
Comparing the Diagnostic Efficacy of Different Calcitonin Stimulation Tests for Sporadic Medullary Thyroid Carcinoma: Calcium Gluconate vs. Calcium Chloride

 , , , and
, , , and 
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
3.1. Confirmed Cases of MTC
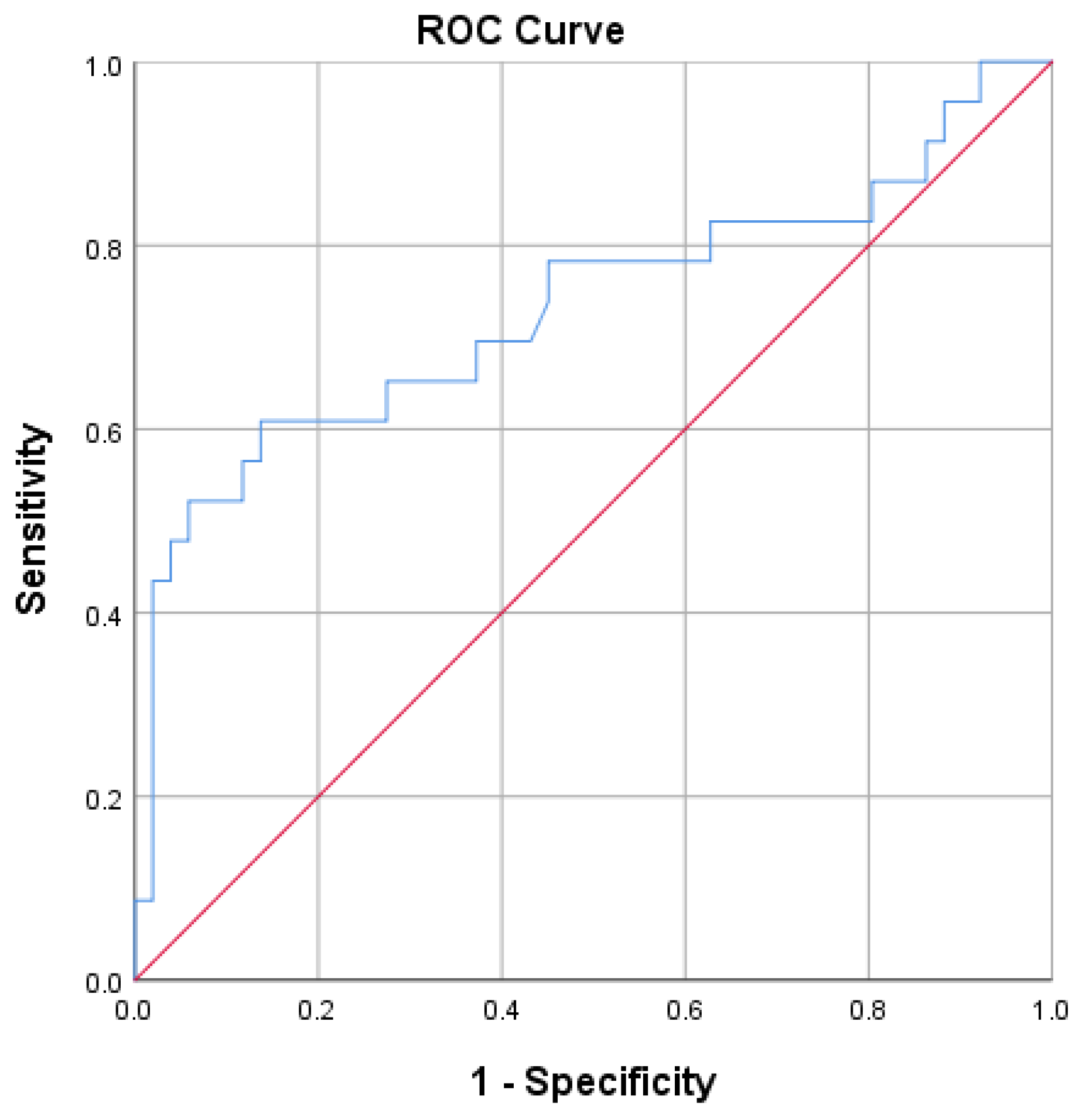
3.2. ROC Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hoff, A.O.; Hoff, P.M. Medullary Thyroid Carcinoma. Hematol./Oncol. Clin. N. Am. 2007, 21, 475–488. [Google Scholar] [CrossRef] [PubMed]
- Pelizzo, M.R.; Mazza, E.I.; Mian, C.; Merante Boschin, I. Medullary thyroid carcinoma. Expert Rev. Anticancer. Ther. 2023, 23, 943–957. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Liang, N.; Sun, H.; Frattini, F.; Sui, C.; Yang, M.; Wang, H.; Dionigi, G. Critically evaluated key points on hereditary medullary thyroid carcinoma. Front. Endocrinol. 2024, 15, 1412942. [Google Scholar] [CrossRef] [PubMed]
- Cohen, E.G.; Shaha, A.R.; Rinaldo, A.; Devaney, K.O.; Ferlito, A. Medullary thyroid carcinoma. Acta Oto-Laryngol. 2004, 124, 544–557. [Google Scholar] [CrossRef] [PubMed]
- Raue, F.; Frank-Raue, K. Epidemiology and clinical presentation of medullary thyroid carcinoma. Recent Results Cancer Res. 2015, 204, 61–90. [Google Scholar] [PubMed]
- Băetu, M.; Olariu, C.A.; Stancu, C.; Caragheorgheopol, A.; Ioachim, D.; Moldoveanu, G.; Corneci, C.; Badiu, C. Thresholds of Basal- And Calcium-Stimulated Calcitonin for Diagnosis of Thyroid Malignancy. Horm. Metab. Res. 2021, 53, 779–786. [Google Scholar] [CrossRef] [PubMed]
- Trimboli, P.; Mian, C.; Piccardo, A.; Treglia, G. Diagnostic tests for medullary thyroid carcinoma: An umbrella review. Endocrine 2023, 81, 183–193. [Google Scholar] [CrossRef] [PubMed]
- Wells, S.A.; Asa, S.L.; Dralle, H.; Elisei, R.; Evans, D.B.; Gagel, R.F.; Lee, N.; Machens, A.; Moley, J.F.; Pacini, F.; et al. Revised American thyroid association guidelines for the management of medullary thyroid carcinoma. Thyroid 2015, 25, 567–610. [Google Scholar] [CrossRef] [PubMed]
- Faggiano, A.; Giannetta, E.; Modica, R.; Albertelli, M.; Barba, L.; Dolce, P.; Motta, C.; Deiana, M.G.; Martinelli, R.; Zamponi, V.; et al. Calcium-stimulated calcitonin test for the diagnosis of medullary thyroid cancer: Results of a multicenter study and comparison between different assays. Minerva Endocrinol. 2023, 48, 253–260. [Google Scholar] [CrossRef] [PubMed]
- Toledo, S.P.A.; Lourenço, D.M.; Santos, M.A.; Tavares, M.R.; Toledo, R.A. Correia-DeurIJEdM Hypercalcitoninemia is not pathognomonic of medullary thyroid carcinoma. Clinics 2009, 64, 699–706. [Google Scholar] [CrossRef] [PubMed]
- Schuetz, M.; Beheshti, M.; Oezer, S.; Novotny, C.; Paul, M.; Hofmann, A.; Bieglmayer, C.; Niederle, B.; Kletter, K.; Dudczak, R.; et al. Calcitonin measurements for early detection of medullary thyroid carcinoma or its premalignant conditions in Hashimoto’s thyroiditis. Anticancer Res. 2006, 26, 723–727. [Google Scholar] [PubMed]
