.; Goodacre, R. Enhancing Disease Diagnosis: Biomedical Applications of Surface-Enhanced Raman Scattering. Appl. Sci. 2019, 9, 1163. [Google Scholar] [CrossRef]
- Bratchenko, L.A.; Khristoforova, Y.A.; Pimenova, I.A.; Snegerev, M.S.; Kupaev, V.I.; Lebedev, P.A.; Kistenev, Y.V.; Bratchenko, I.A. Comparative Study Into the Effect of Detector Noises and Sensitivity on the Serum SERS Analysis: Example of Non-Communicable Diseases Discrimination. J. Biophotonics 2025, e202400475. [Google Scholar] [CrossRef]
- Khristoforova, Y.A.; Bratchenko, L.A.; Skuratova, M.A.; Lebedeva, E.A.; Lebedev, P.A.; Bratchenko, I.A. Raman Spectroscopy in Chronic Heart Failure Diagnosis Based on Human Skin Analysis. J. Biophotonics 2023, 16, e202300016. [Google Scholar] [CrossRef]
- Blake, N.; Gaifulina, R.; Griffin, L.D.; Bell, I.M.; Thomas, G.M.H. Machine Learning of Raman Spectroscopy Data for Classifying Cancers: A Review of the Recent Literature. Diagnostics 2022, 12, 1491. [Google Scholar] [CrossRef]
- Hanna, K.; Krzoska, E.; Shaaban, A.M.; Muirhead, D.; Abu-Eid, R.; Speirs, V. Raman Spectroscopy: Current Applications in Breast Cancer Diagnosis, Challenges and Future Prospects. Br. J. Cancer 2022, 126, 1125–1139. [Google Scholar] [CrossRef]
- Carota, A.G.; Campanella, B.; Del Carratore, R.; Bongioanni, P.; Giannelli, R.; Legnaioli, S. Raman Spectroscopy and Multivariate Analysis as Potential Tool to Follow Alzheimer’s Disease Progression. Anal. Bioanal. Chem. 2022, 414, 4667–4675. [Google Scholar] [CrossRef] [PubMed]
- Ralbovsky, N.M.; Fitzgerald, G.S.; McNay, E.C.; Lednev, I.K. Towards Development of a Novel Screening Method for Identifying Alzheimer’s Disease Risk: Raman Spectroscopy of Blood Serum and Machine Learning. Spectrochim. Acta Part A Mol. Biomol. Spectrosc. 2021, 254, 119603. [Google Scholar] [CrossRef] [PubMed]
- Ryzhikova, E.; Ralbovsky, N.M.; Sikirzhytski, V.; Kazakov, O.; Halamkova, L.; Quinn, J.; Zimmerman, E.A.; Lednev, I.K. Raman Spectroscopy and Machine Learning for Biomedical Applications: Alzheimer’s Disease Diagnosis Based on the Analysis of Cerebrospinal Fluid. Spectrochim. Acta Part A Mol. Biomol. Spectrosc. 2021, 248, 119188. [Google Scholar] [CrossRef]
- Shipp, D.W.; Sinjab, F.; Notingher, I. Raman Spectroscopy: Techniques and Applications in the Life Sciences. Adv. Opt. Photon. 2017, 9, 315–428. [Google Scholar] [CrossRef]
- Al-Sammarraie, S.Z.; Bratchenko, L.A.; Tupikova, E.N.; Skuratova, M.A.; Wang, S.; Lebedev, P.A.; Bratchenko, I.A. Human Blood Plasma SERS Analysis Using Silver Nanoparticles for Cardiovascular Diseases Detection. J. Biomed. Photon Eng. 2024, 10, 010301. [Google Scholar] [CrossRef]
- Yang, B.; Liu, J.; Zhang, F.; Wang, Y.; Liu, X.; Niu, S.; Yuan, Y.; Bi, S. Sensitive Detection of Dextromethorphan Hydrobromide Based on Portable Raman Spectrometer and CuO@AgNPs Nano Composite SERS Substrate. Spectrochim. Acta Part A Mol. Biomol. Spectrosc. 2024, 308, 123798. [Google Scholar] [CrossRef]
- Shin, H.; Choi, B.H.; Shim, O.; Kim, J.; Park, Y.; Cho, S.K.; Kim, H.K.; Choi, Y. Single Test-Based Diagnosis of Multiple Cancer Types Using Exosome-SERS-AI for Early Stage Cancers. Nat. Commun. 2023, 14, 1644. [Google Scholar] [CrossRef]