- Machens, A.; Haedecke, J.; Holzhausen, H.J.; Thomusch, O.; Schneyer, U.; Dralle, H. Differential diagnosis of calcitonin-secreting neuroendocrine carcinoma of the foregut by pentagastrin stimulation. Langenbeck’s Arch. Surg. 2000, 385, 398–401. [Google Scholar] [CrossRef] [PubMed]
- Manatakis, D.K.; Bakavos, A.; Soulou, V.N.; Dimakis, C.; Tseleni-Balafouta, S. Reactive C cell hyperplasia as an incidental finding after thyroidectomy for papillary carcinoma. Hormones 2019, 18, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Sakorafas, G.H.; Nasikas, D.; Thanos, D.; Gantzoulas, S. Incidental thyroid C cell hyperplasia: Clinical significance and implications in practice. Oncol. Res. Treat. 2015, 38, 249–252. [Google Scholar] [CrossRef] [PubMed]
- Perry, A.; Molberg, K.; Albores-Saavedra, J. Physiologic versus neoplastic C-cell hyperplasia of the thyroid: Separation of distinct histologic and biologic entities. Cancer 1996, 77, 750–756. [Google Scholar] [CrossRef]
- Albores-Saavedra, J.; Krueger, J.E. C-Cell Hyperplasia and Medullary Thyroid Microcarcinoma. Endocr. Pathol. 2001, 12, 365–377. [Google Scholar] [CrossRef] [PubMed]
- Guyétant, S.; Josselin, N.; Savagner, F.; Rohmer, V.; Michalak, S.; Saint-André, J.P. C-cell hyperplasia and medullary thyroid carcinoma: Clinicopathological and genetic correlations in 66 consecutive patients. Mod. Pathol. 2003, 16, 756–763. [Google Scholar] [CrossRef] [PubMed]
- Rosario, P.W.; Calsolari, M.R. Basal Serum Calcitonin, After Calcium Stimulation, and in the Needle Washout of Patients with Thyroid Nodules and Mild or Moderate Basal Hypercalcitoninemia. Horm. Metab. Res. 2017, 49, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Colombo, C.; Verga, U.; Mian, C.; Ferrero, S.; Perrino, M.; Vicentini, L.; Dazzi, D.; Opocher, G.; Pelizzo, M.R.; Beck-Peccoz, P.; et al. Comparison of calcium and pentagastrin tests for the diagnosis and follow-up of medullary thyroid cancer. J. Clin. Endocrinol. Metab. 2012, 97, 905–913. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, K.; Elwerr, M.; MacHens, A.; Abuazab, M.; Holzhausen, H.J.; Dralle, H. Hypercalcitoninemia in thyroid conditions other than medullary thyroid carcinoma: A comparative analysis of calcium and pentagastrin stimulation of serum calcitonin. Langenbeck’s Arch. Surg. 2013, 398, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Ubl, P.; Gincu, T.; Keilani, M.; Ponhold, L.; Crevenna, R.; Niederle, B.; Hacker, M.; Li, S. Comparison of side effects of pentagastrin test and calcium stimulation test in patients with increased basal calcitonin concentration: The gender-specific differences. Endocrine 2014, 46, 549–553. [Google Scholar] [CrossRef] [PubMed]
- Băetu, M.; Olariu, C.A.; Nițu, I.; Moldoveanu, G.; Corneci, C.; Badiu, C. Safety of calcitonin stimulation tests with calcium. Hormones 2021, 20, 769–775. [Google Scholar] [CrossRef] [PubMed]
- Kiriakopoulos, A.; Giannakis, P.; Menenakos, E. Calcitonin: Current concepts and differential diagnosis. Ther. Adv. Endocrinol. Metabolism 2022, 13, 20420188221099344. [Google Scholar] [CrossRef] [PubMed]
- Mian, C.; Perrino, M.; Colombo, C.; Cavedon, E.; Pennelli, G.; Ferrero, S.; De Leo, S.; Sarais, C.; Cacciatore, C.; Manfredi, G.I.; et al. Refining calcium test for the diagnosis of medullary thyroid cancer: Cutoffs, procedures, and safety. J. Clin. Endocrinol. Metab. 2014, 99, 1656–1664. [Google Scholar] [CrossRef] [PubMed]
- Deftos, L.J.; Weisman, M.H.; Williams, G.W.; Karpf, D.B.; Frumar, A.M.; Davidson, B.J.; Parthemore, J.G.; Judd, H.L. Influence of age and sex on plasma calcitonin in human beings. N. Engl. J. Med. 1980, 302, 1351–1353. [Google Scholar] [CrossRef] [PubMed]
- Shamonki, I.M.; Frumar, A.M.; Tataryn, I.V.; Meldrum, D.R.; Davidson, B.H.; Parthemore, J.G.; Judd, H.L.; Defto, L.J. Age-Related Changes of Calcitonin Secretion in Females. J. Clin. Endocrinol. Metab. 1980, 50, 437–439. [Google Scholar] [CrossRef] [PubMed]
- Tausanovic, K.M.; Zivaljevic, V.R.; Zorić, G.V.; Jovanovic, M.D.; Stepanovic, B.G.; Milenkovic, M.G.; Paunovic, I.R. Predictive Value of Calcium Test for Preoperative Diagnosis of Medullary Thyroid Carcinoma in Patients with Moderately Elevated Basal Calcitonin. Endocr. Pract. 2021, 27, 1077–1081. [Google Scholar] [CrossRef] [PubMed]
- You, Y.N.; Lakhani, V.; Wells, S.A.; Moley, J.F. Medullary Thyroid Cancer. Surg. Oncol. Clin. N. Am. 2006, 15, 639–660. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Kim, B.H. Current Guidelines for Management of Medullary Thyroid Carcinoma. Endocrinol. Metab. 2021, 36, 514–524. [Google Scholar] [CrossRef] [PubMed]
- Kitahara, C.M.; Sosa, J.A. The changing incidence of thyroid cancer. Nat. Rev. Endocrinol. 2016, 12, 646–653. [Google Scholar] [CrossRef] [PubMed]
- Viola, D.; Elisei, R. Management of Medullary Thyroid Cancer. Endocrinol. Metab. Clin. N. Am. 2019, 48, 285–301. [Google Scholar] [CrossRef] [PubMed]
- Papadakis, G.; Keramidas, I.; Triantafillou, E.; Kanouta, F.; Pappa, T.; Kaltzidou, V.; Tertipi, A.; Iordanidou, L.; Trivizaki, E.; Vecchini, G.; et al. Association of basal and calcium-stimulated calcitonin levels with pathological findings after total thyroidectomy. Anticancer Res. 2015, 35, 4251–4258. [Google Scholar] [PubMed]
- Zayed, A.A.; Ali, M.K.; Jaber, O.I.; Suleiman, M.D.; Ashhab, A.A.; Al_Shweiat, W.M.; Momani, M.S.; Shomaf, M.; AbuRuz, S.M. Is Hashimoto’s thyroiditis a risk factor for medullary thyroid carcinoma? Our experience and a literature review. Endocrine 2015, 48, 629–636. [Google Scholar] [CrossRef] [PubMed]