- Sultangaziyev, A.; Ilyas, A.; Dyussupova, A.; Bukasov, R. Trends in Application of SERS Substrates beyond Ag and Au, and Their Role in Bioanalysis. Biosensors 2022, 12, 967. [Google Scholar] [CrossRef]
- Ullah, R.; Khan, S.; Farman, F.; Bilal, M.; Krafft, C.; Shahzad, S. Demonstrating the Application of Raman Spectroscopy Together with Chemometric Technique for Screening of Asthma Disease. Biomed. Opt. Express 2019, 10, 600–609. [Google Scholar] [CrossRef]
- Guleken, Z.; Tuyji Tok, Y.; Jakubczyk, P.; Paja, W.; Pancerz, K.; Shpotyuk, Y.; Cebulski, J.; Depciuch, J. Development of Novel Spectroscopic and Machine Learning Methods for the Measurement of Periodic Changes in COVID-19 Antibody Level. Measurement 2022, 196, 111258. [Google Scholar] [CrossRef]
- Goulart, A.C.C.; Zângaro, R.A.; Carvalho, H.C.; Silveira, L. Diagnosing COVID-19 in Human Sera with Detected Immunoglobulins IgM and IgG by Means of Raman Spectroscopy. J. Raman Spectrosc. 2021, 52, 2671–2682. [Google Scholar] [CrossRef] [PubMed]
- Carlomagno, C.; Bertazioli, D.; Gualerzi, A.; Picciolini, S.; Banfi, P.I.; Lax, A.; Messina, E.; Navarro, J.; Bianchi, L.; Caronni, A.; et al. COVID-19 Salivary Raman Fingerprint: Innovative Approach for the Detection of Current and Past SARS-CoV-2 Infections. Sci. Rep. 2021, 11, 4943. [Google Scholar] [CrossRef] [PubMed]
- Goulart, A.C.C.; Silveira, L.; Carvalho, H.C.; Dorta, C.B.; Pacheco, M.T.T.; Zângaro, R.A. Diagnosing COVID-19 in Human Serum Using Raman Spectroscopy. Lasers Med. Sci. 2022, 37, 2217–2226. [Google Scholar] [CrossRef] [PubMed]
- Rufino, R.; Silva, J.R.L.E. Bases Celulares e Bioquímicas Da Doença Pulmonar Obstrutiva Crônica. J. Bras. Pneumol. 2006, 32, 241–248. [Google Scholar] [CrossRef]
- Vicol, C.; Buculei, I.; Melinte, O.E.; Dobrin, M.E.; Stavarache, E.I.; Gavrilescu, C.-M.; Postolache, P.; Matei, D.; Trofor, A. The Lipid Profile and Biochemical Parameters of COPD Patients in Relation to Smoking Status. Biomedicines 2022, 10, 2936. [Google Scholar] [CrossRef]
- Rutten, F.H.; Cramer, M.M.; Lammers, J.J.; Grobbee, D.E.; Hoes, A.W. Heart Failure and Chronic Obstructive Pulmonary Disease: An Ignored Combination? Eur. J. Heart Fail. 2006, 8, 706–711. [Google Scholar] [CrossRef]
- Fabbri, L.M.; Luppi, F.; Beghé, B.; Rabe, K.F. Complex Chronic Comorbidities of COPD. Eur. Respir. J. 2008, 31, 204–212. [Google Scholar] [CrossRef]
- Al-Sammarraie, S.Z.; Bratchenko, L.A.; Typikova, E.N.; Lebedev, P.A.; Zakharov, V.P.; Bratchenko, I.A. Silver Nanoparticles-Based Substrate for Blood Serum Analysis under 785 Nm Laser Excitation. J. Biomed. Photon Eng. 2022, 8, 010301. [Google Scholar] [CrossRef]
- Marriott, P.; Efron, B.; Tibshirani, R.J. An Introduction to the Bootstrap. J. R. Stat. Soc. Ser. A 1995, 158, 347. [Google Scholar] [CrossRef]
- Bratchenko, L.A.; Bratchenko, I.A. Avoiding Overestimation and the ‘Black Box’ Problem in Biofluids Multivariate Analysis by Raman Spectroscopy: Interpretation and Transparency With the SP-LIME Algorithm. J. Raman Spectrosc. 2024. [Google Scholar] [CrossRef]
- Kucheryavskiy, S. “mdatools”: Multivariate Data Analysis for Chemometrics, R Package Version 0.9.4; R Foundation for Statistical Computing: Vienna, Austria, 2019.