- MacHens, A.; Lorenz, K.; Weber, F.; Dralle, H. Clinical Significance of Coexistence of Hashimoto Thyroiditis and Graves’ Disease with Differentiated and Medullary Thyroid Cancer. Exp. Clin. Endocrinol. Diabetes 2022, 130, 381–385. [Google Scholar] [CrossRef] [PubMed]
- Malpani, S.; Tandon, A.; Panwar, H.; Khurana, U.; Kapoor, N.; Behera, G.; Gupta, V. Medullary thyroid carcinoma co-existent with Hashimoto’s thyroiditis diagnosed by a comprehensive cytological approach. Diagn. Cytopathol. 2020, 48, 386–389. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, A.M.; Ali, R.M.; Salih, K.M.; Mohammed, K.K.; Kakamad, F.H.; Salih, A.M. Synchronous occurrence of papillary thyroid microcarcinoma, medullary thyroid carcinoma and Hashimoto thyroiditis in a single thyroid: A case report with literature review. Int. J. Surg. Case Rep. 2022, 93, 106888. [Google Scholar] [CrossRef] [PubMed]
- SamieeRad, F.; Emami, A. Synchronous Occurrence of Papillary Thyroid Carcinoma and Medullary Carcinoma in the Setting of Hashimoto’s Thyroiditis and Multi Nodular Goiter. Iran. J. Pathol. 2022, 27, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.Y.; Park, N.H. Concurrent Medullary Carcinoma and Hashimoto’s Thyroiditis: A Case Report with an Emphasis on US Features. J. Korean Soc. Radiol. 2023, 84, 1146–1151. [Google Scholar] [CrossRef] [PubMed]
- Mousa, U.; Gursoy, A.; Ozdemir, H.; Moray, G. Medullary thyroid carcinoma in a patient with Hashimoto’s thyroiditis diagnosed by calcitonin washout from a thyroid nodule. Diagn. Cytopathol. 2013, 41, 644–646. [Google Scholar] [CrossRef] [PubMed]
- Patel, B.; Roy, A.; Badhe, B.; Siddaraju, N. Cytologic aspects of an interesting case of medullary thyroid carcinoma coexisting with Hashimoto’s thyroiditis. J. Cytol. 2016, 33, 100–102. [Google Scholar] [PubMed]
- Maghsoomi, Z.; Emami, Z.; Malboosbaf, R.; Malek, M.; Khamseh, M.E. Efficacy and safety of peptide receptor radionuclide therapy in advanced radioiodine-refractory differentiated thyroid cancer and metastatic medullary thyroid cancer: A systematic review. BMC Cancer 2021, 21, 579. [Google Scholar] [CrossRef] [PubMed]
- Park, H.; Park, J.; Choi, M.S.; Kim, J.; Kim, H.; Shin, J.H.; Kim, J.H.; Kim, J.S.; Kim, S.W.; Chung, J.H.; et al. Preoperative serum calcitonin and its correlation with extent of lymph node metastasis in medullary thyroid carcinoma. Cancers 2020, 12, 2894. [Google Scholar] [CrossRef] [PubMed]
- Bae, S.Y.; Jung, S.P.; Choe, J.H.; Kim, J.S.; Kim, J.H. Prediction of lateral neck lymph node metastasis according to preoperative calcitonin level and tumor size for medullary thyroid carcinoma. Kaohsiung J. Med. Sci. 2019, 35, 772–777. [Google Scholar] [CrossRef] [PubMed]
- Prinzi, A.; Frasca, F.; Russo, M.; Pellegriti, G.; Piticchio, T.; Tumino, D.; Belfiore, A.; Malandrino, P. Pre-Operative Calcitonin and CEA Values May Predict the Extent of Metastases to the Lateral Neck Lymph Nodes in Patients with Medullary Thyroid Cancer. Cancers 2024, 16, 2979. [Google Scholar] [CrossRef] [PubMed]
- Cohen, R.; Campos, J.M.; Salaün, C.; Heshmati, H.M.; Kraimps, J.L.; Proye, C.; Sarfati, E.; Henry, J.F.; Niccoli-Sire, P.; Modigliani, E. Preoperative calcitonin levels are predictive of tumor size and postoperative calcitonin normalization in medullary thyroid carcinoma. J. Clin. Endocrinol. Metab. 2000, 85, 919–922. [Google Scholar] [CrossRef] [PubMed]
- Yip, D.T.; Hassan, M.; Pazaitou-Panayiotou, K.; Ruan, D.T.; Gawande, A.A.; Gaz, R.D.; Moore FDJr Hodin, R.A.; Stephen, A.E.; Sadow, P.M.; Daniels, G.H. Preoperative basal calcitonin and tumor stage correlate with postoperative calcitonin normalization in patients undergoing initial surgical management of medullary thyroid carcinoma. Surgery 2011, 150, 1168–1177. [Google Scholar] [CrossRef] [PubMed]
- Opsahl, E.M.; Akslen, L.A.; Schlichting, E.; Aas, T.; Brauckhoff, K.; Hagen, A.I.; Rosenlund, A.F.; Sigstad, E.; Grøholt, K.K.; Jørgensen, L.H.; et al. The Role of Calcitonin in Predicting the Extent of Surgery in Medullary Thyroid Carcinoma: A Nationwide Population-Based Study in Norway. Eur. Thyroid. J. 2019, 8, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Ni, J.; Tu, P.; Ling, Y. Gender and tumor size-specific calcitonin cutoff value for diagnosing MTC in 10,618 patients with thyroid nodule surgery. Endocrine 2024, 86, 1097–1109. [Google Scholar] [CrossRef] [PubMed]
- Fugazzola, L.; Di Stefano, M.; Censi, S.; Repaci, A.; Colombo, C.; Grimaldi, F.; Magri, F.; Pagotto, U.; Iacobone, M.; Persani, L.; et al. Basal and stimulated calcitonin for the diagnosis of medullary thyroid cancer: Updated thresholds and safety assessment. J. Endocrinol. Investig. 2021, 44, 587–597. [Google Scholar] [CrossRef] [PubMed]
- Niederle, M.B.; Scheuba, C.; Riss, P.; Selberherr, A.; Koperek, O.; Niederle, B. Early Diagnosis of Medullary Thyroid Cancer: Are Calcitonin Stimulation Tests Still Indicated in the Era of Highly Sensitive Calcitonin Immunoassays? Thyroid 2020, 30, 974–984. [Google Scholar] [CrossRef] [PubMed]
- Parthemore, J.G.; Deftos, L.J. The regulation of calcitonin in normal human plasma as assessed by immunoprecipitation and immunoextraction. J. Clin. Investig. 1975, 56, 835–841. [Google Scholar] [CrossRef] [PubMed]
- McLean, G.W.; Rabin, D.; Moore, L.; Deftos, L.J.; Lorber, D.; McKenna, T.J. Evaluation of provocative tests in suspected medullary carcinoma of the thyroid:heterogeneity of calcitonin responses to calcium and pentagastrin. Metabolism 1984, 33, 790–796. [Google Scholar] [CrossRef] [PubMed]