- Zhang, K.; Liu, X.; Man, B.; Yang, C.; Zhang, C.; Liu, M.; Zhang, Y.; Liu, L.; Chen, C. Label-Free and Stable Serum Analysis Based on Ag-NPs/PSi Surface-Enhanced Raman Scattering for Noninvasive Lung Cancer Detection. Biomed. Opt. Express 2018, 9, 4345–4358. [Google Scholar] [CrossRef]
- Kralova, K.; Kral, M.; Vrtelka, O.; Setnicka, V. Comparative Study of Raman Spectroscopy Techniques in Blood Plasma-Based Clinical Diagnostics: A Demonstration on Alzheimer’s Disease. Spectrochim. Acta Part A Mol. Biomol. Spectrosc. 2024, 304, 123392. [Google Scholar] [CrossRef] [PubMed]
- Bonifacio, A.; Dalla Marta, S.; Spizzo, R.; Cervo, S.; Steffan, A.; Colombatti, A.; Sergo, V. Surface-Enhanced Raman Spectroscopy of Blood Plasma and Serum Using Ag and Au Nanoparticles: A Systematic Study. Anal. Bioanal. Chem. 2014, 406, 2355–2365. [Google Scholar] [CrossRef] [PubMed]
- Avci, E.; Yilmaz, H.; Sahiner, N.; Tuna, B.G.; Cicekdal, M.B.; Eser, M.; Basak, K.; Altıntoprak, F.; Zengin, I.; Dogan, S.; et al. Label-Free Surface Enhanced Raman Spectroscopy for Cancer Detection. Cancers 2022, 14, 5021. [Google Scholar] [CrossRef]
- Ndrepepa, G. Uric Acid and Cardiovascular Disease. Clin. Chim. Acta 2018, 484, 150–163. [Google Scholar] [CrossRef]
- Saito, Y.; Tanaka, A.; Node, K.; Kobayashi, Y. Uric Acid and Cardiovascular Disease: A Clinical Review. J. Cardiol. 2021, 78, 51–57. [Google Scholar] [CrossRef]
- Jung, S.W.; Kim, S.-M.; Kim, Y.G.; Lee, S.-H.; Moon, J.-Y. Uric Acid and Inflammation in Kidney Disease. Am. J. Physiol. Ren. Physiol. 2020, 318, F1327–F1340. [Google Scholar] [CrossRef]
- Sarangi, R. Serum Uric Acid in Chronic Obstructive Pulmonary Disease: A Hospital Based Case Control Study. J. Clin. Diagn. Res. 2017, 11, BC09–BC13. [Google Scholar] [CrossRef]
- Yang, H.; Wang, Z.; Xiao, S.; Dai, C.; Wen, X.; Wu, F.; Peng, J.; Tian, H.; Zhou, Y.; Ran, P. Association Between Serum Uric Acid and Lung Function in People with and without Chronic Obstructive Pulmonary Disease. Int. J. Chronic Obstr. Pulm. Dis. 2022, 17, 1069–1080. [Google Scholar] [CrossRef] [PubMed]
- Chakrabarti, B.; Angus, R.M.; Agarwal, S.; Lane, S.; Calverley, P.M.A. Hyperglycaemia as a Predictor of Outcome during Non-Invasive Ventilation in Decompensated COPD. Thorax 2009, 64, 857–862. [Google Scholar] [CrossRef] [PubMed]
- Kubysheva, N.; Boldina, M.; Eliseeva, T.; Soodaeva, S.; Klimanov, I.; Khaletskaya, A.; Bayrasheva, V.; Solovyev, V.; Villa-Vargas, L.A.; Ramírez-Salinas, M.A.; et al. Relationship of Serum Levels of IL-17, IL-18, TNF-α, and Lung Function Parameters in Patients with COPD, Asthma-COPD Overlap, and Bronchial Asthma. Mediat. Inflamm. 2020, 2020, 4652898. [Google Scholar] [CrossRef]
- Chen, Z.; Bai, F.-F.; Han, L.; Zhu, J.; Zheng, T.; Zhu, Z.; Zhou, L.-F. Targeting Neutrophils in Severe Asthma via Siglec-9. Int. Arch. Allergy Immunol. 2018, 175, 5–15. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Group of Subjects | Number of Patients | Mean Age (Min–Max) | Total Number of Spectra |
|---|---|---|---|
| Respiratory diseases (COPD + BA + COPD&BA) | 41 (21 male, 20 female) | 61 (39–74) | 143 |