- Wells SAJr Baylin, S.B.; Linehan, W.M.; Farrell, R.E.; Cox, E.B.; Cooper, C.W. Provocative agents and the diagnosis of medullary carcinoma of the thyroid gland. Ann. Surg. 1978, 188, 139–141. [Google Scholar] [CrossRef] [PubMed]
- Van Lathem, J.J.; Vermaak, W.J.; Kuyl, J.M.; Mollentze, W.; Jansen, S.; Wolmaran, L.; Pelser, H.; Barry, R.; Kruger, A.J.; Wolfaardt, M.; et al. Experience with a provocative test of calcitonin release as a prospective screening for preclinical medullary thyroid carcinoma in MEN type 2A family members. J. Clin. Lab. Anal. 1992, 6, 384–390. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex | Age (Years) | |||||
|---|---|---|---|---|---|---|
| Demographic | Male | Female | p-value | <50 | ≥50 | p-value |
| N | 70 | 106 | 53 | 123 | ||
| Basal Ct | 25.2 ± 11.6 | 25.3 ± 16.4 | 0.97 | 20.6 ± 12 | 27.2 ± 15.2 | <0.01 |
| Stimulated Ct | 669.5 ± 396.9 | 663.4 ± 497.5 | 0.9 | 534.3 ± 330.9 | 724.3 ± 499.1 | 0.01 |
| Pathohistological Diagnosis | Number of Patients | % |
|---|---|---|
| Medullary thyroid carcinoma | 36 | 20.5 |
| C-cell hyperplasia | 119 | 67.6 |
| Papillary thyroid carcinoma | 5 | 2.8 |
| Thyroid follicular nodular disease | 10 | 5.7 |
| Hashimoto thyroiditis | 4 | 2.3 |
| Follicular adenoma | 2 | 1.1 |
| No. | Sex | Age (Years) | TNM | Tu Size (mm) | Test | Basal Ct (pg/mL) | Stimulated Ct (pg/mL) | Associated Pathology |
|---|---|---|---|---|---|---|---|---|
| 1 | Female | 59 | T1NxMx | 4 | Ca-gluconate | 22.2 | 195.8 | HT |
| 2 | Female | 68 | T1NxMx | 5 | Ca-gluconate | 16.3 | 248.0 | TFNB |
| 3 | Male | 63 | T2NxMx | 15 | Ca-gluconate | 12.9 | 266.6 | TFNB |
| 4 | Female | 61 | T1NxMx | 8 | Ca-gluconate | 42.6 | 317.0 | Follicular adenoma |
| 5 | Female | 66 | T1NxMx | 4 | Ca-gluconate | 17.9 | 403.7 | TFNB |
| 6 | Female | 63 | T1NxMx | 8 | Ca-gluconate | 16.6 | 483.9 | TFNB |
| 7 | Female | 55 | T1NxMx | 5 | Ca-gluconate | 28.8 | 488.0 | TFNB |
| 8 | Female | 59 | T1NxMx | 9 | Ca-gluconate | 14.1 | 542.8 | TFNB |
| 9 | Female | 72 | T1NxMx | 8 | Ca-gluconate | 81.2 | 620.4 | HT |
| 10 | Female | 71 | T1NxMx | 6 | Ca-gluconate | 31.4 | 833.5 | TFNB |
| 11 | Female | 54 | T1NxMx | 5 | Ca-gluconate | 36.2 | 839.3 | HT |
| 12 | Female | 66 | T1NxMx | 6 | Ca-gluconate | 17.2 | 990.0 | TFNB |
| 13 | Female | 51 | T1NxMx | 6 | Ca-gluconate | 44.7 | 1217.3 | HT |
| 14 | Female | 66 | T1NxMx | 7 | Ca-gluconate | 47.6 | 1300.0 | TFNB |
| 15 | Female | 76 | T2NxMx | 25 | Ca-gluconate | 34.9 | 1342.1 | PTC |
| 16 | Female | 64 | T1NxMx | 8 | Ca-gluconate | 47.0 | 1360.0 | TFNB |
| 17 | Female | 42 | T1NxMx | 10 | Ca-gluconate | 78.0 | 1370.0 | HT |
| 18 | Male | 45 | T1NxMx | 4 | Ca-gluconate | 21.1 | 1396.9 | TFNB |
| 19 | Female | 60 | T1NxMx | 5 | Ca-gluconate | 47.0 | 1411.0 | TFNB |
| 20 | Female | 72 | T1NxMx | 8 | Ca-gluconate | 47.2 | 1461.4 | TFNB |
| 21 | Female | 61 | T1NxMx | 5 | Ca-gluconate | 48.0 | 1530.0 | TFNB |
| 22 | Male | 56 | T1NxMx | 10 | Ca-gluconate | 48.0 | 1690.0 | TFNB |
| 23 | Female | 63 | T1NxMx | 7 | Ca-gluconate | 47.0 | 3007.0 | TFNB |
| 24 | Female | 44 | T1NxMx | 4 | Ca-chloride | 49.7 | 1125 | TFNB |
| 25 | Female | 46 | T1N1Mx | 11 | Ca-chloride | 34.4 | 1300 | HT |
| 26 | Female | 36 | T1NxMx | 3 | Ca-chloride | 14.0 | 248 | HT |
| 27 | Female | 53 | T1NxMx | 3 | Ca-chloride | 39.0 | 433 | TFNB |
| 28 | Male | 44 | T1NxMx | 3 | Ca-chloride | 32.0 | 367 | PTC |
| 29 | Female | 52 | T1NxMx | 9 | Ca-chloride | 40.0 | 771 | HT |
| 30 | Female | 51 | T1NxMx | 4 | Ca-chloride | 49.5 | 1405 | TFNB |
| 31 | Female | 68 | T2NxMx | 30 | Ca-chloride | 50.1 | 2000 | PTC |
| 32 | Female | 70 | T1NxMx | 8 | Ca-chloride | 75.5 | 184 | HT |
| 33 | Female | 78 | T1NxMx | 7 | Ca-chloride | 34.0 | 637.0 | TFNB |
| 34 | Female | 70 | T1NxMx | 8 | Ca-chloride | 77.0 | 2890 | TFNB |
| 35 | Female | 66 | T1NxMx | 8 | Ca-chloride | 32.0 | 1300 | TFNB |
| 36 | Male | 40 | T1NxMx | 1 | Ca-chloride | 34.0 | 893 | PTC |
| PH Diagnosis | Basal Calcitonin (pg/mL) | Stimulated Calcitonin (pg/mL) |
|---|---|---|
| Medullary thyroid carcinoma | 38.6 ± 18.8 (12.9–81.2) | 1029.8 ± 684.4 (185.0–3007.0) |
| C-cell hyperplasia | 21.8 ± 9.8 (10–65.2) | 581.7 ± 316.6 (108.0–1818.0) |
| Other diseases of the thyroid gland | 22.1 ± 17.6 (11.0–75.8) | 525.5 ± 371.0 (122.0–1654.0) |
| Cut-Off (pg/mL) | AUC | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|
| 31.1 | 0.79 | 69.4% | 87.1% | 55% | 91.6% |
| 16.2 | 88.9% | 37.1% | 26.7% | 92.9% |
| Cut-Off (pg/mL) | AUC | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|
| 810.8 | 0.73 | 60.9% | 87.3% | 66.7% | 79.2% |
| 388.4 | 82.6% | 37.3% | 37.3% | 82.6% |
| Cut-Off (pg/mL) | AUC | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|
| 1076 | 0.69 | 53.8% | 92.1% | 50% | 93.2% |
| 431.5 | 76.9% | 34.8% | 14.7% | 91.2% |
| Ilic et al. (2025) | AUC | Cut-Off (pg/mL) | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|---|
| Basal Ct-H | 0.79 | 31.1 | 69.4% | 87.1% | 55% | 91.6% |
| Basal Ct-L | 16.2 | 88.9% | 37.1% | 26.7% | 92.9% | |
| Stimulated Ct-H | 0.73 | 810.8 | 60.9% | 87.3% | 66.7% | 79.2% |
| Stimulated Ct-L | 388.4 | 82.6% | 37.3% | 37.3% | 82.6% | |
| Faggiano et al. (2023) [9] | ||||||
| Basal Ct-F | 0.8 | 19.2 | 75% | 82% | 84% | 72% |
| Stimulated Ct-F | 0.79 | 445 | 54% | 100% | 100% | 63% |
| Basal Ct-M | 0.76 | 39 | 67% | 97% | 86% | 91% |
| Stimulated Ct-M | 0.9 | 611 | 67% | 100% | 100% | 91% |
| Fugazzola et al. (2021) [49] | ||||||
| Basal Ct-F | 0.91 | 30 | 75.9% | 93.7% | 88% | 86.5% |
| Stimulated Ct-F | 0.84 | 79 | 100% | 50% | 53.8% | 100% |