| Chronic heart failure (CHF) | 103 (76 male, 27 female) | 65 (43–74) | 309 |
| BA, n = 20 | COPD, n = 11 | COPD&BA, n = 10 | p-Value | |||
|---|---|---|---|---|---|---|
| Mean ± SD | ||||||
| Smoker’s index (packs/years) | 0.032 ± 1.66 | 14.46 ± 16.63 | 27.38 ± 12.33 | 0.001 | 0.001 | 0.012 |
| Body mass index | 28.37 ± 4.96 | 26.77 ± 3.72 | 29.20 ± 5.70 | 0.146 | 0.409 | 0.057 |
| Experience of the BA, year | 13.73 ± 8.77 | – | 9.15 ± 8.81 | – | 0.070 | – |
| Experience of the COPD, year | – | 5.50 ± 5.05 | 7.31 ± 4.75 | – | – | 0.289 |
| IGS, μg/day | 301.75 ± 258.98 | 102.50 ± 216.63 | 326.15 ± 261.71 | 0.002 | 0.729 | 0.008 |
| The number of exacerbations per year | 1.55 ± 0.75 | 1.69 ± 1.08 | 2.31 ± 2.06 | 0.728 | 0.273 | 0.525 |
| ACT, scores | 16.82 ± 5.71 | – | 13.15 ± 4.58 | – | 0.047 | – |
| CAT, scores | – | 20.47 ± 8.06 | 22.75 ± 5.40 | – | – | 0.494 |
| FEV1 (%) | 77.40 ± 20.45 | 53.55 ± 28.06 | 53.48 ± 15.24 | 0.006 | 0.002 | 0.956 |
| FVC (%) | 79.17 ± 20.69 | 74.66 ± 34.76 | 65.53 ± 15.26 | 0.632 | 0.051 | 0.505 |
| FEV1/FVC | 0.79 ± 0.09 | 0.62 ± 0.15 | 0.64 ± 0.13 | 0.001 | 0.005 | 0.720 |
| Classification Models | Specificity Mean (Min–Max) | Sensitivity Mean (Min–Max) | Accuracy Mean (Min–Max) | ROC AUC Mean (Min–Max) | |
|---|---|---|---|---|---|
| Respiratory diseases (COPD + BA+ COPD&BA) vs. CHF (pathological referent group) | Training set | 0.95 (0.92–1.0) | 0.94 (0.91–0.99) | 0.95 (0.94–0.98) | 0.97 (0.96–1.0) |
| Test set | 0.97 (0.86–1.0) | 0.85 (0.70–1.0) | 0.92 (0.82–1) | 0.96 (0.85–1.0) | |
| COPD vs. BA | Training set | 0.92 (0.86–1.0) | 0.86 (0.75–0.92) | 0.89 (0.85–0.96) | 0.93 (0.78–0.99) |
| Test set | 0.57 (0.17–1.0) | 0.64 (0.0–1.0) | 0.61 (0.1–1.0) | 0.72 (0.53–1.0) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khristoforova, Y.; Bratchenko, L.; Kupaev, V.; Senyushkin, D.; Skuratova, M.; Wang, S.; Lebedev, P.; Bratchenko, I. Detection of Respiratory Disease Based on Surface-Enhanced Raman Scattering and Multivariate Analysis of Human Serum. Diagnostics 2025, 15, 660. https://doi.org/10.3390/diagnostics15060660
Khristoforova Y, Bratchenko L, Kupaev V, Senyushkin D, Skuratova M, Wang S, Lebedev P, Bratchenko I. Detection of Respiratory Disease Based on Surface-Enhanced Raman Scattering and Multivariate Analysis of Human Serum. Diagnostics. 2025; 15(6):660. https://doi.org/10.3390/diagnostics15060660
Chicago/Turabian StyleKhristoforova, Yulia, Lyudmila Bratchenko, Vitalii Kupaev, Dmitry Senyushkin, Maria Skuratova, Shuang Wang, Petr Lebedev, and Ivan Bratchenko. 2025. "Detection of Respiratory Disease Based on Surface-Enhanced Raman Scattering and Multivariate Analysis of Human Serum" Diagnostics 15, no. 6: 660. https://doi.org/10.3390/diagnostics15060660
APA StyleKhristoforova, Y., Bratchenko, L., Kupaev, V., Senyushkin, D., Skuratova, M., Wang, S., Lebedev, P., & Bratchenko, I. (2025). Detection of Respiratory Disease Based on Surface-Enhanced Raman Scattering and Multivariate Analysis of Human Serum. Diagnostics, 15(6), 660. https://doi.org/10.3390/diagnostics15060660