| Basal Ct-M | 0.97 | 34 | 88.9% | 95% | 88.9% | 92.6% |
| Stimulated Ct-M | 0.90 | 466 | 94.4% | 80% | 68% | 94.2% |
| Niederle et al. (2020) [50] | ||||||
| Basal Ct-F | 0.94 | 23 | 81% | 100% | 100% | 83% |
| Stimulated Ct-F | 0.87 | 780 | 69% | 100% | 100% | 76% |
| Basal Ct-M | 0.89 | 43 | 53% | 100% | 100% | 67% |
| Stimulated Ct-M | 0.85 | 1500 | 55% | 100% | 100% | 68% |
| Rosario and Calsolari (2017) [18] | ||||||
| Basal Ct-H | / | 47 | 50% | 100% | 100% | 92.1% |
| Basal Ct-L | / | 24.6 | 100% | 74.3% | 40% | 100% |
| Stimulated Ct-H | / | 655.2 | 33.3% | 100% | 100% | 89.7% |
| Stimulated Ct-L | / | 186.5 | 100% | 60% | 30% | 100% |
| Mian et al. (2014) [24] | ||||||
| Basal Ct-F | 0.95 | 26 | 81.8% | 97.9% | 94.7% | 92% |
| Stimulated Ct-F | 0.93 | 79 | 100% | 76.6% | 68.7% | 100% |
| Basal Ct-M | 0.94 | 68 | 83.3% | 100% | 100% | 92.9% |
| Stimulated Ct-M | 0.94 | 544 | 77.8% | 85.4% | 68.4% | 89.2% |
| Colombo et al. (2012) [19] | ||||||
| Basal Ct-F | 1 | 18.7 | 100% | 100% | 100% | 100% |
| Stimulated Ct-F | 0.98 | 184 | 100% | 92.9% | 6.6% | 100% |
| Basal Ct-M | 1 | 68 | 100% | 100% | 100% | 100% |
| Stimulated Ct-M | 0.93 | 1620 | 75% | 100% | 100% | 99.9% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ilic, J.; Tausanovic, K.; Zoric, G.; Jovanovic, M.; Buzejic, M.; Ivanis, S.; Parezanovic, M.; Marinkovic, M.; Karamarkovic, N.; Petakov, A.; et al. Comparing the Diagnostic Efficacy of Different Calcitonin Stimulation Tests for Sporadic Medullary Thyroid Carcinoma: Calcium Gluconate vs. Calcium Chloride. Diagnostics 2025, 15, 1850. https://doi.org/10.3390/diagnostics15151850
Ilic J, Tausanovic K, Zoric G, Jovanovic M, Buzejic M, Ivanis S, Parezanovic M, Marinkovic M, Karamarkovic N, Petakov A, et al. Comparing the Diagnostic Efficacy of Different Calcitonin Stimulation Tests for Sporadic Medullary Thyroid Carcinoma: Calcium Gluconate vs. Calcium Chloride. Diagnostics. 2025; 15(15):1850. https://doi.org/10.3390/diagnostics15151850
Chicago/Turabian StyleIlic, Jovan, Katarina Tausanovic, Goran Zoric, Milan Jovanovic, Matija Buzejic, Sara Ivanis, Milan Parezanovic, Milan Marinkovic, Nemanja Karamarkovic, Ana Petakov, and et al. 2025. "Comparing the Diagnostic Efficacy of Different Calcitonin Stimulation Tests for Sporadic Medullary Thyroid Carcinoma: Calcium Gluconate vs. Calcium Chloride" Diagnostics 15, no. 15: 1850. https://doi.org/10.3390/diagnostics15151850
APA StyleIlic, J., Tausanovic, K., Zoric, G., Jovanovic, M., Buzejic, M., Ivanis, S., Parezanovic, M., Marinkovic, M., Karamarkovic, N., Petakov, A., & Zivaljevic, V. (2025). Comparing the Diagnostic Efficacy of Different Calcitonin Stimulation Tests for Sporadic Medullary Thyroid Carcinoma: Calcium Gluconate vs. Calcium Chloride. Diagnostics, 15(15), 1850. https://doi.org/10.3390/diagnostics15151850